
Antithrombotic Strategies in Patients with Atrial Fibrillation and Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention

 ,
,  ,
, 
Abstract
:1. Introduction
2. Trials with VKAs
3. Trials with DOACs
4. Current Recommendations
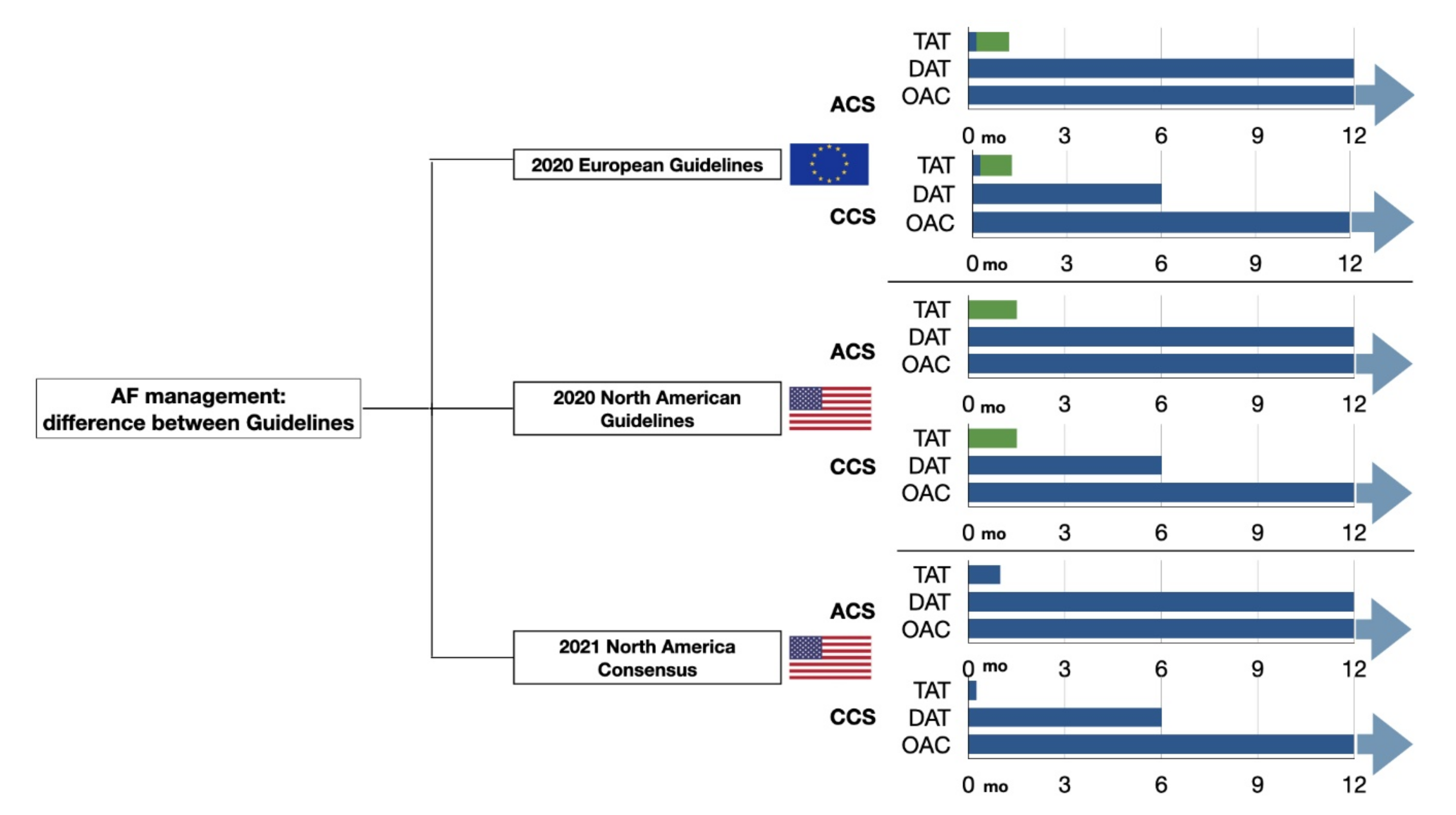
4.1. European Guidelines
4.2. North American Guidelines
4.3. North American Consensus on Antithrombotic Therapy in Patients with AF Undergoing PCI
4.4. 2021. European Heart Rhythm Association Practical Guide
5. Metanalyses
6. Observational Studies
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wijesurendra, R.S.; Casadei, B. Mechanisms of atrial fibrillation. Heart 2019, 105, 1860–1867. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.; Banerjee, A.; Breithardt, G.; Camm, A.J.; Commerford, P.; Freedman, B.; Gonzalez-Hermosillo, J.A.; Halperin, J.L.; Lau, C.P.; Perel, P.; et al. The World Heart Federation Roadmap for Nonvalvular Atrial Fibrillation. Glob. Heart 2017, 12, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.; De Silva, D.A.; Macleod, M.R.; Coutts, S.B.; Schwamm, L.H.; Davis, S.M.; Donnan, G.A. Ischaemic stroke. Nat. Rev. Dis. Primers 2019, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014, 130, e199–e267. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Di Maio, M.; Greco, A.; Bhatt, D.L.; Gibson, C.M.; Goette, A.; Lopes, R.D.; Mehran, R.; Vranckx, P.; Angiolillo, D.J. Safety and Efficacy of Double Antithrombotic Therapy with Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2020, 9. [Google Scholar] [CrossRef]
- Van Rein, N.; Heide-Jørgensen, U.; Lijfering, W.M.; Dekkers, O.M.; Sørensen, H.T.; Cannegieter, S.C. Major Bleeding Rates in Atrial Fibrillation Patients on Single, Dual, or Triple Antithrombotic Therapy. Circulation 2019, 139, 775–786. [Google Scholar] [CrossRef]
- Stroke Prevention in Atrial Fibrillation Study. Final results. Circulation 1991, 84, 527–539. [Google Scholar]
- Michniewicz, E.; Mlodawska, E.; Lopatowska, P.; Tomaszuk-Kazberuk, A.; Malyszko, J. Patients with atrial fibrillation and coronary artery disease-Double trouble. Adv. Med. Sci. 2018, 63, 30–35. [Google Scholar] [CrossRef]
- ACTIVE Writing Group of the ACTIVE Investigators. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesart.tan for prevention of Vascular Events (ACTIVE W): A randomised controlled trial. Lancet 2006, 367, 1903–1912. [Google Scholar] [CrossRef]
- Aguilar, M.I.; Hart, R.; Pearce, L.A. Oral anticoagulants versus antiplatelet therapy for preventing stroke in patients with non-valvular atrial fibrillation and no history of stroke or transient ischemic attacks. Cochrane Database Syst. Rev. 2007, 3, CD006186. [Google Scholar] [CrossRef]
- Ruiz-Nodar, J.M.; Marín, F.; Hurtado, J.A.; Valencia, J.; Pinar, E.; Pineda, J.; Gimeno, J.R.; Sogorb, F.; Valdés, M.; Lip, G.Y. Anticoagulant and antiplatelet therapy use in 426 patients with atrial fibrillation undergoing percutaneous coronary intervention and stent implantation implications for bleeding risk and prognosis. J. Am. Coll. Cardiol. 2008, 51, 818–825. [Google Scholar] [CrossRef] [Green Version]
