
Trajectory of Antidepressant Effects after Single- or Two-Dose Administration of Psilocybin: A Systematic Review and Multivariate Meta-Analysis

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
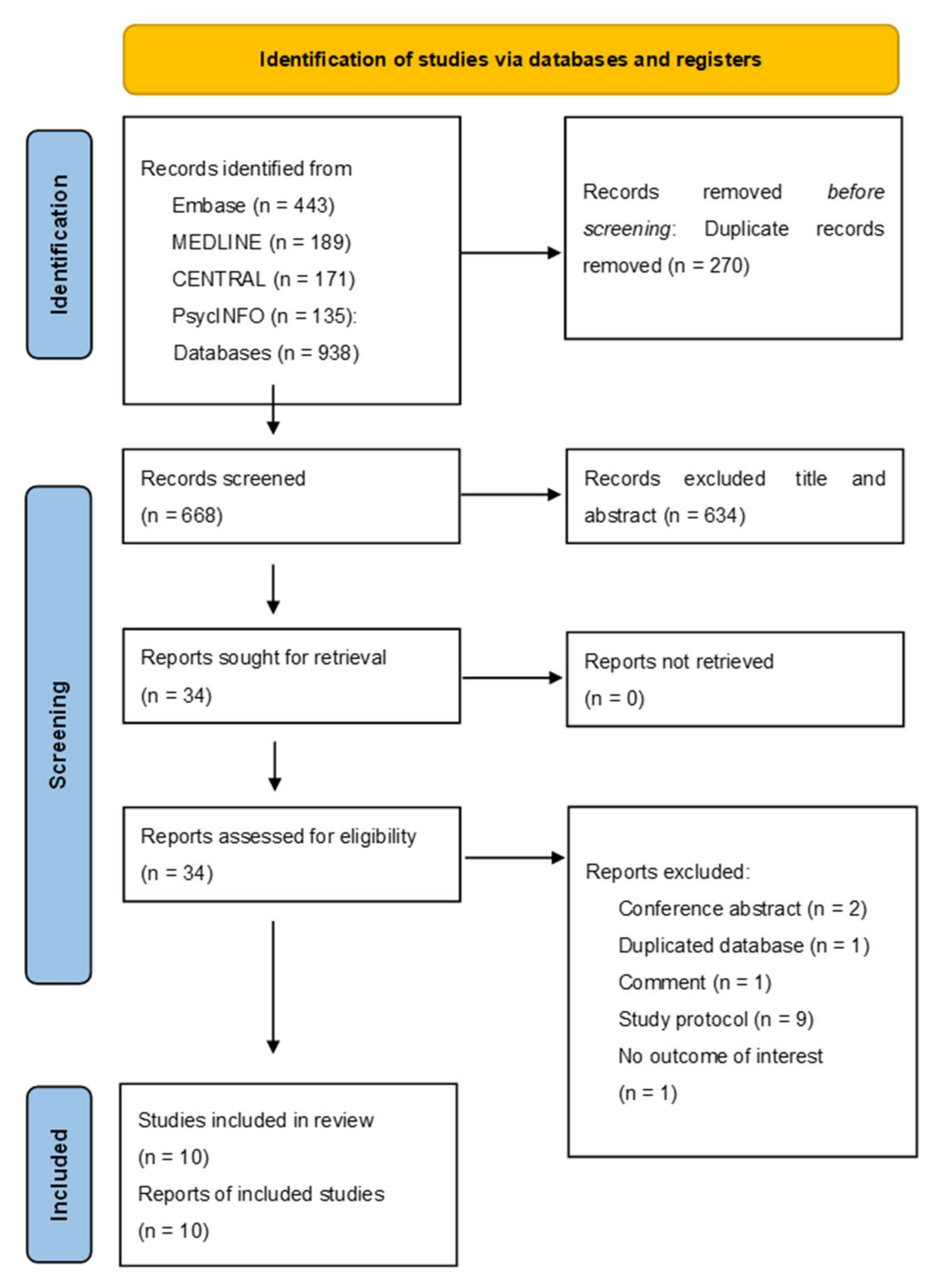
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Outcome Measures
2.4. Data Extraction and Risk of Bias Assessment
2.5. Data Synthesis
2.6. Meta-Regression and Subgroup Analysis
2.7. Publication Bias and Sensitivity Analysis
3. Results
3.1. Quality Assessment
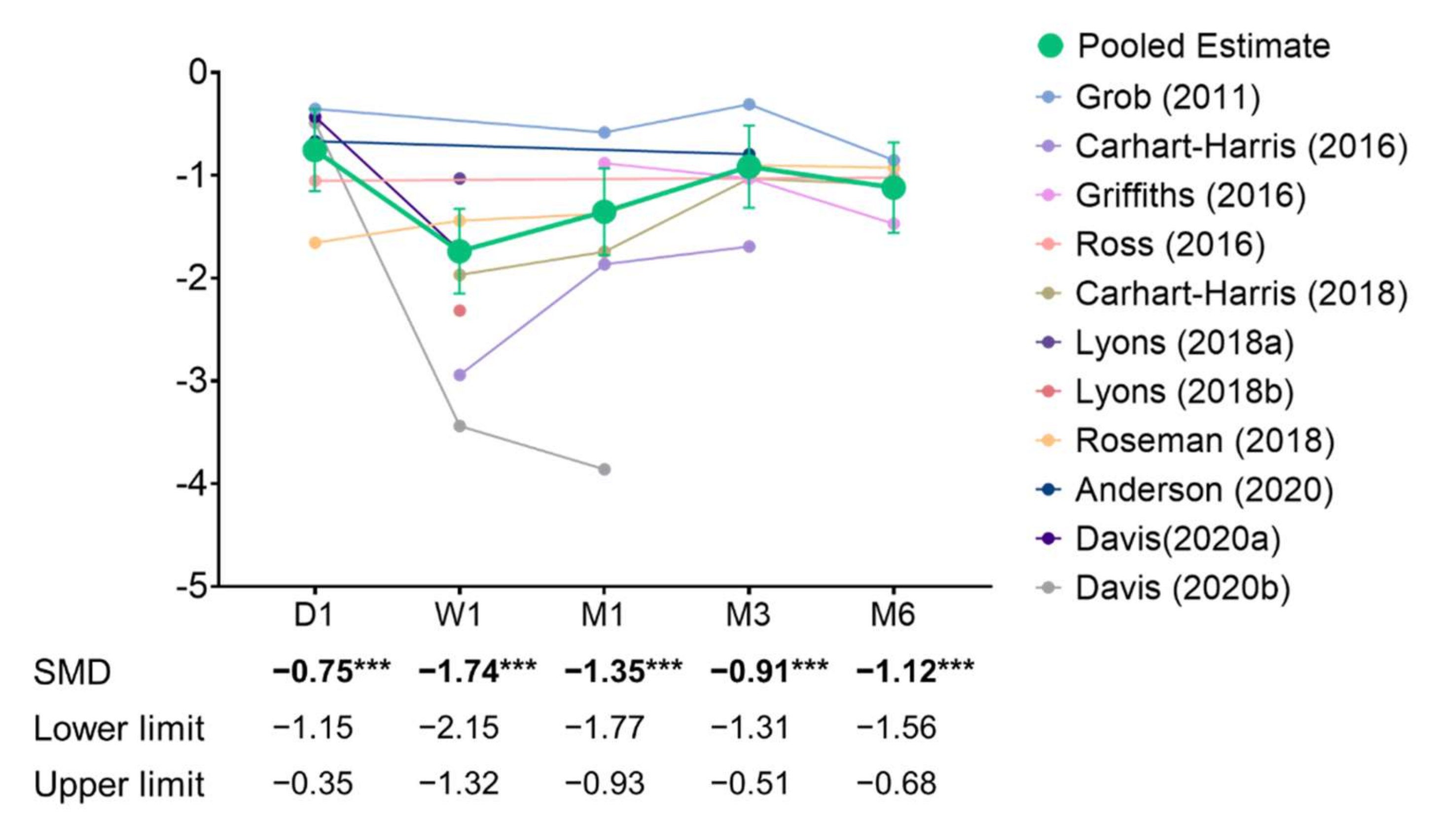
3.2. Primary Outcome: Depressive Symptoms
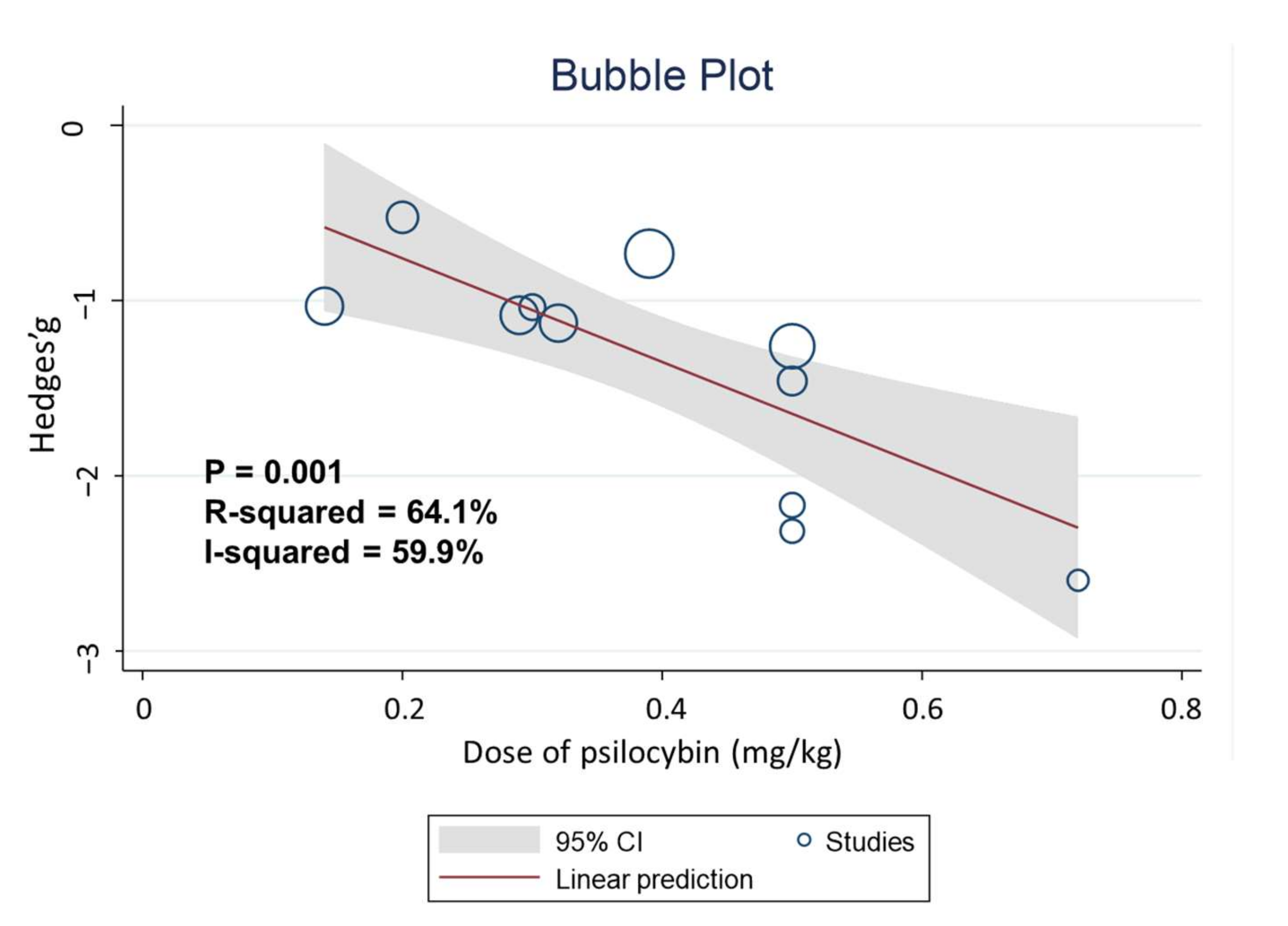
3.3. Meta-Regression and Subgroup Analyses of Primary Outcomes
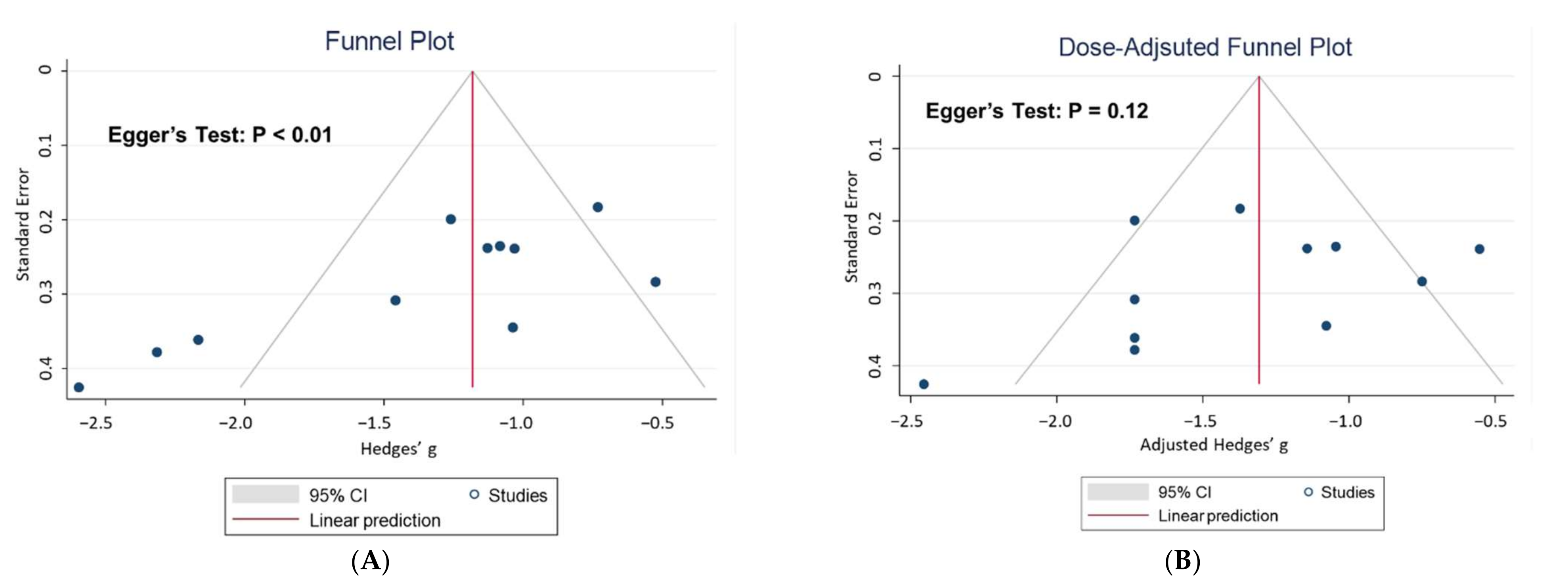
3.4. Publication Bias and Sensitivity Analyses
3.5. Secondary Outcomes: All-Cause Discontinuation, SBP, DBP, and HR Compared with Placebo
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Halberstadt, A.L. Recent advances in the neuropsychopharmacology of serotonergic hallucinogens. Behav. Brain Res. 2014, 277, 99–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M.W.; Griffiths, R.R.; Hendricks, P.S.; Henningfield, J.E. The abuse potential of medical psilocybin according to the 8 factors of the Controlled Substances Act. Neuropharmacology 2018, 142, 143–166. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.A.; Carhart-Harris, R.; Nutt, D.J.; Erritzoe, D. Therapeutic effects of classic serotonergic psychedelics: A systematic review of modern-era clinical studies. Acta Psychiatr. Scand. 2021, 143, 101–118. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.W.; Richards, W.A.; Griffiths, R.R. Human hallucinogen research: Guidelines for safety. J. Psychopharmacol. 2008, 22, 603–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Więckiewicz, G.; Stokłosa, I.; Piegza, M.; Gorczyca, P.; Pudlo, R. Lysergic Acid Diethylamide, Psilocybin and Dimethyltryptamine in Depression Treatment: A Systematic Review. Pharmaceuticals 2021, 14, 793. [Google Scholar] [CrossRef]
