
Salivary Assessments in Post-Liver Transplantation Patients

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Total Protein Content
2.3. Protease Analysis
2.4. Self-Reported Oral Health Questionnaire
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Study Groups
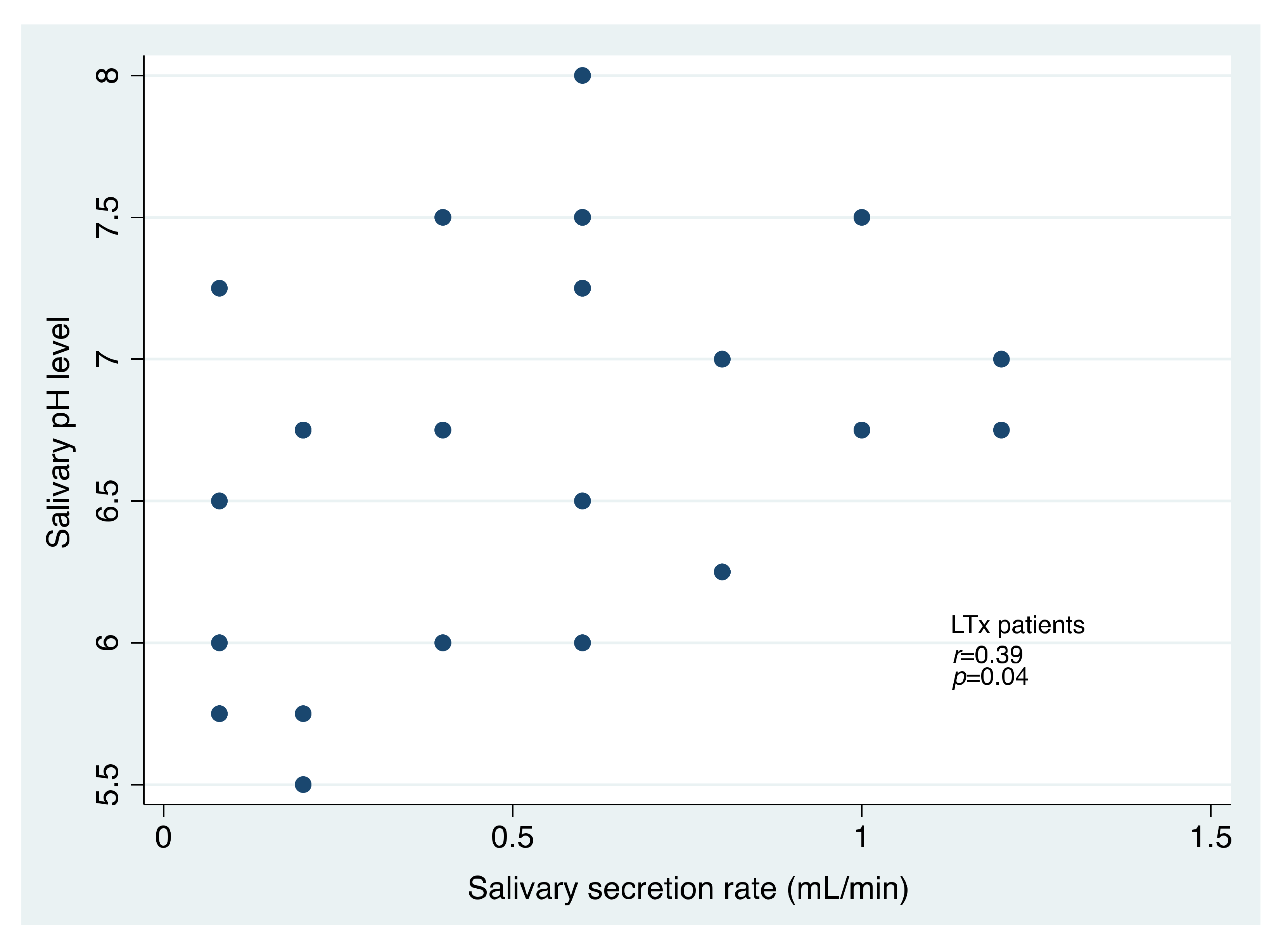
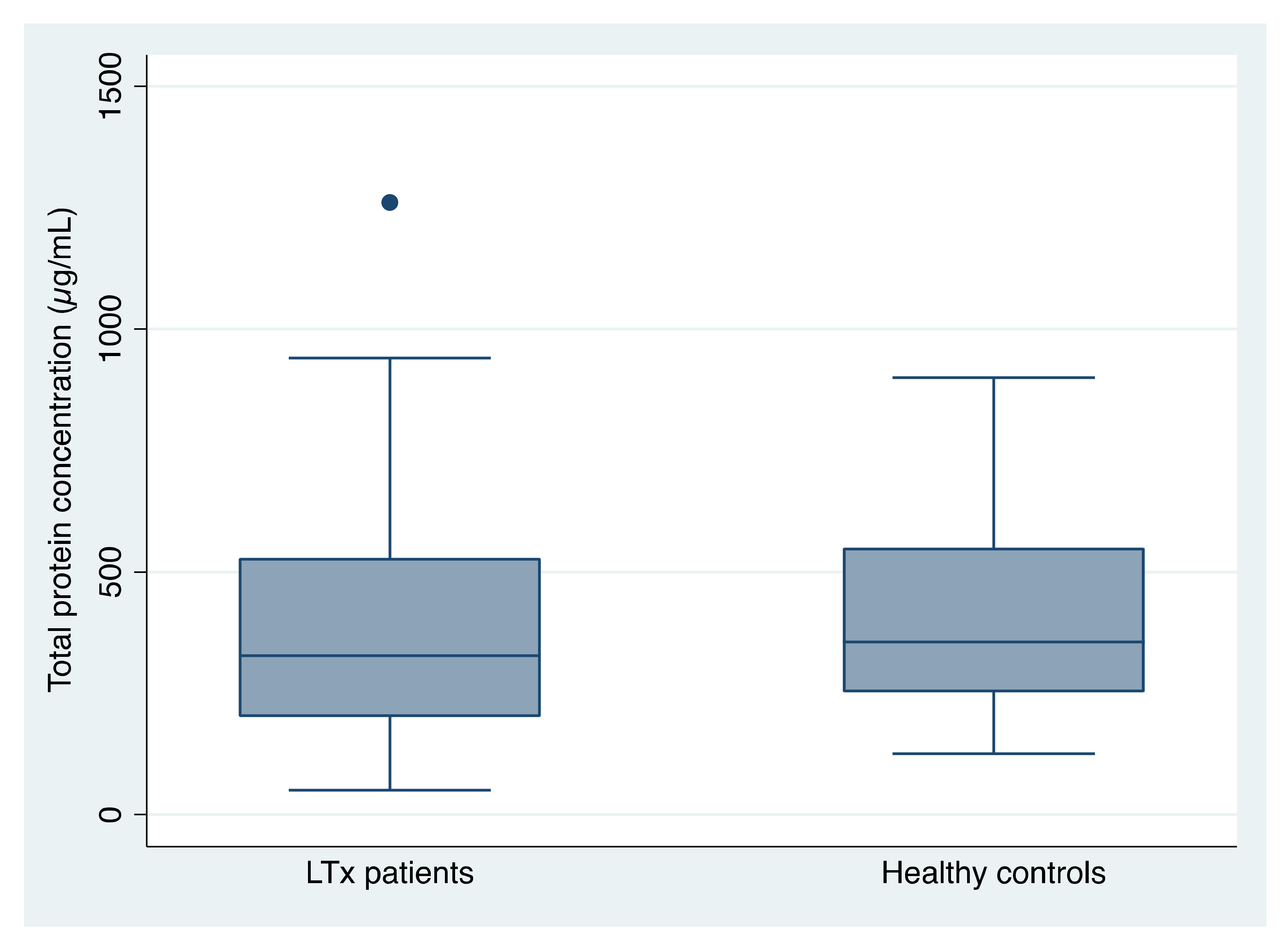
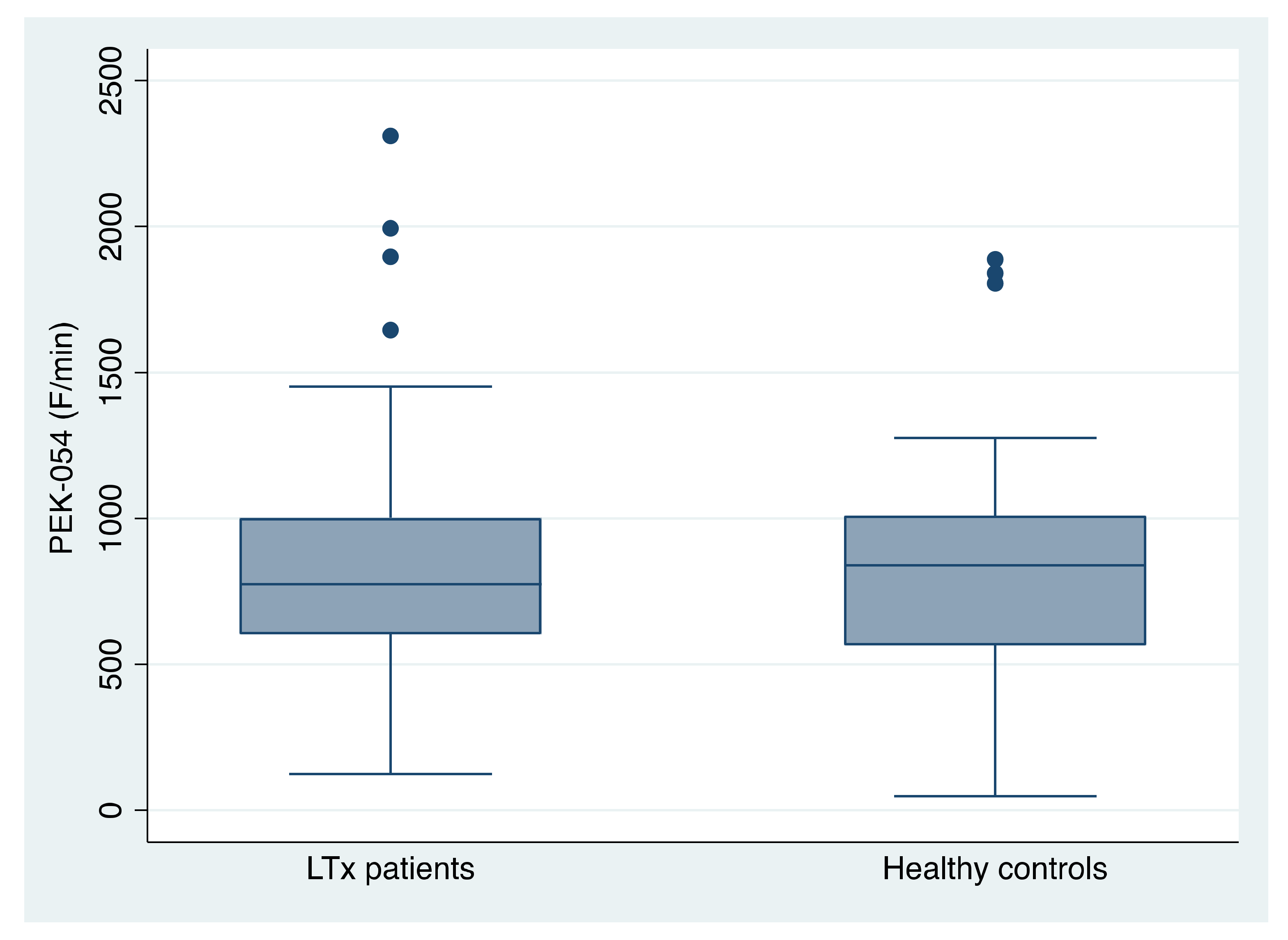
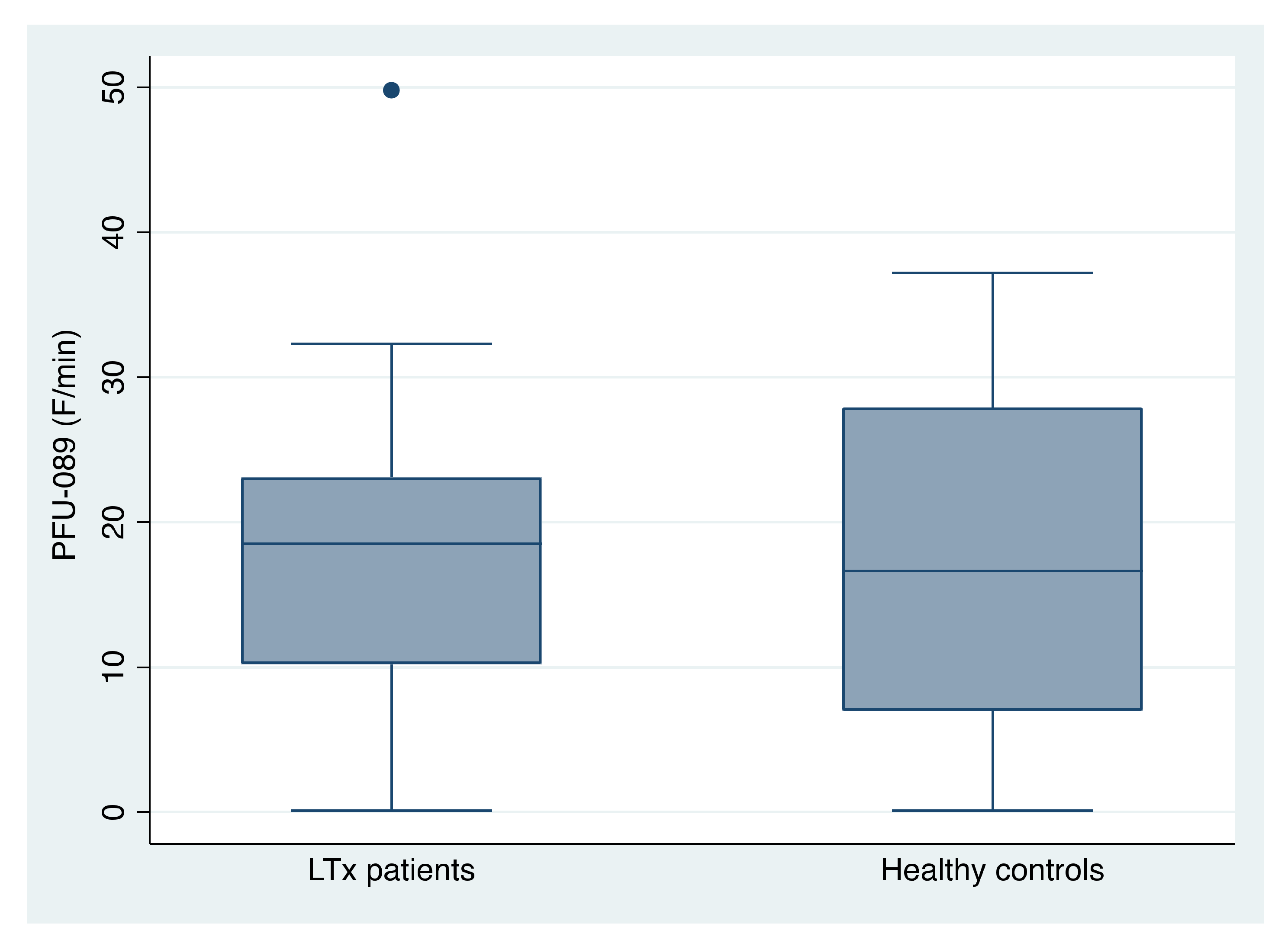
3.2. Salivary Assessments
3.3. Self-Reported Oral Health (SROH)
4. Discussion
4.1. The Total Protein Concentration
4.2. Protease Activity
4.3. Self-Reported Oral Health (SROH) in Relationship with Salivary Assessments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brand, H.S.; Veerman, E.C. Saliva and wound healing. Chin. J. Dent. Res. 2013, 16, 7–12. [Google Scholar] [PubMed]
- Miricescu, D.; Greabu, M.; Totan, A.; Mohora, M.; Didilescu, A.; Mitrea, N.; Arsene, A.L.; Spinu, T.; Totan, C.; Radulescu, R. Oxidative stress—A possible link between systemic and oral diseases. Farmacia 2011, 59, 329–337. [Google Scholar]
- Henson, B.S.; Wong, D.T. Collection, storage, and processing of saliva samples for downstream molecular applications. Methods Mol. Biol. 2010, 666, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.; Lamster, I.B. The diagnostic applications of saliva—A review. Crit. Rev. Oral Biol. Med. 2002, 13, 197–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidovich, E.; Mozer, Y.; Polak, D. Salivary inflammatory cytokines echo the low inflammatory burden in liver-transplanted children. Clin. Oral Investig. 2021, 25, 2993–2998. [Google Scholar] [CrossRef] [PubMed]
