
Surgical Management of Hemorrhoidal Disease in Inflammatory Bowel Disease: A Systematic Review with Proportional Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Characteristics
2.2. Information Sources and Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
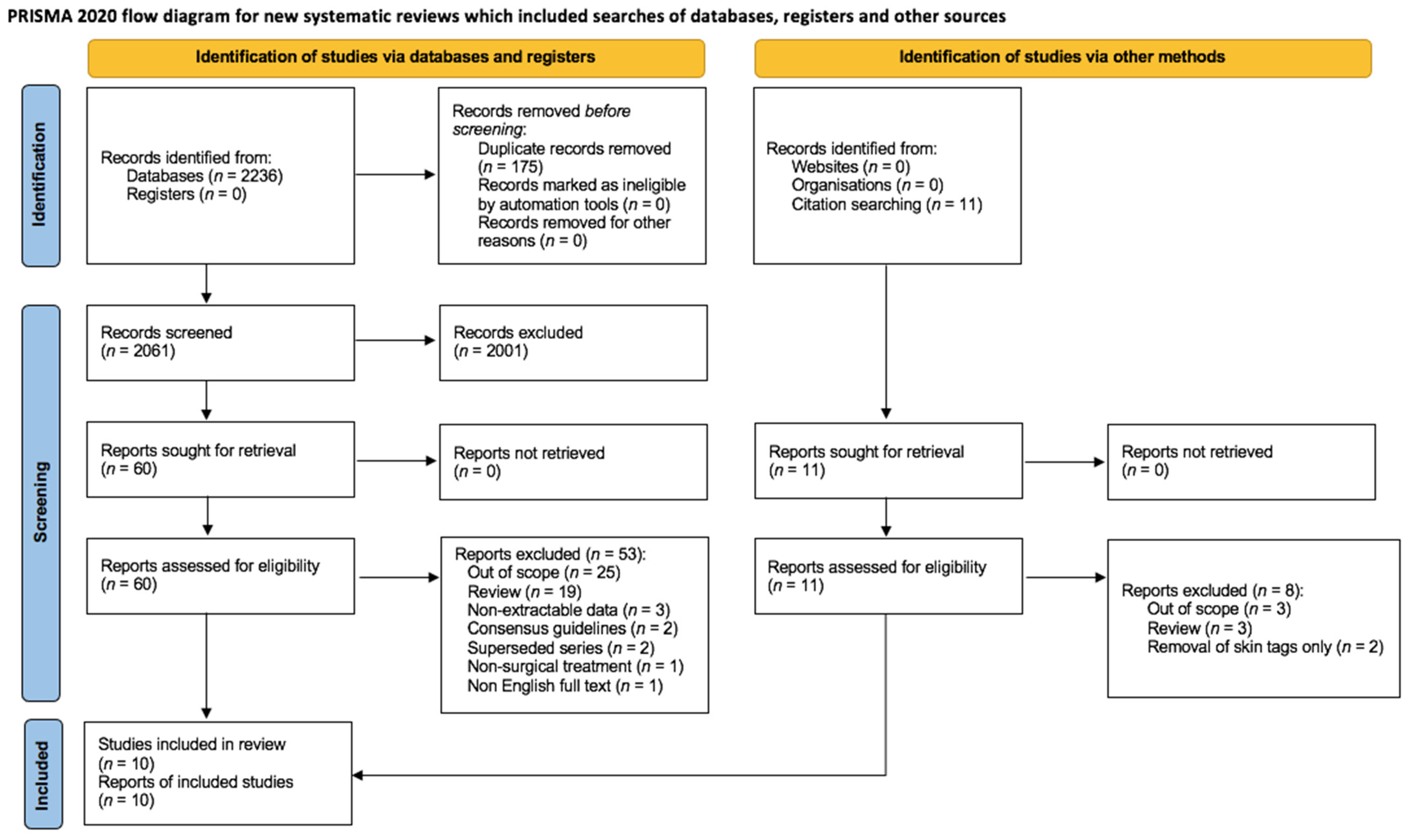
3.1. Selection of Sources of Evidence
3.2. Type of Surgery and Complications
3.3. Risk of Bias within Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Tol, R.R.; Melenhorst, J.; Dirksen, C.D.; Stassen, L.P.S.; Breukink, S.O. Protocol for the development of a Core Outcome Set (COS) for hemorrhoidal disease: An international Delphi study. Int. J. Colorectal Dis. 2017, 32, 1091–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, G.; Sacco, R.; Sammarco, G. Epidemiology of Hemorrhoidal Disease. In Hemorrhoids; Ratto, C., Parello, A., Litta, F., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 3–7. [Google Scholar]
- Ratto, C.; Parello, A.; Litta, F.; De Simone, V.; Grossi, U. Clinical Assessment of Hemorrhoids. In Hemorrhoids; Ratto, C., Parello, A., Litta, F., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 35–45. [Google Scholar]
- McDowell, C.; Farooq, U.; Haseeb, M. Inflammatory Bowel Disease; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Kaplan, G.G.; Windsor, J.W. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Gallo, G.; Martellucci, J.; Sturiale, A.; Clerico, G.; Milito, G.; Marino, F.; Cocorullo, G.; Giordano, P.; Mistrangelo, M.; Trompetto, M. Consensus statement of the Italian society of colorectal surgery (SICCR): Management and treatment of hemorrhoidal disease. Tech. Coloproctol. 2020, 24, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Tol, R.R.; Kleijnen, J.; Watson, A.J.M.; Jongen, J.; Altomare, D.F.; Qvist, N.; Higuero, T.; Muris, J.W.M.; Breukink, S.O.; Henquet, C.J.M. European Society of ColoProctology: Guideline for haemorrhoidal disease. Colorectal. Dis. 2020, 22, 650–662. [Google Scholar] [PubMed]
- De Schepper, H.; Coremans, G.; Denis, M.A.; Dewint, P.; Duinslaeger, M.; Gijsen, I.; Haers, P.; Komen, N.; Remue, C.; Roelandt, P.; et al. Belgian consensus guideline on the management of hemorrhoidal disease. Acta Gastroenterol. Belg. 2021, 84, 101–120. [Google Scholar] [CrossRef] [PubMed]
- Salgueiro, P.; Caetano, A.C.; Oliveira, A.M.; Rosa, B.; Mascarenhas-Saraiva, M.; Ministro, P.; Amaro, P.; Godinho, R.; Coelho, R.; Gaio, R.; et al. Portuguese Society of Gastroenterology Consensus on the Diagnosis and Management of Hemorrhoidal Disease. GE-Port. J. Gastroenterol. 2020, 27, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Koh, S.; Barnajian, M.; Zaghiyan, K.; Fleshner, P. Poster Abstracts. Colorectal Dis. 2015, 17, 38–101. [Google Scholar]
