
Severe Asthma, Telemedicine, and Self-Administered Therapy: Listening First to the Patient

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sadatsafavi, M.; Lynd, L.; Marra, C.; Carleton, B.; Tan, W.C.; Sullivan, S.; Fitzgerald, J.M. Direct Health Care Costs Associated with Asthma in British Columbia. Can. Respir. J. 2010, 17, 74–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Principe, S.; Benfante, A.; Calzetta, L.; Rogliani, P.; Scichilone, N. Age does not affect the efficacy of anti-IL-5/IL-5R in severe asthmatics. World Allergy Organ. J. 2019, 12, 100081. [Google Scholar] [CrossRef] [PubMed]
- Persaud, Y.K.; Portnoy, J.M. Ten Rules for Implementation of a Telemedicine Program to Care for Patients with Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Milne-Ives, M.; Lam, C.; Meinert, E. Digital Technologies for Monitoring and Improving Treatment Adherence in Children and Adolescents with Asthma: Scoping Review of Randomized Controlled Trials. JMIR Pediatr. Parent. 2021, 4, e27999. [Google Scholar] [CrossRef] [PubMed]
- Alida, B.; Stefania, P.; Noemi, C.M.; Maria, I.; Carmen, D.; Nicola, S. Management of severe asthma during the first lockdown phase of SARS-CoV-2 pandemic: Tips for facing the second wave. Pulm. Pharmacol. Ther. 2021, 102083. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, J.M.; Waller, M.; De Lurgio, S.; Dinakar, C. Telemedicine is as effective as in-person visits for patients with asthma. Ann. Allergy Asthma Immunol. 2016, 117, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Poowuttikul, P.; Seth, D. New Concepts and Technological Resources in Patient Education and Asthma Self-Management. Clin. Rev. Allergy Immunol. 2020, 59, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Snoswell, C.L.; Rahja, M.; Lalor, A.F. A Systematic Review and Meta-Analysis of Change in Health-Related Quality of Life for Interactive Telehealth Interventions for Patients with Asthma. Value Health 2021, 24, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, E.; Miao, B.; Pugliese, N.; Huang, D.; Sobieraj, D.M. Systematic Review of mHealth Applications That Interface with Inhaler Sensors in Asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 844–852.e3. [Google Scholar] [CrossRef] [PubMed]
- Caminati, M.; Vaia, R.; Furci, F.; Guarnieri, G.; Senna, G. Uncontrolled Asthma: Unmet Needs in the Management of Patients. J. Asthma Allergy 2021, 14, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Menzella, F.; Ferrari, E.; Ferrucci, S.M.; Lombardi, E.; Alfano, S.; Bonavita, O.; Morini, P.; Rizzi, A.; Matucci, A. Self-administration of omalizumab: Why not? A literature review and expert opinion. Expert Opin. Biol. Ther. 2021, 21, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Gouder, C.; Gouder, S.; Montefort, S. Self-reported satisfaction of patients receiving omalizumab for severe allergic asthma in Malta. Biologicals 2019, 60, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Juniper, E.; O′byrne, P.; Guyatt, G.; Ferrie, P.; King, D. Development and validation of a questionnaire to measure asthma control. Eur. Respir. J. 1999, 14, 902–907. [Google Scholar] [CrossRef]
