
Machine Learning Based on Diffusion Kurtosis Imaging Histogram Parameters for Glioma Grading

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MRI Protocols
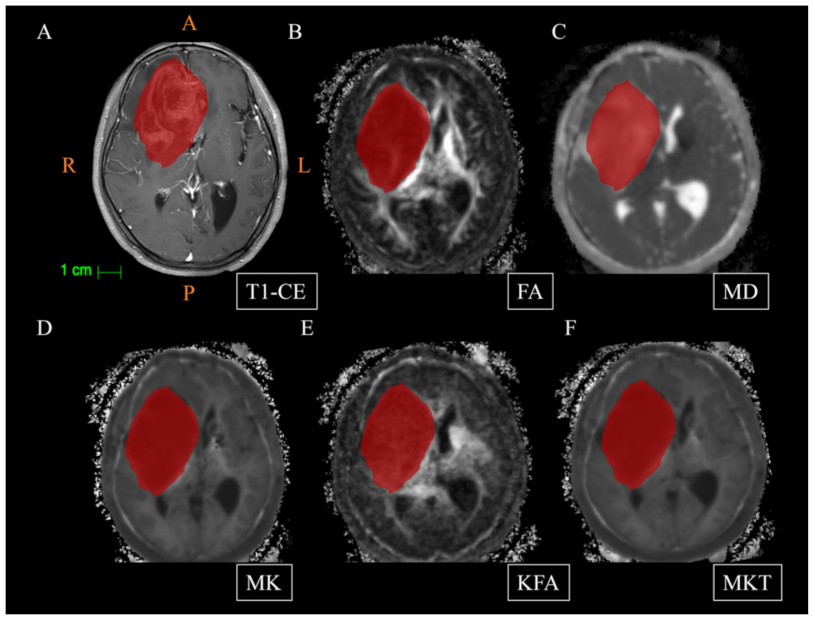
2.3. Data Processing and Delineation of Volumes of Interest (VOIs)
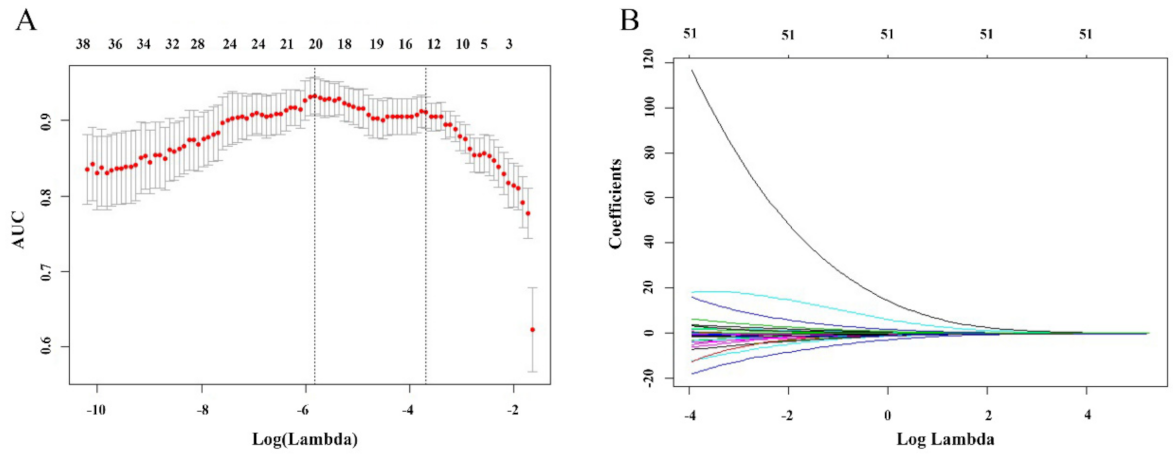
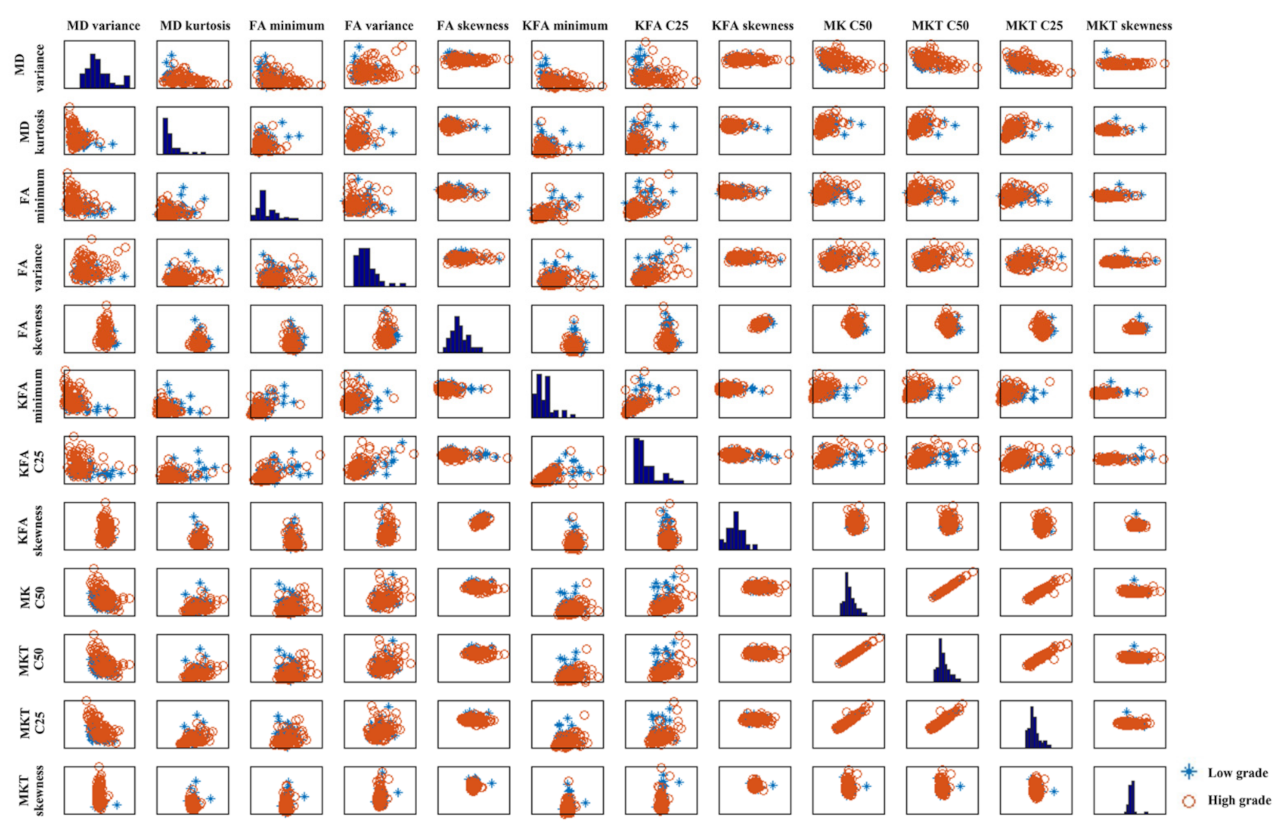
2.4. Feature Selection
2.5. SVM Analysis
2.6. Statistical Analysis
3. Results
3.1. Comparisons of Clinical Data and DKI Histogram Parameters between LGG and HGG
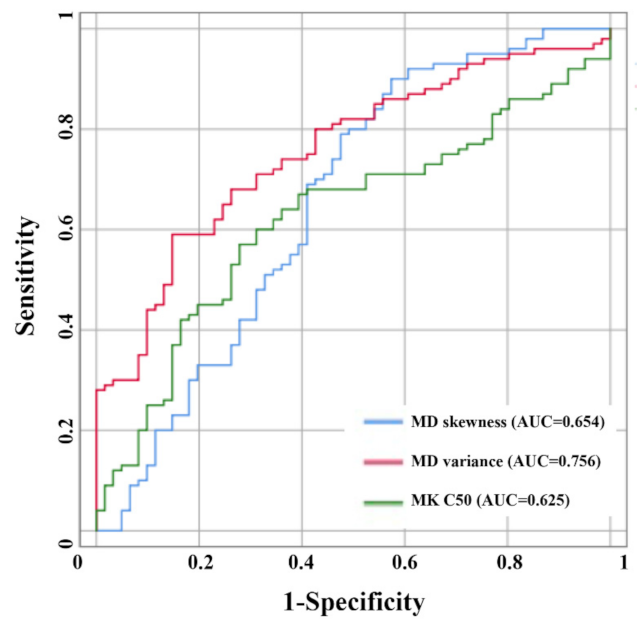
3.2. Logistic Regression and ROC Analysis for Glioma Grading
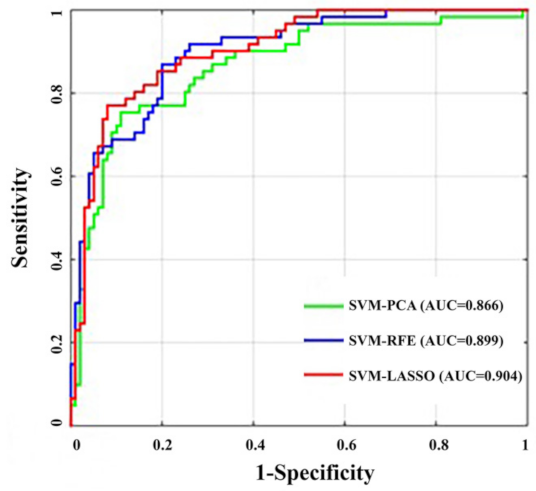
3.3. SVM Analysis for Glioma Grading
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Amico, R.S.; Englander, Z.K.; Canoll, P.; Bruce, J.N. Extent of Resection in Glioma-A Review of the Cutting Edge. World Neurosurg. 2017, 103, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Soliman, R.K.; Gamal, S.A.; Essa, A.A.; Othman, M.H. Preoperative Grading of Glioma Using Dynamic Susceptibility Contrast MRI: Relative Cerebral Blood Volume Analysis of Intra-tumoural and Peri-tumoural Tissue. Clin. Neurol. Neurosurg. 2018, 167, 86–92. [Google Scholar] [CrossRef] [PubMed]
- van Dijken, B.R.J.; van Laar, P.J.; Holtman, G.A.; van der Hoorn, A. Diagnostic accuracy of magnetic resonance imaging techniques for treatment response evaluation in patients with high-grade glioma, a systematic review and meta-analysis. Eur. Radiol. 2017, 27, 4129–4144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkinson, M.D.; Du Plessis, D.G.; Walker, C.; Smith, T.S. Advanced MRI in the management of adult gliomas. Br. J. Neurosurg. 2007, 21, 550–561. [Google Scholar] [CrossRef]
- De Pardieu, M.; Boucebci, S.; Herpe, G.; Fauche, C.; Velasco, S.; Ingrand, P.; Tasu, J.P. Glioma-grade diagnosis using in-phase and out-of-phase T1-weighted magnetic resonance imaging: A prospective study. Diagn. Interv. Imaging 2020, 101, 451–456. [Google Scholar] [CrossRef]
- Upadhyay, N.; Waldman, A.D. Conventional MRI evaluation of gliomas. Br. J. Radiol. 2011, 84, S107–S111. [Google Scholar] [CrossRef] [Green Version]
