
Significant Decrease in the Prevalence of Anxiety and Depression after Hepatitis C Eradication

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Consideration
2.3. Measurements
2.4. Statistical Analysis
3. Results
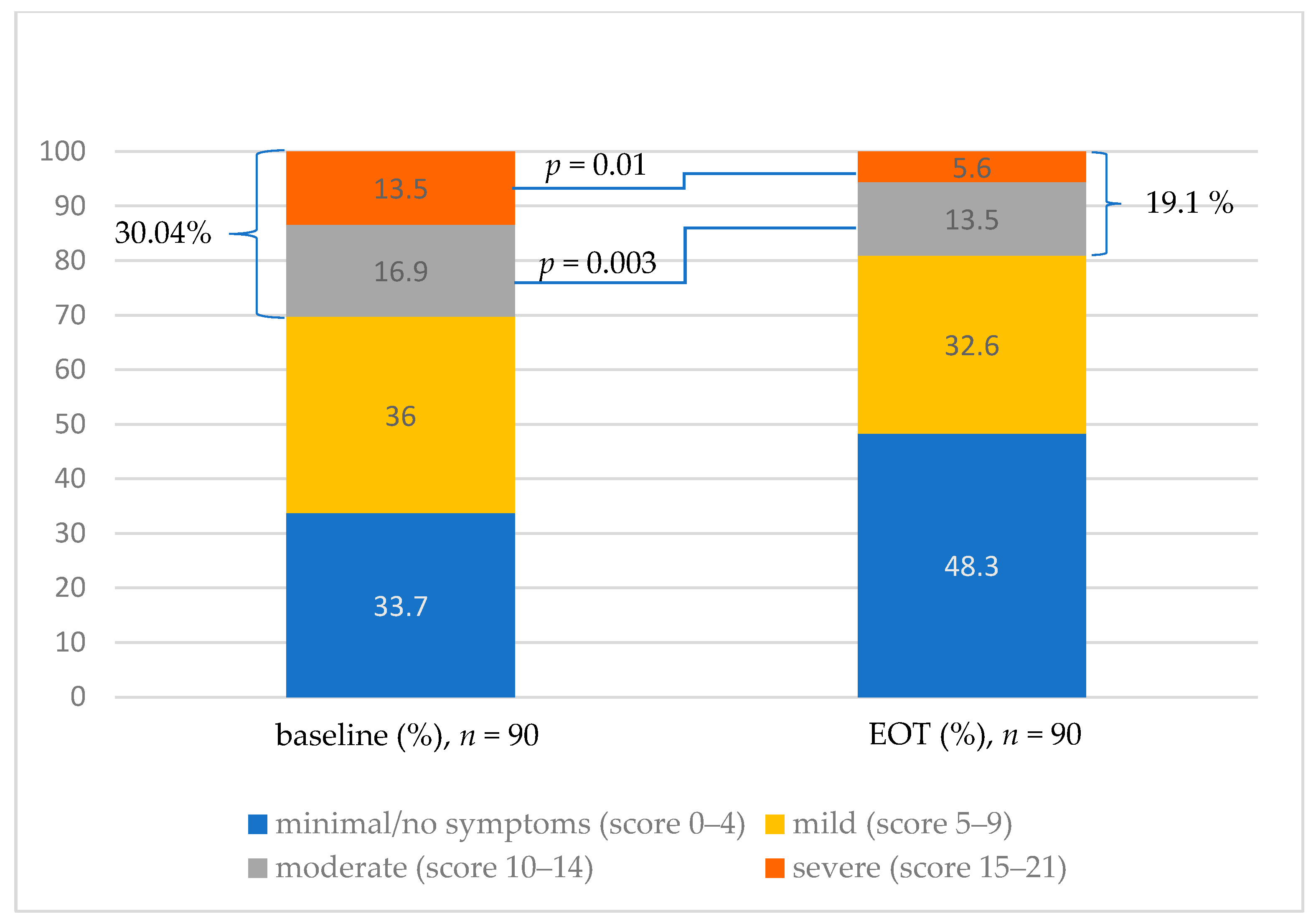
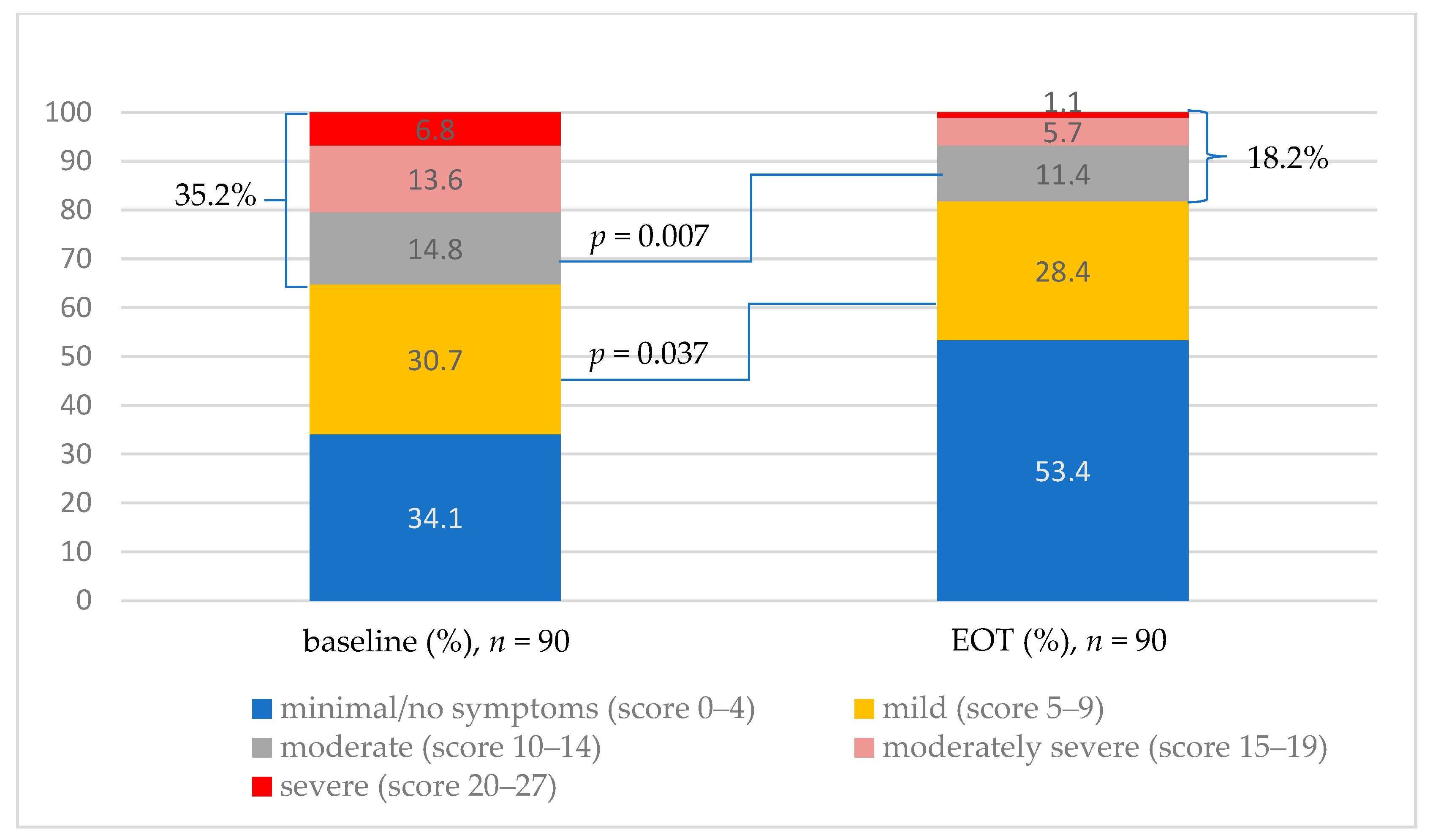
3.1. Prevalence of Anxiety and Depression
3.2. Anxiety and Depression Improvement in Subgroups
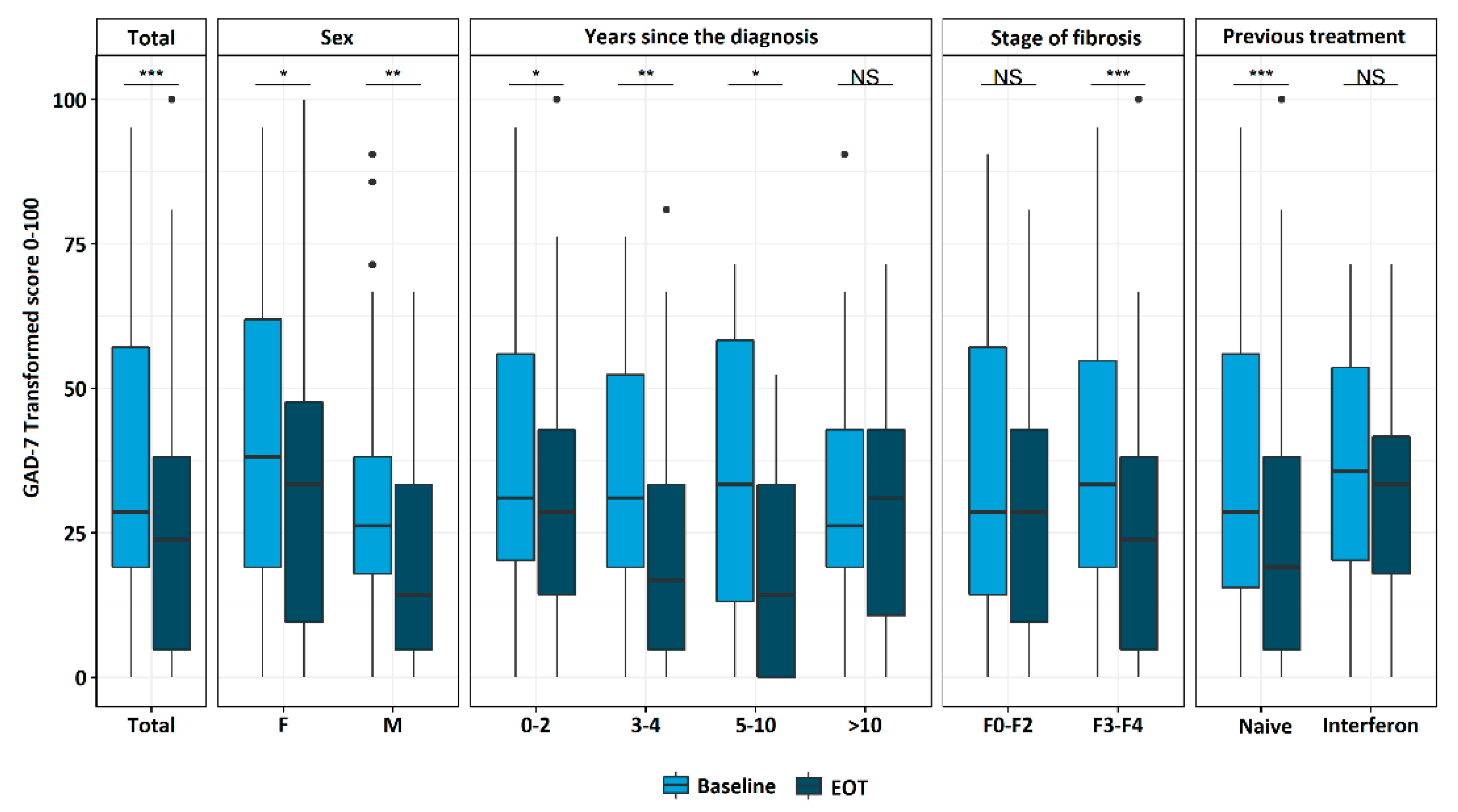
3.2.1. Anxiety Subgroup Analysis
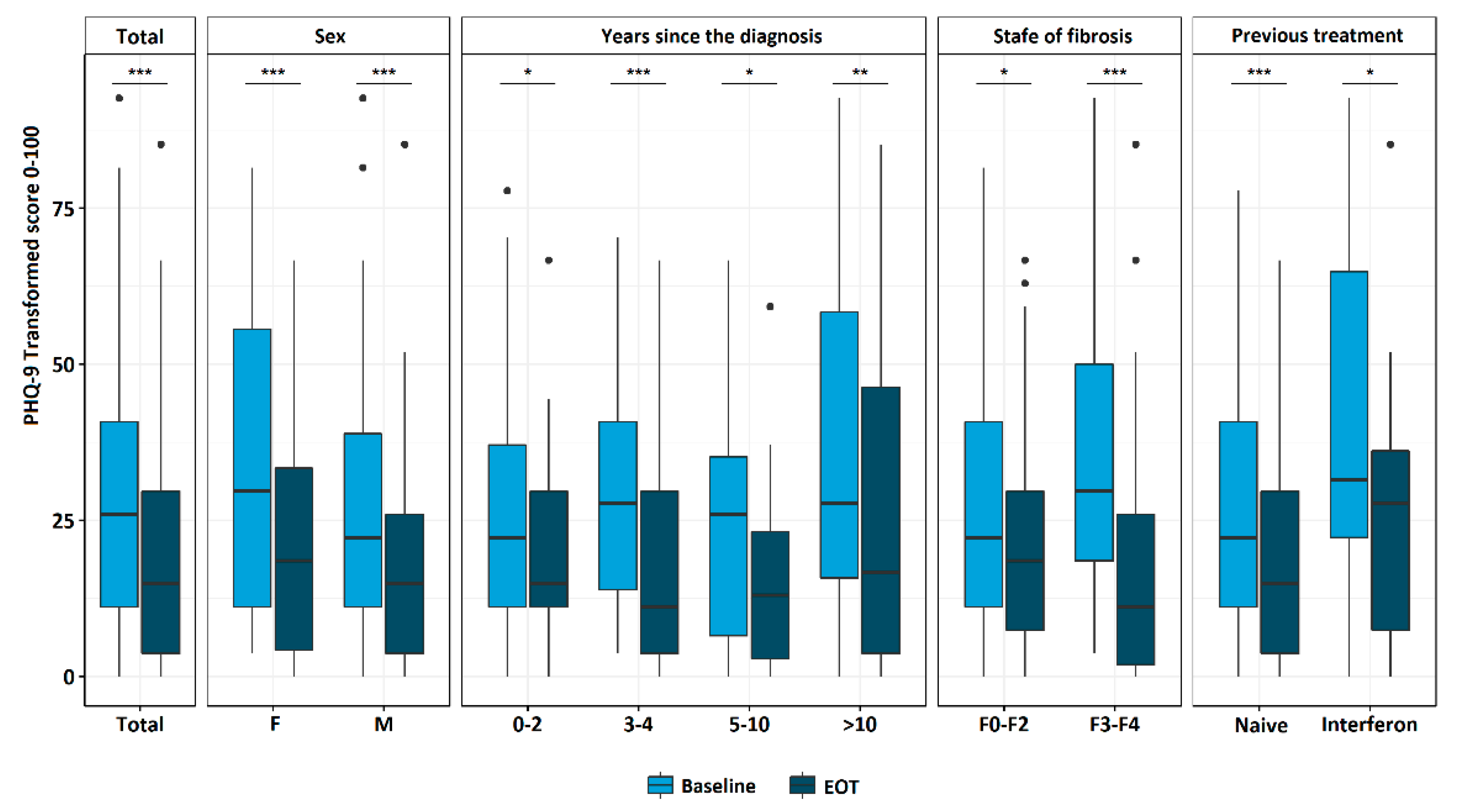
3.2.2. Depression Subgroup Analysis
3.3. Quality of Life Improvement after HCV Eradication
3.3.1. WHOQOL-BREF Results
3.3.2. HQLQ v.2 Results
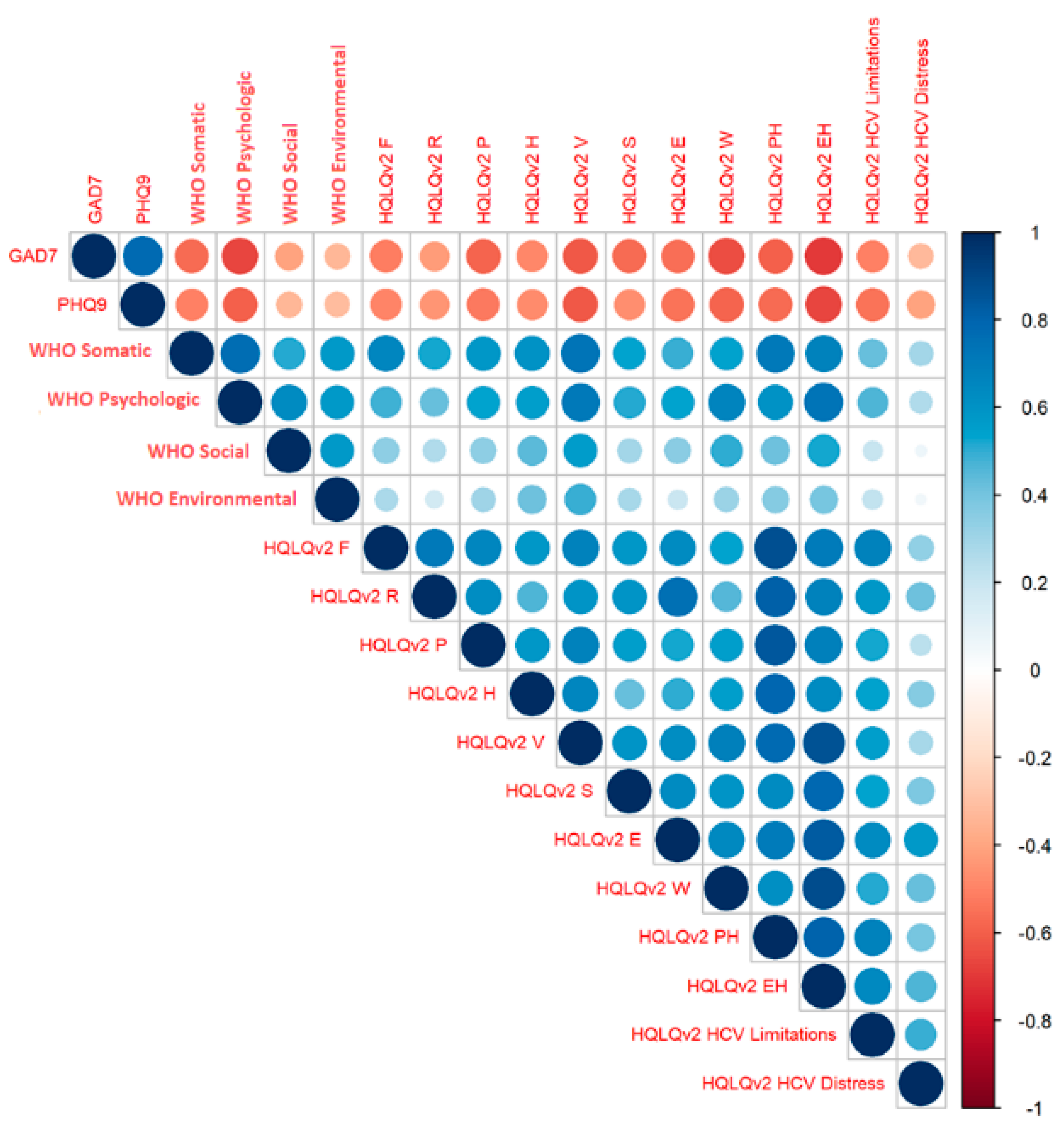
3.4. The Effects of Anxiety and Depression on Quality of Life Impairment
Correlation between Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Centre for Disease Prevention and Control. Hepatitis C. In Annual Epidemiological Report for 2019; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Chen, S.L.; Morgan, T.R. The natural history of hepatitis C virus (HCV) infection. Int. J. Med. Sci. 2006, 3, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores-Chávez, A.; Carrion, J.A.; Forns, X.; Ramos-Casals, M. Extrahepatic manifestations associated with Chronic Hepatitis C Virus Infection. Rev. Esp. Sanid. Penit. 2017, 19, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Bednarska, A.; Horban, A.; Radkowski, M. Central Nervous System as a possible site of HCV replication. Przegl. Epidemiol. 2007, 61, 739–745. [Google Scholar] [PubMed]