- Harvey, J.A. Role of the Serotonin 5-HT2A Receptor in Learning. Learn. Mem. 2003, 10, 355–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulougouris, V.; Glennon, J.C.; Robbins, T.W. Dissociable Effects of Selective 5-HT2A and 5-HT2C Receptor Antagonists on Serial Spatial Reversal Learning in Rats. Neuropsychopharmacology 2007, 33, 2007–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, R.G.; Hallak, J.E.; Baker, G.; Dursun, S. Hallucinogenic/psychedelic 5HT2A receptor agonists as rapid antidepressant therapeutics: Evidence and mechanisms of action. J. Psychopharmacol. 2021, 35, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; Stone, J.M.; Reed, L.J.; Colasanti, A.; Tyacke, R.J.; Leech, R.; Malizia, A.L.; Murphy, K.; et al. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc. Natl. Acad. Sci. USA 2012, 109, 2138–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvão-Coelho, N.L.; Marx, W.; Gonzalez, M.; Sinclair, J.; de Manincor, M.; Perkins, D.; Sarris, J. Classic serotonergic psychedelics for mood and depressive symptoms: A meta-analysis of mood disorder patients and healthy participants. Psychopharmacology 2021, 238, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Pace, B.T.; Nicholas, C.R.; Raison, C.L.; Hutson, P.R. The experimental effects of psilocybin on symptoms of anxiety and depression: A meta-analysis. Psychiatry Res. 2020, 284, 112749. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Shechet, B.; Nicholas, C.R.; Ng, C.W.; Deole, G.; Chen, Z.; Raison, C.L. Post-acute psychological effects of classical serotonergic psychedelics: A systematic review and meta-analysis. Psychol. Med. 2020, 50, 2655–2666. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Chwyl, C.; Bathje, G.J.; Davis, A.K.; Lancelotta, R. A Meta-Analysis of Placebo-Controlled Trials of Psychedelic-Assisted Therapy. J. Psychoact. Drugs 2020, 52, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Romeo, B.; Karila, L.; Martelli, C.; Benyamina, A. Efficacy of psychedelic treatments on depressive symptoms: A meta-analysis. J. Psychopharmacol. 2020, 34, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T.; Whiter, F.; Gallop, K.; Veronese, N.; Solmi, M.; Newton, P.; Stubbs, B. NMDA receptor antagonists and pain relief: A me-ta-analysis of experimental trials. Neurology 2019, 92, e1652–e1662. [Google Scholar] [CrossRef] [PubMed]
- Vargas, A.S.; Luís, Â.; Barroso, M.; Gallardo, E.; Pereira, L. Psilocybin as a new approach to treat depression and anxiety in the context of life-threatening diseases—a systematic review and meta-analysis of clinical trials. Biomedicines 2020, 8, 331. [Google Scholar] [CrossRef] [PubMed]
- Inserra, A.; De Gregorio, D.; Gobbi, G. Psychedelics in Psychiatry: Neuroplastic, Immunomodulatory, and Neurotransmitter Mechanisms. Pharmacol. Rev. 2020, 73, 202–277. [Google Scholar] [CrossRef]
- Agin-Liebes, G.I.; Malone, T.; Yalch, M.M.; Mennenga, S.E.; Ponté, K.L.; Guss, J.; Bossis, A.P.; Grigsby, J.; Fischer, S.; Ross, S. Long-term follow-up of psilocybin-assisted psychotherapy for psychiatric and existential distress in patients with life-threatening cancer. J. Psychopharmacol. 2020, 34, 155–166. [Google Scholar] [CrossRef]