- Seret, J.; Gooset, F.; Durieux, V.; Lecocq, D.; Pirson, M. What Means a Quality Professional-Patient Relationship from The Asthmatic Patients’ Perspective? A Narrative Review of Their Needs and Expectations. Patient Prefer. Adherence 2019, 13, 1951–1960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, K.; Bahana, S.L. Hypersensitivity and adverse reactions to biologics in asthma and allergic diseases. Expert Rev. Clin. Immunol. 2020, 16, 311–319. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Items | Extremely (% Patients) | Very Much (% Patients) | Moderately (% Patients) | A Little (% Patients) | Not at All (% Patients) | |
|---|---|---|---|---|---|---|
| 1 | Self-assessment of breathing and oxygen saturation, patient empowerment | 31 | 25 | 26 | 11 | 7 |
| 2 | Patient’s ability with technology | 27 | 28 | 28 | 12 | 5 |
| 3 | Satisfation to make a virtual visit | 30 | 27 | 20 | 16 | 7 |
| 4 | Perception to be properly followed-up by the doctor with telemedicine management | 21 | 24 | 31 | 15 | 9 |
| 5 | Preference of in-person versus virtual visit | 21 | 28 | 23 | 19 | 9 |
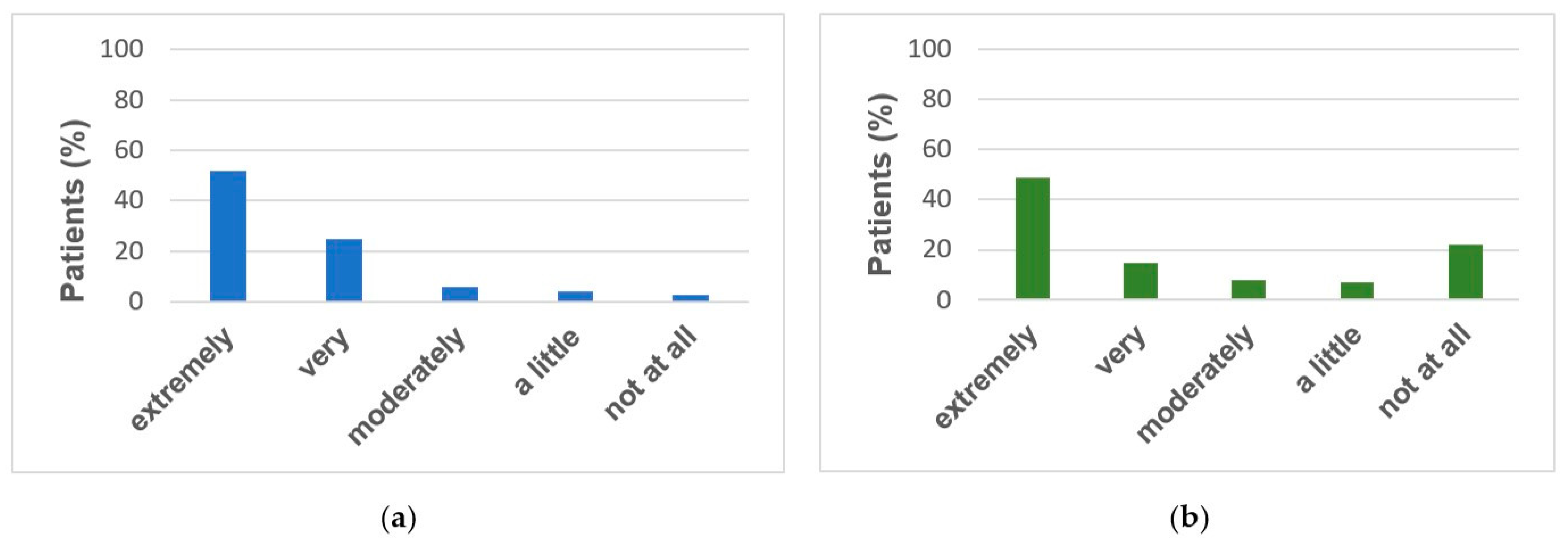
| 6 | Easy self-injection therapy at home | 52 | 25 | 16 | 4 | 3 |
| 7 | Safety and skill about the injection procedure | 50 | 31 | 13 | 5 | 1 |
| 8 | Feeling unanxious | 50 | 25 | 18 | 6 | 1 |
| 9 | Adverse events after self-injection | 49 | 15 | 8 | 7 | 22 |
| 10 | Easy syringe or injector | 60 | 27 | 7 | 0 | 6 |
| 11 | Recommendation to another severe asthma patient about self-injection | 54 | 32 | 10 | 1 | 3 |
| 12 | Clear training at clinic | 66 | 31 | 2 | 0 | 1 |
| 13 | Patient’s choice influenced by the COVID-19 pandemic | 19 | 13 | 17 | 17 | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarnieri, G.; Caminati, M.; Achille, A.; Vaia, R.; Chieco Bianchi, F.; Senna, G.; Vianello, A. Severe Asthma, Telemedicine, and Self-Administered Therapy: Listening First to the Patient. J. Clin. Med. 2022, 11, 960. https://doi.org/10.3390/jcm11040960
Guarnieri G, Caminati M, Achille A, Vaia R, Chieco Bianchi F, Senna G, Vianello A. Severe Asthma, Telemedicine, and Self-Administered Therapy: Listening First to the Patient. Journal of Clinical Medicine. 2022; 11(4):960. https://doi.org/10.3390/jcm11040960
Chicago/Turabian StyleGuarnieri, Gabriella, Marco Caminati, Alessia Achille, Rachele Vaia, Fulvia Chieco Bianchi, Gianenrico Senna, and Andrea Vianello. 2022. "Severe Asthma, Telemedicine, and Self-Administered Therapy: Listening First to the Patient" Journal of Clinical Medicine 11, no. 4: 960. https://doi.org/10.3390/jcm11040960