- Adinolfi, L.E.; Nevola, R.; Rinaldi, L.; Romano, C.; Giordano, M. Chronic Hepatitis C virus infection and depression. Clin. Liver Dis. 2017, 21, 517–534. [Google Scholar] [CrossRef] [PubMed]
- Lucaciu, L.A.; Dumitrascu, D.L. Depression and suicide ideation in chronic hepatitis C patients untreated and treated with interferon: Prevalence, prevention, and treatment. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2015, 28, 440. [Google Scholar]
- Alonso, J.; Angermeyer, M.C.; Bernert, S.; Bruffaerts, R.; Brugha, T.S.; Bryson, H.; Girolamo, G.; Graaf, R.; Demyttenaere, K.; Gasquet, I.; et al. Prevalence of mental disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand. 2004, 109, 21–27. [Google Scholar] [CrossRef]
- Kiejna, A.; Piotrowski, P.; Adamowski, T.; Moskalewicz, J.; Wciórk, J.; Stokwiszewski, J.; Rabczenko, D.; Es S Ler, R.C.K.; Kiejna, A.; Wysocki, M.J. The prevalence of common mental disorders in the population of adult poles by sex and age structure-an EZOP Poland study. Psychiatr. Pol. 2015, 49, 15–27. [Google Scholar] [CrossRef]
- Fletcher, N.F.; Yang, J.P.; Farquhar, M.J.; Hu, K.; Davis, C.; He, Q.; Dowd, K.; Ray, S.C.; Krieger, S.E.; Neyts, J.; et al. Hepatitis C Virus infection of neuroepithelioma cell lines. Gastroenterology 2010, 139, 1365–1374.e2. [Google Scholar] [CrossRef] [Green Version]
- Zacks, S.; Beavers, K.; Theodore, D.; Dougherty, K.; Batey, B.; Shumaker, J.; Galanko, J.; Shrestha, R.; Fried, M.W. Social stigmatization and hepatitis C virus infection. J. Clin. Gastroenterol. 2006, 40, 220–224. [Google Scholar] [CrossRef]