- Anderson, B.T.; Danforth, A.; Daroff, R.; Stauffer, C.; Ekman, E.; Agin-Liebes, G.; Trope, A.; Boden, M.T.; Dilley, J.; Mitchell, J.; et al. Psilocybin-assisted group therapy for de-moralized older long-term AIDS survivor men: An open-label safety and feasibility pilot study. EClinicalMedicine 2020, 27, 100538. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.K.; Barrett, F.S.; May, D.G.; Cosimano, M.P.; Sepeda, N.D.; Johnson, M.W.; Finan, P.H.; Griffiths, R.R. Effects of psilocybin-assisted therapy on major depressive disorder: A randomized clinical trial. JAMA Psychiatry 2021, 78, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Lyons, T.; Carhart-Harris, R.L. More Realistic Forecasting of Future Life Events After Psilocybin for Treatment-Resistant Depression. Front. Psychol. 2018, 9, 1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roseman, L.; Nutt, D.J.; Carhart-Harris, R.L. Quality of Acute Psychedelic Experience Predicts Therapeutic Efficacy of Psilocybin for Treatment-Resistant Depression. Front. Pharmacol. 2018, 8, 974. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Baujat, B.; Mahé, C.; Pignon, J.-P.; Hill, C. A graphical method for exploring heterogeneity in meta-analyses: Application to a meta-analysis of 65 trials. Stat. Med. 2002, 21, 2641–2652. [Google Scholar] [CrossRef]
- Pustejovsky, J.E.; Tipton, E. Small-Sample Methods for Cluster-Robust Variance Estimation and Hypothesis Testing in Fixed Effects Models. J. Bus. Econ. Stat. 2017, 36, 672–683. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Bolstridge, M.; Day, C.M.J.; Rucker, J.; Watts, R.; Erritzoe, D.E.; Kaelen, M.; Giribaldi, B.; Bloomfield, M.; Pilling, S.; et al. Psilocybin with psychological support for treatment-resistant depression: Six-month follow-up. Psychopharmacology 2018, 235, 399–408. [Google Scholar] [CrossRef] [Green Version]
- Carhart-Harris, R.L.; Bolstridge, M.; Rucker, J.; Day, C.M.J.; Erritzoe, D.; Kaelen, M.; Bloomfield, M.; Rickard, J.A.; Forbes, B.; Feilding, A.; et al. Psilocybin with psychological support for treatment-resistant depression: An open-label feasibility study. Lancet Psychiatry 2016, 3, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef]