- Xiao, H.F.; Chen, Z.Y.; Lou, X.; Wang, Y.L.; Gui, Q.P.; Wang, Y.; Shi, K.N.; Zhou, Z.Y.; Zheng, D.D.; Wang, D.J.; et al. Astrocytic tumour grading: A comparative study of three-dimensional pseudocontinuous arterial spin labelling, dynamic susceptibility contrast-enhanced perfusion-weighted imaging, and diffusion-weighted imaging. Eur. Radiol. 2015, 25, 3423–3430. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Jiang, J.; Shen, N.; Zhao, L.; Zhang, J.; Qin, Y.; Zhang, S.; Li, L.; Zhu, W. Stretched-exponential model diffusion-weighted imaging as a potential imaging marker in preoperative grading and assessment of proliferative activity of gliomas. Am. J. Transl. Res. 2018, 10, 2659–2668. [Google Scholar]
- Yan, R.; Haopeng, P.; Xiaoyuan, F.; Jinsong, W.; Jiawen, Z.; Chengjun, Y.; Tianming, Q.; Ji, X.; Mao, S.; Yueyue, D.; et al. Non-Gaussian diffusion MR imaging of glioma: Comparisons of multiple diffusion parameters and correlation with histologic grade and MIB-1 (Ki-67 labeling) index. Neuroradiology 2016, 58, 121–132. [Google Scholar] [CrossRef]
- Jiang, L.; Xiao, C.Y.; Xu, Q.; Sun, J.; Chen, H.; Chen, Y.C.; Yin, X. Analysis of DTI-Derived Tensor Metrics in Differential Diagnosis between Low-grade and High-grade Gliomas. Front. Aging Neurosci. 2017, 9, 271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inano, R.; Oishi, N.; Kunieda, T.; Arakawa, Y.; Yamao, Y.; Shibata, S.; Kikuchi, T.; Fukuyama, H.; Miyamoto, S. Voxel-based clustered imaging by multiparameter diffusion tensor images for glioma grading. Neuroimage Clin. 2014, 5, 396–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lope-Piedrafita, S. Diffusion Tensor Imaging (DTI). Methods Mol. Biol. 2018, 1718, 103–116. [Google Scholar] [PubMed]
- Rosenkrantz, A.B.; Padhani, A.R.; Chenevert, T.L.; Koh, D.M.; De Keyzer, F.; Taouli, B.; Le Bihan, D. Body diffusion kurtosis imaging: Basic principles, applications, and considerations for clinical practice. J. Magn. Reson. Imaging 2015, 42, 1190–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arab, A.; Wojna-Pelczar, A.; Khairnar, A.; Szabo, N.; Ruda-Kucerova, J. Principles of diffusion kurtosis imaging and its role in early diagnosis of neurodegenerative disorders. Brain Res. Bull. 2018, 139, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Raja, R.; Sinha, N.; Saini, J.; Mahadevan, A.; Rao, K.N.; Swaminathan, A. Assessment of tissue heterogeneity using diffusion tensor and diffusion kurtosis imaging for grading gliomas. Neuroradiology 2016, 58, 1217–1231. [Google Scholar] [CrossRef]