- Zickmund, S.; Ho, E.Y.; Masuda, M.; Ippolito, L.; LaBrecque, D.R. “They treated me like a leper”. Stigmatization and the quality of life of patients with hepatitis C. J. Gen. Intern. Med. 2003, 18, 835–844. [Google Scholar] [CrossRef] [Green Version]
- Golden, J.; O’Dwyer, A.M.; Conroy, R.M. Depression and anxiety in patients with hepatitis C: Prevalence, detection rates and risk factors. Gen. Hosp. Psychiatry 2005, 27, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Stepanova, M.; Nader, F.; Lam, B.; Hunt, S. The patient’s journey with chronic hepatitis C from interferon plus ribavirin to interferon- and ribavirin-free regimens: A study of health-related quality of life. Aliment. Pharmacol. Ther. 2015, 42, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Bianchi, G.; Amodio, P.; Salerno, F.; Merli, M.; Panella, C.; Loguercio, C.; Apolone, G.; Niero, M.; Abbiati, R. Factors associated with poor health-related quality of life of patients with cirrhosis. Gastroenterology 2001, 120, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Henry, L. Systematic review: Patient-reported outcomes in chronic hepatitis C—The impact of liver disease and new treatment regimens. Aliment. Pharmacol. Ther. 2015, 41, 497–520. [Google Scholar] [CrossRef] [PubMed]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Stepanova, M.; Reddy, R.; Manns, M.P.; Bourliere, M.; Gordon, S.C.; Schiff, E.; Tran, T.; Younossi, I.; Racila, A. Viral eradication is required for sustained improvement of patient-reported outcomes in patients with hepatitis C. Liver Int. 2019, 39, 54–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orley, J.D. Introduction, Administration, Scoring and Generic Version of the Assessment Field Trial Version