
Long-Term Efficacy and Safety of Rifaximin in Japanese Patients with Hepatic Encephalopathy: A Multicenter Retrospective Study
 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Ethics
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
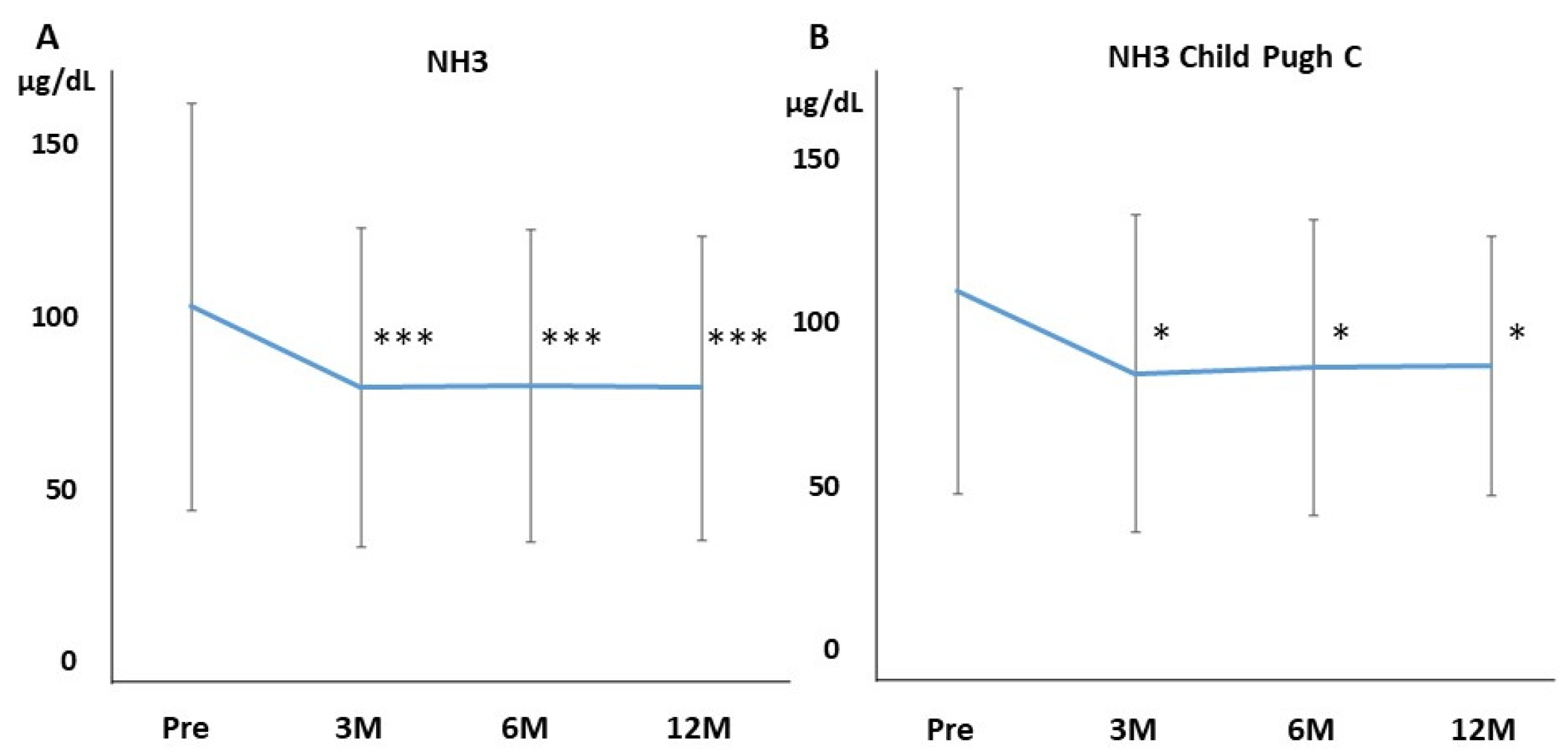
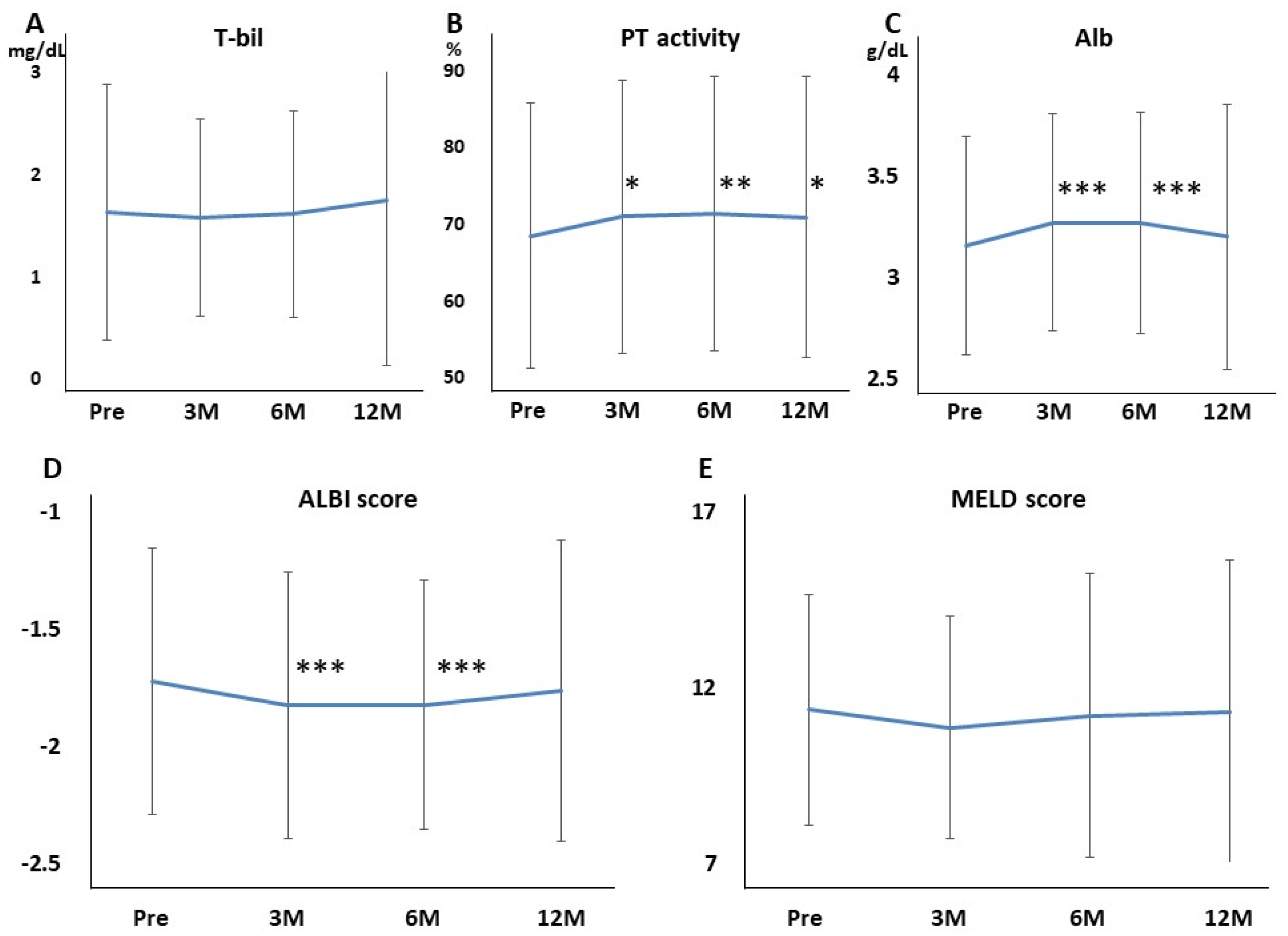
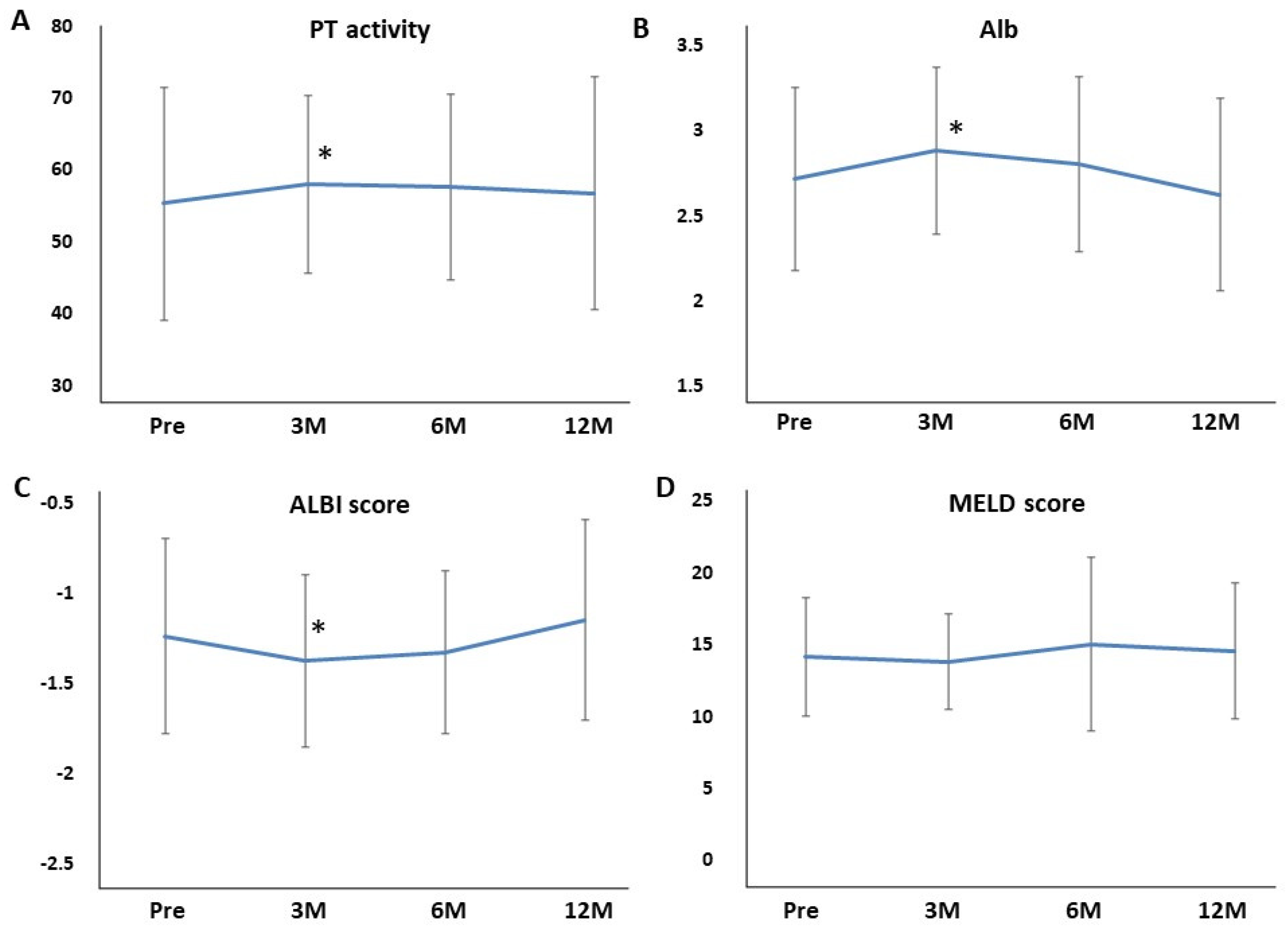
3.2. Efficacy of Long-Term Rifaximin Use
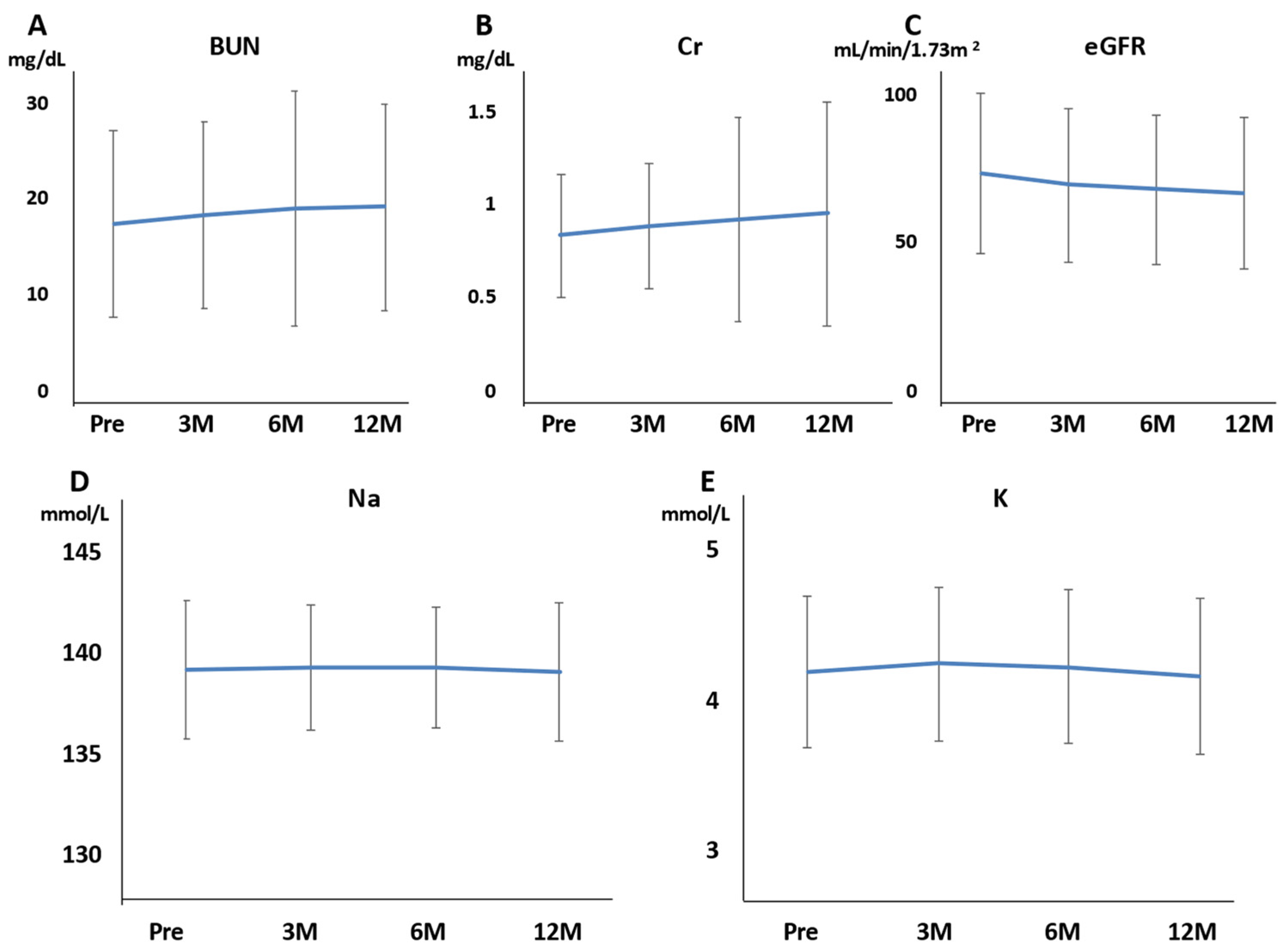
3.3. Safety of Long-Term Rifaximin Use
3.4. The Efficacy and Safety of Long-Term Rifaximin Use in Patients with Child–Pugh C
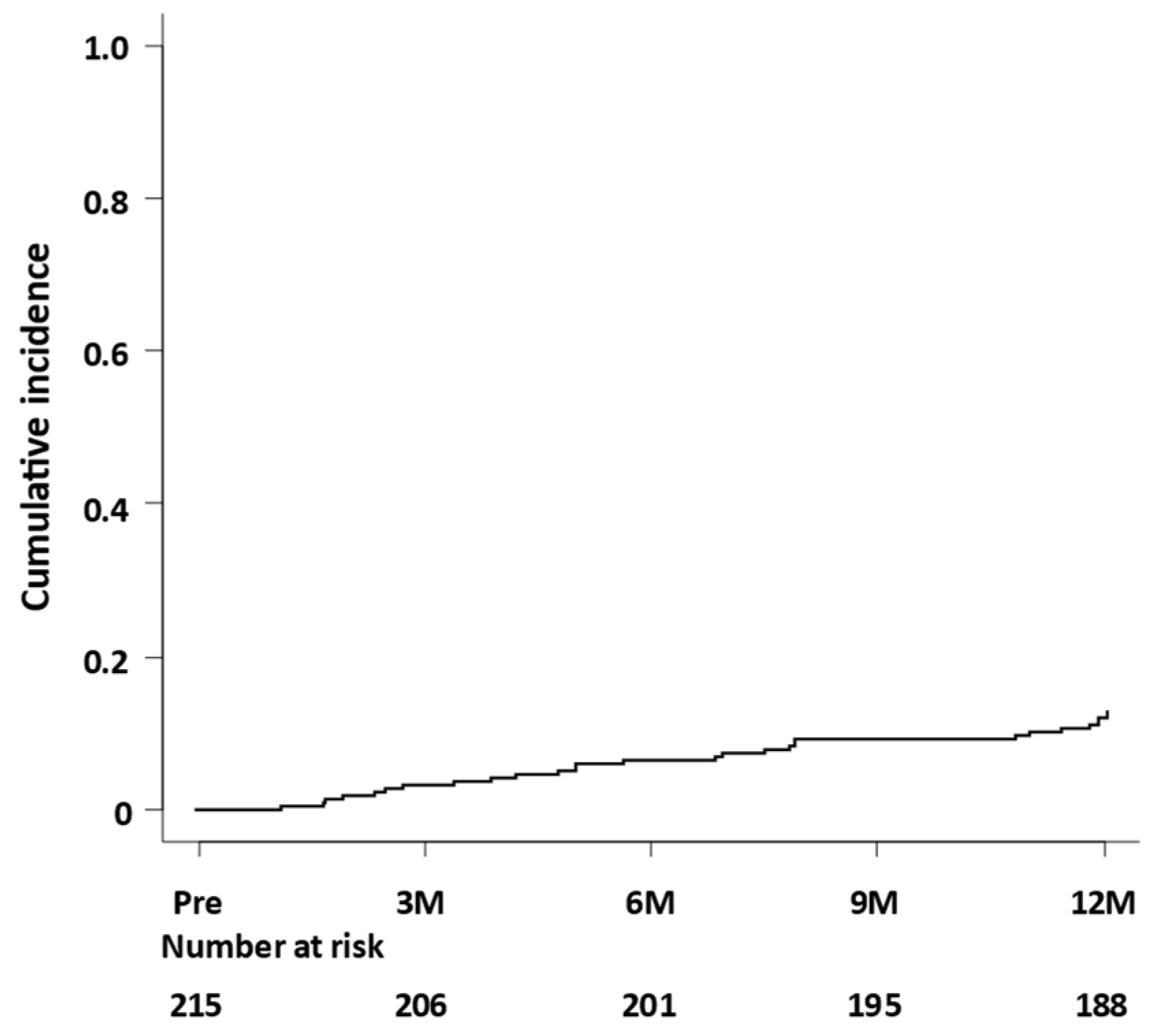
3.5. Risk Factors of HE Occurrence during Rifaximin Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic encephalopathy definition, nomenclature, diagnosis, and quantification. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Atluri, D.K.; Prakash, R.; Mullen, K.D. Pathogenesis, diagnosis, and treatment of hepatic encephalopathy. J. Clin. Exp. Hepatol. 2011, 1, 77–86. [Google Scholar] [CrossRef] [Green Version]
- American Association for the Study of Liver Diseases; European Association for the Study of the Liver. Hepatic enceph-alopathy in chronic liver disease: 2014 practice guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef] [Green Version]
- Conn, H.O. Trail making and number-connection tests in the assessment of mental state in portal systemic encephalopathy. Am. J. Dig. Dis. 1977, 22, 541–550. [Google Scholar] [CrossRef]
- Greinert, R.; Zipprich, A.; Simón-Talero, M.; Stangl, F.; Ludwig, C.; Wienke, A.; Praktiknjo, M.; Höhne, K.; Trebicka, J.; Genescà, J.; et al. Covert hepatic encephalopathy and spontaneous portosystemic shunts increase the risk of developing overt hepatic encephalopathy. Liver Int. 2020, 40, 3093–3102. [Google Scholar] [CrossRef] [PubMed]