- Wang, X.; Gao, W.; Li, F.; Shi, W.; Li, H.; Zeng, Q. Diffusion kurtosis imaging as an imaging biomarker for predicting prognosis of the patients with high-grade gliomas. Magn. Reson. Imaging 2019, 63, 131–136. [Google Scholar] [CrossRef]
- Hempel, J.M.; Schittenhelm, J.; Brendle, C.; Bender, B.; Bier, G.; Skardelly, M.; Tabatabai, G.; Castaneda Vega, S.; Ernemann, U.; Klose, U. Histogram analysis of diffusion kurtosis imaging estimates for in vivo assessment of 2016 WHO glioma grades: A cross-sectional observational study. Eur. J. Radiol. 2017, 95, 202–211. [Google Scholar] [CrossRef]
- Qi, X.X.; Shi, D.F.; Ren, S.X.; Zhang, S.Y.; Li, L.; Li, Q.C.; Guan, L.M. Histogram analysis of diffusion kurtosis imaging derived maps may distinguish between low and high grade gliomas before surgery. Eur. Radiol. 2018, 28, 1748–1755. [Google Scholar] [CrossRef]
- Kim, M.; Jung, S.Y.; Park, J.E. Diffusion- and perfusion-weighted MRI radiomics model may predict isocitrate dehydrogenase (IDH) mutation and tumor aggressiveness in diffuse lower grade glioma. Eur. Radiol. 2020, 30, 2142–2151. [Google Scholar] [CrossRef]
- Abdalla, G.; Dixon, L.; Sanverdi, E.; Machado, P.M.; Kwong, J.S.W.; Panovska-Griffiths, J.; Rojas-Garcia, A.; Yoneoka, D.; Veraart, J.; Van Cauter, S.; et al. The diagnostic role of diffusional kurtosis imaging in glioma grading and differentiation of gliomas from other intra-axial brain tumours: A systematic review with critical appraisal and meta-analysis. Neuroradiology 2020, 62, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.; Le, D.; Lim, J.I.; Chan, R.V.P.; Yao, X. Supervised Machine Learning Based Multi-Task Artificial Intelligence Classification of Retinopathies. J. Clin. Med. 2019, 8, 872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madelin, G.; Poidevin, F.; Makrymallis, A.; Regatte, R.R. Classification of sodium MRI data of cartilage using machine learning. Magn. Reson. Med. 2015, 74, 1435–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisdas, S.; Shen, H.; Thust, S.; Katsaros, V.; Stranjalis, G.; Boskos, C.; Brandner, S.; Zhang, J. Texture analysis- and support vector machine-assisted diffusional kurtosis imaging may allow in vivo gliomas grading and IDH-mutation status prediction: A preliminary study. Sci. Rep. 2018, 8, 6108. [Google Scholar] [CrossRef]
