
Analgesia Nociception Index-Guided Remifentanil versus Standard Care during Propofol Anesthesia: A Randomized Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Study Design
2.2.1. Randomization
2.2.2. Anesthesia
- -
- In the Standard group, intraoperative remifentanil management was left to the discretion of the anesthesiologist in charge of the patient, according to their usual practice. In both institutions, ANI monitoring was not part of standard practice, so in this group, the anesthesiologist was blinded to the ANI.
- -
- In the ANI group, intraoperative remifentanil was guided by the ANI value, and could be modified every 5 min. If ANI was <50, remifentanil Ce was increased by 0.5 ng mL−1. If ANI was >70, remifentanil Ce was decreased by 0.5 ng mL−1. If ANI was between 50 and 70, no changes were made. The minimal remifentanil Ce allowed in the protocol was 1 ng mL−1. Several safety items regarding the management of hemodynamic changes were added to our algorithm: if SBP was >130 mmHg on two consecutive measurements, nicardipine 1 mg kg−1 was administered. Conversely, if SBP was <80 mmHg, patients received 500 mL of crystalloids. If SBP remained low, ephedrine was administered (3 mg boluses) until blood pressure was restored. Finally, if heart rate (HR) decreased below 45 bpm, patients received atropine (1 mg). Atropine or ephedrine administration resulted in the discontinuation of the ANI-guidance algorithm: patients were managed as in standard practice for the rest of the procedure.
2.2.3. Postoperative Period
2.3. Data Collection
2.4. Aims and Outcome Measures
- The quality of anesthesia: the related outcome measures were the total dose of propofol, the number of changes in remifentanil Ce, duration of anesthesia, time to emergence (between remifentanil discontinuation and extubation), potential awareness and surgeon’s satisfaction.
- Postoperative analgesia: the related outcome measures were postoperative cumulated morphine consumption 12 and 24 h after surgery, the proportion of patients requiring nefopam or ketoprofen, VAS scores, incidence of nausea, vomiting, urinary retention, respiratory depression requiring oxygen administration and patient’s satisfaction.