December 1996; Programme on Mental Health World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Jaracz, K.; Kalfoss, M.; Górna, K.; Bączyk, G. Quality of life in Polish respondents: Psychometric properties of the Polish WHOQOL—Bref. Scand. J. Caring Sci. 2006, 20, 251–260. [Google Scholar] [CrossRef]
- Bayliss, M.S.; Maruish, M.E. Hepatitis Quality of Life QuestionnaireTM, (Version 2) [HQLQv2TM] Administration and Scoring Supplement; QualityMetric Incorporated: Lincoln, RI, USA, 2004. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Marcellin, F.; Roux, P.; Protopopescu, C.; Duracinsky, M.; Spire, B.; Carrieri, M.P. Patient-reported outcomes with direct-acting antivirals for the treatment of chronic hepatitis C: Current knowledge and outstanding issues. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 259–268. [Google Scholar] [CrossRef]
- Baran, R. Health-related quality of life, health state, function and wellbeing of chronic HCV patients treated with interferon-free, oral DAA regimens: Patient-reported outcome results from the AVIATOR study. NEW Evid. Virol. 2014, 3, 36–45. [Google Scholar]
- Ślusarska, B.J.; Nowicki, G.; Piasecka, H.; Zarzycka, D.; Mazur, A.; Saran, T.; Bednarek, A. Validation of the polish language version of the patient health questionnaire-9 in a population of adults aged 35–64. Ann. Agric. Environ. Med. 2019, 26, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Adinolfi, L.E.; Nevola, R.; Lus, G.; Restivo, L.; Guerrera, B.; Romano, C.; Zampino, R.; Rinaldi, L.; Sellitto, A.; Giordano, M.; et al. Chronic hepatitis C virus infection and neurological and psychiatric disorders: An overview. World J. Gastroenterol. 2015, 21, 2269. [Google Scholar] [CrossRef]