- Grob, C.S.; Danforth, A.L.; Chopra, G.S.; Hagerty, M.; McKay, C.R.; Halberstadt, A.L.; Greer, G.R. Pilot Study of Psilocybin Treatment for Anxiety in Patients with Advanced-Stage Cancer. Arch. Gen. Psychiatry 2011, 68, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B.; Mennenga, S.E.; Belser, A.; Kalliontzi, K.; Babb, J.; et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: A randomized controlled trial. J. Psychopharmacol. 2016, 30, 1165–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harmer, C.J.; Goodwin, G.M.; Cowen, P. Why do antidepressants take so long to work? A cognitive neuropsychological model of antidepressant drug action. Br. J. Psychiatry 2009, 195, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.; Giribaldi, B.; Watts, R.; Baker-Jones, M.; Murphy-Beiner, A.; Murphy, R.; Martell, J.; Blemings, A.; Erritzoe, D.; Nutt, D.J.; et al. Trial of Psilocybin versus Es-citalopram for depression. N. Engl. J. Med. 2021, 384, 1402–1411. [Google Scholar] [CrossRef]
- Lingam, R.; Scott, J. Treatment non-adherence in affective disorders. Acta Psychiatr. Scand. 2002, 105, 164–172. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Leech, R.; Williams, T.; Erritzoe, D.; Abbasi, N.; Bargiotas, T. Implications for psychedelic-assisted psy-chotherapy: Functional magnetic resonance imaging study with psilocybin. Br. J. Psychiatry 2012, 200, 238–244. [Google Scholar] [CrossRef]
- Corriger, A.; Pickering, G. Ketamine and depression: A narrative review. Drug Des. Dev. Ther. 2019, 13, 3051–3067. [Google Scholar] [CrossRef] [Green Version]
