
Fatigue and Associated Factors in an Immune-Mediated Inflammatory Disease Population: A Cross-Sectional Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethics Approval
2.3. Instruments
2.4. Data Analysis
3. Results
3.1. Study Population
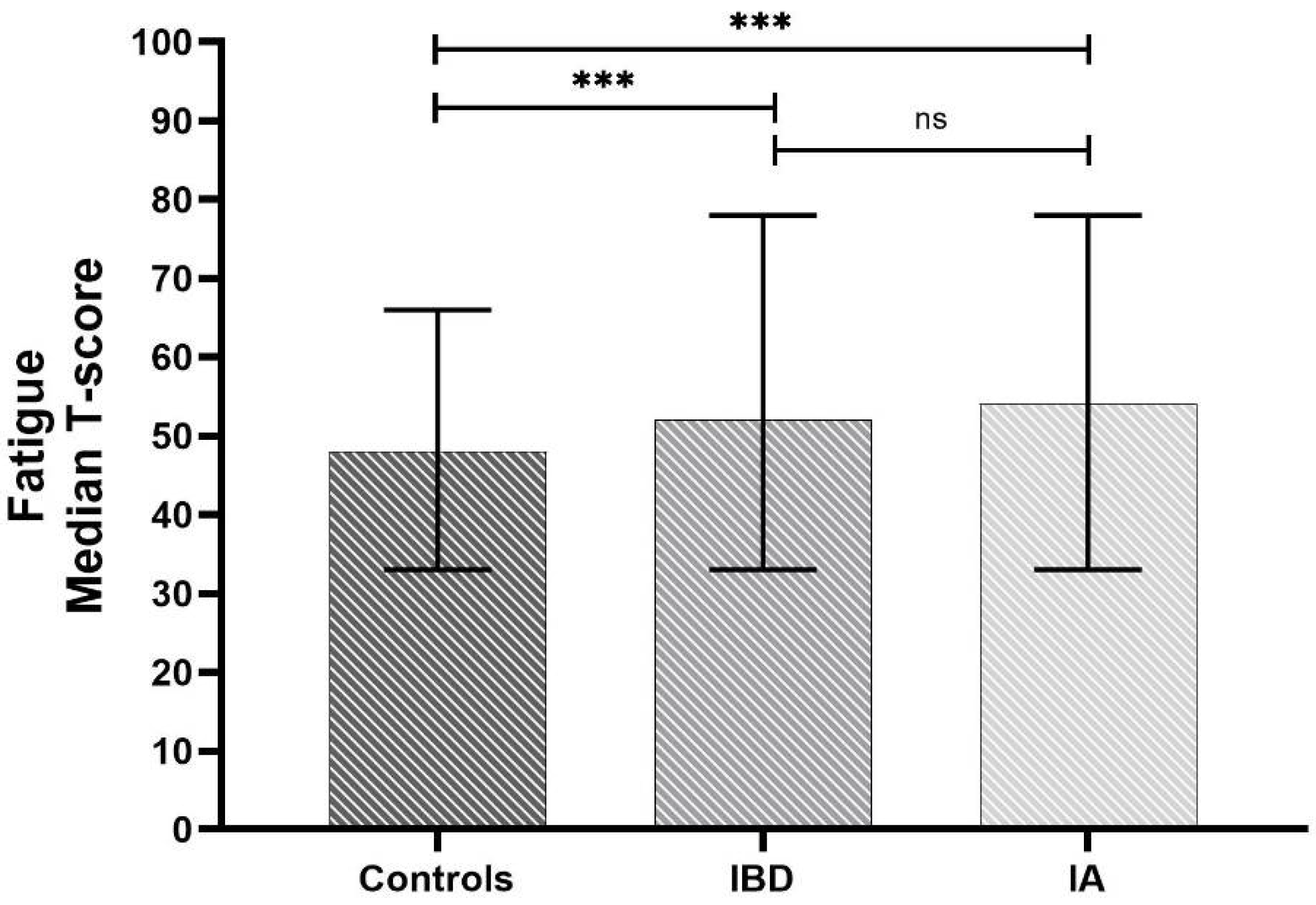
3.2. IMIDs Patients Have Increased Fatigue Compared with Healthy Controls
3.3. Variables Associated with Fatigue
3.4. Mood Disorders Are Strongly Associated with Fatigue in IMIDs Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finsterer, J.; Mahjoub, S.Z. Fatigue in healthy and diseased individuals. Am. J. Hosp. Palliat. Care. 2014, 31, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Rahman, P.; Inman, R.D.; El-Gabalawy, H.; Krause, D.O. Pathophysiology and pathogenesis of immune-mediated inflammatory diseases: Commonalities and differences. J. Rheumatol. Suppl. 2010, 85, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Borren, N.Z.; van der Woude, C.J.; Ananthakrishnan, A.N. Fatigue in IBD: Epidemiology, pathophysiology and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 247–259. [Google Scholar] [CrossRef]
- Dures, E.; Cramp, F.; Hackett, K.; Primdahl, J. Fatigue in inflammatory arthritis. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101526. [Google Scholar] [CrossRef] [PubMed]
- Geenen, R.; Dures, E. A biopsychosocial network model of fatigue in rheumatoid arthritis: A systematic review. Rheumatology 2019, 58 (Suppl. 5), v10–v21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, K.; Dures, E.; Ng, W.-F. Fatigue in inflammatory rheumatic diseases: Current knowledge and areas for future research. Nat. Rev. Rheumatol. 2021, 17, 651–664. [Google Scholar] [CrossRef]
- Marrie, R.A.; Walld, R.; Bolton, J.M.; Sareen, J.; Walker, J.R.; Patten, S.B.; Singer, A.; Lix, L.M.; Hitchon, C.A.; El-Gabalawy, R.; et al. Increased incidence of psychiatric disorders in immune-mediated inflammatory disease. J. Psychosom. Res. 2017, 101, 17–23. [Google Scholar] [CrossRef]
- Katchamart, W.; Narongroeknawin, P.; Chanapai, W.; Thaweeratthakul, P.; Srisomnuek, A. Prevalence of and factors associated with depression and anxiety in patients with rheumatoid arthritis: A multicenter prospective cross-sectional study. Int. J. Rheum. Dis. 2020, 23, 302–308. [Google Scholar] [CrossRef]
- Neuendorf, R.; Harding, A.; Stello, N.; Hanes, D.; Wahbeh, H. Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J. Psychosom. Res. 2016, 87, 70–80. [Google Scholar] [CrossRef]