- Ramirez Martinez-Acitores, L.; Hernandez Ruiz de Azcarate, F.; Casanas, E.; Serrano, J.; Hernandez, G.; Lopez-Pintor, R.M. Xerostomia and Aalivary Flow in Patients Taking Antihypertensive Drugs. Int. J. Environ. Res. Public Health 2020, 17, 2478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulthuis, M.S.; Jan Jager, D.H.; Brand, H.S. Relationship among perceived stress, xerostomia, and salivary flow rate in patients visiting a saliva clinic. Clin. Oral Investig. 2018, 22, 3121–3127. [Google Scholar] [CrossRef] [Green Version]
- Helenius-Hietala, J.; Ruokonen, H.; Gronroos, L.; Rissanen, H.; Suominen, L.; Isoniemi, H.; Meurman, J.H. Self-reported oral symptoms and signs in liver transplant recipients and a control population. Liver Transpl. 2013, 19, 155–163. [Google Scholar] [CrossRef]
- Didilescu, A.C.; Lazu, A.; Pronk, C.; Vacaru, R.P.; Brand, H.S. Clinical periodontal and dental findings in liver transplant patients: A systematic review and meta-analysis. Br. Dent. J. 2020, 228, 108–116. [Google Scholar] [CrossRef]
- Didilescu, A.C.; Vacaru, R.P.; Pronk, C.; Scheau, C.; Lazu, A.; Dan, L.P.; Brand, H.S. Oral diseases after liver transplantation: A systematic review and meta-analysis. Br. Dent. J. 2021, 231, 117–124. [Google Scholar] [CrossRef]
- Verhulst, M.J.L.; Teeuw, W.J.; Bizzarro, S.; Muris, J.; Su, N.; Nicu, E.A.; Nazmi, K.; Bikker, F.J.; Loos, B.G. A rapid, non-invasive tool for periodontitis screening in a medical care setting. BMC Oral Health 2019, 19, 87. [Google Scholar] [CrossRef]
- Genco, R.J.; Falkner, K.L.; Grossi, S.; Dunford, R.; Trevisan, M. Validity of self-reported measures for surveillance of periodontal disease in two western New York population-based studies. J. Periodontol. 2007, 78, 1439–1454. [Google Scholar] [CrossRef] [PubMed]
- Lazu, A.; Didilescu, A.C.; Dan, L.P.; Brand, H.S.; Sfeatcu, R. Self-reported oral health among Romanian patients with liver transplant: A pilot study. Rom. J. Oral Rehabil. 2020, 12, 244–249. [Google Scholar]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Beck, J.D.; Taylor, G.W.; Borgnakke, W.S.; Page, R.C.; Genco, R.J. Self-reported measures for surveillance of periodontitis. J. Dent. Res. 2013, 92, 1041–1047. [Google Scholar] [CrossRef]
