
Efficacy of Different Doses of Daprodustat for Anemic Non-dialysis Patients with Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis

 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Collection
2.2. Selection Criteria
2.3. Data Extraction
- Characteristics of the enrolled population at the baseline and summary of the eligible trials including study ID (last name of first author/publication year), study arms, mean age, percentage of females, mean body mass index (BMI), hemoglobin, TIBC, ferritin, transferrin saturation (TSAT), hepcidin, race, baseline epoetin alfa dose, prior diseases, baseline eGFR, stage of CKDs, inclusion and exclusion criteria of eligible studies, time of follow-up, primary endpoints, and conclusions;
- Outcomes: serum HB, ferritin, TIBC, and serum iron;
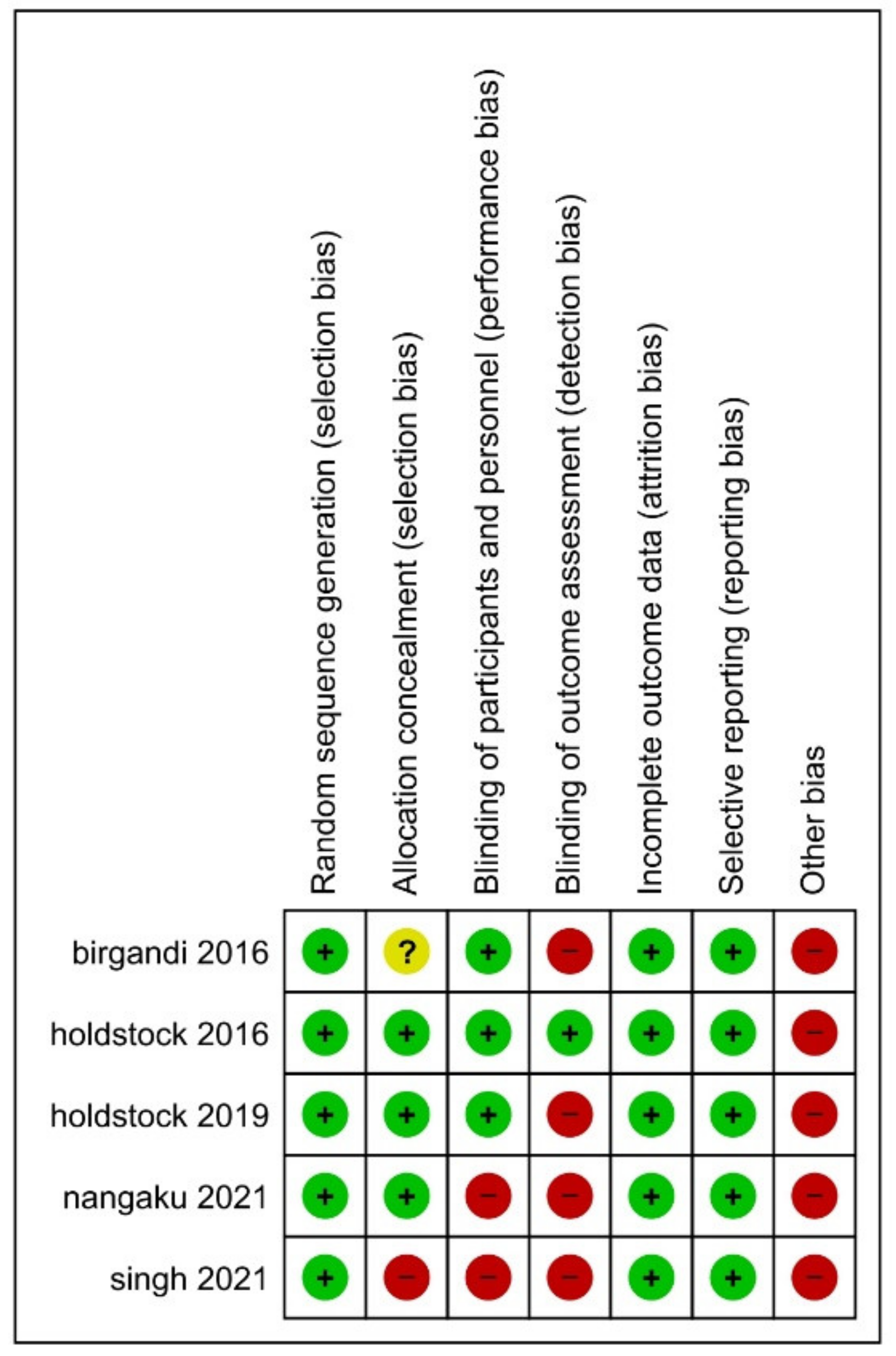
- Domains of risk of the bias assessment tool.