- Urban, P.; Macaya, C.; Rupprecht, H.J.; Kiemeneij, F.; Emanuelsson, H.; Fontanelli, A.; Pieper, M.; Wesseling, T.; Sagnard, L. Randomized evaluation of anticoagulation versus antiplatelet therapy after coronary stent implantation in high-risk patients: The multicenter aspirin and ticlopidine trial after intracoronary stenting (MATTIS). Circulation 1998, 98, 2126–2132. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation 2016, 134, e123–e155. [Google Scholar]
- Capodanno, D.; Alfonso, F.; Levine, G.N.; Valgimigli, M.; Angiolillo, D.J. ACC/AHA Versus ESC Guidelines on Dual Antiplatelet Therapy: JACC Guideline Comparison. J Am Coll. Cardiol. 2018, 72, 2915–2931. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar] [PubMed]
- Lucà, F.; Giubilato, S.; Fusco, S.; Leone, A.; Poli, S.; Rao, C.M.; Iorio, A.; Gelsomino, S.; Gabrielli, D.; Colivicchi, F.; et al. The Combination of Oral Anticoagulant and Antiplatelet Therapies: Stay One Step Ahead. J Cardiovasc. Pharmacol. Ther. 2020, 25, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Andreotti, F.; D’Amario, D.; Vergallo, R.; Montone, R.A.; Niccoli, G.; Crea, F. Randomised trials and meta-analyses of double vs triple antitrombotic therapy fo.or atrial fibrillation-ACS/PCI: A critical appraisal. Int. J. Cardiol. Heart Vasc. 2020, 28, 100524. [Google Scholar]
- Dewilde, W.J.; Oirbans, T.; Verheugt, F.W.; Kelder, J.C.; De Smet, B.J.; Herrman, J.P.; Adriaenssens, T.; Vrolix, M.; Heestermans, A.A.; Vis, M.M.; et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: An open-label, randomised, controlled trial. Lancet 2013, 381, 1107–1115. [Google Scholar] [CrossRef]
- Fiedler, K.A.; Maeng, M.; Mehilli, J.; Schulz-Schüpke, S.; Byrne, R.A.; Sibbing, D.; Hoppmann, P.; Schneider, S.; Fusaro, M.; Ott, I.; et al. Duration of Triple Therapy in Patients Requiring Oral Anticoagulation After Drug-Eluting Stent Implantation: The ISAR-TRIPLE Trial. J. Am. Coll. Cardiol. 2015, 65, 1619–1629. [Google Scholar] [CrossRef] [Green Version]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.; Wildgoose, P.; van Eickels, M.; Lip, G.Y.; Cohen, M.; Husted, S.; et al. An open-label, randomized, controlled, multicenter study exploring two treatment strategies of rivaroxaban and a dose-adjusted oral vitamin K antagonist treatment strategy in subjects with atrial fibrillation who undergo percutaneous coronary intervention (PIONEER AF-PCI). Am. Heart J. 2015, 169, 472–478.e5. [Google Scholar]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [Green Version]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Paciaroni, M.; Agnelli, G.; Micheli, S.; Caso, V. Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke: A meta-analysis of randomized controlled trials. Stroke 2007, 38, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, R.; Lewis, S.; Berge, E.; Sandercock, P.A.; Koudstaal, P.J. Risk of early death and recurrent stroke and effect of heparin in 3169 patients with acute ischemic stroke and atrial fibrillation in the International Stroke Trial. Stroke 2001, 32, 2333–2337. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, S.; Kaikita, K.; Akao, M.; Ako, J.; Matoba, T.; Nakamura, M.; Miyauchi, K.; Hagiwara, N.; Kimura, K.; Hirayama, A.; et al. Antithrombotic Therapy for Atrial Fibrillation with Stable Coronary Disease. N. Engl. J. Med. 2019, 381, 1103–1113. [Google Scholar] [CrossRef]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.; Li, J.; Berg, J.M.T.; et al. Optimal Antithrombotic Regimens for Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: An Updated Network Meta-analysis. JAMA Cardiol. 2020, 5, 582–589. [Google Scholar] [CrossRef]