- Pitiphat, W.; Garcia, R.I.; Douglass, C.W.; Joshipura, K.J. Validation of self-reported oral health measures. J. Public Health Dent. 2002, 62, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Blicher, B.; Joshipura, K.; Eke, P. Validation of self-reported periodontal disease: A systematic review. J. Dent. Res. 2005, 84, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Heaton, B.; Gordon, N.B.; Garcia, R.I.; Rosenberg, L.; Rich, S.; Fox, M.P.; Cozier, Y.C. A Clinical Validation of Self-Reported Periodontitis Among Participants in the Black Womens Health Study. J. Periodontol. 2017, 88, 582–592. [Google Scholar] [CrossRef]
- Gursoy, U.K.; Fteita, D.; Bikker, F.J.; Grande, M.A.; Nazmi, K.; Gursoy, M.; Kononen, E.; Belstrom, D. Elevated Baseline Salivary Protease Activity May Predict the Steadiness of Gingival Inflammation During Periodontal Healing: A 12-Week Follow-Up Study on Adults. Pathogens 2020, 9, 751. [Google Scholar] [CrossRef]
- Shaila, M.; Pai, G.P.; Shetty, P. Salivary protein concentration, flow rate, buffer capacity and pH estimation: A comparative study among young and elderly subjects, both normal and with gingivitis and periodontitis. J. Indian Soc. Periodontol. 2013, 17, 42–46. [Google Scholar] [CrossRef]
- Beltzer, E.K.; Fortunato, C.K.; Guaderrama, M.M.; Peckins, M.K.; Garramone, B.M.; Granger, D.A. Salivary flow and alpha-amylase: Collection technique, duration, and oral fluid type. Physiol. Behav. 2010, 101, 289–296. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Navazesh, M.; Kumar, S.K. Measuring salivary flow: Challenges and opportunities. J. Am. Dent. Assoc. 2008, 139, 35S–40S. [Google Scholar] [CrossRef] [PubMed]
- Vacaru, R.P.; Didilescu, A.C.; Constantinescu, I.; Maruntelu, I.; Tanase, M.; Stanciu, I.A.; Kaman, W.E.; Brand, H.S. Salivary Enzymatic Activity and Carious Experience in Children: A Cross-Sectional Study. Children 2022, 9, 343. [Google Scholar] [CrossRef] [PubMed]