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Literature Search Results
3.2. Characteristics of the Enrolled Population at the Baseline and Summary of the Eligible Trials
3.3. Efficacy Outcomes
3.3.1. Serum HB
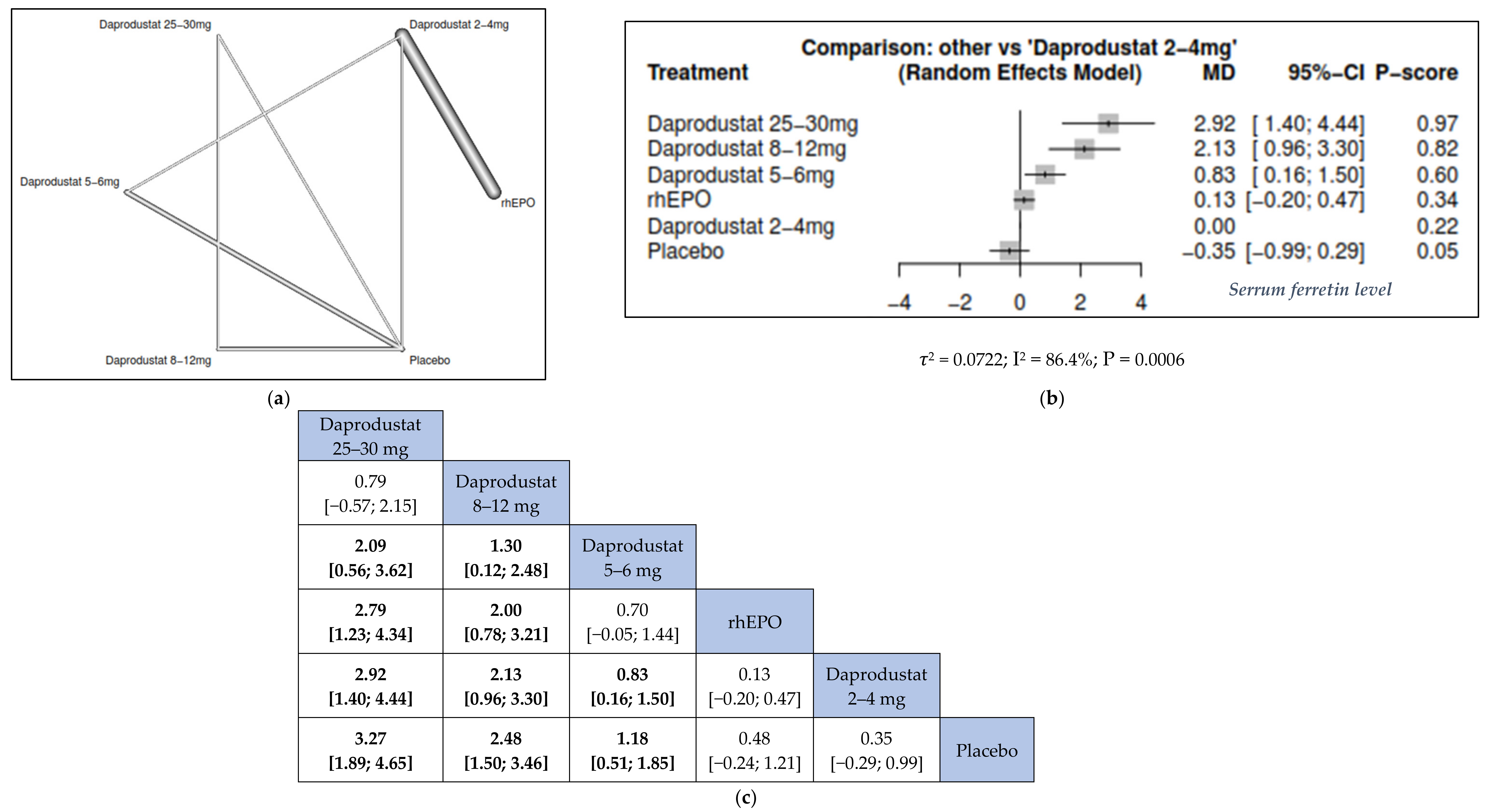
3.3.2. Serum Ferritin
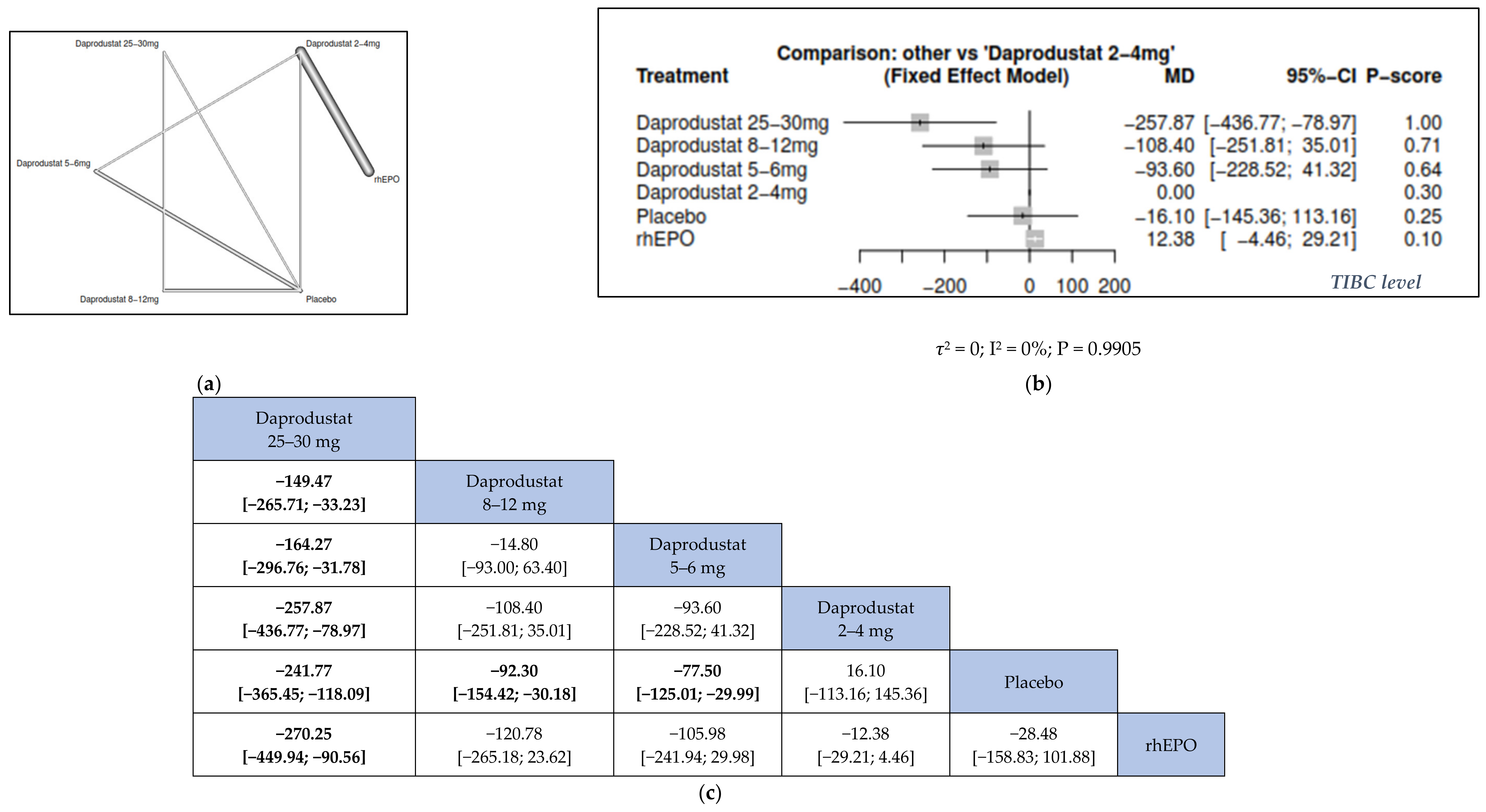
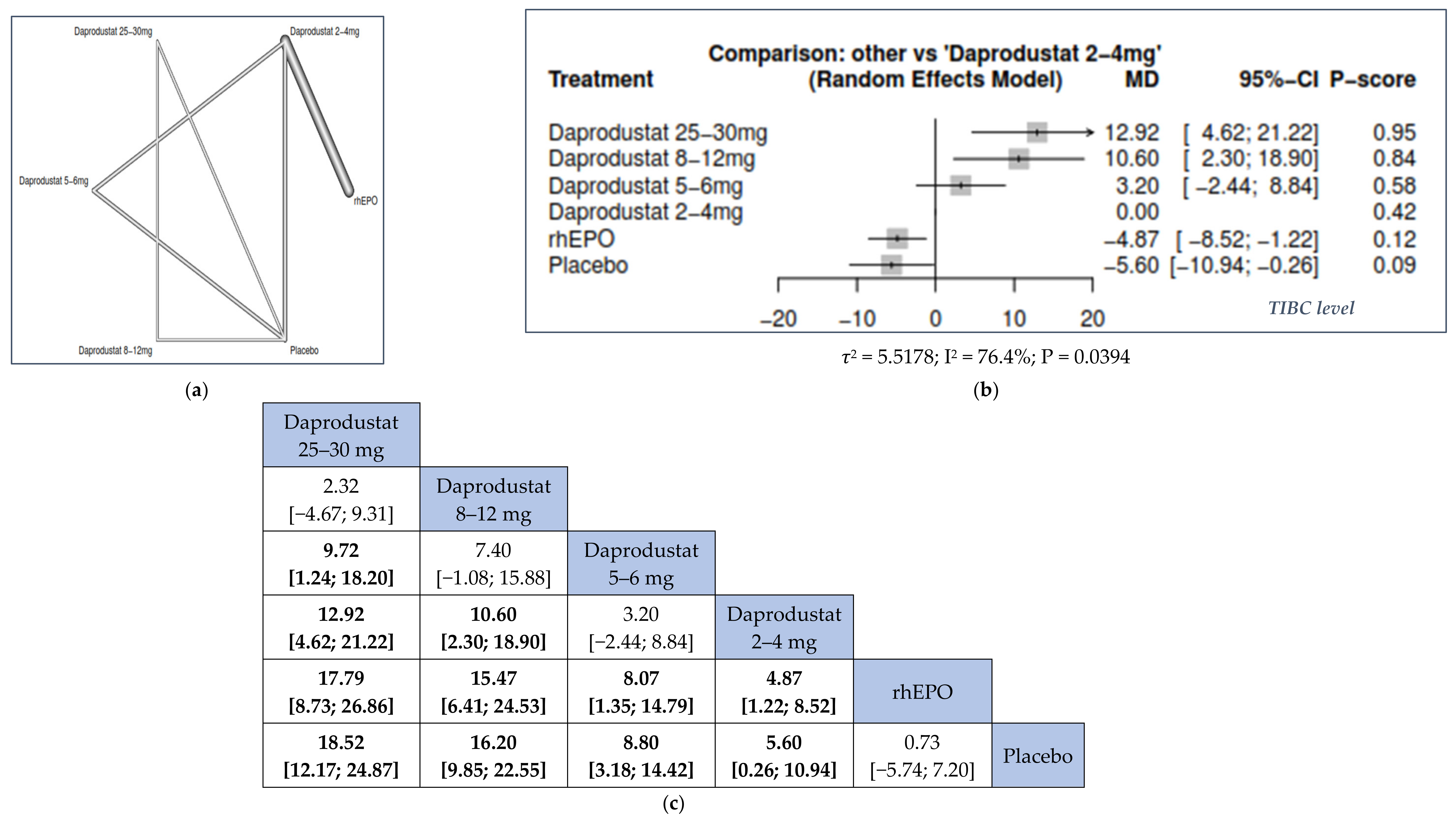
3.3.3. Total Iron-Binding Capacity (TIBC)
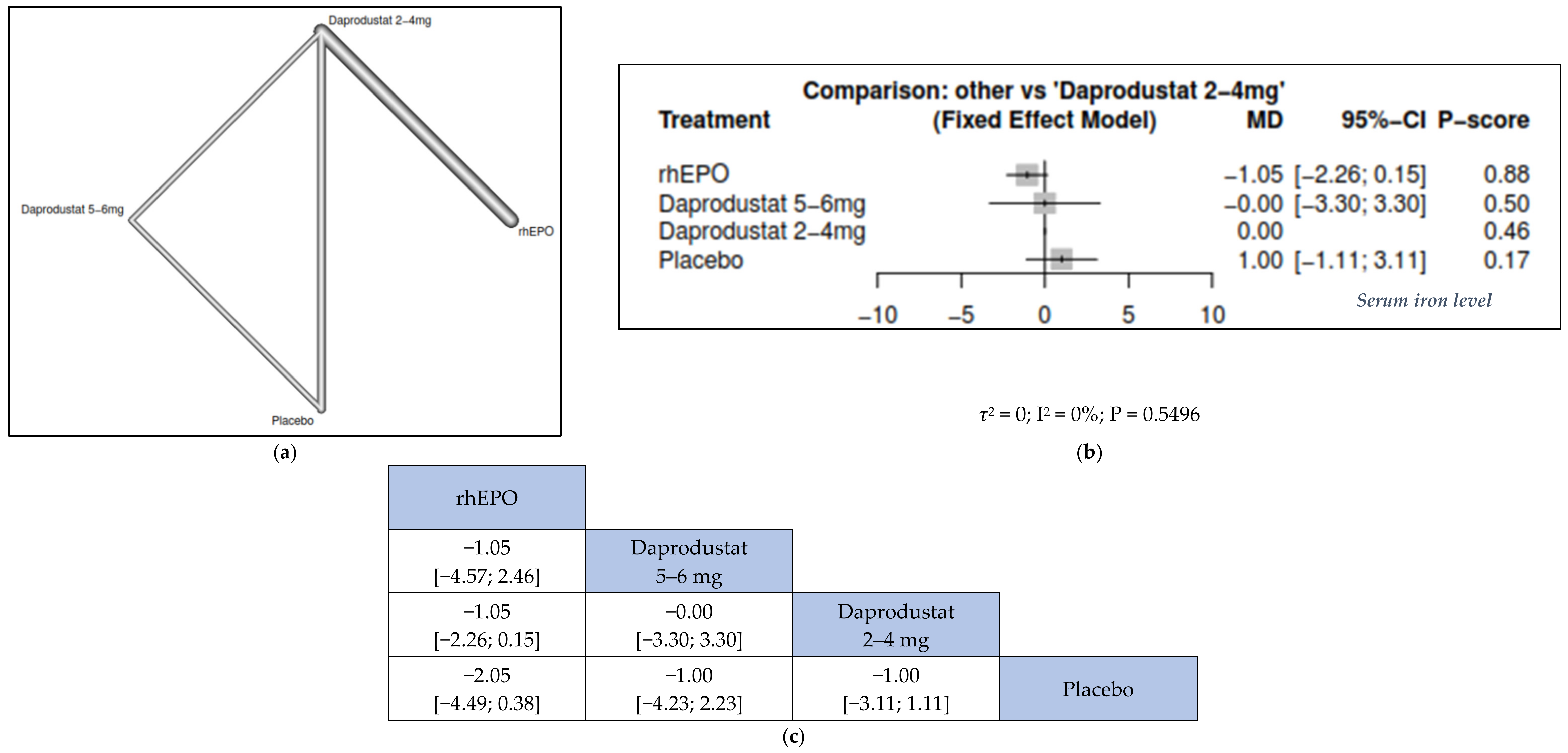
3.3.4. Serum Iron



3.3.5. Lipid Level
3.3.6. Cardiovascular (CV) Outcomes
3.4. Safety Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [CrossRef] [Green Version]
- Inker, L.A.; Grams, M.E.; Levey, A.S.; Coresh, J.; Cirillo, M.; Collins, J.F.; Gansevoort, R.T.; Gutierrez, O.M.; Hamano, T.; Heine, G.H.; et al. Relationship of Estimated GFR and Albuminuria to Concurrent Laboratory Abnormalities: An Individual Participant Data Meta-analysis in a Global Consortium. Am. J. Kidney Dis. 2019, 73, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Foreword. Kidney Int. Suppl. 2012, 2, 280. [CrossRef] [PubMed]
- Portolés, J.; Martín, L.; Broseta, J.J.; Cases, A. Anemia in Chronic Kidney Disease: From Pathophysiology and Current Treatments, to Future Agents. Front. Med. 2021, 8, 642296. [Google Scholar] [CrossRef]
- Babitt, J.L.; Lin, H.Y. Mechanisms of Anemia in CKD. J. Am. Soc. Nephrol. 2012, 23, 1631–1634. [Google Scholar] [CrossRef] [Green Version]