- Chronic pain: presence of pain 3 months after the procedure.
2.5. Statistical Analysis
3. Results
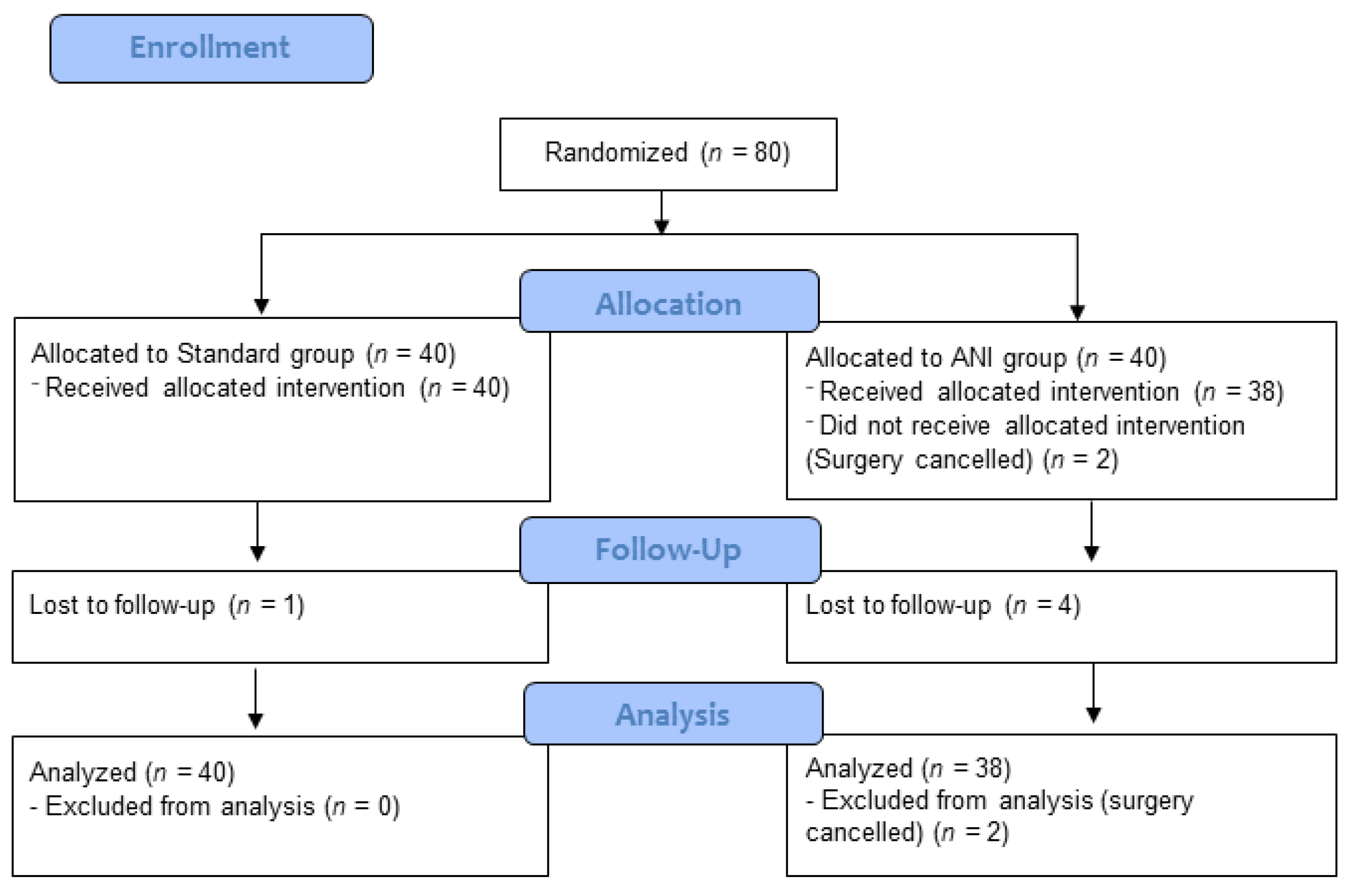
3.1. Population
3.2. Remifentanil
3.3. Quality of Anesthesia
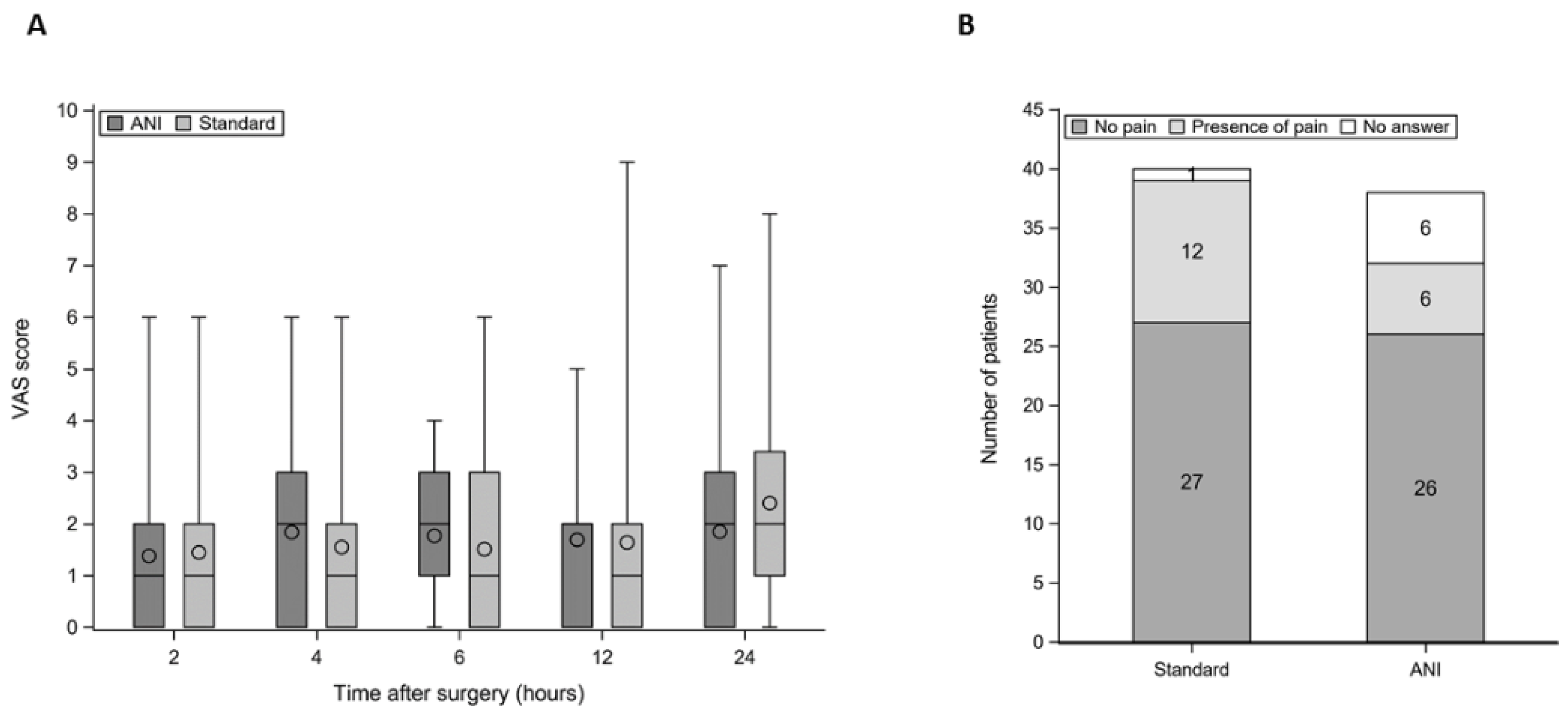
3.4. Postoperative Analgesia
3.5. Chronic Pain
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jeanne, M.; Clément, C.; De Jonckheere, J.; Logier, R.; Tavernier, B. Variations of the analgesia nociception index during general anaesthesia for laparoscopic abdominal surgery. J. Clin. Monit. Comput. 2012, 26, 289–294. [Google Scholar] [CrossRef]
- Jeanne, M.; Delecroix, M.; De Jonckheere, J.; Keribedj, A.; Logier, R.; Tavernier, B. Variations of the analgesia nociception index during propofol anesthesia for total knee replacement. Clin. J. Pain 2014, 30, 1084–1088. [Google Scholar] [CrossRef]
- Ledowski, T.; Averhoff, L.; Tiong, W.S.; Lee, C. Analgesia Nociception Index (ANI) to predict intraoperative haemodynamic changes: Results of a pilot investigation. Acta Anaesthesiol. Scand. 2014, 58, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Gruenewald, M.; Ilies, C. Monitoring the nociception-anti-nociception balance. Best Pract. Res. Clin. Anaesthesiol. 2013, 27, 235–247. [Google Scholar] [CrossRef]
- Gruenewald, M.; Herz, J.; Schoenherr, T.; Thee, C.; Steinfath, M.; Bein, B. Measurement of the nociceptive balance by Analgesia Nociception Index and Surgical Pleth Index during sevoflurane-remifentanil anesthesia. Minerva Anestesiol. 2015, 81, 480–489. [Google Scholar]
- Sabourdin, N.; Arnaout, M.; Louvet, N.; Guye, M.L.; Piana, F.; Constant, I. Pain monitoring in anesthetized children: First assessment of skin conductance and analgesia-nociception index at different infusion rates of remifentanil. Pediatr. Anesth. 2013, 23, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Funcke, S.; Sauerlaender, S.; Pinnschmidt, H.O.; Saugel, B.; Bremer, K.; Reuter, D.; Nitzschke, R. Validation of Innovative Techniques for Monitoring Nociception during General Anesthesia: A Clinical Study Using Tetanic and Intracutaneous Electrical Stimulation. Anesthesiology 2017, 127, 272–283. [Google Scholar] [CrossRef]
