1. Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide, and acute myocardial infarction (MI) is the most outstanding result [
1]. Atherosclerosis is the main pathogenic feature behind these diseases and is considered an inflammatory process [
2]. Inflammation is a defense reaction to the aggression of microorganisms such as bacteria, physical insults or chemical products. Periodontitis (PER) is an infectious inflammatory disease caused by an interaction between host responses and microbial dysbiosis that results in a loss of alveolar bone loss and can lead to tooth loss if left untreated [
3]. Observational studies support an association between periodontitis and cardiovascular disease [
4,
5,
6]. However, other studies have shown controversial results [
7,
8], which could impact public health policies if new risk factors for MI are identified. PER is associated with multiple bacterial species, mainly
Bacteroidetes, and, more specifically, with the genera
Porphyromonas,
Prevotella,
Tannerella and
Capnocytophaga. These bacteria are involved in the development of atherosclerosis in animals [
9] and are associated with symptomatic atherosclerosis [
10] and its markers [
11] in humans. We must emphasize the importance of the oral cavity in systemic diseases, as it is part of the digestive tract and the high level of interindividual contamination through mouth-to-mouth contact [
12]. In the past few decades, incredible efforts have been made to improve our knowledge of the risk factors associated with MI. However, the pathogenic mechanisms involved in the development of atherosclerosis remain unclear. One of the most important methods to prevent MI and one of the most effective strategies to perform this is to control cardiovascular risk factors [
13]. Some data show that there are differences related to sex/gender in coronary artery disease, and specific risk factors have been identified [
14,
15,
16]. Exposure to risk factors is very common among patients who have developed CVD, but exposure to the same risk factors is also very prevalent among people who have not developed coronary heart disease [
17].