- Janus, M.M.; Keijser, B.J.; Bikker, F.J.; Exterkate, R.A.; Crielaard, W.; Krom, B.P. In vitro phenotypic differentiation towards commensal and pathogenic oral biofilms. Biofouling 2015, 31, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Chauncey, H.H. Salivary enzymes. J. Am. Dent. Assoc. 1961, 63, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Aframian, D.J.; Davidowitz, T.; Benoliel, R. The distribution of oral mucosal pH values in healthy saliva secretors. Oral Dis. 2006, 12, 420–423. [Google Scholar] [CrossRef]
- Maldupa, I.; Brinkmane, A.; Mihailova, A. Comparative analysis of CRT Buffer, GC saliva check buffer tests and laboratory titration to evaluate saliva buffering capacity. Stomatologija 2011, 13, 55–61. [Google Scholar]
- Davidovich, E.; Asher, R.; Shapira, J.; Brand, H.S.; Veerman, E.C.; Shapiro, R. Mucosal pH, dental findings, and salivary composition in pediatric liver transplant recipients. Transplantation 2013, 96, 102–107. [Google Scholar] [CrossRef]
- Pedersen, A.M.; Bardow, A.; Jensen, S.B.; Nauntofte, B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002, 8, 117–129. [Google Scholar] [CrossRef]
- Gholami, N.; Hosseini Sabzvari, B.; Razzaghi, A.; Salah, S. Effect of stress, anxiety and depression on unstimulated salivary flow rate and xerostomia. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 11, 247–252. [Google Scholar] [CrossRef]
- Zahed, M.; Bahador, M.; Hosseini Asl, M.K.; Lavaee, F.; Azad, A.; Bahador, A. Oro-Dental Health of Patients with Chronic Hepatic Failure. Int. J. Organ Transpl. Med. 2020, 11, 115–121. [Google Scholar]
- Abelson, D.C.; Mandel, I.D.; Karmiol, M. Salivary studies in alcoholic cirrhosis. Oral Surg. Oral Med. Oral Pathol. 1976, 41, 188–192. [Google Scholar] [CrossRef]