- Yoshiji, H.; Nagoshi, S.; Akahane, T.; Asaoka, Y.; Ueno, Y.; Ogawa, K.; Kawaguchi, T.; Kurosaki, M.; Sakaida, I.; Shimizu, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2020. Hepatol. Res. 2021, 51, 725–749. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Scaldaferri, F.; Petito, V.; Paroni Sterbini, F.; Pecere, S.; Lopetuso, L.R.; Palladini, A.; Gerardi, V.; Masucci, L.; Pompili, M.; et al. The Role of Antibiotics in Gut Microbiota Modulation: The Eubiotic Effects of Rifaximin. Dig. Dis. 2016, 34, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Kimer, N.; Krag, A.; Moller, S.; Bendtsen, F.; Gluud, L.L. Systematic review with meta-analysis: The effects of rifaximin in hepatic encephalopathy. Aliment. Pharmacol. Ther. 2014, 40, 123–132. [Google Scholar] [CrossRef]
- Bass, N.M.; Mullen, K.D.; Sanyal, A. Rifaximin treatment in hepatic encephalopathy. N. Engl. J. Med. 2010, 362, 1071–1081. [Google Scholar] [CrossRef] [Green Version]
- Mas, A.; Rodés, J.; Sunyer, L.; Rodrigo, L.; Planas, R.; Vargas, V.; Castells, L.; Rodríguez-Martínez, D.; Fernández-Rodríguez, C.; Coll, I.; et al. Comparison of rifaximin and lactitol in the treatment of acute hepatic encephalopathy: Results of a randomized, double-blind, double-dummy, controlled clinical trial. J. Hepatol. 2003, 38, 51–58. [Google Scholar] [CrossRef]
- Mullen, K.D.; Sanyal, A.J.; Bass, N.M.; Poordad, F.F.; Sheikh, M.Y.; Frederick, T.; Bortey, E.; Forbes, W.P. Rifaximin Is Safe and Well Tolerated for Long-term Maintenance of Remission From Overt Hepatic Encephalopathy. Clin. Gastroenterol. Hepatol. 2014, 12, 1390–1397.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, K.; Endo, R.; Takikawa, Y.; Moriyasu, F.; Aoyagi, Y.; Moriwaki, H.; Terai, S.; Sakaida, I.; Sakai, Y.; Nishiguchi, S.; et al. Efficacy and safety of rifaximin in Japanese patients with hepatic encephalopathy: A phase II/III, multicenter, randomized, evaluator-blinded, active-controlled trial and a phase III, multicenter, open trial. Hepatol. Res. 2017, 48, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Endo, S.; Imai, M.; Azumi, M.; Nozawa, Y.; Sano, T.; Iwanaga, A.; Honma, T.; Yoshida, T. Changes in the body composition and nutritional status after long-term rifaximin therapy for hyperammonemia in Japanese patients with hepatic encephalopathy. Intern. Med. 2020, 59, 2465–2469. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Sezaki, H.; Suzuki, F.; Kasuya, K.; Sano, T.; Fujiyama, S.; Kawamura, Y.; Hosaka, T.; Akuta, N.; Saitoh, S.; et al. Real-world effects of long-term rifaximin treatment for Japanese patients with hepatic encephalopathy. Hepatol. Res. 2019, 49, 1406–1413. [Google Scholar] [CrossRef] [PubMed]
- Nishida, S.; Hamada, K.; Nishino, N.; Fukushima, D.; Koyanagi, R.; Horikawa, Y.; Shiwa, Y.; Saitoh, S. Efficacy of long-term rifaximin treatment for hepatic encephalopathy in the Japanese. World J. Hepatol. 2019, 11, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Hiramine, Y.; Uto, H.; Mawatari, S.; Kanmura, S.; Imamura, Y.; Hiwaki, T.; Saishoji, A.; Kakihara, A.; Maenohara, S.; Tokushige, K.; et al. Efficacy of rifaximin, a poorly absorbed rifamycin antimicrobial agent, for hepatic encephalopathy in Japanese patients. Hepatol. Res. 2021, 51, 445–460. [Google Scholar] [CrossRef] [PubMed]
- Testa, R.; Eftimiadi, C.; Sukkar, G.S.; De Leo, C.; Rovida, S.; Schito, G.C.; Celle, G. A non-absorbable rifamycin for treatment of hepatic encephalopathy. Drugs Under Exp. Clin. Res. 1985, 11, 387–392. [Google Scholar]
- Kaji, K.; Takaya, H.; Saikawa, S.; Furukawa, M.; Sato, S.; Kawaratani, H.; Kitade, M.; Moriya, K.; Namisaki, T.; Akahane, T.; et al. Rifaximin ameliorates hepatic encephalopathy and endotoxemia without affecting the gut microbiome diversity. World J. Gastroenterol. 2017, 23, 8355–8366. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S. The role of microbiota in hepatic encephalopathy. Gut Microbes 2014, 5, 397–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conn, H.O.; Liberathal, M.M. The Hepatic Coma Syndromes and Lactulose; Williams and Wilkins: Philadelphia, PA, USA, 1979; pp. 1–121. [Google Scholar]
