
Efficacy of Acupuncture on Quality of Life, Functional Performance, Dyspnea, and Pulmonary Function in Patients with Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Clinical Trial

 , , , ,
, , , ,  ,
,  , and
, and 
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
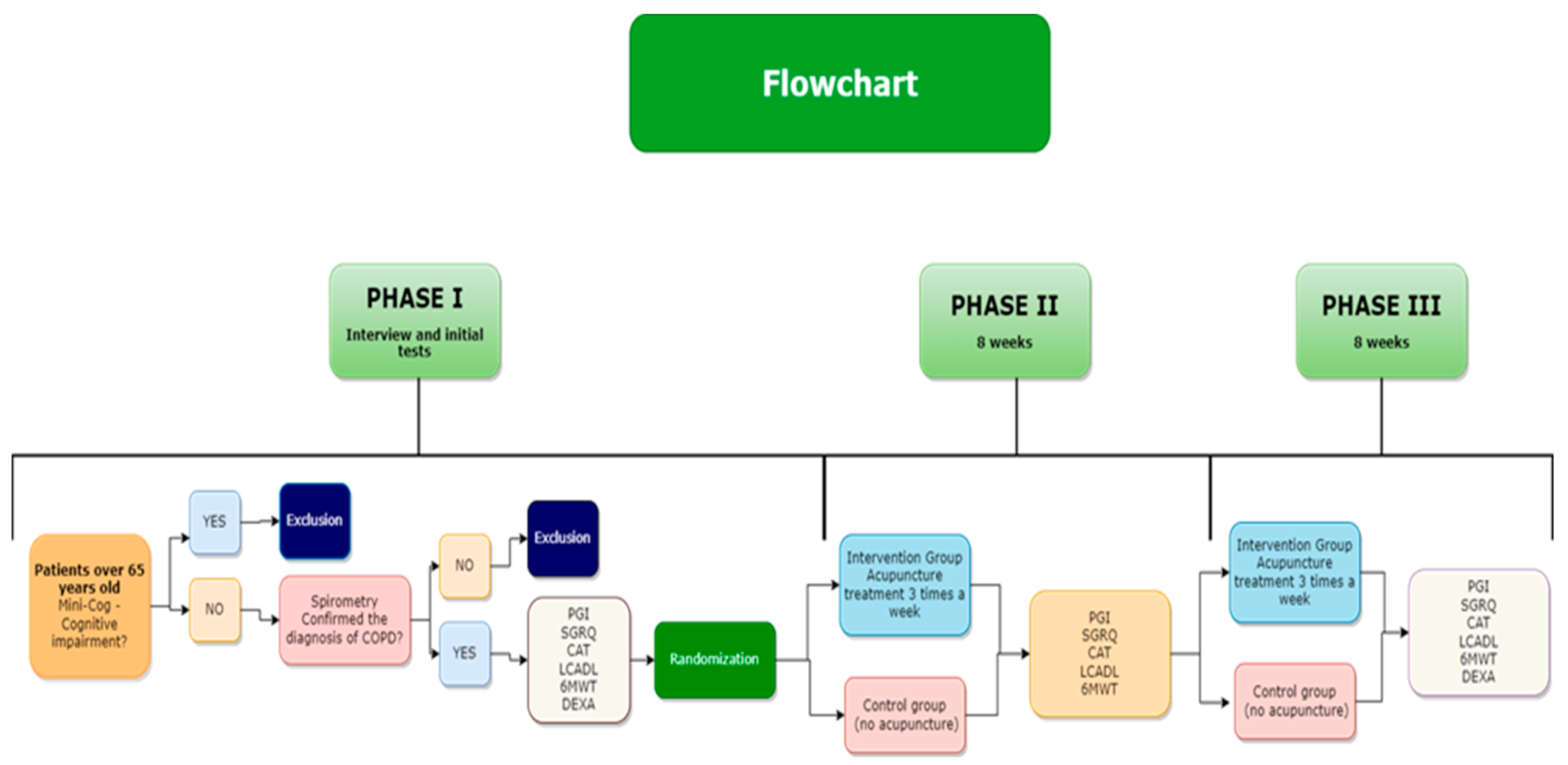
2.1. Design
2.2. Patients
2.3. Randomization
2.4. Eligibility
2.4.1. Inclusion Criteria
- Clinical diagnosis of COPD according to GOLD [1].