- Takeda, K.; Noguchi, R.; Namisaki, T.; Moriya, K.; Akahane, T.; Kitade, M.; Kawaratani, H.; Shimozato, N.; Kaji, K.; Takaya, H.; et al. Efficacy and tolerability of interferon-free regimen for patients with genotype-1 HCV infection. Exp. Ther. Med. 2018, 16, 2743–2750. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, J.; Rodgers, J.; Hess, E. 3435 Predicting Linkage-to-care outcomes among patients screened for Hepatitis C in an Urban Academic Emergency Department. J. Clin. Transl. Sci. 2019, 3, 124–125. [Google Scholar] [CrossRef] [Green Version]
- Barboza, K.C.; Salinas, L.M.; Sahebjam, F.; Jesudian, A.B.; Weisberg, I.L.; Sigal, S.H. Impact of depressive symptoms and hepatic encephalopathy on health-related quality of life in cirrhotic hepatitis C patients. Metab. Brain Dis. 2016, 31, 869–880. [Google Scholar] [CrossRef]
- Nardelli, S.; Riggio, O.; Rosati, D.; Gioia, S.; Ridola, L.; Farcomeni, A. Hepatitis C virus eradication with directly acting antivirals improves health-related quality of life and psychological symptoms. World J. Gastroenterol. 2019, 25, 6928–6938. [Google Scholar] [CrossRef]
- Juanbeltz, R.; Martínez-Baz, I.; San Miguel, R.; Goñi-Esarte, S.; Cabasés, J.M.; Castilla, J. Impact of successful treatment with direct-acting antiviral agents on health-related quality of life in chronic hepatitis C patients. PLoS ONE 2018, 13, e0205277. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.; Rao, H.; Shang, J.; Chen, H.; Li, J.; Xie, Q.; Gao, Z.; Wang, L.; Wei, J.; Jiang, J.; et al. A cross-sectional assessment of health-related quality of life in Chinese patients with chronic hepatitis c virus infection with EQ-5D. Health Qual. Life Outcomes 2018, 16, 124. [Google Scholar] [CrossRef] [Green Version]
