
Dehydration Status at Admission Predicts Recurrence in Patients with Traumatic Chronic Subdural Hematoma

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Definition of Dehydration
2.3. Statistics
3. Results
3.1. Patient Characteristics
3.2. Dehydration Status at Admission
3.3. Risk of CSDH Recurrence
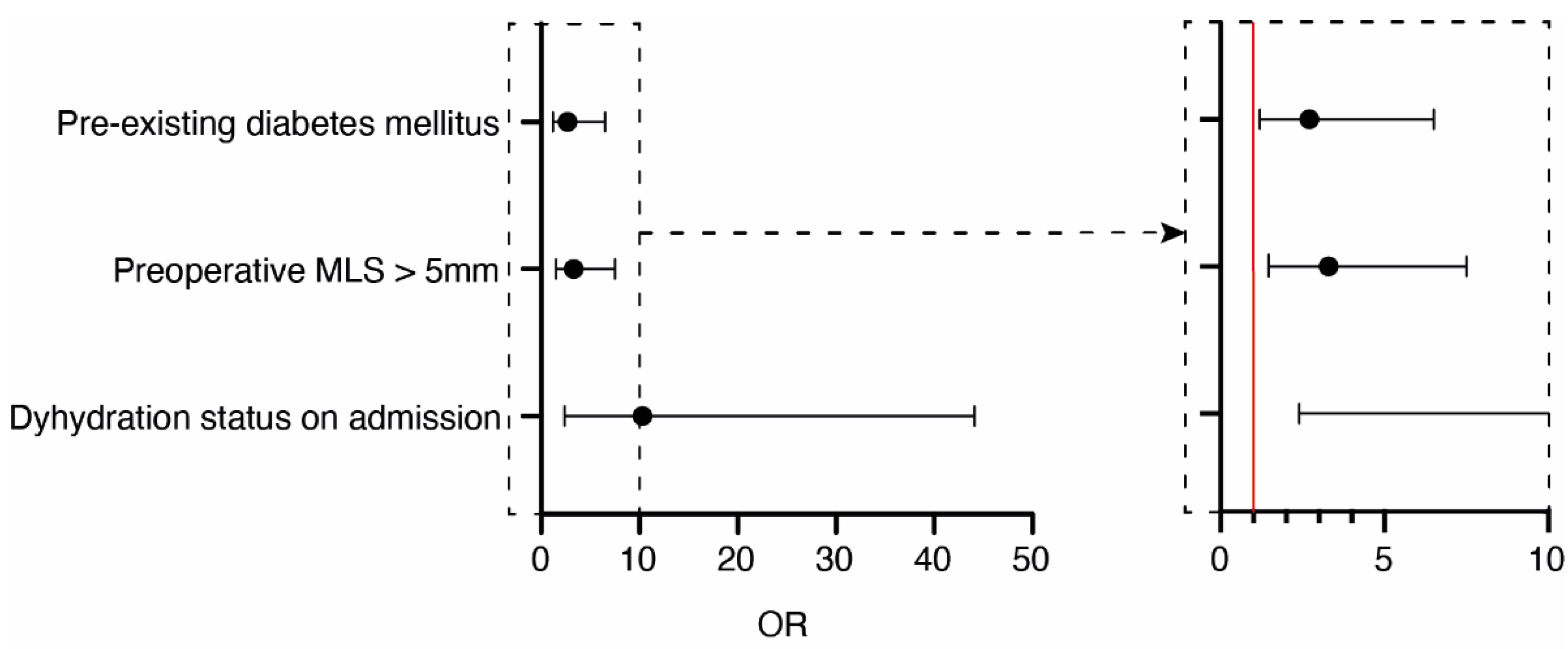
3.4. Multivariate Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kolias, A.G.; Chari, A.; Santarius, T.; Hutchinson, P.J. Chronic subdural haematoma: Modern management and emerging therapies. Nat. Rev. Neurol. 2014, 10, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Gazzeri, R.; Laszlo, A.; Faiola, A.; Colangeli, M.; Comberiati, A.; Bolognini, A.; Callovini, G. Clinical investigation of chronic subdural hematoma: Relationship between surgical approach, drainage location, use of antithrombotic drugs and postoperative recurrence. Clin. Neurol. Neurosurg. 2020, 191, 105705. [Google Scholar] [CrossRef] [PubMed]
- Cofano, F.; Pesce, A.; Vercelli, G.; Mammi, M.; Massara, A.; Minardi, M.; Palmieri, M.; D’Andrea, G.; Fronda, C.; Lanotte, M.M.; et al. Risk of Recurrence of Chronic Subdural Hematomas After Surgery: A Multicenter Observational Cohort Study. Front. Neurol. 2020, 11, 560269. [Google Scholar] [CrossRef]
- Maughan, R.J. Hydration, morbidity, and mortality in vulnerable populations. Nutr. Rev. 2012, 70 (Suppl. 2), S152–S155. [Google Scholar] [CrossRef] [PubMed]
- Shirreffs, S.M. Markers of hydration status. Eur. J. Clin. Nutr. 2003, 57 (Suppl. 2), S6–S9. [Google Scholar] [CrossRef]
- Stookey, J.D.; Purser, J.L.; Pieper, C.F.; Cohen, H.J. Plasma hypertonicity: Another marker of frailty? J. Am. Geriatr. Soc. 2004, 52, 1313–1320. [Google Scholar] [CrossRef]
- Manz, F.; Wentz, A. The importance of good hydration for the prevention of chronic diseases. Nutr. Rev. 2005, 63, S2–S5. [Google Scholar] [CrossRef] [PubMed]
- Ferry, M. Strategies for ensuring good hydration in the elderly. Nutr. Rev. 2005, 63, S22–S29. [Google Scholar] [CrossRef] [PubMed]
- Edlmann, E.; Giorgi-Coll, S.; Whitfield, P.C.; Carpenter, K.L.H.; Hutchinson, P.J. Pathophysiology of chronic subdural haematoma: Inflammation, angiogenesis and implications for pharmacotherapy. J. Neuroinflamm. 2017, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Komai, T.; Yamamoto, S. Fibrinolytic enzyme in the lining walls of chronic subdural hematoma. J. Neurosurg. 1978, 48, 197–200. [Google Scholar] [CrossRef]
- Murakami, H.; Hirose, Y.; Sagoh, M.; Shimizu, K.; Kojima, M.; Gotoh, K.; Mine, Y.; Hayashi, T.; Kawase, T. Why do chronic subdural hematomas continue to grow slowly and not coagulate? Role of thrombomodulin in the mechanism. J. Neurosurg. 2002, 96, 877–884. [Google Scholar] [CrossRef]