- Does, M.D.; Olesen, J.L.; Harkins, K.D.; Serradas-Duarte, T.; Gochberg, D.F.; Jespersen, S.N.; Shemesh, N. Evaluation of principal component analysis image denoising on multi-exponential MRI relaxometry. Magn. Reson. Med. 2019, 81, 3503–3514. [Google Scholar] [CrossRef]
- Lin, X.; Li, C.; Zhang, Y.; Su, B.; Fan, M.; Wei, H. Selecting Feature Subsets Based on SVM-RFE and the Overlapping Ratio with Applications in Bioinformatics. Molecules 2017, 23, 52. [Google Scholar] [CrossRef] [Green Version]
- Sanz, H.; Valim, C.; Vegas, E.; Oller, J.M.; Reverter, F. SVM-RFE: Selection and visualization of the most relevant features through non-linear kernels. BMC Bioinform. 2018, 19, 432. [Google Scholar] [CrossRef] [Green Version]
- Xia, J.; Sun, L.; Xu, S.; Xiang, Q.; Zhao, J.; Xiong, W.; Xu, Y.; Chu, S. A Model Using Support Vector Machines Recursive Feature Elimination (SVM-RFE) Algorithm to Classify Whether COPD Patients Have Been Continuously Managed According to GOLD Guidelines. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 2779–2786. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Delgado, A.F.; Fahlstrom, M.; Nilsson, M.; Berntsson, S.G.; Zetterling, M.; Libard, S.; Alafuzoff, I.; van Westen, D.; Latt, J.; Smits, A.; et al. Diffusion Kurtosis Imaging of Gliomas Grades II and III—A Study of Perilesional Tumor Infiltration, Tumor Grades and Subtypes at Clinical Presentation. Radiol. Oncol. 2017, 51, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Zhou, X.J. Diffusion MRI of cancer: From low to high b-values. J. Magn. Reson. Imaging 2019, 49, 23–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Agha, M.; Abushab, K.; Quffa, K.; Al-Agha, S.; Alajerami, Y.; Tabash, M. Efficiency of High and Standard b Value Diffusion-Weighted Magnetic Resonance Imaging in Grading of Gliomas. J. Oncol. 2020, 2020, 6942406. [Google Scholar] [CrossRef] [PubMed]