- Parkinson, J.T.; Foley, É.M.; Jadon, D.R.; Khandaker, G.M. Depression in patients with spondyloarthritis: Prevalence, incidence, risk factors, mechanisms and management. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20970028. [Google Scholar] [CrossRef] [PubMed]
- Matcham, F.; Rayner, L.; Steer, S.; Hotopf, M. The prevalence of depression in rheumatoid arthritis: A systematic review and meta-analysis. Rheumatology 2013, 52, 2136–2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonough, E.; Ayearst, R.; Eder, L.; Chandran, V.; Rosen, C.F.; Thavaneswaran, A.; Gladman, D.D. Depression and anxiety in psoriatic disease: Prevalence and associated factors. J. Rheumatol. 2014, 41, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Schneeberger, E.E.; Marengo, M.F.; Dal Pra, F.; Maldonado Cocco, J.A.; Citera, G. Fatigue assessment and its impact in the quality of life of patients with ankylosing spondylitis. Clin. Rheumatol. 2015, 34, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Weldring, T.; Smith, S.M.S. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. insights 2013, 6, 61–68. [Google Scholar] [CrossRef]
- Boyce, M.B.; Browne, J.P.; Greenhalgh, J. The experiences of professionals with using information from patient-reported outcome measures to improve the quality of healthcare: A systematic review of qualitative research. BMJ Qual. Saf. 2014, 23, 508–518. [Google Scholar] [CrossRef]
- Jette, D.U.; Halbert, J.; Iverson, C.; Miceli, E.; Shah, P. Use of standardized outcome measures in physical therapist practice: Perceptions and applications. Phys. Ther. 2009, 89, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Hewlett, S.; Dures, E.; Almeida, C. Measures of fatigue: Bristol Rheumatoid Arthritis Fatigue Multi-Dimensional Questionnaire (BRAF MDQ), Bristol Rheumatoid Arthritis Fatigue Numerical Rating Scales (BRAF NRS) for severity, effect, and coping, Chalder Fatigue Questionnaire (CFQ), Checklist. Arthritis Care Res. 2011, 63 (Suppl. 1), S263–S286. [Google Scholar] [CrossRef]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M. The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Med Care. 2007, 45 (Suppl. 1), S3–S11. [Google Scholar] [CrossRef] [Green Version]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum. 2006, 54, 2665–2673. [Google Scholar] [CrossRef]