- Nelson, E.; Conger, B.; Douglass, R.; Gephart, D.; Kirk, J.; Page, R.; Clark, A.; Johnson, K.; Stone, K.; Wasson, J.; et al. Functional health status levels of primary care patients. JAMA J. Am. Med. Assoc. 1983, 249, 3331–3338. [Google Scholar] [CrossRef]
- Cinar, S.; Ozdogan, O.C.; Alahdab, Y. Impact of education provided by nurses on quality of life, anxiety, and depression in patients receiving Hepatitis C virus therapy. Gastroenterol. Nurs. 2015, 38, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Zarębska-Michaluk, D.; Jaroszewicz, J.; Lorenc, B.; Klapaczyński, J.; Tudrujek-Zdunek, M.; Sitko, M.; Mazur, W.; Janczewska, E.; Pabjan, P.; et al. Changes in patient profile, treatment effectiveness, and safety during 4 years of access to interferon-free therapy for hepatitis C virus infection. Polish Arch. Intern. Med. 2020, 130, 163–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Total | Missing Data, n (%) |
|---|---|---|---|
| Age (years) (mean ± SD) | 43.8 ± 12.6 | 0 (0.0%) | |
| Sex, n (%) | Female | 45 (50.0) | 0 (0.0%) |
| Male | 45 (50.0) | 0 (0.0%) | |
| Time since diagnosis-categories (years), n (%) | 0–2 | 34 (38.2) | 1 (1.1%) |
| 3–4 | 20 (22.5) | ||
| 5–10 | 12 (13.5) | ||
| >10 | 23 (25.8) | ||
| Fibrosis-categories, n (%) | F0 | 3 (3.3) | 0 (0.0%) |
| F0/F1 | 6 (6.7) | ||
| F1 | 25 (27.8) | ||
| F1/F2 | 2 (2.2) | ||
| F2 | 21 (23.3) | ||