- Zumbrennen-Bullough, K.; Babitt, J.L. The Iron Cycle in Chronic Kidney Disease (CKD): From Genetics and Experimental Models to CKD Patients. Nephrol. Dial. Transplant. 2014, 29, 263–273. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.; Parfrey, P.; Adamson, J.W.; Aljama, P.; Berns, J.S.; Bohlius, J.; Drüeke, T.B.; Finkelstein, F.O.; Fishbane, S.; Ganz, T.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. KDIGO Clinical Practice Guide-Line for Anemia in Chronic Kidney Disease. Kidney Int. Suppl. 2012, 2, 279–335. [Google Scholar]
- Shepshelovich, D.; Rozen-Zvi, B.; Avni, T.; Gafter, U.; Gafter-Gvili, A. Intravenous Versus Oral Iron Supplementation for the Treatment of Anemia in CKD: An Updated Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2016, 68, 677–690. [Google Scholar] [CrossRef]
- Besarab, A.; Kline Bolton, W.; Browne, J.K.; Egrie, J.C.; Nissenson, A.R.; Okamoto, D.M.; Schwab, S.J.; Goodkin, D.A. The Effects of Normal as Compared with Low Hematocrit Values in Patients with Cardiac Disease Who Are Receiving Hemodialysis and Epoetin. N. Engl. J. Med. 1998, 339, 584–590. [Google Scholar] [CrossRef]
- Drüeke, T.B.; Locatelli, F.; Clyne, N.; Eckardt, K.-U.; Macdougall, I.C.; Tsakiris, D.; Burger, H.-U.; Scherhag, A. Normalization of Hemoglobin Level in Patients with Chronic Kidney Disease and Anemia. N. Engl. J. Med. 2006, 355, 2071–2084. [Google Scholar] [CrossRef] [Green Version]
- Pfeffer, M.A.; Burdmann, E.; Chen, C.-Y.; Cooper, M.E.; De Zeeuw, D.; Eckardt, K.-U.; Feyzi, J.M.; Ivanovich, P.; KewalRamani, R.; Levey, A.S.; et al. A Trial of Darbepoetin Alfa in Type 2 Diabetes and Chronic Kidney Disease. N. Engl. J. Med. 2009, 361, 2019–2032. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Szczech, L.; Tang, K.L.; Barnhart, H.; Sapp, S.; Wolfson, M.; Reddan, D. Correction of Anemia with Epoetin Alfa in Chronic Kidney Disease. N. Engl. J. Med. 2006, 355, 2085–2098. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, J.M.; Sharma, N.; Dikdan, S. Hypoxia-Inducible Factor and Its Role in the Management of Anemia in Chronic Kidney Disease. Int. J. Mol. Sci. 2018, 19, 389. [Google Scholar] [CrossRef] [Green Version]
- Sugahara, M.; Tanaka, T.; Nangaku, M. Prolyl Hydroxylase Domain Inhibitors as a Novel Therapeutic Approach against Anemia in Chronic Kidney Disease. Kidney Int. 2017, 92, 306–312. [Google Scholar] [CrossRef]
- Gupta, N.; Wish, J.B. Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitors: A Potential New Treatment for Anemia in Patients With CKD. Am. J. Kidney Dis. 2017, 69, 815–826. [Google Scholar] [CrossRef] [Green Version]
- Lee, F.S.; Percy, M.J. The HIF Pathway and Erythrocytosis. Annu. Rev. Pathol. Mech. Dis. 2011, 6, 165–192. [Google Scholar] [CrossRef]
- Provenzano, R.; Besarab, A.; Sun, C.H.; Diamond, S.A.; Durham, J.H.; Cangiano, J.L.; Aiello, J.R.; Novak, J.E.; Lee, T.; Leong, R.; et al. Oral Hypoxia–Inducible Factor Prolyl Hydroxylase Inhibitor Roxadustat (FG-4592) for the Treatment of Anemia in Patients with CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 982–991. [Google Scholar] [CrossRef]
- Mastrogiannaki, M.; Matak, P.; Keith, B.; Simon, M.C.; Vaulont, S.; Peyssonnaux, C. HIF-2α, but not HIF-1α, Promotes Iron Absorption in Mice. J. Clin. Investig. 2009, 119, 1159–1166. [Google Scholar] [CrossRef]
- Ding, H.; Yan, C.-Z.; Shi, H.; Zhao, Y.-S.; Chang, S.-Y.; Yu, P.; Wu, W.-S.; Zhao, C.-Y.; Chang, Y.-Z.; Duan, X.-L. Hepcidin Is Involved in Iron Regulation in the Ischemic Brain. PLoS ONE 2011, 6, e25324. [Google Scholar] [CrossRef] [Green Version]