- Hohenstein, A.; Erber, R.; Schilling, L.; Weigel, R. Increased mRNA expression of VEGF within the hematoma and imbalance of angiopoietin-1 and -2 mRNA within the neomembranes of chronic subdural hematoma. J. Neurotrauma 2005, 22, 518–528. [Google Scholar] [CrossRef]
- Nakagawa, T.; Kodera, T.; Kubota, T. Expression of matrix metalloproteinases in the chronic subdural haematoma membrane. Acta Neurochir. 2000, 142, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Dmitrieva, N.I.; Burg, M.B. Elevated sodium and dehydration stimulate inflammatory signaling in endothelial cells and promote atherosclerosis. PLoS ONE 2015, 10, e0128870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.R.; Lee, K.S.; Shim, J.J.; Yoon, S.M.; Bae, H.G.; Doh, J.W. Multiple Densities of the Chronic Subdural Hematoma in CT Scans. J. Korean Neurosurg. Soc. 2013, 54, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Lacey, J.; Corbett, J.; Forni, L.; Hooper, L.; Hughes, F.; Minto, G.; Moss, C.; Price, S.; Whyte, G.; Woodcock, T.; et al. A multidisciplinary consensus on dehydration: Definitions, diagnostic methods and clinical implications. Ann. Med. 2019, 51, 232–251. [Google Scholar] [CrossRef] [PubMed]
- Eizenberg, Y.; Grossman, E.; Tanne, D.; Koton, S. Admission Hydration Status and Ischemic Stroke Outcome-Experience from a National Registry of Hospitalized Stroke Patients. J. Clin. Med. 2021, 10, 3292. [Google Scholar] [CrossRef]
- Rowat, A.; Graham, C.; Dennis, M. Dehydration in hospital-admitted stroke patients: Detection, frequency, and association. Stroke 2012, 43, 857–859. [Google Scholar] [CrossRef] [Green Version]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. Biom. Z. 2018, 60, 431–449. [Google Scholar] [CrossRef] [Green Version]
- Stavrinou, P.; Katsigiannis, S.; Lee, J.H.; Hamisch, C.; Krischek, B.; Mpotsaris, A.; Timmer, M.; Goldbrunner, R. Risk Factors for Chronic Subdural Hematoma Recurrence Identified Using Quantitative Computed Tomography Analysis of Hematoma Volume and Density. World Neurosurg. 2017, 99, 465–470. [Google Scholar] [CrossRef]
- Jack, A.; O’Kelly, C.; McDougall, C.; Findlay, J.M. Predicting recurrence after chronic subdural haematoma drainage. Can. J. Neurol. Sci. 2015, 42, 34–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, H.; Hirashima, Y.; Hamada, H.; Hayashi, N.; Origasa, H.; Endo, S. Independent predictors of recurrence of chronic subdural hematoma: Results of multivariate analysis performed using a logistic regression model. J. Neurosurg. 2003, 98, 1217–1221. [Google Scholar] [CrossRef] [PubMed]