- Lockwood, A.H. Blood Ammonia Levels and Hepatic Encephalopathy. Metab. Brain Dis. 2004, 19, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Citro, V.; Milan, G.; Tripodi, F.S.; Gennari, A.; Sorrentino, P.; Gallotta, G.; Postiglione, A.; Tarantino, G. Mental status impairment in patients with West Haven grade zero hepatic encephalopathy: The role of HCV infection. J. Gastroenterol. 2007, 42, 79–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Miwa, T.; Maeda, T.; Ogiso, Y.; Imai, A.; Suetsugu, A.; Takai, K.; Shimizu, M. Usefulness of the Stroop Test in diagnosing minimal hepatic encephalopathy and predicting overt hepatic encephalopathy. Hepatol. Commun. 2021, 5, 1518–1526. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Okusaka, T.; Mitsunaga, S.; Ueno, H.; Tamai, T.; Suzuki, T.; Hayato, S.; Kadowaki, T.; Okita, K.; Kumada, H. Safety and pharmacokinetics of lenvatinib in patients with advanced hepato-cellular carcinoma. Clin. Cancer Res. 2016, 22, 1385–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, M.; Kawaoka, T.; Aikata, H.; Kodama, K.; Uchikawa, S.; Ohya, K.; Morio, K.; Fujino, H.; Nakahara, T.; Murakami, E.; et al. Percutaneous transvenous shunt occlusion for portosystemic encephalopathy due to lenvatinib administration to a patient with hepatocellular carcinoma and portosystemic shunt. Clin. J. Gastroenterol. 2019, 12, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Meng, Y.; Xiao, W.; Wang, H.; Sun, L.; Fu, Z.; Xiong, X.; Zhang, S. Hepatic encephalopathy induced by Lenvatinib and anti-PD-1 mAb in a patient with ad-vanced hepatocellular carcinoma: A case report. Mol. Clin. Oncol. 2021, 14, 110. [Google Scholar] [CrossRef] [PubMed]
- Narita, R.; Kotoh, K.; Yoneda, A.; Motomura, M.; Harada, M. Factors Raising Serum Ammonia Level During Lenvatinib Treatment of Patients With Hepatocellular Carcinoma. Anticancer Res. 2020, 40, 5271–5276. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first line treatment of patients with unresectable hepatocel-lular carcinoma: A randomized phase 3 non inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- De Marco, F.; Santamaria, A.; D’arienzo, A. Rifaximin in collateral treatment of portal-systemic encephalopathy: A prelimi-nary report. Curr. Ther. Res. 1984, 36, 668–674. [Google Scholar]
