
Premature Mortality in Type 2 Diabetes Mellitus Associated with Heart Failure and Chronic Kidney Disease: 20 Years of Real-World Data

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
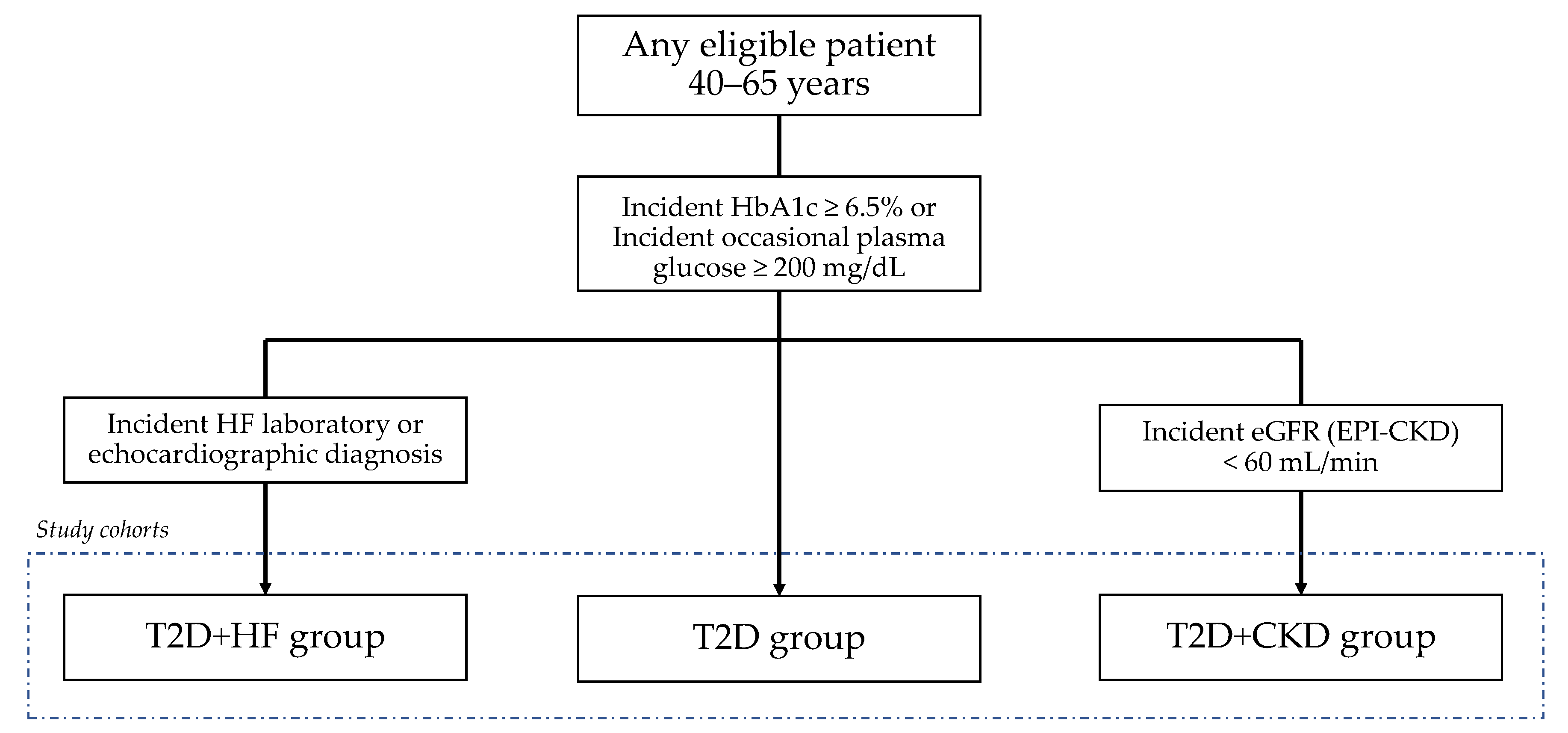
2.1. Study Design and Participant Selection
2.2. Type 2 Diabetes Mellitus Inclusion Criteria
2.3. Heart Failure Inclusion Criteria
2.4. Chronic Kidney Disease Inclusion Criteria
2.5. Additional Definitions
2.6. Outcome Measurements
2.7. Data Collection and Statistical Analysis
2.8. Ethical Approval
3. Results
3.1. T2D Cohort
3.2. T2D and HF Cohort
3.3. T2D and CKD Cohort
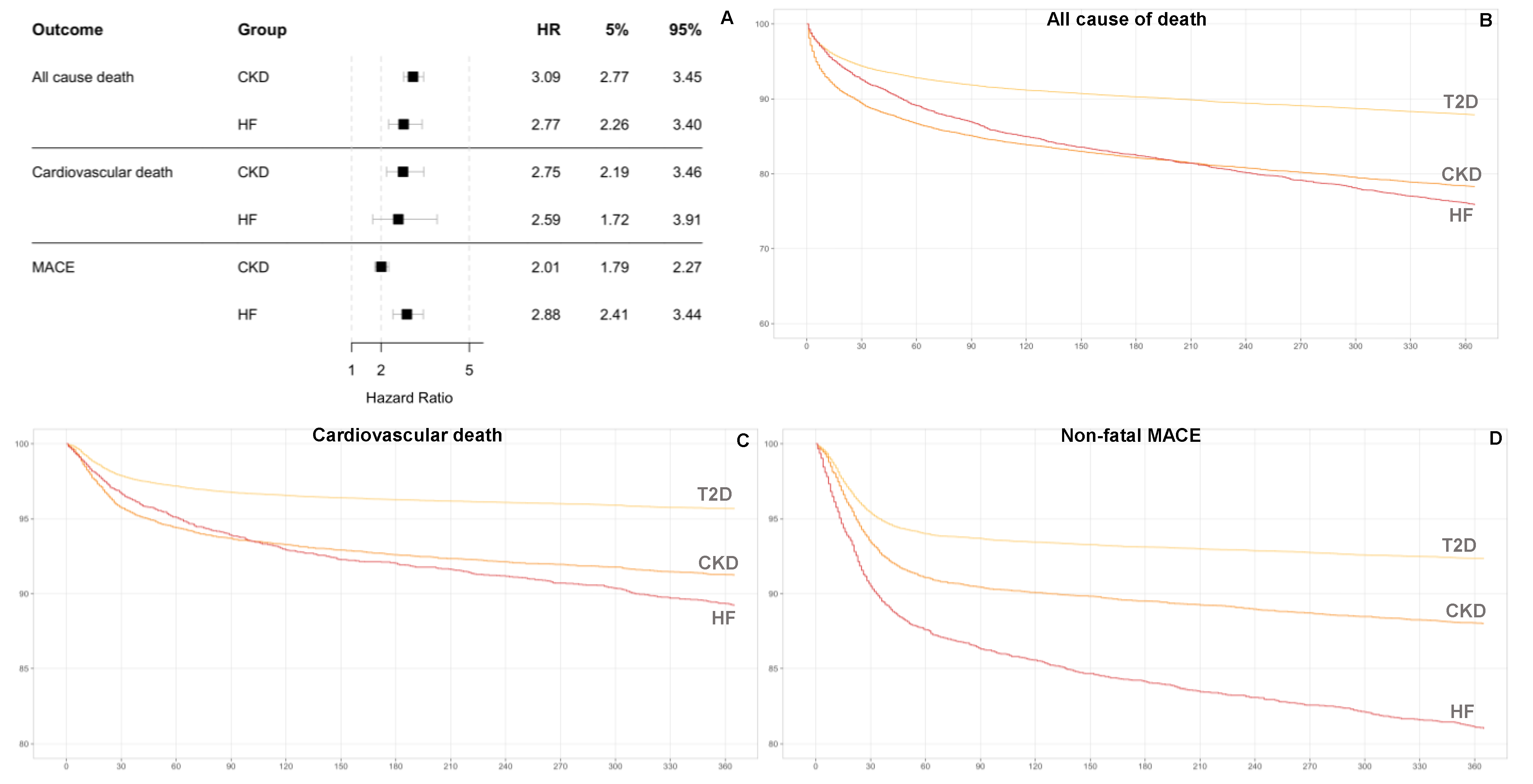
3.4. Mortality Risk
3.5. Non-Fatal MACEs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes-Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raposo, J.F. Diabetes: Factos e números 2016, 2017 e 2018. Rev. Port. Diabetes 2020, 15, 19–27. [Google Scholar]
- Fontes-Carvalho, R.; Santos-Ferreira, D.; Raz, I.; Marx, N.; Ruschitzka, F.; Cosentino, F. Protective effects of SGLT-2 inhibitors across the cardiorenal continuum: Two faces of the same coin. Eur. J. Prev. Cardiol. 2021, zwab034. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, D. Heart Failure, Diabetes Mellitus, and Chronic Kidney Disease: A Clinical Conundrum. Circ. Heart Fail. 2016, 9, e003316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Severino, P.; D’Amato, A.; Prosperi, S.; Fanisio, F.; Birtolo, L.I.; Costi, B.; Netti, L.; Chimenti, C.; Lavalle, C.; Maestrini, V.; et al. Myocardial Tissue Characterization in Heart Failure with Preserved Ejection Fraction: From Histopathology and Cardiac Magnetic Resonance Findings to Therapeutic Targets. Int. J. Mol. Sci. 2021, 22, 7650. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, E.; Idris, I. Early onset type 2 diabetes: Risk factors, clinical impact and management. Ther. Adv. Chronic Dis. 2014, 5, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Hillier, T.A.; Pedula, K.L. Complications in young adults with early-onset type 2 diabetes: Losing the relative protection of youth. Diabetes Care 2003, 26, 2999–3005. [Google Scholar] [CrossRef] [Green Version]