- Helenius-Hietala, J.; Ruokonen, H.; Gronroos, L.; Rissanen, H.; Vehkalahti, M.M.; Suominen, L.; Isoniemi, H.; Meurman, J.H. Oral mucosal health in liver transplant recipients and controls. Liver Transpl. 2014, 20, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Rojas, G.; Bravo, L.; Cordero, K.; Sepulveda, L.; Elgueta, L.; Diaz, J.C.; Urzua, B.; Morales, I. Integrity of the oral tissues in patients with solid-organ transplants. J. Transpl. 2012, 2012, 603769. [Google Scholar] [CrossRef]
- Hoek, G.H.; Brand, H.S.; Veerman, E.C.; Amerongen, A.V. Toothbrushing affects the protein composition of whole saliva. Eur. J. Oral Sci. 2002, 110, 480–481. [Google Scholar] [CrossRef] [PubMed]
- Fiyaz, M.; Ramesh, A.; Ramalingam, K.; Thomas, B.; Shetty, S.; Prakash, P. Association of salivary calcium, phosphate, pH and flow rate on oral health: A study on 90 subjects. J. Indian Soc. Periodontol. 2013, 17, 454–460. [Google Scholar] [CrossRef]
- Amerongen, A.V.; Veerman, E.C. Saliva—The defender of the oral cavity. Oral Dis. 2002, 8, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Oppenheim, F.G.; Salih, E.; Siqueira, W.L.; Zhang, W.; Helmerhorst, E.J. Salivary proteome and its genetic polymorphisms. Ann. N. Y. Acad. Sci. 2007, 1098, 22–50. [Google Scholar] [CrossRef]
- Bikker, F.J.; Nascimento, G.G.; Nazmi, K.; Silbereisen, A.; Belibasakis, G.N.; Kaman, W.E.; Lopez, R.; Bostanci, N. Salivary Total Protease Activity Based on a Broad-Spectrum Fluorescence Resonance Energy Transfer Approach to Monitor Induction and Resolution of Gingival Inflammation. Mol. Diagn. Ther. 2019, 23, 667–676. [Google Scholar] [CrossRef] [Green Version]
- Kaman, W.E.; Hulst, A.G.; van Alphen, P.T.; Roffel, S.; van der Schans, M.J.; Merkel, T.; van Belkum, A.; Bikker, F.J. Peptide-based fluorescence resonance energy transfer protease substrates for the detection and diagnosis of Bacillus species. Anal. Chem. 2011, 83, 2511–2517. [Google Scholar] [CrossRef]