- UEG Week 2017 Poster Presentations. United Eur. Gastroenterol. J. 2017, 5, A161–A836. [CrossRef]
- Jeffery, P.J.; Parks, A.G.; Ritchie, J.K. Treatment of haemorrhoids in patients with inflammatory bowel disease. Lancet 1977, 1, 1084–1085. [Google Scholar] [CrossRef]
- Hughes, L.E. Surgical pathology and management of anorectal Crohn’s disease. J. R. Soc. Med. 1978, 71, 644–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keighley, M.R.; Allan, R.N. Current status and influence of operation on perianal Crohn’s disease. Int. J. Colorectal Dis. 1986, 1, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Wolkomir, A.F.; Luchtefeld, M.A. Surgery for symptomatic hemorrhoids and anal fissures in Crohn’s disease. Dis. Colon Rectum 1993, 36, 545–547. [Google Scholar] [CrossRef] [PubMed]
- D’Ugo, S.; Franceschilli, L.; Cadeddu, F.; Leccesi, L.; Blanco, G.D.V.; Calabrese, E.; Milito, G.; Di Lorenzo, N.; Gaspari, A.L.; Sileri, P. Medical and surgical treatment of haemorrhoids and anal fissure in Crohn’s disease: A critical appraisal. BMC Gastroenterol. 2013, 13, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, N.P.; Lightner, A.L.; Habermann, E.B.; Mathis, K.L. Hemorrhoidectomy and Excision of Skin Tags in IBD: Harbinger of Doom or Simply a Disease Running Its Course? Dis. Colon Rectum 2019, 62, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- Lightner, A.L.; Kearney, D.; Giugliano, D.; Hull, T.; Holubar, S.D.; Koh, S.; Zaghiyan, K.; Fleshner, P.R. Excisional Hemorrhoidectomy: Safe in Patients With Crohn’s Disease? Inflamm. Bowel Dis. 2020, 26, 1390–1393. [Google Scholar] [CrossRef] [PubMed]
- Karin, E.; Avital, S.; Dotan, I.; Skornick, Y.; Greenberg, R. Doppler-guided haemorrhoidal artery ligation in patients with Crohn’s disease. Colorectal Dis. 2012, 14, 111–114. [Google Scholar] [CrossRef]
- Goligher, J.; Duthie, H.; Nixon, H. Surgery of the Anus Rectum and Colon; Bailliere Tiudall: London, UK, 1984. [Google Scholar]
- Alexander-Williams, J.; Buchmann, P. Perianal Crohn’s disease. World J. Surg. 1980, 4, 203–208. [Google Scholar] [CrossRef]
- Cracco, N.; Zinicola, R. Is haemorrhoidectomy in inflammatory bowel disease harmful? An old dogma re-examined. Colorectal Dis. 2014, 16, 516–519. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Loftus, E.V., Jr.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Sandborn, W.J. Perianal Crohn’s disease findings other than fistulas in a population-based cohort. Inflamm. Bowel Dis. 2012, 18, 43–48. [Google Scholar] [CrossRef]