- Ability to offer written authorization or nominate a person to read the Statement of Free and Informed Consent, giving the research patient’s agreement.
- Patients over 65 years of age with preserved cognitive function according to the Mini-Cog, that is, those who scored at least 3 to 5 points [30].
- Absence of exacerbation and stability of drug treatment in the last month.
- A 3-month absence from participation in a pulmonary rehabilitation program.
2.4.2. Exclusion Criteria
- Patient with a previous medical diagnosis of a disease that affects cognitive function and inhibits understanding of the questionnaires.
- Patients unable to perform any of the assessments.
- Previous acupuncture therapy.
- Being, or having been, in a rehabilitation group in the last 3 months before starting the protocol.
- Patients who present an exacerbation of the clinical condition during the collection period will be excluded.
2.5. Intervention
Acupuncture
- (a)
- the Traditional Chinese Medicine needling style will be used, based on the literature in the area and clinical consensus.
- (b)
- treatment reasoning will be based on Chinese acupuncture literature, consensual methods, and literary references.
- (c)
- the selection of needling points will not change throughout the treatment.
- (d)
- the needling will be manual.
- Zusanli-stomach 36 (ST36 bilateral).
- Xuehai-spleen 10 (SP10 bilateral)
- Qihai-Ren Mai 6 (RM6 or CV6).
- Danzhong–Ren Mai 17 (RM17 or CV17).
- Chize-lung 5 (LU5 bilateral).
- Lieque-lung 7 (LU7 bilateral).
2.6. Outcome Measures
2.6.1. Questionnaires, Scales and Tests
Mini-Cog
Double Energy X-ray Absorptiometry (DEXA)
Spirometry
Patient-Generated Index (PGI)
Saint George’s Respiratory Questionnaire (SGRQ)
London Chest Activity of Daily Living (LCADL)
Six-Minute Walk Test (6MWT)
COPD Assessment Test (CAT)
2.7. Ethics
2.8. Analyses
Treatment of Lost Data (Missing Data)
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for Prevention, Diagnosis and Management of COPD; Global Initiative for Chronic Obstructive Lung Disease: Fontana, WI, USA, 2022; p. 177. [Google Scholar]
- Sin, D.D.; Anthonisen, N.R.; Soriano, J.B.; Agusti, A.G. Mortality in COPD: Role of comorbidities. Eur. Respir. J. 2006, 28, 1245–1257. [Google Scholar] [CrossRef] [PubMed]
- da Silva Lage, V.K.; de Paula, F.A.; Dos Santos, J.M.; Costa, H.S.; da Silva, G.P.; Lima, L.P.; Santos, J.N.V.; de Almeida, H.C.; Figueiredo, P.H.S.; Bernardo-Filho, M.; et al. Are oxidative stress biomarkers and respiratory muscles strength associated with COPD-related sarcopenia in older adults? Exp. Geront. 2021, 157, 111630. [Google Scholar] [CrossRef]
- Decramer, M.; Janssens, W.; Miravitlles, M. Chronic obstructive pulmonary disease. Lancet 2012, 379, 1341–1351. [Google Scholar] [CrossRef]
- Arrieiro, A.N.; Soares, L.A.; Prates, A.C.N.; Figueiredo, P.H.S.; Costa, H.S.; Simão, A.P.; Neves, C.D.C.; dos Santos, J.M.; Santos, L.M.D.M.; Avelar, N.C.P.; et al. Inflammation Biomarkers Are Independent Contributors to Functional Performance in Chronic Conditions: An Exploratory Study. Int. J. Med. Sci. Health Res. 2021, 5, 30–37. [Google Scholar] [CrossRef]
- De-Miguel-Diez, J.; Jimenez-Garcia, R.; Hernandez-Barrera, V.; De-Miguel-Yanes, J.M.; Carabantes-Alarcon, D.; Lopez-De-Andres, A. Assessing the Impact of Gender and COPD on the Incidence and Mortality of Hospital-Acquired Pneumonia. A Retrospective Cohort Study Using the Spanish National Discharge Database (2016–2019). J. Clin. Med. 2021, 10, 5453. [Google Scholar] [CrossRef]