| F2/F3 | 5 (5.6) | ||
| F3 | 19 (21.1) | ||
| F4 | 9 (10.0) | ||
| Fibrosis-categories, n (%) | F0–F2 | 57 (63.3) | 0 (0.0%) |
| F3–F4 | 33 (36.7) | ||
| Earlier HCV treatment, n (%) | No | 75 (84.3) | 1 (1.1%) |
| Yes—interferon | 14 (15.7) |
| Variable | Baseline Summary Score | EOT Summary Score | Missing Data, n (%) | p |
|---|---|---|---|---|
| GAD-7, n | 89 | 89 | 1 (1.1%) | <0.001 |
| mean ± SD | 7.6 ± 5.1 | 5.6 ± 4.9 | ||
| median [Q1–Q3] | 6.0 [4.0, 12.0] | 5.0 [1.0, 8.0] | ||
| (min–max) | 0.0–20.0 | 0.0–21.0 | ||
| PHQ-9, n | 88 | 88 | 2 (2.2%) | <0.001 |
| mean ± SD | 8.2 ± 6.4 | 5.5 ± 5.2 | ||
| median [Q1–Q3] | 7.0 [3.0, 11.0] | 4.0 [1.0, 8.0] | ||
| (min–max) | 0.0–25.0 | 0.0–23.0 |
| WHOQOL-BREF Domain | Baseline, n = 90 | EOT, n = 90 | p | |
|---|---|---|---|---|
| somatic | median [Q1–Q3] | 60.7 [50.0, 74.1] | 71.4 [60.7, 81.2] | <0.001 |
| psychologic | median [Q1–Q3] | 70.8 [62.5, 79.2] | 75.0 [66.7, 83.3] | 0.004 |
| social | median [Q1–Q3] | 75.0 [58.3, 81.2] | 75.0 [66.7, 75.0] | 0.186 |
| environmental | median [Q1–Q3] | 65.6 [59.4, 74.2] | 71.9 [62.5, 78.1] | 0.003 |
| HQLQv.2 Domain | Baseline, Mean ± SD n = 90 | EOT, Mean ± SD n = 90 | p |
|---|---|---|---|
| F | 58.81 ± 6.61 | 59.71 ± 5.84 | 0.189 |
| R | 58.36 ± 8.36 | 59.67 ± 6.87 | 0.129 |
| P | 52.83 ± 9.02 | 55.22 ± 9.63 | 0.031 |
| H | 52.60 ± 9.07 | 55.55 ± 8.15 | <0.001 |
| V | 53.56 ± 14.09 | 58.63 ± 13.06 | 0.001 |
| S | 63.45 ± 16.58 | 68.87 ± 15.03 | 0.004 |
| E | 55.02 ± 8.37 | 57.13 ± 6.80 | 0.005 |
| W | 55.78 ± 11.84 | 58.95 ± 11.42 | 0.014 |
| PCS | 55.98 ± 6.36 | 57.32 ± 6.42 | 0.037 |