- Rudwaleit, M.; van der Heijde, D.; Landewé, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.; Landewé, R.; Lie, E.; Kvien, T.K.; Braun, J.; Baker, D.; van der Heijde, D. Ankylosing Spondylitis Disease Activity Score (ASDAS): Defining cut-off values for disease activity states and improvement scores. Ann. Rheum. Dis. 2011, 70, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Michelsen, B.; Sexton, J.; Smolen, J.S.; Aletaha, D.; Krogh, N.S.; van der Heijde, D.; Kvien, T.K.; Hetland, M.L. Can disease activity in patients with psoriatic arthritis be adequately assessed by a modified Disease Activity index for PSoriatic Arthritis (DAPSA) based on 28 joints? Ann. Rheum. Dis. 2018, 77, 1736–1741. [Google Scholar] [CrossRef] [PubMed]
- Prevoo, M.L.; van ’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef] [Green Version]
- Rosa-Gonçalves, D.; Bernardes, M.; Costa, L. Quality of life and functional capacity in patients with rheumatoid arthritis-Cross-sectional study. Reumatol. Clin. 2018, 14, 360–366. [Google Scholar] [CrossRef]
- Knowles, S.R.; Graff, L.A.; Wilding, H.; Hewitt, C.; Keefer, L.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part I. Inflamm. Bowel. Dis. 2018, 24, 742–751. [Google Scholar] [CrossRef]
- Gudu, T.; Gossec, L. Quality of life in psoriatic arthritis. Expert Rev. Clin. Immunol. 2018, 14, 405–417. [Google Scholar] [CrossRef]
- Kwan, Y.H.; Fong, W.; Tan, V.I.C.; Lui, N.L.; Malhotra, R.; Østbye, T.; Thumboo, J. A systematic review of quality-of-life domains and items relevant to patients with spondyloarthritis. Semin. Arthritis Rheum. 2017, 47, 175–182. [Google Scholar] [CrossRef]
- Schreiner, P.; Rossel, J.-B.; Biedermann, L.; Valko, P.O.; Baumann, C.R.; Greuter, T.; Scharl, M.; Vavricka, S.R.; Pittet, V.; Juillerat, P.; et al. Fatigue in inflammatory bowel disease and its impact on daily activities. Aliment. Pharmacol. Ther. 2021, 53, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Pilgaard, T.; Hagelund, L.; Stallknecht, S.E.; Jensen, H.H.; Esbensen, B.A. Severity of fatigue in people with rheumatoid arthritis, psoriatic arthritis and spondyloarthritis-Results of a cross-sectional study. PLoS ONE 2019, 14, e0218831. [Google Scholar] [CrossRef] [PubMed]
- Mancina, R.M.; Pagnotta, R.; Pagliuso, C.; Albi, V.; Bruno, D.; Garieri, P.; Doldo, P.; Spagnuolo, R. Gastrointestinal Symptoms of and Psychosocial Changes in Inflammatory Bowel Disease: A Nursing-Led Cross-Sectional Study of Patients in Clinical Remission. Medicina 2020, 56, 45. [Google Scholar] [CrossRef] [Green Version]
- Kappelman, M.D.; Long, M.D.; Martin, C.; DeWalt, D.A.; Kinneer, P.M.; Chen, W.; Lewis, J.D.; Sandler, R.S. Evaluation of the patient-reported outcomes measurement information system in a large cohort of patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2014, 12, 1315–1323. [Google Scholar] [CrossRef] [Green Version]