- Man, W.; Donaldson, A.V.; Maddocks, M.; Martolini, D.; Polkey, M. Muscle function in COPD: A complex interplay. Int. J. Chronic Obstr. Pulm. Dis. 2012, 7, 523–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimenta, S.; Silva, C.G.; Flora, S.; Hipólito, N.; Burtin, C.; Oliveira, A.; Morais, N.; Brites-Pereira, M.; Carreira, B.P.; Januário, F.; et al. What Motivates Patients with COPD to Be Physically Active? A Cross-Sectional Study. J. Clin. Med. 2021, 10, 5631. [Google Scholar] [CrossRef]
- Lage, V.K.D.S.; da Silva, G.P.; Lacerda, A.C.R.; de Paula, F.A.; Lima, L.P.; Santos, J.N.V.; de Almeida, H.C.; Pinto, A.G.F.; Figueiredo, P.H.S.; Costa, H.S.; et al. Functional tests associated with sarcopenia in moderate chronic obstructive pulmonary disease. Expert Rev. Respir. Med. 2020, 15, 569–576. [Google Scholar] [CrossRef]
- Sanchez-Ramirez, D.C. Impact of Pulmonary Rehabilitation Services in Patients with Different Lung Diseases. J. Clin. Med. 2022, 11, 407. [Google Scholar] [CrossRef]
- Regueiro, E.M.G.; Di Lorenzo, V.A.P.; Parizotto, A.P.D.D.; Negrini, F.; Sampaio, L.M.M. Analysis of metabolic and ventilatory demand during the execution of daily life activities in individuals with chronic obstructive pulmonary disease. Rev. Lat. Am. Enfermagem. 2006, 14, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Feeny, D.H.; Patrick, D.L. Measuring health-related quality of life. Ann. Intern. Med. 1993, 118, 622–629. [Google Scholar] [CrossRef] [PubMed]
- WHOQOL Group. The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Cardoso, R.F.; Ruta, D.; De Oliveira, T.M.; Costa, M.C.B.; Fonseca, A.A.; Figueiredo, P.H.S.; Bastone, A.D.C.; De Alcântara, M.A.; Lacerda, A.C.R.; Lima, V.P. Portuguese translation and validation of the Patient Generated Index instrument for patients with Chronic Obstructive Pulmonary Disease: Individualized quality of life assessment. J. Bras. Pneumol. 2020, 46, e20190272. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-S. Guidelines for Chinese medicine rehabilitation of chronic obstructive pulmonary disease. World J. Tradit. Chin. Med. 2020, 6, 295. [Google Scholar] [CrossRef]
- Suzuki, M.; Yokoyama, Y.; Yamazaki, H. Research into Acupuncture for Respiratory Disease in Japan: A Systematic Review. Acupunct. Med. 2009, 27, 54–60. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Benchmarks for the Practice of Acupuncture; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. WHO Global Report on Traditional and Complementary Medicine 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Política Nacional de Práticas Integrativas e Complementares No SUS; Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica: Rio de Janeiro, Brazil, 2015. [Google Scholar]
- Souto-Miranda, S.; Mendes, M.A.; Cravo, J.; Andrade, L.; Spruit, M.A.; Marques, A. Functional Status Following Pulmonary Rehabilitation: Responders and Non-Responders. J. Clin. Med. 2022, 11, 518. [Google Scholar] [CrossRef] [PubMed]
- Deering, B.M.; Fullen, B.; Egan, C.; McCormack, N.; Kelly, E.; Pender, M.; Costello, R.W. Acupuncture as an Adjunct to Pulmonary Rehabilitation. J. Cardiopulm. Rehabil. Prev. 2011, 31, 392–399. [Google Scholar] [CrossRef]
- Feng, J.; Wang, X.; Li, X.; Zhao, D.; Xu, J. Acupuncture for chronic obstructive pulmonary disease (COPD). Medicine 2016, 95, e4879. [Google Scholar] [CrossRef]