| MCS | 56.06 ± 13.27 | 60.53 ± 11.28 | 0.005 |
| HCV Limitations | 58.42 ± 12.61 | 63.10 ± 11.96 | <0.001 |
| HCV Distress | 79.62 ± 22.84 | 84.30 ± 20.46 | 0.034 |
| WHOQOL-BREF Domain | No Anxiety (<10) Mean ± SD | Anxiety (>10) Mean ± SD | p |
| somatic | 22.50 ± 2.77 | 19.00 (3.15) | <0.0001 2 |
| psychologic | 22.19 ± 2.40 | 19.89 (2.83) | 0.0062 1 |
| social | 11.71 ± 1.93 | 9.96 (2.71) | 0.0008 1 |
| environmental | 29.90 ± 3.88 | 27.22 (3.49) | 0.0029 2 |
| WHOQOL-BREF Domain | No Depression (<10) Mean ± SD | Depression (>10) Mean ± SD | p |
| somatic | 22.82 ± 2.68 | 19.03 ± 3.02 | <0.001 1 |
| psychologic | 22.26 ± 2.42 | 20.03 ± 2.80 | <0.001 1 |
| social | 11.81 ± 1.88 | 9.97 ± 2.64 | <0.000 2 |
| environmental | 30.00 ± 3.94 | 27.58 ± 3.58 | 0.004 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slonka, J.; Piotrowski, D.; Janczewska, E.; Pisula, A.; Musialik, J.; Jaroszewicz, J. Significant Decrease in the Prevalence of Anxiety and Depression after Hepatitis C Eradication. J. Clin. Med. 2022, 11, 3044. https://doi.org/10.3390/jcm11113044
Slonka J, Piotrowski D, Janczewska E, Pisula A, Musialik J, Jaroszewicz J. Significant Decrease in the Prevalence of Anxiety and Depression after Hepatitis C Eradication. Journal of Clinical Medicine. 2022; 11(11):3044. https://doi.org/10.3390/jcm11113044
Chicago/Turabian StyleSlonka, Justyna, Damian Piotrowski, Ewa Janczewska, Arkadiusz Pisula, Joanna Musialik, and Jerzy Jaroszewicz. 2022. "Significant Decrease in the Prevalence of Anxiety and Depression after Hepatitis C Eradication" Journal of Clinical Medicine 11, no. 11: 3044. https://doi.org/10.3390/jcm11113044