- Unterhofer, C.; Freyschlag, C.F.; Thome, C.; Ortler, M. Opening the Internal Hematoma Membrane Does Not Alter the Recurrence Rate of Chronic Subdural Hematomas: A Prospective Randomized Trial. World Neurosurg. 2016, 92, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Majovsky, M.; Masopust, V.; Netuka, D.; Benes, V. Flexible endoscope-assisted evacuation of chronic subdural hematomas. Acta Neurochir. 2016, 158, 1987–1992. [Google Scholar] [CrossRef] [PubMed]
- Song, D.H.; Kim, Y.S.; Chun, H.J.; Yi, H.J.; Bak, K.H.; Ko, Y.; Oh, S.J. The Predicting Factors for Recurrence of Chronic Subdural Hematoma Treated with Burr Hole and Drainage. Korean J. Neurotrauma 2014, 10, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujitani, S.; Ishikawa, O.; Miura, K.; Takeda, Y.; Goto, H.; Maeda, K. Factors predicting contralateral hematoma growth after unilateral drainage of bilateral chronic subdural hematoma. J. Neurosurg. 2017, 126, 755–759. [Google Scholar] [CrossRef]
- Hani, L.; Vulcu, S.; Branca, M.; Fung, C.; Z’Graggen, W.J.; Murek, M.; Raabe, A.; Beck, J.; Schucht, P. Subdural versus subgaleal drainage for chronic subdural hematomas: A post hoc analysis of the TOSCAN trial. J. Neurosurg. 2019, 133, 11147–11155. [Google Scholar] [CrossRef]
- Bartley, A.; Jakola, A.S.; Tisell, M. The influence of irrigation fluid temperature on recurrence in the evacuation of chronic subdural hematoma. Acta Neurochir. 2020, 162, 485–488. [Google Scholar] [CrossRef] [Green Version]
- Leroy, H.A.; Aboukais, R.; Reyns, N.; Bourgeois, P.; Labreuche, J.; Duhamel, A.; Lejeune, J.P. Predictors of functional outcomes and recurrence of chronic subdural hematomas. J. Clin. Neurosci. 2015, 22, 1895–1900. [Google Scholar] [CrossRef]
- Borger, V.; Vatter, H.; Oszvald, A.; Marquardt, G.; Seifert, V.; Guresir, E. Chronic subdural haematoma in elderly patients: A retrospective analysis of 322 patients between the ages of 65–94 years. Acta Neurochir. 2012, 154, 1549–1554. [Google Scholar] [CrossRef]
- Gelabert-Gonzalez, M.; Iglesias-Pais, M.; Garcia-Allut, A.; Martinez-Rumbo, R. Chronic subdural haematoma: Surgical treatment and outcome in 1000 cases. Clin. Neurol. Neurosurg. 2005, 107, 223–229. [Google Scholar] [CrossRef]
- Uno, M.; Toi, H.; Hirai, S. Chronic Subdural Hematoma in Elderly Patients: Is This Disease Benign? Neurol. Med. Chir. 2017, 57, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Fotenos, A.F.; Mintun, M.A.; Snyder, A.Z.; Morris, J.C.; Buckner, R.L. Brain volume decline in aging: Evidence for a relation between socioeconomic status, preclinical Alzheimer disease, and reserve. Arch. Neurol. 2008, 65, 113–120. [Google Scholar] [CrossRef]