- Bingham Iii, C.O.; Gutierrez, A.K.; Butanis, A.; Bykerk, V.P.; Curtis, J.R.; Leong, A.; Lyddiatt, A.; Nowell, W.B.; Orbai, A.M.; Bartlett, S.J. PROMIS Fatigue short forms are reliable and valid in adults with rheumatoid arthritis. J. Patient-Rep. Outcomes. 2019, 3, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, M.C.; Ogdie, A.; Puravath, A.; Reveille, J.D. Reliability and Validity of Patient-reported Outcomes Measurement Information System Short Forms in Ankylosing Spondylitis. J. Rheumatol. 2020, 47, 1182–1188. [Google Scholar] [CrossRef]
- López-Medina, C.; Schiotis, R.E.; Font-Ugalde, P.; Castro-Villegas, M.C.; Calvo-Gutiérrez, J.; Ortega-Castro, R.; Jiménez-Gasco, R.; Escudero-Contreras, A.; Collantes-Estévez, E. Assessment of Fatigue in Spondyloarthritis and Its Association with Disease Activity. J. Rheumatol. 2016, 43, 751–757. [Google Scholar] [CrossRef]
- Haugeberg, G.; Hoff, M.; Kavanaugh, A.; Michelsen, B. Psoriatic arthritis: Exploring the occurrence of sleep disturbances, fatigue, and depression and their correlates. Arthritis Res. Ther. 2020, 22, 198. [Google Scholar] [CrossRef]
- Hammam, N.; Gamal, R.M.; Rashed, A.M.; Elfetoh, N.A.; Mosad, E.; Khedr, E.M. Fatigue in Rheumatoid Arthritis Patients: Association With Sleep Quality, Mood Status, and Disease Activity. Reumatol Clin. 2020, 5 Pt 1, 339–344. [Google Scholar] [CrossRef]
- Esbensen, B.A.; Stallknecht, S.E.; Madsen, M.E.; Hagelund, L.; Pilgaard, T. Correlations of fatigue in Danish patients with rheumatoid arthritis, psoriatic arthritis and spondyloarthritis. PLoS ONE 2020, 15, e0237117. [Google Scholar] [CrossRef]
- Chavarría, C.; Casanova, M.J.; Chaparro, M.; Barreiro-de Acosta, M.; Ezquiaga, E.; Bujanda, L.; Rivero, M.; Argüelles-Arias, F.; Martín-Arranz, M.D.; Martínez-Montiel, M.P.; et al. Prevalence and Factors Associated With Fatigue in Patients With Inflammatory Bowel Disease: A Multicentre Study. J. Crohns Colitis. 2019, 13, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Cook, K.F.; Jensen, S.E.; Schalet, B.D.; Beaumont, J.L.; Amtmann, D.; Czajkowski, S.; Dewalt, D.A.; Fries, J.F.; Pilkonis, P.A.; Reeve, B.B.; et al. PROMIS measures of pain, fatigue, negative affect, physical function, and social function demonstrated clinical validity across a range of chronic conditions. J. Clin. Epidemiol. 2016, 73, 89–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cella, D.; Lai, J.-S.; Jensen, S.E.; Christodoulou, C.; Junghaenel, D.U.; Reeve, B.B.; Stone, A.A. PROMIS Fatigue Item Bank had Clinical Validity across Diverse Chronic Conditions. J. Clin. Epidemiol. 