- Kaman, W.E.; Galassi, F.; de Soet, J.J.; Bizzarro, S.; Loos, B.G.; Veerman, E.C.; van Belkum, A.; Hays, J.P.; Bikker, F.J. Highly specific protease-based approach for detection of porphyromonas gingivalis in diagnosis of periodontitis. J. Clin. Microbiol. 2012, 50, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaman, W.E.; Voskamp-Visser, I.; de Jongh, D.M.; Endtz, H.P.; van Belkum, A.; Hays, J.P.; Bikker, F.J. Evaluation of a D-amino-acid-containing fluorescence resonance energy transfer peptide library for profiling prokaryotic proteases. Anal. Biochem. 2013, 441, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Schmalz, G.; Kauffels, A.; Widmer, F.; Widmer, K.; Slotta, J.E.; Mausberg, R.F.; Kollmar, O. Periodontal pathogenic bacteria and aMMP-8 findings depending on periodontal conditions of patients before and after liver transplantation. Clin. Oral Investig. 2017, 21, 745–752. [Google Scholar] [CrossRef]
- Sorsa, T.; Gursoy, U.K.; Nwhator, S.; Hernandez, M.; Tervahartiala, T.; Leppilahti, J.; Gursoy, M.; Kononen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of matrix metalloproteinases, especially MMP-8, in gingival creviclular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontol. 2000 2016, 70, 142–163. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.P.; Trevisan, G.L.; Macedo, G.O.; Palioto, D.B.; Souza, S.L.; Grisi, M.F.; Novaes, A.B., Jr.; Taba, M., Jr. Salivary interleukin-6, matrix metalloproteinase-8, and osteoprotegerin in patients with periodontitis and diabetes. J. Periodontol. 2010, 81, 384–391. [Google Scholar] [CrossRef]
- Norrman, A.E.; Tervahartiala, T.; Sahlberg, E.; Sorsa, T.; Ruokonen, H.; Gronroos, L.; Meurman, J.H.; Isoniemi, H.; Nordin, A.; Aberg, F.; et al. Salivary Biomarkers and Oral Health in Liver Transplant Recipients, with an Emphasis on Diabetes. Diagnostics 2021, 11, 662. [Google Scholar] [CrossRef]