- Nanayakkara, N.; Curtis, A.J.; Heritier, S.; Gadowski, A.M.; Pavkov, M.E.; Kenealy, T.; Owens, D.R.; Thomas, R.L.; Song, S.; Wong, J.; et al. Impact of age at type 2 diabetes mellitus diagnosis on mortality and vascular complications: Systematic review and meta-analyses. Diabetologia 2021, 64, 275–287. [Google Scholar] [CrossRef]
- Wou, C.; Unwin, N.; Huang, Y.; Roglic, G. Implications of the growing burden of diabetes for premature cardiovascular disease mortality and the attainment of the Sustainable Development Goal target 3.4. Cardiovasc. Diagn. Ther. 2019, 9, 140–149. [Google Scholar] [CrossRef]
- Heald, A.H.; Stedman, M.; Davies, M.; Livingston, M.; Alshames, R.; Lunt, M.; Rayman, G.; Gadsby, R. Estimating life years lost to diabetes: Outcomes from analysis of National Diabetes Audit and Office of National Statistics data. Cardiovasc. Endocrinol. Metab. 2020, 9, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Braunwald, E. Diabetes, heart failure, and renal dysfunction: The vicious circles. Prog. Cardiovasc. Dis. 2019, 62, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Ge, J.; Lam, C.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Angiotensin–neprilysin inhibition in heart failure with preserved ejection fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Dunlay, S.M.; Givertz, M.M.; Aguilar, D.; Allen, L.A.; Chan, M.; Desai, A.S.; Deswal, A.; Dickson, V.V.; Kosiborod, M.N.; Lekavich, C.L.; et al. Type 2 Diabetes Mellitus and Heart Failure, A Scientific Statement From the American Heart Association and Heart Failure Society of America. J. Card. Fail. 2019, 25, 584–619. [Google Scholar] [CrossRef]
- Taal, M.W.; Brenner, B.M. Predicting initiation and progression of chronic kidney disease: Developing renal risk scores. Kidney Int. 2006, 70, 1694–1705. [Google Scholar] [CrossRef] [Green Version]