2016, 73, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liuzza, M.T.; Spagnuolo, R.; Antonucci, G.; Grembiale, R.D.; Cosco, C.; Iaquinta, F.S.; Funari, V.; Dastoli, S.; Nistico, S.; Doldo, P. Psychometric evaluation of an Italian custom 4-item short form of the PROMIS anxiety item bank in immune-mediated inflammatory diseases: An item response theory analysis. PeerJ 2021, 9, e12100. [Google Scholar] [CrossRef]
- Enoka, R.M.; Duchateau, J. Translating Fatigue to Human Performance. Med. Sci. Sports Exerc. 2016, 48, 2228–2238. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Healthy Controls (n = 206) | IBD (n = 137) | IA (n = 103) | p | |
|---|---|---|---|---|
| Demographic and Anthropometric | ||||
| Age (years) | 53 (37–65) | 49 (39–58) | 53 (42–61) | 0.157 |
| Gender, n male (%) | 126 (61.2) | 87 (63.5) | 39 (37.9) | 7.1 × 10−5a |
| BMI (Kg/m2) | 25 (22–27) | 24 (22–27) | 25 (23–27) | 0.165 |
| Smoking, n = yes (%) | 91 (44.2) | 29 (21.2) | 39 (37.9) | 6.5 × 10−5b |
| Physical Activity, n = yes (%) | 73 (34.5) | 56 (40.9) | 27 (26.2) | 0.061 |
| High school diploma, n = yes (%) | 121 (58.7) | 98 (71.5) | 59 (57.3) | 0.027c |
| Marital status, n = not married (%) | 73 (35.4) | 34 (24.8) | 26 (25.2) | 0.056 |
| Occupation, n = yes (%) | 84 (40.8) | 69 (50.4) | 47 (45.6) | 0.213 |
| Disease characteristics | ||||
| Crohn’s Disease | - | 39 (28.5) | - | - |
| Ulcerative Colitis | - | 98 (71.5) | - | - |
| Rheumatoid Arthritis | - | - | 31 (30.1) | - |
| Spondyloarthritis | - | - | 72 (69.9) | - |
| Disease duration (years) | - | 12 (7–18) | 10 (5–14) | 0.012 |
| Active Disease, n = yes (%) | - | 31 (22.6) | 34 (33.0) | 0.073 |
| ESR (mm/h) | - | 8 (4–16) | 10 (5–19) | 0.021 |
| CRP (mg/dL) | - | 0.3 (0.3–0.6) | 0.4 (0.2–1.5) | 0.651 |
| Medications n (%) | ||||
| Steroids | - | 18 (13.1) | 15 (14.6) | 0.751 |
| Biological DMARDs | - | 26 (19.0) | 64 (62.1) | 8.16 × 10−16 |
| Methotrexate | - | 1 (0.7) | 40 (38.8) | 8.27 × 10−15 |
| Mesalamine | - | 122 (89.1) | - | - |
| Mood disorders | ||||
| Anxiety, n = yes (%) | 96 (46.6) | 88 (64.2) | 63 (61.2) | 0.002d |
| Anxiety, t-score | 49 (43–55) | 55 (46–63) | 53 (46–60) | 1.34 × 10−4e |
| Depression, n = yes (%) | 60 (29.1) | 55 (40.1) | 49 (47.6) | 0.004f |
| Depression, t-score | 45 (38–51) | 45 (38–56) | 49 (38–56) | 4.46 × 10−4g |
| Variables | OR (CI 95%) | p |
|---|---|---|
| Age | 1.02 (1.00–1.04) | 0.108 |
| BMI | 1.09 (0.99–1.19) | 0.072 |
| Gender | 1.3 × 10−5 | |
| Male | 0.29 (0.17–0.51) | |
| Female | 1 | |
| Disease | 0.012 | |
| IA | 2.01 (1.17–3.46) | |
| IBD | 1 | |
| Smoking | 0.543 | |