- Lee, S.O.; Kang, S.H.; Abdel-Massih, R.C.; Brown, R.A.; Razonable, R.R. Spectrum of early-onset and late-onset bacteremias after liver transplantation: Implications for management. Liver Transpl. 2011, 17, 733–741. [Google Scholar] [CrossRef] [Green Version]
- Seymour, G.J.; Ford, P.J.; Cullinan, M.P.; Leishman, S.; Yamazaki, K. Relationship between periodontal infections and systemic disease. Clin. Microbiol. Infect. 2007, 13, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Fishman, J.A. AST Infectious Diseases Community of Practice. Introduction: Infection in solid organ transplant recipients. Am. J. Transplant. 2009, 9, S3–S6. [Google Scholar] [CrossRef]
- Herzer, K.; Sterneck, M.; Welker, M.W.; Nadalin, S.; Kirchner, G.; Braun, F.; Malessa, C.; Herber, A.; Pratschke, J.; Weiss, K.H.; et al. Current Challenges in the Post-Transplant Care of Liver Transplant Recipients in Germany. J. Clin. Med. 2020, 9, 3570. [Google Scholar] [CrossRef]
- Kauffels, A.; Schmalz, G.; Kollmar, O.; Slotta, J.E.; Weig, M.; Gross, U.; Bader, O.; Ziebolz, D. Oral findings and dental behaviour before and after liver transplantation—A single-centre cross-sectional study. Int. Dent. J. 2017, 67, 244–251. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | LTx Patients | Healthy Controls |
|---|---|---|
| Age Mean (SD) | 54.4 (9.4) | 53.3 (9.7) |
| Males N (%) | 11 (42.3) | 7 (26.9) |
| Smoking N (%) | 3 (11.5) | 5 (19.2) |
| Rural N (%) | 5 (19.2) | 1 (3.8) |
| Tertiary education N (%) | 18 (69.23) | 17 (65.38) |
| Frequency of dental check-ups per year | ||
| N (%) | ||
| 0 | 14 (53.85) | 10 (38.46) |
| 1 | 3 (11.54) | 6 (23.08) |
| 2 | 9 (34.62) | 10 (38.46) |
| SROH QUESTION (Abbreviation) | LTx Patients | Healthy Controls | p-Value |
|---|---|---|---|
| Q1. Have gum disease | |||
| Yes | 6 (50%) | 6 (50%) | 0.78 1 |
| No | 13 (46.43%) | 15 (53.57%) | |