- Holdstock, L.; Meadowcroft, A.M.; Maier, R.; Johnson, B.M.; Jones, D.; Rastogi, A.; Zeig, S.; Lepore, J.J.; Cobitz, A.R. Four-Week Studies of Oral Hypoxia-Inducible Factor–Prolyl Hydroxylase Inhibitor GSK1278863 for Treatment of Anemia. J. Am. Soc. Nephrol. 2016, 27, 1234–1244. [Google Scholar] [CrossRef]
- Lenihan, C.R.; Winkelmayer, W.C. The Dawning of a New Day in CKD Anemia Care? J. Am. Soc. Nephrol. 2016, 27, 968–970. [Google Scholar] [CrossRef]
- Zheng, Q.; Wang, Y.; Yang, H.; Sun, L.; Fu, X.; Wei, R.; Liu, Y.N.; Liu, W.J. Efficacy and Safety of Daprodustat for Anemia Therapy in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2021, 11, 573645. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Boutron, I.; Page, M.J.; Higgins, J.P.T.; Altman, D.G.; Lundh, A.; Hróbjartsson, A. Chapter 7: Considering Bias and Conflicts of Interest Among the Included Studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 9 March 2022).
- Brigandi, R.A.; Johnson, B.; Oei, C.; Westerman, M.; Olbina, G.; de Zoysa, J.; Roger, S.D.; Sahay, M.; Cross, N.; McMahon, L.; et al. A Novel Hypoxia-Inducible Factor-Prolyl Hydroxylase Inhibitor (GSK1278863) for Anemia in CKD: A 28-Day, Phase 2A Randomized Trial. Am. J. Kidney. Dis. 2016, 67, 861–871. [Google Scholar] [CrossRef] [Green Version]
- Holdstock, L.; Cizman, B.; Meadowcroft, A.M.; Biswas, N.; Johnson, B.M.; Jones, D.; Kim, S.G.; Zeig, S.; Lepore, J.J.; Cobitz, A.R. Daprodustat for Anemia: A 24-Week, Open-Label, Randomized Controlled Trial in Participants with Chronic Kidney Disease. Clin. Kidney J. 2019, 12, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.K.; Carroll, K.; McMurray, J.J.; Solomon, S.; Jha, V.; Johansen, K.L.; Lopes, R.D.; Macdougall, I.C.; Obrador, G.T.; Waikar, S.S.; et al. Daprodustat for the Treatment of Anemia in Patients Not Undergoing Dialysis. N. Engl. J. Med. 2021, 385, 2313–2324. [Google Scholar] [CrossRef] [PubMed]
- Nangaku, M.; Hamano, T.; Akizawa, T.; Tsubakihara, Y.; Nagai, R.; Okuda, N.; Kurata, K.; Nagakubo, T.; Jones, N.P.; Endo, Y.; et al. Daprodustat Compared with Epoetin Beta Pegol for Anemia in Japanese Patients Not on Dialysis: A 52-Week Randomized Open-Label Phase 3 Trial. Am. J. Nephrol. 2021, 52, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.M.; Stier, B.A.; Caltabiano, S. Effect of Food and Gemfibrozil on the Pharmacokinetics of the Novel Prolyl hy-droxylase Inhibitor GSK1278863. Clin. Pharmacol. Drug Dev. 2014, 3, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Ariazi, J.L.; Duffy, K.J.; Adams, D.F.; Fitch, D.M.; Luo, L.; Pappalardi, M.; Biju, M.; DiFilippo, E.H.; Shaw, T.; Wiggall, K.; et al. Discovery and Preclinical Characterization of GSK1278863 (Daprodustat), a Small Molecule Hypoxia In-ducible Factor-Prolyl Hydroxylase Inhibitor for Anemia. J. Pharmacol. Exp. Ther. 2017, 363, 336–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratcliffe, P.J. HIF-1 and HIF-2: Working Alone or Together in Hypoxia? J. Clin. Investig. 2007, 117, 862–865. [Google Scholar] [CrossRef] [Green Version]
- Kapitsinou, P.P.; Liu, Q.; Unger, T.L.; Rha, J.; Davidoff, O.; Keith, B.; Epstein, J.A.; Moores, S.L.; Erickson-Miller, C.L.; Haase, V.H. Hepatic HIF-2 Regulates Erythropoietic Responses to Hypoxia in Renal Anemia. Blood 2010, 116, 3039–3048. [Google Scholar] [CrossRef] [Green Version]