- Cihangiroglu, M.M.; Ozturk-Isik, E.; Firat, Z.; Kilickesmez, O.; Ulug, A.M.; Ture, U. Preoperative grading of supratentorial gliomas using high or standard b-value diffusion-weighted MR imaging at 3T. Diagn. Interv. Imaging 2017, 98, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Sui, Y.; Xiong, Y. Differentiation of Low- and High-Grade Gliomas Using High b-Value Diffusion Imaging with a Non-Gaussian Diffusion Model. AJNR Am. J. Neuroradiol. 2016, 37, 1643–1649. [Google Scholar] [CrossRef] [Green Version]
- Raab, P.; Hattingen, E.; Franz, K.; Zanella, F.E.; Lanfermann, H. Cerebral gliomas: Diffusional kurtosis imaging analysis of microstructural differences. Radiology 2010, 254, 876–881. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR Biomed. 2010, 23, 698–710. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A.; Ramani, A.; Lu, H.; Kaczynski, K. Diffusional kurtosis imaging: The quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn. Reson. Med. 2005, 53, 1432–1440. [Google Scholar] [CrossRef]
- Nedaie, A.; Najafi, A.A. Support vector machine with Dirichlet feature mapping. Neural Netw. 2018, 98, 87–101. [Google Scholar] [CrossRef]
- Lee, J.; Jain, R.; Khalil, K.; Griffith, B.; Bosca, R.; Rao, G.; Rao, A. Texture Feature Ratios from Relative CBV Maps of Perfusion MRI Are Associated with Patient Survival in Glioblastoma. AJNR Am. J. Neuroradiol. 2016, 37, 37–43. [Google Scholar] [CrossRef]
- Wu, S.; Zheng, J.; Li, Y.; Yu, H.; Shi, S.; Xie, W.; Liu, H.; Su, Y.; Huang, J.; Lin, T. A Radiomics Nomogram for the Preoperative Prediction of Lymph Node Metastasis in Bladder Cancer. Clin. Cancer Res. 2017, 23, 6904–6911. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Tian, J.; Dong, D.; Gu, D.; Dong, Y.; Zhang, L.; Lian, Z.; Liu, J.; Luo, X.; Pei, S.; et al. Radiomics Features of Multiparametric MRI as Novel Prognostic Factors in Advanced Nasopharyngeal Carcinoma. Clin. Cancer Res. 2017, 23, 4259–4269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cauter, S.; De Keyzer, F.; Sima, D.M.; Sava, A.C.; D’Arco, F.; Veraart, J.; Peeters, R.R.; Leemans, A.; Van Gool, S.; Wilms, G.; et al. Integrating diffusion kurtosis imaging, dynamic susceptibility-weighted contrast-enhanced MRI, and short echo time chemical shift imaging for grading gliomas. Neuro Oncol. 