- Lip, G.; Collet, J.P.; Haude, M.; Byrne, R.; Chung, E.H.; Fauchier, L.; Halvorsen, S.; Lau, D.; Lopez-Cabanillas, N.; Lettino, M.; et al. 2018 Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: A joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). Europace 2019, 21, 192–193. [Google Scholar]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C.; Ellinor, P.T., Jr.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration With the Society of Thoracic Surgeons. Circulation 2019, 140, e125–e151. [Google Scholar]
- Sarafoff, N.; Martischnig, A.; Wealer, J.; Mayer, K.; Mehilli, J.; Sibbing, D.; Kastrati, A. Triple therapy with aspirin, prasugrel, and vitamin K antagonists in patients with drug-eluting stent implantation and an indication for oral anticoagulation. J. Am. Coll. Cardiol. 2013, 61, 2060–2066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, L.R.; Ju, C.; Zettler, M.; Messenger, J.C.; Cohen, D.J.; Stone, G.W.; Baker, B.A.; Effron, M.; Peterson, E.D.; Wang, T.Y. Outcomes of Patients With Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention Receiving an Oral Anticoagulant and Dual Antiplatelet Therapy: A Comparison of Clopidogrel Versus Prasugrel From the TRANSLATE-ACS Study. JACC Cardiovasc. Interv. 2015, 8, 1880–1889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamberts, M.; Gislason, G.H.; Olesen, J.B.; Kristensen, S.L.; Olsen, A.M.S.; Mikkelsen, A.; Christensen, C.B.; Lip, G.Y.; Køber, L.; Torp-Pedersen, C.; et al. Oral anticoagulation and antiplatelets in atrial fibrillation patients after myocardial infarction and coronary intervention. J. Am. Coll. Cardiol. 2013, 62, 981–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, O.Ö.; Bico, B.; Chaudhry, U.; Wagner, H.; Koul, S.; Tydén, P.; Scherstén, F.; Jovinge, S.; Svensson, P.J.; Smith, J.G.; et al. Concomitant use of warfarin and ticagrelor as an alternative to triple antithrombotic therapy after an acute coronary syndrome. Thromb. Res. 2015, 135, 26–30. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Bhatt, D.L.; Cannon, C.P.; Eikelboom, J.W.; Gibson, C.M.; Goodman, S.G.; Granger, C.B.; Holmes, D.R.; Lopes, R.D.; Mehran, R.; et al. Antithrombotic Therapy in Patients With Atrial Fibrillation Treated With Oral Anticoagulation Undergoing Percutaneous Coronary Intervention: A North American Perspective: 2021 Update. Circulation 2021, 143, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.; Goette, A.; Tijssen, J.; Eckardt, L.; Lewalter, T.; Vranckx, P.; Valgimigli, M. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur. Heart J. 2019, 40, 3757–3767. [Google Scholar]
- Galli, M.; Andreotti, F.; Porto, I.; Crea, F. Intracranial haemorrhages vs. stent thromboses with direct oral anticoagulant plus single antiplatelet agent or triple antithrombotic therapy: A meta-analysis of randomized trials in atrial fibrillation and percutaneous coronary intervention/acute coronary syndrome patients. Europace 2020, 22, 538–546. [Google Scholar]