- Goel, H.L.; Mercurio, A.M. VEGF Targets the Tumour Cell. Nat. Cancer 2013, 13, 871–882. [Google Scholar] [CrossRef]
- Fogli, S.; Mogavero, S.; Egan, C.G.; Del Re, M.; Danesi, R. Pathophysiology and Pharmacological Targets of VEGF in Diabetic Macular Edema. Pharmacol. Res. 2016, 103, 149–157. [Google Scholar] [CrossRef]
- Tsubakihara, Y.; Akizawa, T.; Nangaku, M.; Onoue, T.; Yonekawa, T.; Matsushita, H.; Endo, Y.; Cobitz, A. A 24-Week Anemia Correction Study of Daprodustat in Japanese Dialysis Patients. Ther. Apher. Dial. 2020, 24, 108–114. [Google Scholar] [CrossRef]
- Akizawa, T.; Tsubakihara, Y.; Nangaku, M.; Endo, Y.; Nakajima, H.; Kohno, T.; Imai, Y.; Kawase, N.; Hara, K.; Lepore, J.; et al. Effects of Daprodustat, a Novel Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor on Anemia Man-agement in Japanese Hemodialysis Subjects. Am. J. Nephrol. 2017, 45, 127–135. [Google Scholar] [CrossRef]
- Meadowcroft, A.M.; Cizman, B.; Holdstock, L.; Biswas, N.; Johnson, B.M.; Jones, D.; NKaldun Nossuli, A.; Lepore, J.J.; Aarup, M.; Cobitz, A.R. Daprodustat for Anemia: A 24-Week, Open-Label, Randomized Controlled Trial in Participants on Hemodialysis. Clin. Kidney J. 2019, 12, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Provenzano, G.; Corradi, Z.; Monsorno, K.; Fedrizzi, T.; Ricceri, L.; Scattoni, M.L.; Bozzi, Y. Comparative Gene Expression Analysis of Two Mouse Models of Autism: Transcriptome Profiling of the BTBR and En2−/− Hippocampus. Front. Neurosci. 2016, 10, 396. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Zhou, X.J. Potential Mechanisms of Adverse Outcomes in Trials of Anemia Correction with Erythropoietin in Chronic Kidney Disease. Nephrol. Dial. Transplant. 2009, 24, 1082–1088. [Google Scholar] [CrossRef] [Green Version]