Treatment of MI has high-level time-critical conditions; the earlier patients have access to treatment, the higher the chances of survival. After the acute phase, to prevent a new event, secondary prevention remains essential. The adequate management of risk factors has successfully improved prognosis after MI. However, despite this progress, there is still a need to find innovative methods to maximize secondary prevention and to find any risk factors that could precede them [
18]. Our goals were (1) to identify risk factors associated with MI in men with and without periodontitis and (2) to investigate which risk factors influence the prognosis of the progression of MI.
2. Materials and Methods
2.1. Study Participants
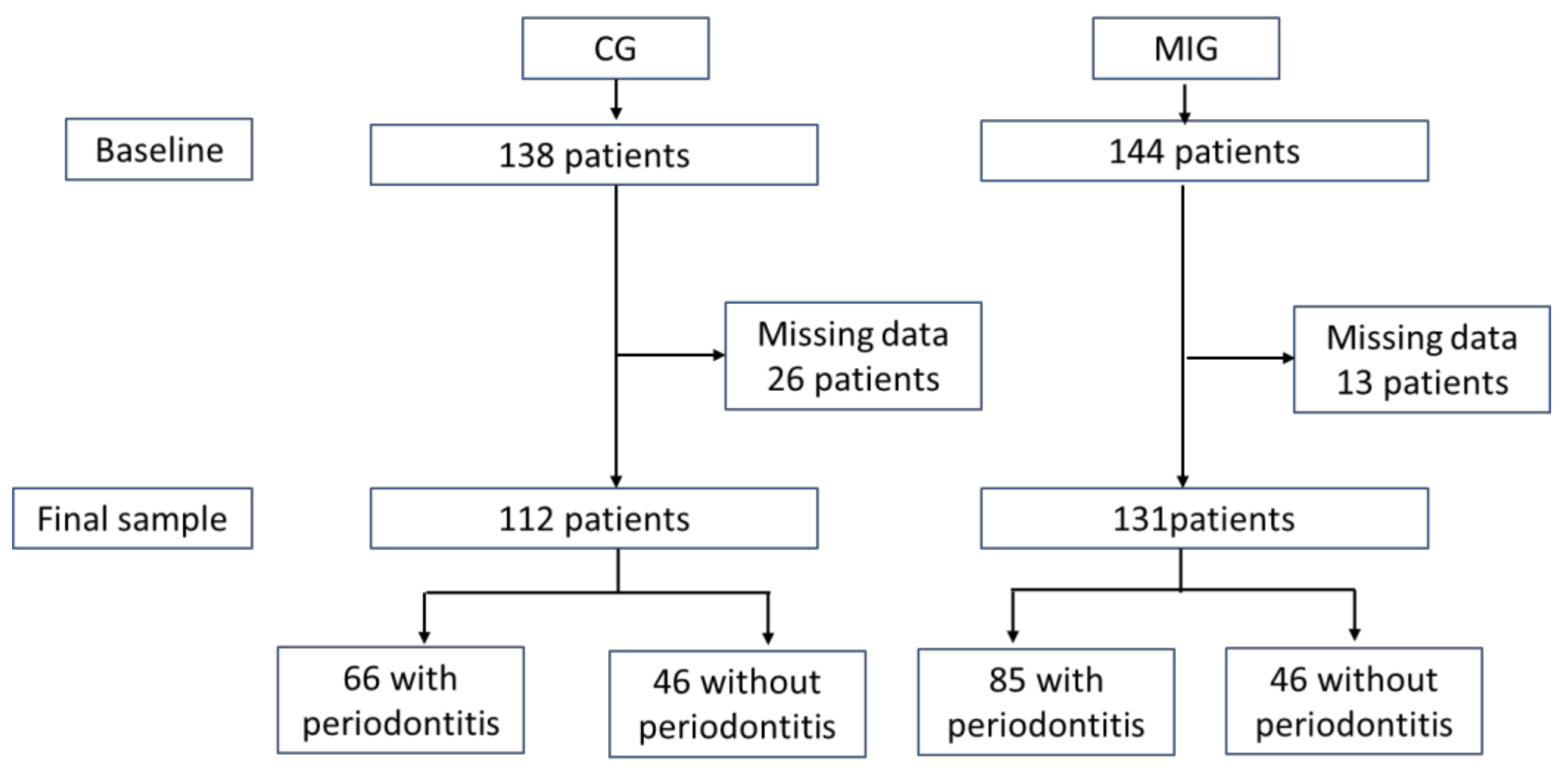
The test group (MIG) consisted of male patients who had a first episode of MI in the previous 48 h who attended the University Hospital, Sevilla, from February 2017 to February 2019. During the same period, the control group (CG) was recruited from male patients attending at the School of Dentistry of the University of Seville without a history of MI. Both groups were asked to participate in the study and signed an informed consent form. The protocol was approved by the Ethics Committee of the same hospital (1588-N-20, 21 December 2016). Both groups were divided into two other groups according to the presence or absence of PER. PER were diagnosed according to the stage III and IV definition of the 2017 World Workshop on Classification of Periodontal and Peri-Implant Diseases and Condition [
19]: clinical attachment level ≥ 5 mm at 2 ≥ sites in ≥ 2 non-adjacent teeth. Severe PER was defined as 30% tooth with probing depth ≥ 4 at 2 ≥ interproximal sites. Furthermore, the number of sites with a clinical attachment level ≥ 5 mm and the number of teeth were recorded. MIG was followed for at least two years.
The sample size was obtained considering the combination of two dichotomous variables: cardiovascular (yes/no) and PER (yes/no) and with the means of data for the clinical attachment level (CAL) (0.01, 0.27 and 0.07) and the main quantitative variables of the groups (0.4). A minimum sample size of 43 patients was obtained when the values were established at 5% and the power at 90% (for factor A: CVD) and 99% (for factor B: PER) and for interaction.
2.2. Clinical Data
General data were recorded: age, height, weight, body mass index (BMI), abdominal waist circumference and smoking status. We consider a smoker as someone who smoked at least one cigarette per day and nonsmokers as those who do not currently smoke.