2014, 16, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Maximov, I.I.; Tonoyan, A.S.; Pronin, I.N. Differentiation of glioma malignancy grade using diffusion MRI. Phys. Med. 2017, 40, 24–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cauter, S.; Veraart, J.; Sijbers, J.; Peeters, R.R.; Himmelreich, U.; De Keyzer, F.; Van Gool, S.W.; Van Calenbergh, F.; De Vleeschouwer, S.; Van Hecke, W.; et al. Gliomas: Diffusion kurtosis MR imaging in grading. Radiology 2012, 263, 492–501. [Google Scholar] [CrossRef] [Green Version]
- Alexiou, G.A.; Zikou, A.; Tsiouris, S.; Goussia, A.; Kosta, P.; Papadopoulos, A.; Voulgaris, S.; Kyritsis, A.P.; Fotopoulos, A.D.; Argyropoulou, M.I. Correlation of diffusion tensor, dynamic susceptibility contrast MRI and (99 m)Tc-Tetrofosmin brain SPECT with tumour grade and Ki-67 immunohistochemistry in glioma. Clin. Neurol. Neurosurg. 2014, 116, 41–45. [Google Scholar] [CrossRef]
- Rotkopf, L.T.; Tiedt, S.; Puhr-Westerheide, D.; Herzberg, M.; Reidler, P.; Kellert, L.; Feil, K.; Thierfelder, K.M.; Dorn, F.; Liebig, T.; et al. Ischemic Core Volume Combined with the Relative Perfusion Ratio for Stroke Outcome Prediction after Endovascular Thrombectomy. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2020, 30, 321–326. [Google Scholar] [CrossRef]
- Beppu, T.; Inoue, T.; Shibata, Y.; Kurose, A.; Arai, H.; Ogasawara, K.; Ogawa, A.; Nakamura, S.; Kabasawa, H. Measurement of fractional anisotropy using diffusion tensor MRI in supratentorial astrocytic tumors. J. Neurooncol. 2003, 63, 109–116. [Google Scholar] [CrossRef]
- Falk Delgado, A.; Nilsson, M.; van Westen, D.; Falk Delgado, A. Glioma Grade Discrimination with MR Diffusion Kurtosis Imaging: A Meta-Analysis of Diagnostic Accuracy. Radiology 2018, 287, 119–127. [Google Scholar] [CrossRef]
- Tietze, A.; Hansen, M.B.; Ostergaard, L.; Jespersen, S.N.; Sangill, R.; Lund, T.E.; Geneser, M.; Hjelm, M.; Hansen, B. Mean Diffusional Kurtosis in Patients with Glioma: Initial Results with a Fast Imaging Method in a Clinical Setting. AJNR Am. J. Neuroradiol. 2015, 36, 1472–1478. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histopathological Characteristic | LGG (n = 61) | HGG (n = 100) | T/χ2 Value | p Value |
|---|---|---|---|---|
| Age | 48.77 ± 10.90 | 52.43 ± 13.98 | 4.608 | 0.006 |
| Sex (male) | 29 (47.54%) | 58 (58.00%) | 1.669 | 0.254 |