- Fond, G.; Loundou, A.; Rabu, C.; MacGregor, A.; Lançon, C.; Brittner, M.; Micoulaud-Franchi, J.-A.; Richieri, R.; Courtet, P.; Abbar, M.; et al. Ketamine administration in depressive disorders: A systematic review and meta-analysis. Psychopharmacology 2014, 231, 3663–3676. [Google Scholar] [CrossRef]
- Garcia-Romeu, A.; Barrett, F.S.; Carbonaro, T.M.; Johnson, M.W.; Griffiths, R.R. Optimal dosing for psilocybin pharmacotherapy: Considering weight-adjusted and fixed dosing approaches. J. Psychopharmacol. 2021, 35, 353–361. [Google Scholar] [CrossRef]
- Nicholas, C.R.; Henriquez, K.M.; Gassman, M.C.; Cooper, K.M.; Muller, D.; Hetzel, S.; Brown, R.T.; Cozzi, N.V.; Thomas, C.; Hutson, P.R. High dose psilocybin is associated with positive subjective effects in healthy volunteers. J. Psychopharmacol. 2018, 32, 770–778. [Google Scholar] [CrossRef]
- Holze, F.; Vizeli, P.; Ley, L.; Müller, F.; Dolder, P.; Stocker, M.; Duthaler, U.; Varghese, N.; Eckert, A.; Borgwardt, S.; et al. Acute dose-dependent effects of lysergic acid diethylamide in a double-blind placebo-controlled study in healthy subjects. Neuropsychopharmacology 2020, 46, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.M.; McCaffrey, D.F. Bias reduction in standard errors for linear regression with multi-stage samples. Surv. Methodol. 2002, 28, 169–181. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Dx | Sample Size | Age (Years) | Female | Depression Severity | Dosing | Psychiatric Comorbidities | Study Design | Dropout | Serious AE |
|---|---|---|---|---|---|---|---|---|---|---|
| Grob 2011 | Cancer | 12 | 36–58 | 91.6% | Mild; BDI a, active arm, 16.1; placebo arm, 14.5 | Oral single dose, 0.20 mg/kg | Yes. Specific psychiatric disorders were not mentioned | Double-blind RCT | 0 | No |
| Carhart-Haris 2016 | MDD (TRD) | 12 | 42.7 (10.2) | 50% | Severe; BDI, 33.7 | Oral two doses, 10 mg and 25 mg, 7 days apart | Excluding psychotic disorder, serious suicide attempts, mania, and drug or alcohol dependence | Open-label single-arm trial | 0 | No |