- Fernández-Jané, C.; Vilaró, J.; Fei, Y.; Wang, C.; Liu, J.; Huang, N.; Xia, R.; Tian, X.; Hu, R.-X.; Yu, M.; et al. Filiform needle acupuncture for copd: A systematic review and meta-analysis. Complement. Ther. Med. 2019, 47, 102182. [Google Scholar] [CrossRef]
- Hsieh, P.-C.; Yang, M.-C.; Wu, Y.-K.; Chen, H.-Y.; Tzeng, I.-S.; Hsu, P.-S.; Lee, C.-T.; Chen, C.-L.; Lan, C.-C. Acupuncture therapy improves health-related quality of life in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2019, 35, 208–218. [Google Scholar] [CrossRef]
- Xie, Y.; Li, J.-S.; Yu, X.-Q.; Li, S.-Y.; Zhang, N.-Z.; Li, Z.-G.; Shao, S.-J.; Guo, L.-X.; Zhu, L.; Zhang, Y.-J. Effectiveness of Bufei Yishen Granule combined with acupoint sticking therapy on quality of life in patients with stable chronic obstructive pulmonary disease. Chin. J. Integr. Med. 2013, 19, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.-W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D.; on behalf of the STRICTA Revision Group. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT Statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filho, S.T.R.; Lourenço, R.A. The performance of the Mini-Cog in a sample of low educational level elderly. Dement. Neuropsychol. 2009, 3, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, P.-C.; Cheng, C.-F.; Wu, C.-W.; Tzeng, I.-S.; Kuo, C.-Y.; Hsu, P.-S.; Lee, C.-T.; Yu, M.-C.; Lan, C.-C. Combination of Acupoints in Treating Patients with Chronic Obstructive Pulmonary Disease: An Apriori Algorithm-Based Association Rule Analysis. Evid. Based Complement. Altern. Med. 2020, 2020, 8165296. [Google Scholar] [CrossRef]
- Borson, S.; Scanlan, J.M.; Chen, P.; Ganguli, M. The Mini-Cog as a Screen for Dementia: Validation in a Population-Based Sample. J. Am. Geriatr. Soc. 2003, 51, 1451–1454. [Google Scholar] [CrossRef]
- Pereira, C.A.D.C.; Sato, T.; Rodrigues, S.C. Novos valores de referência para espirometria forçada em brasileiros adultos de raça branca. J. Bras. Pneumol. 2007, 33, 397–406. [Google Scholar] [CrossRef]
- Sociedade Brasileira de Pneumologia e Tisiologia. II Consenso Brasileiro sobre Doença Pulmonar Obstrutiva Crônica—DPOC. J. Bras. Pneumol. 2004, 30, 1–52. [Google Scholar]
- De Sousa, T.C.; Jardim, J.R.; Jones, P.W. Validação do Questionário do Hospital Saint George na Doença Respiratória (SGRQ) em pacientes portadores de doença pulmonar obstrutiva crônica no Brasil. J. Pneumol. 2000, 26, 119–128. [Google Scholar] [CrossRef] [Green Version]
- Carpes, M.F.; Mayer, A.F.; Simon, K.M.; Jardim, J.R.; Garrod, R. Versão brasileira da escala London Chest Activity of Daily Living para uso em pacientes com doença pulmonar obstrutiva crônica. J. Bras. Pneumol. 2012, 34, 128–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, J.P.; Gonçalves, P.A.G.; da Fontoura, F.F.; Mattiello, R.; Florian, J. Aplicabilidade da escala London Chest Activity of Daily Living em pacientes em lista de espera para transplante de pulmão. J. Bras. Pneumol. 2013, 39, 92–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; MacIntyre, N.R.; McKay, R.T.; Johnson, D.; Wanger, J.S.; Zeballos, R.J.; Bittner, V.; et al. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Neves, C.D.; Lage, V.K.; Lima, L.P.; Matos, M.A.; Vieira, L.; Teixeira, A.L.; Figueiredo, P.H.; Costa, H.S.; Lacerda, A.C.R.; Mendonça, V.A. Inflammatory and oxidative biomarkers as determinants of functional capacity in patients with COPD assessed by 6-min walk test-derived outcomes. Exp. Gerontol. 2021, 152, 111456. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Silva, G.P.F.D.; Morano, M.T.A.P.; Viana, C.M.S.; Magalhães, C.B.D.A.; Pereira, E.D.B. Validação do Teste de Avaliação da DPOC em português para uso no Brasil. J. Bras. Pneumol. 2013, 39, 402–408. [Google Scholar] [CrossRef] [Green Version]