- Orme, R.C.; Parker, W.; Thomas, M.R.; Judge, H.M.; Baster, K.; Sumaya, W.; Morgan, K.P.; McMellon, H.C.; Richardson, J.D.; Grech, E.D.; et al. Study of Two Dose Regimens of Ticagrelor Compared with Clopidogrel in Patients Undergoing Percutaneous Coronary Intervention for Stable Coronary Artery Disease (STEEL-PCI). Circulation 2018, 138, 1290–1300. [Google Scholar] [CrossRef]
- Franchi, F.; Rollini, F.; Been, L.; Briceno, M.; Maaliki, N.; Wali, M.; Rivas, A.; Pineda, A.M.; Suryadevara, S.; Soffer, D.; et al. Pharmacodynamic and Pharmacokinetic Effects of a Low Maintenance Dose Ticagrelor Regimen Versus Standard Dose Clopidogrel in Diabetes Mellitus Patients Without Previous Major Cardiovascular Events Undergoing Elective Percutaneous Coronary Intervention: The OPTIMUS-6 Study. Circulation 2020, 142, 1500–1502. [Google Scholar]
- Steffel, J.; Collins, R.; Antz, M.; Cornu, P.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; Rowell, N.; et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europace 2021, 23, 1612–1676. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Potpara, T.S.; Mujovic, N.; Proietti, M.; Dagres, N.; Hindricks, G.; Collet, J.P.; Valgimigli, M.; Heidbuchel, H.; Lip, G. Revisiting the effects of omitting aspirin in combined antithrombotic therapies for atrial fibrillation and acute coronary syndromes or percutaneous coronary interventions: Meta-analysis of pooled data from the PIONEER AF-PCI, RE-DUAL PCI, and AUGUSTUS trials. Europace 2020, 22, 33–46. [Google Scholar]
- Galli, M.; Andreotti, F.; D’Amario, D.; Vergallo, R.; Montone, R.A.; Porto, I.; Crea, F. Dual therapy with direct oral anticoagulants significantly increases the risk of stent thrombosis compared to triple therapy. Eur. Heart J. Cardiovasc. Pharm. 2020, 6, 128–129. [Google Scholar] [CrossRef]
- Haller, P.M.; Sulzgruber, P.; Kaufmann, C.; Geelhoed, B.; Tamargo, J.; Wassmann, S.; Schnabel, R.B.; Westermann, D.; Huber, K.; Niessner, A.; et al. Bleeding and ischaemic outcomes in patients treated with dual or triple antithrombotic therapy: Systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Pharm. 2019, 5, 226–236. [Google Scholar] [CrossRef]
- Andò, G.; Costa, F. Double or triple antithrombotic therapy after coronary stenting and atrial fibrillation: A systematic review and meta-analysis of randomized clinical trials. Int. J. Cardiol. 2020, 302, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.U.; Osman, M.; Khan, M.U.; Khan, M.S.; Zhao, D.; Mamas, M.A.; Savji, N.; Al-Abdouh, A.; Hasan, R.K.; Michos, E.D. Dual Versus Triple Therapy for Atrial Fibrillation After Percutaneous Coronary Intervention: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2020, 172, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Golwala, H.B.; Cannon, C.P.; Steg, P.G.; Doros, G.; Qamar, A.; Ellis, S.G.; Oldgren, J.; Berg, J.M.T.; Kimura, T.; Hohnloser, S.H.; et al. Safety and efficacy of dual vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2018, 39, 1726–1735a. [Google Scholar] [CrossRef]