- Jiang, Q.; Jiang, X.H.; Zheng, M.H.; Jiang, L.M.; Chen, Y.P.; Wang, L. Rifaximin versus nonabsorbable disaccharides in the man-agement of hepatic encephalopathy: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2008, 20, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Sharma, B.C.; Agrawal, A.; Sarin, S.K. Primary prophylaxis of overt hepatic encephalopathy in patients with cir-rhosis: An open labeled randomized controlled trial of lactulose versus no lactulose. J. Gastroenterol. Hepatol. 2012, 27, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Leevy, C.B.; Phillips, J.A. Hospitalizations during the use of rifaximin versus lactulose for the treatment of hepatic encepha-lopathy. Dig. Dis. Sci. 2007, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.C.; Sharma, P.; Lunia, M.K.; Srivastava, S.; Goyal, R.; Sarin, S.K. A Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic Encephalopathy. Am. J. Gastroenterol. 2013, 108, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Kudo, M. ALBI Score as a novel tool in staging and treatment planning for hepato-cellular carcinoma: Advantage of ALBI grade for universal assessment of hepatic function. Liver Cancer 2017, 6, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2015, 31, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Kudo, M. Newly Proposed ALBI Grade and ALBI-T Score as Tools for Assessment of Hepatic Function and Prognosis in Hepatocellular Carcinoma Patients. Liver Cancer 2018, 8, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Kim, W.R. Advanced liver disease study group. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Tokumoto, Y.; Joko, K.; Michitaka, K.; Mashiba, T.; Hiraoka, A.; Ochi, H.; Koizumi, Y.; Tada, F.; Hirooka, M.; et al. Effects of long-term entecavir treatment on the incidence of hepatocellular car-cinoma in chronic hepatitis B patients. Hepatol. Int. 2016, 10, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Tahata, Y.; Hikita, H.; Mochida, S.; Kawada, N.; Enomoto, N.; Ido, A.; Yoshiji, H.; Miki, D.; Hiasa, Y.; Takikawa, Y.; et al. Sofosbuvir plus velpatasvir treatment for hepatitis C virus in patients with de-compensated cirrhosis: A Japanese real-world multicenter study. J. Gastroenterol. 2021, 56, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Oshita, K.; Ohira, M.; Honmyo, N.; Kobayashi, T.; Murakami, E.; Aikata, H.; Baba, Y.; Kawano, R.; Awai, K.; Chayama, K.; et al. Treatment outcomes after splenectomy with gastric devascularization or bal-loon-occluded retrograde transvenous obliteration for gastric varices: A propensity score-weighted analysis from a single institution. J. Gastroenterol. 2020, 55, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, G.; Jesudian, A.B. Small Intestinal Bacterial Overgrowth in Patients with Cirrhosis. J. Clin. Exp. Hepatol. 2018, 9, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Ostberg, T.; Bertilsson, G.; Jendeberg, L.; Berkenstam, A.; Uppenberg, J. Identification of residues in the PXR ligand binding domain critical for species specific and constitutive activation. JBIC J. Biol. Inorg. Chem. 2002, 269, 4896–4904. [Google Scholar] [CrossRef] [PubMed]
- Kliewer, S.A.; Goodwin, B.; Willson, T.M. The Nuclear Pregnane X Receptor: A Key Regulator of Xenobiotic Metabolism. Endocr. Rev. 2002, 23, 687–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mencarelli, A.; Renga, B.; Palladino, G.; Claudio, D.; Ricci, P.; Distrutti, E.; Barbanti, M.; Baldelli, F.; Fiorucci, S. Inhibition of NF-kB by a PXR-dependent pathway mediates counter-regulatory activities of rifaximin on innate immunity in intestinal epithelial cells. Eur. J. Pharmacol. 2011, 668, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.C.; Lee, S.; McPhail, M.J.W.; Da Silva, K.; Guilly, S.; Zamalloa, A.; Witherden, E.; Støy, S.; Vijay, G.K.M.; Pons, N.; et al. Rifaximin reduces gut-derived inflammation and mucin degradation in cirrhosis and encephalopathy: RIFSYS randomised controlled trial. J. Hepatol. 2021, 76, 332–342. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | (n = 215) |