- Jang, K.M.; Choi, H.H.; Mun, H.Y.; Nam, T.K.; Park, Y.S.; Kwon, J.T. Critical Depressed Brain Volume Influences the Recurrence of Chronic Subdural Hematoma after Surgical Evacuation. Sci. Rep. 2020, 10, 1145. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, K.; Brown, R.A.; Araujo, D.; Narayanan, S.; Arnold, D.L. Correlation between brain volume change and T2 relaxation time induced by dehydration and rehydration: Implications for monitoring atrophy in clinical studies. Neuroimage Clin. 2014, 6, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Elias, S.; Hoffman, R.; Saharov, G.; Brenner, B.; Nadir, Y. Dehydration as a Possible Cause of Monthly Variation in the Incidence of Venous Thromboembolism. Clin. Appl. Thromb. Hemost. 2016, 22, 569–574. [Google Scholar] [CrossRef]
- Hooper, L.; Bunn, D.K.; Downing, A.; Jimoh, F.O.; Groves, J.; Free, C.; Cowap, V.; Potter, J.F.; Hunter, P.R.; Shepstone, L. Which Frail Older People Are Dehydrated? The UK DRIE Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1341–1347. [Google Scholar] [CrossRef] [Green Version]
- Teno, J.M.; Gozalo, P.; Mitchell, S.L.; Tyler, D.; Mor, V. Survival after multiple hospitalizations for infections and dehydration in nursing home residents with advanced cognitive impairment. JAMA 2013, 310, 319–320. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.; Pei, L.; Gao, Y.; Zhao, L.; Fang, H.; Bunda, B.; Fisher, L.; Wang, Y.; Li, S.; Li, Y.; et al. Dehydration Status Predicts Short-Term and Long-Term Outcomes in Patients with Cerebral Venous Thrombosis. Neurocrit. Care 2019, 30, 478–483. [Google Scholar] [CrossRef]
- Montano, N.; Stifano, V.; Skrap, B.; Mazzucchi, E. Management of residual subdural hematoma after burr-hole evacuation. The role of fluid therapy and review of the literature. J. Clin. Neurosci. 2017, 46, 26–29. [Google Scholar] [CrossRef]
- Janowski, M.; Kunert, P. Intravenous fluid administration may improve post-operative course of patients with chronic subdural hematoma: A retrospective study. PLoS ONE 2012, 7, e35634. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Non-Dehydration (n = 256) | Dehydration (n = 9) | p-Value |
|---|---|---|---|
| Median age (IQR, yrs) | 79 (73–85) | 81 (74–86) | 0.71 |
| Female sex | 91 (36%) | 4 (44%) | 0.73 |
| Preoperative anticoagulant medication | 186 (73%) | 6 (67%) | 0.32 |
| Platelet inhibition | 23 (9%) | 2 (22%) | 0.2 |
| Vitamin K antagonists | 123 (48%) | 3 (33%) | 0.5 |
| Combination | 40 (16%) | 1 (11%) | 1.0 |
| Median Markwalder grading scale (IQR) | 1 (1–2) | 1 (0–1) | 0.07 |
| Median GCS (IQR) | 15 (14–15) | 15 (15–15) | 0.55 |