- McClellan, W.M.; Flanders, W.D. Risk Factors for Progressive Chronic Kidney Disease. J. Am. Soc. Nephrol. 2003, 14, S65–S70. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Varadhan, A.; Stephan, K.; Gupta, R.; Vyas, A.V.; Ranchal, P.; Aronow, W.S.; Hawwa, N.; Lanier, G.M. Growing role of SGLT2i in heart failure: Evidence from clinical trials. Expert Rev. Clin. Pharmacol. 2022, 15, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Heath, R.; Johnsen, H.; Strain, W.D.; Evans, M. Emerging Horizons in Heart Failure with Preserved Ejection Fraction: The Role of SGLT2 Inhibitors. Diabetes Ther. 2022, 13, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [Green Version]
- Sundström, J.; Bodegard, J.; Bollmann, A.; Vervloet, M.G.; Mark, P.B.; Karasik, A.; Taveira-Gomes, T.; Botana, M.; Birkeland, K.I.; Thuresson, M.; et al. Prevalence, outcomes, and cost of CKD in a contemporary population of 2·4 million patients from 11 countries: The CaReMe CKD study. Prepr. Lancet 2022. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| T2D (n = 14,986) | T2D + HF (n = 1101) | T2D + CKD (n = 3114) | |
|---|---|---|---|
| Demographics | |||
| Age (years)—mean (SD) | 55.69 (6.58) | 58.32 (5.83) | 58.36 (5.96) |
| Sex (males)—n (%) | 8486 (56.63) | 667 (60.58) | 1692 (54.34) |
| General comorbidities—n (%) | |||
| Hypertension | 4783 (31.92) | 51 (68.21) | 1855 (59.57) |
| Cardiovascular disease | 1095 (7.31) | 674 (61.22) | 668 (21.45) |
| Cardiorenal disease | 284 (1.9) | 775 (70.39) | 264 (8.48) |
| Myocardial infarction | 370 (2.47) | 314 (28.52) | 200 (6.42) |
| Unstable angina | 125 (0.83) | 89 (8.08) | 89 (2.86) |
| Stable angina | 325 (2.17) | 260 (23.61) | 227 (7.29) |
| Atrial fibrillation | 159 (1.06) | 197 (17.89) | 120 (3.85) |
| Stroke | 475 (3.17) | 207 (18.8) | 299 (9.6) |
| Peripheral artery disease | 41 (0.27) | 53 (4.81) | 44 (1.41) |