|---|---|
| Age (years) | 69.7 ± 11.6 |
| Sex (male/female) | 138/77 |
| Body mass index (kg/m2) | 24.8 ± 4.7 |
| Etiology (HBV/HCV/Alcohol/NASH/others) | 22/37/66/29/61 |
| Child–Pugh (A/B/C) | 14/174/27 |
| History of hepatic encephalopathy (yes/no) | 163/52 |
| Presence of overt hepatic encephalopathy (yes/no) | 34/181 |
| Administration of lactulose (yes/no) | 116/99 |
| Presence of esophagogastric varices (yes/no) | 119/96 |
| Presence of a portosystemic shunt (yes/no/unknown) | 107/106/2 |
| Presence of splenomegaly (yes/no/splenectomy) | 160/54/1 |
| Presence of ascites (yes/no) | 79/136 |
| Presence of spontaneous bacterial peritonitis (yes/no) | 0/215 |
| Presence of hepatocellular carcinoma (yes/no) | 74/141 |
| Stage of hepatocellular carcinoma (1/2/3/4) | 27/30/11/6 |
| Variables | (n = 215) |
|---|---|
| Hemoglobin (g/dL) | 11.8 ± 2.1 |
| Platelet (×104/μL) | 10.9 ± 5.7 |
| Prothrombin activity (%) | 68.5 ± 17.3 |
| Serum albumin (g/dL) | 3.2 ± 0.5 |
| Aspartate aminotransferase (U/L) | 46.7 ± 24.9 |
| Alanine aminotransferase (U/L) | 29.7 ± 15.9 |
| Total bilirubin (mg/dL) | 1.6 ± 1.2 |
| Serum ammonia (μg/dL) | 102.9 ± 59.1 |
| Blood urine nitrogen (mg/dL) | 17.3 ± 9.7 |
| Serum creatine (mg/dL) | 0.8 ± 0.3 |
| Estimated glomerular filtration (mL/min/1.73 m2) | 72.8 ± 27.0 |
| Serum sodium (mEq/L) | 139.2 ± 3.4 |
| Serum potassium (mEq/L) | 4.2 ± 0.5 |
| ALBI score | −1.72 ± 0.57 |
| MELD score | 11.0 ± 3.3 |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (per year increase) | 1.00 (0.96–1.03) | 0.909 | ||
| Sex (male) | 0.52 (0.24–1.12) | 0.094 | 0.61 (0.27–1.37) | 0.234 |
| Etiology (HCV vs. except HCV) | 0.71 (0.28–1.78) | 0.464 | ||
| Child–Pugh C (vs. A, B) | 1.66 (0.63–4.41) | 0.307 | ||