| Griffiths 2016 | Cancer | 56 | 56.3 (10.0) | 49.0% | Mild; BDI, active arm, 17.7; placebo arm, 18.4 | Oral single dose, 22 or 30 mg | All participants had a psychiatric disorder, including adjustment disorder, dysthymia, GAD, or MDD | Double-blind RCT | 5 | No |
| Ross 2016 | Cancer | 31 | 56.3 (12.9) | 62.1% | Mild; BDI, active arm, 15.0; placebo arm, 16.8 | Oral single dose, 0.3 mg/kg | Adjustment disorder and GAD | Double-blind RCT | 3 | No |
| Carhart-Haris 2018 | MDD (TRD) | 20 | 44.0 (11.0) | 30% | Severe; BDI, 34.5 | Oral two doses, 10 mg and 25 mg, 7 days apart | Excluding psychotic disorder, serious suicide attempts, mania, and drug or alcohol dependence | Open-label single-arm trial | 1 | No |
| Lyons 2018 | MDD (TRD) | 15 | 45.4 (11.2) | 26% | Severe; BDI, 34.3 | Oral two doses, 10 mg and 25 mg, 7 days apart | Unavailable | Open-label single-arm trial | 0 | No |
| Roseman 2018 | MDD (TRD) | 20 | 44.7 (10.9) | 30% | Severe; BDI, 33.7 | Oral two doses, 10 mg and 25 mg, 7 days apart | Excluding psychotic disorder, serious suicide attempts, mania, and drug or alcohol dependence | Open-label single-arm trial | 0 | No |
| Agin-Liebes 2020 | Cancer | 15 | 53 (13.5) | 60.0% | Mild; BDI, 14.1 | Oral single dose, 0.3 mg/kg | Adjustment disorder and GAD | Post-RCT follow-up study | 1 | No |
| Anderson 2020 | HIV/Cancer | 18 | 59.2 (4.4) | 0.0% | Moderate; CESD b, 20.1 | Oral single dose, 0.30-0.36 mg/kg | Mood disorder, anxiety disorder, and insomnia | Open-label single-arm trial | 0 | No |
| Davis 2020 | MDD | 27 | 39.8 (12.2) | 60% | Severe, BDI, active arm, 31.9; placebo arm, 34.5 | Oral two doses, 20 mg and 30 mg, 1.6 weeks apart | Excluding psychotic disorder, bipolar disorder, and drug or alcohol dependence | RCT, blinded rater | 3 | No |