- McCullough, P.A.; Barnhart, H.X.; Inrig, J.K.; Reddan, D.; Sapp, S.; Patel, U.D.; Singh, A.K.; Szczech, L.A.; Califf, R.M. Cardiovascular Toxicity of Epoetin-Alfa in Patients with Chronic Kidney Disease. Am. J. Nephrol. 2013, 37, 549–558. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fadlalmola, H.; Al-Sayaghi, K.; Al-Hebshi, A.; Aljohani, M.; Albalawi, M.; Kashari, O.; Alem, A.; Alrasheedy, M.; Balelah, S.; Almuteri, F.; et al. Efficacy of Different Doses of Daprodustat for Anemic Non-dialysis Patients with Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2022, 11, 2722. https://doi.org/10.3390/jcm11102722
Fadlalmola H, Al-Sayaghi K, Al-Hebshi A, Aljohani M, Albalawi M, Kashari O, Alem A, Alrasheedy M, Balelah S, Almuteri F, et al. Efficacy of Different Doses of Daprodustat for Anemic Non-dialysis Patients with Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis. Journal of Clinical Medicine. 2022; 11(10):2722. https://doi.org/10.3390/jcm11102722
Chicago/Turabian StyleFadlalmola, Hammad, Khaled Al-Sayaghi, Abdulqader Al-Hebshi, Maher Aljohani, Mohammed Albalawi, Ohoud Kashari, Alaa Alem, Mariam Alrasheedy, Saud Balelah, Faten Almuteri, and et al. 2022. "Efficacy of Different Doses of Daprodustat for Anemic Non-dialysis Patients with Chronic Kidney Disease: A Systematic Review and Network Meta-Analysis" Journal of Clinical Medicine 11, no. 10: 2722. https://doi.org/10.3390/jcm11102722