2.3. Dietary Assessment
The Mediterranean Diet Adherence Screener (MDA) [
20] was used. It consists of 12 questions on frequency of food consumption and 2 questions on food intake habits considered characteristic of the Spanish Mediterranean diet. Each question was scored 0 or 1. The final MAD score ranged from 0 to 14 and was classified as Very low (range), Low, High and Very high.
2.4. Physical Activity
Based on Minnesota Leisure Time Physical Activity [
21], we asked for the hours spent on walking, any sport, household activity and other physical activity per week and obtained the average weekly exercise hours.
2.5. Oral Examination
A calibrated explorer (PB) recorded the depth of the probing pocket at six sites per tooth as the distance between the gingival margin and the bottom of the pocket and the level of clinical attachment as the distance between the cemento–enamel junction and the bottom of the pocket. Bleeding on probing was also recorded after 10 s [
22] at four sites around each tooth.
2.6. Biochemical Parameters
In CG, venous blood samples were obtained after a fasting period and in MIG within 48 h after the acute episode in the routine cardiac control. The following biochemical parameters were obtained: fasting glycemia, urea, creatinine, uric acid, GPT, GGT, cholesterol, triglycerides, HDL, LDL, VLDL, total cholesterol/HDL index, albumin, total bilirubin, phosphorus, calcium, HbA1c, TSH, iron, cortisol and CRP for all patients and high sensitivity troponine-1 and alkaline phosphatase for cardiac patients using routine analytical methods.
2.7. Microbiological Sample
In each patient, the three deepest periodontal pockets were selected. After the removal of the supragingival plaque and isolation of the area, paper points were inserted into the gingival sulcus for 30 s. The samples were pooled, stored in Eppendorfs and immediately processed. DNA was extracted in 24 h using the High Pure PCR Template Preparation Kit (Roche, Mannheim, Germany) and divided into aliquots for the microIDent PCR test (Hain Lifescience, Nehren, Germany). DNA-STRIP technology was used to record the species of Porphyromonas gingivalis (Pg), Tannerella forsythia (Tf), Treponema denticola (Td), Prevotella intermedia (Pi) and Aggregatibacter actinomycetemcomitans (Aa), as previously described. For the determination of analytical sensitivity, a series of plasmid dilutions was used containing target sequences detectable with micro-IDent®plus11. The following detection limits were determined: Aa specie: 50–100 genome equivalents/PCR or 1000–5000 genome equivalents/paper point; all other species: 500–1000 genome equivalents/PCR or 10,000–50,000 genome equivalents/paper point. The results were classified into 5 groups according to bioburden: not detectable (<104, Aa < 103), within the limit (104, Aa 103), increased (<105, Aa < 104), high (<106, Aa < 105) and very high (≥106, Aa ≥ 105).
2.8. Cardiological Parameters
At baseline, the following cardiovascular risk factors were recorded in MIG: Previous history of hypertension, diabetes mellitus, dyslipidemia, smoking and history of ischemic cardiopathy. The left ventricular ejection fraction (LVEF) was visually estimated by agreement between two observers and categorized into 4 groups: preserved > 50%, slightly reduced 40–49%, moderately reduced 31–40% and severe < 30%. Platelet antiaggregant therapy: Clopidogrel, Prasugrel and Ticagrelor. Type of acute coronary syndrome that differentiates ST elevation. Location of coronary obstruction. Number of coronary vessels affected with severe stenosis, dividing them into ≤two and >three affected vessels. The patients were followed until February 2020, and the following parameters were recorded: LVEF, major adverse cardiac events (MACE) and death. MACE is defined as a composite of nonfatal MI nonfatal stroke, repeated revascularization or admission due to a cardiovascular event [
23].