| Variable | Estimate | SE | Z-Value | p-Value |
|---|---|---|---|---|
| Dose | −1.89 | 0.84 | −2.25 | 0.02* |
| Size | −0.002 | 0.01 | −0.17 | 0.86 |
| Age | 0.01 | 0.02 | 0.4 | 0.64 |
| Female | 0.28 | 0.52 | 0.54 | 0.59 |
| Study Duration (Month) | 0.02 | 0.07 | 0.33 | 0.74 |
| MDD vs Cancer | −0.28 | 0.28 | −1.02 | 0.31 |
| Two Doses vs Single Dose | −0.50 | 0.26 | −1.96 | 0.049* |
| Severity (Severe vs Non-severe) | −0.29 | 0.28 | −1.02 | 0.31 |
| RCT vs Non-RCT | 0.20 | 0.27 | 0.74 | 0.46 |
| With vs Without Psychotherapy | −0.37 | 0.33 | −1.11 | 0.26 |
| Placebo-controlled vs Pre-post Change | −0.27 | 0.30 | −0.89 | 0.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, C.-L.; Liang, C.-S.; Yang, F.-C.; Tu, Y.-K.; Hsu, C.-W.; Carvalho, A.F.; Stubbs, B.; Thompson, T.; Tsai, C.-K.; Yeh, T.-C.; et al. Trajectory of Antidepressant Effects after Single- or Two-Dose Administration of Psilocybin: A Systematic Review and Multivariate Meta-Analysis. J. Clin. Med. 2022, 11, 938. https://doi.org/10.3390/jcm11040938
Yu C-L, Liang C-S, Yang F-C, Tu Y-K, Hsu C-W, Carvalho AF, Stubbs B, Thompson T, Tsai C-K, Yeh T-C, et al. Trajectory of Antidepressant Effects after Single- or Two-Dose Administration of Psilocybin: A Systematic Review and Multivariate Meta-Analysis. Journal of Clinical Medicine. 2022; 11(4):938. https://doi.org/10.3390/jcm11040938
Chicago/Turabian StyleYu, Chia-Ling, Chih-Sung Liang, Fu-Chi Yang, Yu-Kang Tu, Chih-Wei Hsu, Andre F. Carvalho, Brendon Stubbs, Trevor Thompson, Chia-Kuang Tsai, Ta-Chuan Yeh, and et al. 2022. "Trajectory of Antidepressant Effects after Single- or Two-Dose Administration of Psilocybin: A Systematic Review and Multivariate Meta-Analysis" Journal of Clinical Medicine 11, no. 4: 938. https://doi.org/10.3390/jcm11040938