- Committee for Medicinal Products for Human Use (CHMP). Guideline on missing data in confirmatory clinical trials. Lond. Eur. Med. Agency 2010, 44, 1–12. [Google Scholar]
- Lewith, G.T.; Prescott, P.; Davis, C.L. Can a standardized acupuncture technique palliate disabling breathlessness: A single-blind, placebo-controlled crossover study. Chest 2004, 125, 1783–1790. [Google Scholar] [CrossRef]
- Wang, J.; Li, J.; Yu, X.; Xie, Y. Acupuncture Therapy for Functional Effects and Quality of Life in COPD Patients: A Systematic Review and Meta-Analysis. Biomed. Res. Int. 2018, 2018, 3026726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, Y. The Dilemma of Placebo Needles in Acupuncture Research. Acupunct. Med. 2017, 35, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Chae, Y.; Lee, Y.S.; Enck, P. How placebo needles differ from placebo pills? Front. Psychiatry 2018, 9, 243. [Google Scholar] [CrossRef] [PubMed]
- Moffet, H.H. Sham acupuncture may be as efficacious as true acupuncture: A systematic review of clinical trials. J. Altern. Complement. Med. 2009, 15, 213–216. [Google Scholar] [CrossRef]
- Zhang, C.S.; Tan, H.Y.; Zhang, G.S.; Zhang, A.L.; Xue, C.C.; Xie, Y.M. Placebo devices as effective control methods in acupuncture clinical trials: A systematic review. PLoS ONE 2015, 10, e0140825. [Google Scholar] [CrossRef]
- Shiwa, S.R.; Costa, L.O.P.; Moser, A.D.D.L.; Aguiar, I.D.C.; Oliveira, L.V.F.D. PEDro: A base de dados de evidências em fisioterapia. Fisioter. Em. Mov. 2011, 24, 523–533. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardoso, R.F.; Lacerda, A.C.R.; Lima, V.P.; de Oliveira, L.F.F.; de Oliveira, S.F.F.; Araújo, R.P.; Castro, C.L.F.e.; da Silva, F.P.; de Paiva, L.V.; Dietrich, L.; et al. Efficacy of Acupuncture on Quality of Life, Functional Performance, Dyspnea, and Pulmonary Function in Patients with Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Clinical Trial. J. Clin. Med. 2022, 11, 3048. https://doi.org/10.3390/jcm11113048
Cardoso RF, Lacerda ACR, Lima VP, de Oliveira LFF, de Oliveira SFF, Araújo RP, Castro CLFe, da Silva FP, de Paiva LV, Dietrich L, et al. Efficacy of Acupuncture on Quality of Life, Functional Performance, Dyspnea, and Pulmonary Function in Patients with Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(11):3048. https://doi.org/10.3390/jcm11113048
Chicago/Turabian StyleCardoso, Renato Fleury, Ana Cristina Rodrigues Lacerda, Vanessa Pereira Lima, Lucas Fróis Fernandes de Oliveira, Sofia Fróis Fernandes de Oliveira, Rafaela Paula Araújo, Cecylia Leiber Fernandes e Castro, Flávia Pereira da Silva, Lizânia Vieira de Paiva, Lia Dietrich, and et al. 2022. "Efficacy of Acupuncture on Quality of Life, Functional Performance, Dyspnea, and Pulmonary Function in Patients with Chronic Obstructive Pulmonary Disease: Protocol for a Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 11: 3048. https://doi.org/10.3390/jcm11113048