| Histology | Oligodendroglioma (25, 40.98%) Diffuse astrocytoma (36, 59.01%) | Anaplastic astrocytoma (25, 25%) Anaplastic oligodendroglioma (13, 13%) Glioblastoma (61, 61%) Gliosarcoma (1, 1%) | - |
| Mean | Minimum | Maximum | Variance | C25 | C50 | C75 | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|---|---|---|
| FA | |||||||||
| LGG | 0.06 ± 0.02 a | 0.01 ± 0.01 a | 0.23 ± 0.08 a | 0.03 ± 0.01 a | 0.04 ± 0.01 a | 0.06 ± 0.02 a | 0.08 ± 0.03 a | 1.23 ± 0.47 | 5.33 ± 2.17 |
| HGG | 0.07 ± 0.03 a | 0.02 ± 0.00 | 0.06 ± 0.02 | 0.03 ± 0.01 | 0.04 ± 0.02 | 0.06 ± 0.03 | 0.09 ± 0.03 | 0.81 ± 0.43 | 3.75 ± 1.32 |
| T value | −0.959 | 2.734 | 0.640 | −1.676 | 0.153 | −1.199 | −1.700 | 5.766 | 5.752 |
| p value | 0.339 | 0.007 * | 0.523 | 0.096 | 0.879 | 0.232 | 0.091 | <0.001 * | <0.001 * |
| MD | |||||||||
| LGG | 2.50 ± 0.62 | 1.75 ± 0.53 | 3.72 ± 0.78 | 0.39 ± 0.18 | 2.24 ± 0.56 | 2.44 ± 0.62 | 2.75 ± 0.74 | 0.35 ± 0.79 | 3.83 ± 2.09 |
| HGG | 2.41 ± 0.58 | 1.73 ± 0.52 | 3.29 ± 0.66 | 0.25 ± 0.08 | 2.21 ± 0.55 | 2.40 ± 0.59 | 2.57 ± 0.62 | 0.65 ± 0.57 | 3.49 ± 1.64 |
| T value | −0.948 | 0.174 | −3.570 | −6.564 | 0.301 | −0.491 | −1.638 | −2.642 | 1.172 |
| p value | 0.344 | 0.862 | <0.001 * | <0.001 * | 0.764 | 0.624 | 0.103 | 0.010 * | 0.243 |
| MK | |||||||||
| LGG | 0.53 ± 0.08 | 0.38 ± 0.06 | 0.84 ± 0.34 | 0.07 ± 0.03 | 0.48 ± 0.08 | 0.52 ± 0.08 | 0.57 ± 0.09 | 0.57 ± 0.76 | 4.07 ± 5.31 |
| HGG | 0.08 ± 0.05 | 0.37 ± 0.09 | 0.84 ± 0.29 | 0.08 ± 0.05 | 0.51 ± 0.10 | 0.57 ± 0.11 | 0.63 ± 0.12 | 0.11 ± 0.56 | 2.99 ± 1.43 |
| T value | −2.962 | 0.968 | 0.000 | −2.122 | −2.783 | −3.578 | −3.691 | 4.392 | 1.926 |
| p value | 0.002 * | 0.334 | 1.000 | 0.035 * | 0.006 * | <0.001 * | <0.001 * | <0.001 * | 0.056 |
| KFA | |||||||||
| LGG | 0.08 ± 0.04 | 0.02 ± 0.01 | 0.23 ± 0.13 | 0.03 ± 0.02 | 0.06 ± 0.03 | 0.08 ± 0.04 | 0.10 ± 0.05 | 0.95 ± 0.42 | 4.36 ± 1.47 |
| HGG | 0.07 ± 0.04 | 0.01 ± 0.01 | 0.22 ± 0.17 | 0.03 ± 0.02 | 0.05 ± 0.03 | 0.06 ± 0.04 | 0.09 ± 0.05 | 0.94 ± 0.45 | 4.26 ± 1.58 |
| T value | 1.508 | 3.244 | 0.378 | −0.399 | 2.552 | 1.756 | 1.172 | 0.064 | 0.426 |
| p value | 0.134 | 0.001 * | 0.706 | 0.691 | 0.012 * | 0.081 | 0.243 | 0.949 | 0.670 |
| MKT | |||||||||
| LGG | 0.53 ± 0.08 | 0.38 ± 0.06 | 0.83 ± 0.34 | 0.07 ± 0.03 | 0.48 ± 0.07 | 0.52 ± 0.08 | 0.57 ± 0.86 | 0.56 ± 0.76 | 4.05 ± 5.28 |