| Microvascular disease | 301 (2.01) | 227 (20.62) | 294 (9.44) |
| Clinical assessment—median (IQR) | |||
| Systolic blood pressure (mmHg) | 138 (20) | 137 (26) | 138 (22) |
| Diastolic blood pressure (mmHg) | 85 (11) | 80 (15) | 82 (14) |
| Body mass index (kg/m2) | 29.98 (6.55) | 29.75 (7.46) | 30.07 (6.69) |
| Waist circumference (cm) | 102 (15) | 104 (17.75) | 104 (17) |
| Laboratory assessment—median (IQR) | |||
| Glycated hemoglobin (%) | 6.9 (1.3) | 7 (1.9) | 7.1 (1.9) |
| LDL cholesterol (mg/dL) | 121.73 (52) | 109 (53) | 113.8 (54) |
| HDL cholesterol (mg/dL) | 43 (16) | 38 (16.15) | 41 (16.2) |
| Total cholesterol (mg/dL) | 201 (60) | 176 (61.1) | 188 (64.32) |
| Triglycerides (mg/dL) | 145 (103) | 126 (93) | 148 (105) |
| BNP (pg/mL) | 123.1 (298.6) | 273.1 (560.7) | 124.2 (428.2) |
| NT-proBNP (pg/mL) | 377.9 (1589.85) | 3732 (5193.8) | 6036.15 (2304.15) |
| Serum creatinine (mg/mL) | 0.8 (0.3) | 0.9 (0.6) | 1.4 (0.6) |
| Albumin to Creatinine Ratio (mg/g) | 12.2 (22.2) | 32 (216.91) | 17 (65.5) |
| eGFR (mL/min, MDRD) | 91.5 (31.02) | 79.25 (54.66) | 53.41 (18.26) |
| Baseline medication, diabetes—n (%) | |||
| Oral antidiabetics | 4128 (27.55) | 504 (45.78) | 1608 (51.64) |
| Insulins | 249 (1.66) | 218 (19.8) | 399 (12.81) |
| Metformin | 3636 (24.26) | 444 (40.33) | 1495 (48.01) |
| SGLT-2 inhibitors | 20 (0.13) | 18 (1.63) | 67 (2.15) |
| DPP-4 inhibitors | 745 (4.97) | 245 (22.25) | 706 (22.67) |
| Sulfonylurea | 1297 (8.65) | 266 (24.16) | 826 (26.53) |
| GLP-1 receptor agonists | 24 (0.16) | 11 (1) | 45 (1.45) |
| Meglitinides | 236 (1.57) | 60 (5.45) | 214 (6.87) |
| Glitazones | 62 (0.41) | 24 (2.18) | 98 (3.15) |
| Acarbose | 265 (1.77) | 62 (5.63) | 204 (6.55) |
| Patients (n) | Person-Years Cohort Total | Event Rate per Person-Year | Follow-Up (Days) Mean (SD) | Time to Event Mean (SD) | HR (95% CI) | ||
|---|---|---|---|---|---|---|---|