- Lopes, R.D.; Hong, H.; Harskamp, R.E.; Bhatt, D.L.; Mehran, R.; Cannon, C.P.; Granger, C.B.; Verheugt, F.; Li, J.; Berg, J.M.T.; et al. Safety and Efficacy of Antithrombotic Strategies in Patients With Atrial Fibrillation Undergoing Percutaneous Coronary Intervention: A Network Meta-analysis of Randomized Controlled Trials. JAMA Cardiol. 2019, 4, 747–755. [Google Scholar] [CrossRef]
- Cavallari, I.; Patti, G. Meta-Analysis Comparing the Safety and Efficacy of Dual Versus Triple Antithrombotic Therapy in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention. Am. J. Cardiol. 2018, 121, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Kheiri, B.; Osman, M.; Bakhit, A.; Radaideh, Q.; Abdalla, A.; Barbarawi, M.; Zayed, Y.; Ahmed, S.; Bachuwa, G.; Hassan, M. Dual versus triple therapy for patients with atrial fibrillation and acute coronary syndrome: A meta-analysis and trial sequential analysis of randomized controlled trials. J. Thromb. Thrombolysis 2019, 48, 511–513. [Google Scholar] [CrossRef]
- Brunetti, N.D.; Tarantino, N.; De Gennaro, L.; Correale, M.; Santoro, F.; Di Biase, M. Direct oral anticoagulants versus standard triple therapy in atrial fibrillation and PCI: Meta-analysis. Open Heart 2018, 5, e000785. [Google Scholar] [CrossRef]
- Piccini, J.P.; Jones, W.S. Triple Therapy for Atrial Fibrillation after PCI. N. Engl. J. Med. 2017, 377, 1580–1582. [Google Scholar] [CrossRef]
- Stenestrand, U.; Lindbäck, J.; Wallentin, L.; RIKS-HIARegistr. Anticoagulation therapy in atrial fibrillation in combination with acute myocardial infarction influences long-term outcome: A prospective cohort study from the Register of Information and Knowledge About Swedish Heart Intensive Care Admissions (RIKS-HIA). Circulation 2005, 112, 3225–3231. [Google Scholar] [CrossRef] [Green Version]
- Lamberts, M.; Olesen, J.B.; Ruwald, M.H.; Hansen, C.M.; Karasoy, D.; Kristensen, S.L.; Køber, L.; Torp-Pedersen, C.; Gislason, G.H.; Hansen, M.L. Bleeding after initiation of multiple antithrombotic drugs, including triple therapy, in atrial fibrillation patients following myocardial infarction and coronary intervention: A nationwide cohort study. Circulation 2012, 126, 1185–1193. [Google Scholar] [CrossRef] [Green Version]
- De Luca, L.; Rubboli, A.; Bolognese, L.; Gonzini, L.; Urbinati, S.; Murrone, A.; di Uccio, F.S.; Ferrari, F.; Lucà, F.; Caldarola, P.; et al. Antithrombotic management of patients with acute coronary syndrome and atrial fibrillation undergoing coronary stenting: A prospective, observational, nationwide study. BMJ Open 2020, 10, e041044. [Google Scholar] [CrossRef]
- De Luca, L.; Rubboli, A.; Bolognese, L.; Uguccioni, M.; Lucci, D.; Blengino, S.; Campodonico, J.; Meynet, I.; Prever, S.M.B.; Di Lenarda, A.; et al. Is percutaneous coronary intervention safe during uninterrupted direct oral anticoagulant therapy in patients with atrial fibrillation and acute coronary syndromes? Open Heart 2021, 8, e001677. [Google Scholar] [CrossRef] [PubMed]