- Dundar, N.; Kus, A.; Gurkan, Y.; Toker, K.; Solak, M. Analgesia nociception index (ani) monitoring in patients with thoracic paravertebral block: A randomized controlled study. J. Clin. Monit. Comput. 2018, 32, 481–486. [Google Scholar] [CrossRef]
- Upton, H.D.; Ludbrook, G.L.; Wing, A.; Sleigh, J.W. Intraoperative “Analgesia Nociception Index”—Guided Fentanyl Administration during Sevoflurane Anesthesia in Lumbar Discectomy and Laminectomy: A Randomized Clinical Trial. Anesth. Analg. 2017, 125, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Szental, J.A.; Webb, A.; Weeraratne, C.; Campbell, A.; Sivakumar, H.; Leong, S. Postoperative pain after laparoscopic cholecystectomy is not reduced by intraoperative analgesia guided by analgesia nociception index (ANI®) monitoring: A randomized clinical trial. Br. J. Anaesth. 2015, 114, 640–645. [Google Scholar] [CrossRef] [Green Version]
- Jiao, Y.; He, B.; Tong, X.; Xia, R.; Zhang, C.; Shi, X. Intraoperative monitoring of nociception for opioid administration: A meta-analysis of randomized controlled trials. Minerva Anestesiol. 2019, 85, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Ledowski, T. Objective monitoring of nociception: A review of current commercial solutions. Br. J. Anaesth. 2019, 123, e312. [Google Scholar] [CrossRef]
- Meijer, F.S.; Niesters, M.; van Velzen, M.; Martini, C.H.; Olofsen, E.; Edry, R.; Sessler, D.I.; van Dorp, E.L.A.; Dahan, A.; Boon, M. Does nociception monitor-guided anesthesia affect opioid consumption? A systematic review of randomized controlled trials. J. Clin. Monit. Comput. 2020, 34, 629–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanaya, N.; Hirata, N.; Kurosawa, S.; Nakayama, M.; Namiki, A. Differential effects of propofol and sevoflurane on heart rate variability. Anesthesiology 2003, 98, 34–40. [Google Scholar] [CrossRef]
- Ledowski, T.; Bein, B.; Hanss, R.; Paris, A.; Fudickar, W.; Scholz, J.; Tonner, P.H. Neuroendocrine stress response and heart rate variability: A comparison of total intravenous versus balanced anesthesia. Anesth. Analg. 2005, 101, 1700–1705. [Google Scholar] [CrossRef]