| Presence of esophagogastric varices | 1.28 (0.58–2.82) | 0.542 | ||
| Presence of a portosystemic shunt | 2.42 (1.05–5.58) | 0.037 | 1.68 (0.68–4.13) | 0.262 |
| Presence of splenomegaly | 1.02 (0.41–2.56) | 0.965 | ||
| Presence of ascites | 1.21 (0.53–2.76) | 0.645 | ||
| Presence of HCC | 2.32 (0.87–6.15) | 0.091 | 1.92 (0.69–5.32) | 0.209 |
| Stage of HCC | 1.13 (0.49–2.94) | 0.724 | ||
| Alanine aminotransferase at baseline | 1.00 (0.97–1.02) | 0.735 | ||
| Blood urine nitrogen at baseline | 1.01 (0.98–1.05) | 0.548 | ||
| Creatinine at baseline | 1.33 (0.47–3.78) | 0.592 | ||
| Serum sodium at baseline | 1.06 (0.94–1.20) | 0.323 | ||
| Serum albumin at baseline | 0.44 (0.21–0.90) | 0.025 | 0.58 (0.23–1.44) | 0.241 |
| Total bilirubin at baseline | 1.14 (0.88–1.49) | 0.316 | ||
| Prothrombin activity at baseline | 0.96 (0.95–0.99) | <0.001 | 0.98 (0.95–1.00) | 0.049 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawaratani, H.; Kondo, Y.; Tatsumi, R.; Kawabe, N.; Tanabe, N.; Sakamaki, A.; Okumoto, K.; Uchida, Y.; Endo, K.; Kawaguchi, T.; et al. Long-Term Efficacy and Safety of Rifaximin in Japanese Patients with Hepatic Encephalopathy: A Multicenter Retrospective Study. J. Clin. Med. 2022, 11, 1571. https://doi.org/10.3390/jcm11061571
Kawaratani H, Kondo Y, Tatsumi R, Kawabe N, Tanabe N, Sakamaki A, Okumoto K, Uchida Y, Endo K, Kawaguchi T, et al. Long-Term Efficacy and Safety of Rifaximin in Japanese Patients with Hepatic Encephalopathy: A Multicenter Retrospective Study. Journal of Clinical Medicine. 2022; 11(6):1571. https://doi.org/10.3390/jcm11061571
Chicago/Turabian StyleKawaratani, Hideto, Yasuteru Kondo, Ryoji Tatsumi, Naoto Kawabe, Norikazu Tanabe, Akira Sakamaki, Kazuo Okumoto, Yoshihito Uchida, Kei Endo, Takumi Kawaguchi, and et al. 2022. "Long-Term Efficacy and Safety of Rifaximin in Japanese Patients with Hepatic Encephalopathy: A Multicenter Retrospective Study" Journal of Clinical Medicine 11, no. 6: 1571. https://doi.org/10.3390/jcm11061571