| HGG | 0.57 ± 0.11 | 0.37 ± 0.09 | 0.83 ± 0.29 | 0.08 ± 0.05 | 0.51 ± 0.10 | 0.57 ± 0.11 | 0.63 ± 0.12 | 0.11 ± 0.56 | 2.98 ± 1.43 |
| T value | −3.192 | 0.960 | −0.020 | −2.122 | −2.785 | −3.568 | −3.689 | 4.360 | 1.916 |
| p value | 0.002 * | 0.338 | 0.984 | 0.035 * | 0.006 * | <0.001 * | <0.001 * | <0.001 * | 0.057 |
| B | SE | Wald | OR (95%CI) | p | |
|---|---|---|---|---|---|
| FA skewness | −2.669 | 0.678 | 15.509 | 0.069 (0.018–0.262) | <0.001 |
| MD variance | 16.087 | 3.259 | 24.360 | 96.95 (1.63–576.79) | <0.001 |
| MD skewness | −0.0965 | 0.486 | 3.934 | 0.381 (0.147–0.989) | 0.047 |
| MK C50 | −663.238 | 274.430 | 5.841 | 0.000 (0.000–0.000) | 0.016 |
| KFA C25 | −56.660 | 14.118 | 16.107 | 0.000 (0.000–0.000) | <0.001 |
| AUC | Cutoff | Sensitivity | Specificity | |
|---|---|---|---|---|
| MD variance | 0.756 | 0.31 | 0.590 | 0.852 |
| MD skewness | 0.654 | 0.49 | 0.600 | 0.689 |
| MK C50 | 0.625 | 0.54 | 0.570 | 0.721 |
| AUC | Accuracy | Sensitivity | Specificity | F1 Score | |
|---|---|---|---|---|---|
| SVM-PCA | 0.866 ± 0.061 | 0.820 ± 0.056 | 0.754 ± 0.148 | 0.890 ± 0.123 | 0.845 ± 0.122 |
| SVM-RFE | 0.899 ± 0.079 | 0.814 ± 0.055 | 0.869 ± 0.146 | 0.800 ± 0.150 | 0.908 ± 0.092 |
| SVM-LASSO | 0.904 ± 0.069 | 0.857 ± 0.081 | 0.771 ± 0.152 | 0.920 ± 0.094 | 0.863 ± 0.135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, L.; Zhou, L.; Ai, Z.; Xiao, C.; Liu, W.; Geng, W.; Chen, H.; Xiong, Z.; Yin, X.; Chen, Y.-C. Machine Learning Based on Diffusion Kurtosis Imaging Histogram Parameters for Glioma Grading. J. Clin. Med. 2022, 11, 2310. https://doi.org/10.3390/jcm11092310
Jiang L, Zhou L, Ai Z, Xiao C, Liu W, Geng W, Chen H, Xiong Z, Yin X, Chen Y-C. Machine Learning Based on Diffusion Kurtosis Imaging Histogram Parameters for Glioma Grading. Journal of Clinical Medicine. 2022; 11(9):2310. https://doi.org/10.3390/jcm11092310
Chicago/Turabian StyleJiang, Liang, Leilei Zhou, Zhongping Ai, Chaoyong Xiao, Wen Liu, Wen Geng, Huiyou Chen, Zhenyu Xiong, Xindao Yin, and Yu-Chen Chen. 2022. "Machine Learning Based on Diffusion Kurtosis Imaging Histogram Parameters for Glioma Grading" Journal of Clinical Medicine 11, no. 9: 2310. https://doi.org/10.3390/jcm11092310