| All Cause Death | T2D | 14,123 | 12,572.37 | 0.05 | 324.92 (102.72) | 91.91 (105.15) | - |
| T2D + CKD | 3002 | 2502.96 | 0.15 | 304.44 (121.20) | 77.93 (96.49) | 3.09 (2.77–3.45) | |
| T2D + HF | 1003 | 842.36 | 0.14 | 306.54 (115.05) | 126.26 (113.86) | 2.77 (2.26–3.40) | |
| Cardiovascular death | T2D | 14,179 | 12,632.98 | 0.01 | 325.20 (101.94) | 62.24 (81.09) | - |
| T2D + CKD | 3035 | 2531.41 | 0.03 | 304.44 (119.86) | 69.71 (84.56) | 2.75 (2.19–3.46) | |
| T2D + HF | 1012 | 852.26 | 0.04 | 307.39 (114.15) | 111.16 (112.87) | 2.59 (1.72–3.91) | |
| MACEs | T2D | 14,179 | 12,214.51 | 0.06 | 314.43 (114.42) | 49.89 (73.27) | - |
| T2D + CKD | 3035 | 2371.61 | 0.13 | 285.22 (134.50) | 56.44 (73.07) | 2.01 (1.79–2.27) | |
| T2D + HF | 1012 | 715.87 | 0.32 | 258.19 (147.54) | 66.06 (90.34) | 2.88 (2.41–3.44) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavina, C.; Carvalho, D.S.; Dias, D.M.; Bernardo, F.; Martinho, H.; Couceiro, J.; Santos-Araújo, C.; Dinis-Oliveira, R.J.; Taveira-Gomes, T. Premature Mortality in Type 2 Diabetes Mellitus Associated with Heart Failure and Chronic Kidney Disease: 20 Years of Real-World Data. J. Clin. Med. 2022, 11, 2131. https://doi.org/10.3390/jcm11082131
Gavina C, Carvalho DS, Dias DM, Bernardo F, Martinho H, Couceiro J, Santos-Araújo C, Dinis-Oliveira RJ, Taveira-Gomes T. Premature Mortality in Type 2 Diabetes Mellitus Associated with Heart Failure and Chronic Kidney Disease: 20 Years of Real-World Data. Journal of Clinical Medicine. 2022; 11(8):2131. https://doi.org/10.3390/jcm11082131
Chicago/Turabian StyleGavina, Cristina, Daniel Seabra Carvalho, Daniel Martinho Dias, Filipa Bernardo, Hugo Martinho, João Couceiro, Carla Santos-Araújo, Ricardo Jorge Dinis-Oliveira, and Tiago Taveira-Gomes. 2022. "Premature Mortality in Type 2 Diabetes Mellitus Associated with Heart Failure and Chronic Kidney Disease: 20 Years of Real-World Data" Journal of Clinical Medicine 11, no. 8: 2131. https://doi.org/10.3390/jcm11082131