2.9. Statistical Analysis
SPSS 25.0 software (IBM, Armonk, NY, USA) was used for statistical analyzes. Descriptive statistics included means, standard deviations, medians, quartiles and percentages. The normal distribution of the quantitative data was verified using the Kolmogorov–Smirnov test. The statistical ANOVA test for parametric distribution and the Mann–Whitney U and Kruskal–Wallis tests for the nonparametric distribution were used. The post hoc test utilized for the parametric distribution was Student’s t test with the previous Levine test on the homogeneity of variances, and for nonparametric distribution, the Mann–Whitney U test was used. Categorical variables were analyzed with a chi-square test to determine the groups that make a difference, and the standardized residuals were corrected according to the Haberman method. Values of p < 0.05 were considered statistically significant. Binary logistic regression analysis was used to estimate the association between different variables and the risk of MI and MACE at follow-up. We used logistic regression analysis to model the probability of an event occurring based on other factors. It includes the Backward LR method that considers all confounding variables. It starts from all variables that, in the two-by-two crosses, have shown a relationship with the variable to be estimated; the method is step-by-step exclusion, eliminating in each iteration the variable for which its relationship with the one to be estimated presents less significance until only the most relevant is left.
4. Discussion
Our results show that periodontitis is related to MI, as demonstrated in the literature [
24,
25,
26]. Furthermore, another main finding of this study is that periodontitis should be considered as a risk factor in MI follow-up, such as Eppendorf. In MIG, we found no differences in cardiovascular risk factors between periodontitis patients and no periodontitis patients including hypertension, diabetes mellitus, dyslipidemia and smoking. These risk factors are the most prevalent in some published studies [
27,
28]. In addition, other risk factors such as waist circumference and HbA1c are not different between the groups. Therefore, our data highlight that patients with those same systemic conditions could have another risk factor, such as PER. Some authors show that CVD patients do not have any of the classic risk factors and 60% of them have not experienced MI [
29]. We agree with some authors who propose an inflammatory genetic component in coronary artery disease [
30]; our data suggest that one of the infectious diseases that can stimulate the inflammatory statement is periodontitis through oral bacteria.
The percentages of cardiac variables are not statistically different between MIGNOPER and MIGPER. In the MIG follow-up, the only variable that had statistical differences between MIGPER and MIGNOPER is LVEF. LVEF is one of the most important parameters for verifying the functional statement of cardiac function, so it is very important for the prognosis of patients with MI to consider all factors that could influence it. The number of MACE and two types of MACE, non-fatal MI and admission due to CV events, was high in MIGPER but not statistically different. These data reveal a worse recovery after the acute event, which could be explained by more severe periodontal conditions. We must note that MIGs were followed for at least one year and patients, due to cardiac conditions, were not treated for PER. We can conclude that PER can alter cardiac recovery and influences left ventricular remodeling and future cardiac events.
When we analyzed the results of binary logistic regression, a strong association was observed between average weekly exercise hours, MDA and smoking in MI patients. The binary logistic regression analysis shows an association between PER, weight, average weekly exercise hours, dyslipidemia and MACE. Therefore, the number of teeth and PER, which indicate unhealthy periodontal conditions, are part of factors that can be related to MI and affect cardiac evolution. Missing teeth is associated with an increased risk of MI and discriminates patients with high cardiovascular risk [
31]; low physical activity with an inadequate diet that produces a metabolic syndrome is associated with a high risk of major adverse cardiovascular events [
32]. Furthermore, exercise-based cardiac rehabilitation is essential in cardiac patients’ recovery of cardiac patients [
33]; a recent cohort study tried to associate the impact of periodontitis and subgingival bacteria on recurrent CVD events such as MI, stroke and death caused by CVD. The results cannot show an association between the periodontal bacteria that we have studied, although an association between periodontitis and more CVD events is shown. [
34].