| Don’t know | 7 (58.33%) | 5 (41.67%) | |
| Q2. Teeth/gum health | |||
| Poor | 6 (54.55%) | 5 (45.45%) | 0.88 2 |
| Fair | 4 (36.36%) | 7 (63.64%) | |
| Good | 9 (47.37%) | 10 (52.63%) | |
| Very good | 4 (57.14%) | 3 (42.86%) | |
| Excellent | 1 (100%) | 0 | |
| Don’t know | 2 (66.67%) | 1 (33.33%) | |
| Q3. Had gum treatment | |||
| Yes | 11 (44%) | 14 (56%) | 0.41 1 |
| No | 15 (55.56%) | 12 (44.44%) | |
| Q4. Loose tooth | |||
| Yes | 9 (52.94%) | 8 (47.06%) | 0.17 2 |
| No | 14 (43.75%) | 18 (56.25%) | |
| Don’t know | 3 (100%) | 0 | |
| Q5. Lost bone | |||
| Yes | 3 (33.33%) | 6 (66.67%) | 0.29 2 |
| No | 23 (54.76%) | 19 (45.24%) | |
| Don’t know | 0 | 1 (100%) | |
| Q6. Tooth does not look right | |||
| Yes | 4 (44.44%) | 5 (55.56%) | 0.73 2 |
| No | 22 (52.38%) | 20 (47.62%) | |
| Don’t know | 0 | 1 (100%) | |
| Q7. Floss use | |||
| Yes | 7 (31.82%) | 15 (68.18%) | 0.02 1,* |
| No | 19 (63.33%) | 11 (36.67%) | |
| Q8. Mouthwash use | |||
| Yes | 12 (34.29%) | 23 (65.71%) | 0.003 2,* |
| No | 14 (82.35%) | 3 (17.65%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Didilescu, A.C.; Lazu, A.; Vlădan, C.; Scheau, C.; Dan Popa, L.; Șurlin, P.; Kaman, W.E.; Brand, H.S. Salivary Assessments in Post-Liver Transplantation Patients. J. Clin. Med. 2022, 11, 3152. https://doi.org/10.3390/jcm11113152
Didilescu AC, Lazu A, Vlădan C, Scheau C, Dan Popa L, Șurlin P, Kaman WE, Brand HS. Salivary Assessments in Post-Liver Transplantation Patients. Journal of Clinical Medicine. 2022; 11(11):3152. https://doi.org/10.3390/jcm11113152
Chicago/Turabian StyleDidilescu, Andreea Cristiana, Adelina Lazu, Cristian Vlădan, Cristian Scheau, Laura Dan Popa, Petra Șurlin, Wendy Esmeralda Kaman, and Hendrik Simon Brand. 2022. "Salivary Assessments in Post-Liver Transplantation Patients" Journal of Clinical Medicine 11, no. 11: 3152. https://doi.org/10.3390/jcm11113152