| Yes | 1.20 (0.67–2.15) | |
| No | 1 | |
| High school diploma | 0.003 | |
| Yes | 0.41 (0.23–0.74) | |
| No | 1 | |
| Physical activity | 0.244 | |
| Yes | 0.72 (0.42–1.25) | |
| No | 1 | |
| Marital status, single | 1 | |
| Yes | 1.00 (0.55–1.82) | |
| No | 1 | |
| Occupation | 0.005 | |
| Yes | 0.47 (0.28–0.80) | |
| No | 1 | |
| Disease duration | 1.01 (0.98–1.05) | 0.449 |
| Disease activity | 0.019 | |
| Yes | 2.12 (1.13–3.97) | |
| No | 1 | |
| ESR | 1.02 (1.00–1.04) | 0.109 |
| CRP | 1.02 (0.89–1.16) | 0.830 |
| Steroids treatment | 0.014 | |
| Yes | 3.20 (1.27–8.08) | |
| No | 1 | |
| Biological treatment | 0.132 | |
| Yes | 1.52 (0.88–2.64) | |
| No | 1 | |
| Anxiety | 1.40 × 10−9 | |
| Yes | 5.90 (3.32–10.49) | |
| No | 1 | |
| Depression | 3.80 × 10−11 | |
| Yes | 9.70 (4.95–19.03) | |
| No | 1 |
| Variables | OR (CI 95%) | p |
|---|---|---|
| Age | 0.98 (0.96–1.01) | 0.224 |
| BMI | 1.14 (1.00–1.29) | 0.050 |
| Gender | 0.092 | |
| Male | 0.53 (0.25–1.11) | |
| Female | 1 | |
| Type of disease | 0.085 | |
| IA | 1.89 (0.92–3.84) | |
| IBD | 1 | |
| High school diploma | 0.143 | |
| Yes | 0.51 (0.21–1.26) | |
| No | 1 | |
| Occupation | 0.108 | |
| Yes | 0.54 (0.25–1.15) | |
| No | 1 | |
| Disease activity | 0.121 | |
| Yes | 1.89 (0.85–4.23) | |
| No | 1 | |
| Steroids treatment | 0.054 | |
| Yes | 3.06 (0.98–9.55) | |
| No | 1 | |
| Anxiety | 0.002 | |
| Yes | 6.15 (1.51–6.59) | |
| No | 1 | |
| Depression | 1.3 × 10−5 | |
| Yes | 5.92 (2.66–13.17) | |
| No | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iaquinta, F.S.; Grembiale, R.D.; Mauro, D.; Pantano, I.; Naty, S.; Cosco, C.; Iacono, D.; Gaggiano, E.; Ruggiero, A.; Ciccia, F.; et al. Fatigue and Associated Factors in an Immune-Mediated Inflammatory Disease Population: A Cross-Sectional Study. J. Clin. Med. 2022, 11, 2455. https://doi.org/10.3390/jcm11092455
Iaquinta FS, Grembiale RD, Mauro D, Pantano I, Naty S, Cosco C, Iacono D, Gaggiano E, Ruggiero A, Ciccia F, et al. Fatigue and Associated Factors in an Immune-Mediated Inflammatory Disease Population: A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(9):2455. https://doi.org/10.3390/jcm11092455
Chicago/Turabian StyleIaquinta, Francesco Salvatore, Rosa Daniela Grembiale, Daniele Mauro, Ilenia Pantano, Saverio Naty, Cristina Cosco, Daniela Iacono, Emanuela Gaggiano, Annarita Ruggiero, Francesco Ciccia, and et al. 2022. "Fatigue and Associated Factors in an Immune-Mediated Inflammatory Disease Population: A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 9: 2455. https://doi.org/10.3390/jcm11092455