- De Luca, L.; Bolognese, L.; Rubboli, A.; Vetrano, A.; Callerame, M.; Rivetti, L.; Gonzini, L.; Gabrielli, D.; Di Lenarda, A.; Gulizia, M.M.; et al. Combinations of antithrombotic therapies prescribed after percutaneous coronary intervention in patients with acute coronary syndromes and atrial fibrillation: Data from the nationwide MATADOR-PCI registry. Eur. Heart J. Cardiovasc. Pharm. 2021, 7, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- De Luca, L.; Di Lenarda, A.; Rubboli, A.; Bolognese, L.; Gonzini, L.; Fortuni, F.; Navazio, A.; Poletti, F.; Ledda, A.; Urbinati, S.; et al. Post-discharge antithrombotic management and clinical outcomes of patients with new-onset or pre-existing atrial fibrillation and acute coronary syndromes undergoing coronary stenting: Follow-up data of the MATADOR-PCI study. Eur. J. Intern. Med. 2021, 88, 28–34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Design, Randomization | Patients (n) | Treatment Arms | AF (%) | Maximum Days in ASA in DAT Group | ACS (%) | Follow Up (mo) | Primary Outcome | |
|---|---|---|---|---|---|---|---|---|
| WOEST | RCT open label, 1:1 | 573 | VKA + P2Y12i for 1 or 12 mo vs. VKA + aspirin + P2Y12i for 1 or 12 mo | 69 | <1 | 28 | 12 | Any bleeding events (TIMI and GUSTO criteria) |
| ISAR-TRIPLE | RCT open label, 1:1 | 614 | 6 we of VKA + clopidogrel + aspirin vs. 6 mo of VKA + clopidogrel + aspirin | 84 | / | 32 | 9 | A composite of death, MI, ST, stroke, or major bleeding |
| PIONEER-AF | RCT open label, 1:1:1 | 2124 | rivaroxaban (15 mg/od) + P2Y12i vs. rivaroxaban (2.5 mg/bid) + aspirin + P2Y12i vs. VKA + aspirin + P2Y12i | 100 | 3 | 52 | 12 | Clinically significant bleeding (TIMI major, minor bleeding, or bleeding requiring medical attention) |
| RE-DUAL PCI | RCT open label, 1:1:1 | 2725 | dabigatran (110 mg/bid) + P2Y12i vs. dabigatran (150 mg/bid) + P2Y12i vs. VKA + aspirin (1–3 months) + P2Y12i | 100 | 5 | 51 | 14 | Clinically significant bleeding (ISTH major bleeding or clinically relevant nonmajor bleeding event) |
| AUGUSTUS | RCT open label, 2 × 2 | 4614 | apixaban (5 mg/bid) + P2Y12i vs. apixaban (5 mg/bid) + aspirin + P2Y12i vs. VKA + P2Y12i vs. VKA + aspirin + P2Y12 | 100 | 14 | 60 | 6 | Clinically significant bleeding (ISTH major or clinically relevant nonmajor bleeding) |
| ENTRUST-AF PCI | RCT open label, 1:1 | 1506 | Edoxaban (60 mg/od) + P2Y12i vs. VKA + aspirin (1–12 mo) + P2Y12 | 100 | 5 | 52 | 12 | Major or clinically relevant nonmajor bleeding (according to ISTH criteria) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Luca, L.; Mistrulli, R.; Veneziano, F.A.; Grigioni, F.; Volpe, M.; Musumeci, F.; Gabrielli, D. Antithrombotic Strategies in Patients with Atrial Fibrillation and Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention. J. Clin. Med. 2022, 11, 512. https://doi.org/10.3390/jcm11030512
De Luca L, Mistrulli R, Veneziano FA, Grigioni F, Volpe M, Musumeci F, Gabrielli D. Antithrombotic Strategies in Patients with Atrial Fibrillation and Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention. Journal of Clinical Medicine. 2022; 11(3):512. https://doi.org/10.3390/jcm11030512
Chicago/Turabian StyleDe Luca, Leonardo, Raffaella Mistrulli, Francesco Antonio Veneziano, Francesco Grigioni, Massimo Volpe, Francesco Musumeci, and Domenico Gabrielli. 2022. "Antithrombotic Strategies in Patients with Atrial Fibrillation and Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention" Journal of Clinical Medicine 11, no. 3: 512. https://doi.org/10.3390/jcm11030512