| Unilateral CSDH | 185 (72%) | 9 (100%) | 0.12 |
| Preoperative MLS > 5 mm | 94 (37%) | 5 (56%) | 0.30 |
| Presence of CSDH septations | 91 (36%) | 6 (67%) | 0.08 |
| BHC | 250 (98%) | 9 (100%) | 0.82 |
| Admission Na > 145 mmol/L | 7 (3%) | 1 (11%) | 0.24 |
| Admission eGFR < 30 mL/min | 6 (2%) | 9 (100%) | <0.0001 |
| Admission urea > 7.5 mmol/L | 58 (23%) | 6 (67%) | 0.007 |
| Recurrence of SDH | 27 (11%) | 5 (56%) | 0.002 |
| Median GOS at discharge (IQR) | 5 (4–5) | 5 (4–5) | 0.55 |
| Median mRS at discharge (IQR) | 1 (0–3) | 0 (0–1) | 0.1 |
| Variables | No CSDH Recurrence (n = 233) | CSDH Recurrence (n = 32) | p-Value |
|---|---|---|---|
| Median age (IQR, yrs) | 79 (73–85) | 80 (72–85) | 0.68 |
| Female sex | 85 (37%) | 10 (31%) | 0.70 |
| Pre-existing diabetes mellitus | 42 (18%) | 11 (34%) | 0.06 |
| Pre-existing arterial hypertonus | 140 (60%) | 20 (63%) | 0.85 |
| Preoperative anticoagulant medication | 171 (73%) | 21 (66%) | 0.40 |
| Platelet inhibition | 22 (9%) | 3 (9%) | 1.00 |
| Vitamin K antagonists | 112 (48%) | 14 (41%) | 0.71 |
| Combination | 37 (16%) | 4 (13%) | 0.80 |
| Median Markwalder grading scale (IQR) | 1 (1–2) | 1 (0–2) | 0.83 |
| Median GCS (IQR) | 15 (14–15) | 15 (14–15) | 0.31 |
| Admission U/Cr > 80 | 4 (2%) | 5 (16%) | 0.002 |
| Unilateral CSDH | 171 (73%) | 23 (72%) | 0.83 |
| Preoperative MLS > 5 mm | 79 (34%) | 20 (63%) | 0.003 |
| Presence of CSDH septations | 83 (36%) | 14 (44%) | 0.44 |
| BHC Length of hospital stay (IQR, days) | 228 (98%) 6 (4–9) | 31 (97%) 6 (4–10) | 0.54 0.86 |
| Median GOS at discharge (IQR) | 5 (4–5) | 5 (4–5) | 0.70 |
| Median mRS at discharge (IQR) | 1 (0–3) | 1 (0–3) | 0.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mainka, N.; Borger, V.; Hadjiathanasiou, A.; Hamed, M.; Potthoff, A.-L.; Vatter, H.; Schuss, P.; Schneider, M. Dehydration Status at Admission Predicts Recurrence in Patients with Traumatic Chronic Subdural Hematoma. J. Clin. Med. 2022, 11, 1178. https://doi.org/10.3390/jcm11051178
Mainka N, Borger V, Hadjiathanasiou A, Hamed M, Potthoff A-L, Vatter H, Schuss P, Schneider M. Dehydration Status at Admission Predicts Recurrence in Patients with Traumatic Chronic Subdural Hematoma. Journal of Clinical Medicine. 2022; 11(5):1178. https://doi.org/10.3390/jcm11051178
Chicago/Turabian StyleMainka, Niklas, Valeri Borger, Alexis Hadjiathanasiou, Motaz Hamed, Anna-Laura Potthoff, Hartmut Vatter, Patrick Schuss, and Matthias Schneider. 2022. "Dehydration Status at Admission Predicts Recurrence in Patients with Traumatic Chronic Subdural Hematoma" Journal of Clinical Medicine 11, no. 5: 1178. https://doi.org/10.3390/jcm11051178