- Eglinton, T.W.; Barclay, M.L.; Gearry, R.B.; Frizelle, F.A. The spectrum of perianal Crohn’s disease in a population-based cohort. Dis. Colon Rectum 2012, 55, 773–777. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; McC Mortensen, N.J.; Jewell, D.P.; George, B. Perianal Crohn’s disease. Br. J. Surg. 2004, 91, 801–814. [Google Scholar] [CrossRef] [PubMed]
- Simillis, C.; Thoukididou, S.N.; Slesser, A.A.; Rasheed, S.; Tan, E.; Tekkis, P.P. Systematic review and network meta-analysis comparing clinical outcomes and effectiveness of surgical treatments for haemorrhoids. Br. J. Surg. 2015, 102, 1603–1618. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author | Year | Country | Study Period (Years) | N * | CD | UC | Active IBD at Surgery | Type of Operation | Complications (N) | Average Follow-Up (Months) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| CD | UC | ||||||||||
| Jeffery [13] | 1977 | UK | 40 | 20 | 4 | 16 | nr | OEH | 1 | 3 | 480 |
| Hughes [14] | 1978 | UK | 6 | 2 | 2 | 0 | nr | OEH | 1 | / | 72 |
| Keighley [15] | 1986 | UK | 1 | 2 | 2 | 0 | nr | RBL | 1 | / | 12 |
| Wolkomir [16] | 1993 | USA | 15 | 17 | 17 | 0 | 0 | CEH ^ | 4 | / | 137 |
| Karin [20] | 2012 | Israel | 4 | 13 | 13 | 0 | nr | DGHAL | 3 | / | 18 |
| D’Ugo [17] | 2013 | Italy | 8 | 9 | 9 | 0 | 0 | Mixed § | 1 | / | 37 |
| Koh [11] | 2015 | USA | 14 | 9 | 9 | 0 | 1 | OEH | 0 | / | 28 |
| Lee [12] | 2017 | S. Korea | 11 | 44 | 0 | 44 | nr | OEH | / | 0 | nr |
| McKenna [18] | 2019 | USA ° | 17 | 70 | 27 | 43 | nr | Mixed ¶ | 2 | 3 | 29 |
| Lightner [19] | 2020 | USA ° | 24 | 36 | 36 | 0 | nr | OEH | 4 | / | 31.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grossi, U.; Gallo, G.; Di Tanna, G.L.; Bracale, U.; Ballo, M.; Galasso, E.; Kazemi Nava, A.; Zucchella, M.; Cinetto, F.; Rattazzi, M.; et al. Surgical Management of Hemorrhoidal Disease in Inflammatory Bowel Disease: A Systematic Review with Proportional Meta-Analysis. J. Clin. Med. 2022, 11, 709. https://doi.org/10.3390/jcm11030709
Grossi U, Gallo G, Di Tanna GL, Bracale U, Ballo M, Galasso E, Kazemi Nava A, Zucchella M, Cinetto F, Rattazzi M, et al. Surgical Management of Hemorrhoidal Disease in Inflammatory Bowel Disease: A Systematic Review with Proportional Meta-Analysis. Journal of Clinical Medicine. 2022; 11(3):709. https://doi.org/10.3390/jcm11030709
Chicago/Turabian StyleGrossi, Ugo, Gaetano Gallo, Gian Luca Di Tanna, Umberto Bracale, Mattia Ballo, Elisa Galasso, Andrea Kazemi Nava, Martino Zucchella, Francesco Cinetto, Marcello Rattazzi, and et al. 2022. "Surgical Management of Hemorrhoidal Disease in Inflammatory Bowel Disease: A Systematic Review with Proportional Meta-Analysis" Journal of Clinical Medicine 11, no. 3: 709. https://doi.org/10.3390/jcm11030709