The relationship between MI and PER has been extensively studied. A recent meta-analysis of cohort studies indicates that PD is modestly associated with the risk of MI, especially in women [
24]. In a 13-year prospective study, severe PER was shown to be associated with an increased incidence of coronary heart disease regardless of the established cardiovascular risk factors [
35]. A review reports on the proceedings of the workshop jointly organized by the EFP and the World Heart Federation (WHF). They concluded that there is epidemiological evidence for significant associations between periodontitis and CVD and recommended that dentists, physicians and patients visit dental and medical practices [
36].
The general characteristics of the patients show that the most important factor that can distinguish the different conditions is physical activity and a healthy diet and not the anthropometric variables. We have to consider that we usually have a hypercaloric diet in our countries that results in a specific weight; our results show that the more important factors are the dietary components and their consumption. Various diet indices have shown that unhealthy eating patterns are associated with severe PER [
37,
38] and others are associated only with obese men [
39]. Mediterranean components such as salads, fruits and vegetables were associated with a lower level of clinical attachment level [
40], and MDA produces a significant decrease in the saliva levels of
Pg,
Pi and
Tp [
41]. Physical activity has been associated with PER in general populations [
42,
43] and can improve periodontal health in patients with T2 diabetes mellitus [
44] and obese women [
45]. The Mediterranean diet and moderate physical activity are some of the most important recommendations for the primary prevention of CVD [
46]. Smoking has been considered a common risk factor for PER and cardiovascular disease [
47] and we show that the proportion of current smokers was high in MIG. The number of teeth has the lowest value in MIGPER, indicating that both conditions have an increasing effect, this result is in agreement with previous data that can discriminate patients with a high risk of MI [
31].
We show that the number of leukocytes was high in both MIGs, as previously reported [
48]. An association of leukocyte counts and systemic inflammation was demonstrated in patients with PD [
49]. Our data show that the number of monocytes is low in both MIGs. This could be explained by the margination of monocytes to the coronary vasculature shown in patients after coronary artery reperfusion, which could potentially contribute to the drop in circulating monocytes [
50].
Some of the biochemical parameters show differences between MIG and CG as consequences of MI conditions, but they cannot differentiate if they suffer from PER or NOPER. CRP is the only variable that increases in MIGPER that demonstrates the possible summation effects of cardiac and periodontal conditions. CRP is synthesized by the liver in response to any type of infection and is mainly stimulated by interleukin-6. It is a short pentatrexin, a multimeric pattern recognition protein that is considered a relatively moderate predictor of coronary heart disease [
51], but CRP is also a strong predictor of cardiovascular mortality during the year after an MI event [
52]. As we discuss below, our patients with PER suffered more MACE and worse LVEF at follow-up.
Our microbiological results show lower values for
Pg,
Tf,
Td and
Pi in CGNOPER and similar high figures in both MIG and CGPER. Therefore, cardiac patients have gingival microbiota compatible with periodontopathogen bacteria.
Pg and
Tf, the main periodontopathogen bacteria related to PER, are present in large numbers in MIGNOPER, so they are not related to periodontal conditions. We can deduce some deleterious effects on cardiovascular conditions. This aspect agrees with previous data. The presence of all these bacteria was detected in subgingival samples of cardiovascular patients who required endarterectomy [
53,
54]. One of them,
Pg, has been associated with the development of atherosclerosis in animal models [
55]. The oral microbiota is part of the digestive tract and is related to the gut microbiota. Research in animals shows that oral
Pg infection disrupts oral and cecal microbiomes, altering their community membership and functional potential [
56].
Our study has some limitations. Our patients are Spanish; share specific diet, environmental and cultural characteristics that are different from other populations; and the results should be evaluated based on these issues. We studied only male patients and the results cannot apply to women. The patients with MIG were explored 48 h after suffering from an MI, so they are patients who survived and had a cardiac recovery; we cannot explore those who did not survive and perhaps they had the worst cardiac conditions.


 ,
, 

{kind=link}