- Sabourdin, N.; Barrois, J.; Louvet, N.; Rigouzzo, A.; Guye, M.-L.; Dadure, C.; Constant, I. Pupillometry-guided Intraoperative Remifentanil Administration versus Standard Practice Influences Opioid Use: A Randomized Study. Anesthesiology 2017, 127, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Le Gall, L.; David, A.; Carles, P.; Leuillet, S.; Chastel, B.; Fleureau, C.; Dewitte, A.; Ouattara, A. Benefits of intraoperative analgesia guided by the Analgesia Nociception Index (ANI) in bariatric surgery: An unmatched case-control study. Anaesth. Crit. Care Pain Med. 2019, 38, 35–39. [Google Scholar] [CrossRef]
- Dostalova, V.; Schreiberova, J.; Bartos, M.; Kukralova, L.; Dostal, P. Surgical Pleth Index and Analgesia Nociception Index for intraoperative analgesia in patients undergoing neurosurgical spinal procedures: A comparative randomized study. Minerva Anestesiol. 2019, 85, 1265–1272. [Google Scholar] [CrossRef]
- Anderson, T.A. Intraoperative Analgesia-Nociception Monitors: Where We Are and Where We Want To Be. Anesth. Analg. 2020, 130, 1261–1263. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Thee, C.; Gruenewald, M.; Wnent, J.; Illies, C.; Hoecker, J.; Hanss, R.; Steinfath, M.; Bein, B. Comparison of surgical stress index-guided analgesia with standard clinical practice during routine general anesthesia: A pilot study. Anesthesiology 2010, 112, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Meijer, F.S.; Martini, C.H.; Broens, S.; Boon, M.; Niesters, M.; Aarts, L.; Olofsen, E.; van Velzen, M.; Dahan, A. Nociception-guided versus Standard Care during Remifentanil-Propofol Anesthesia: A Randomized Controlled Trial. Anesthesiology 2019, 130, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Funcke, S.; Pinnschmidt, H.O.; Wesseler, S.; Brinkmann, C.; Beyer, B.; Jazbutyte, V.; Behem, C.R.; Trepte, C.; Nitzschke, R. Guiding Opioid Administration by 3 Different Analgesia Nociception Monitoring Indices During General Anesthesia Alters Intraoperative Sufentanil Consumption and Stress Hormone Release: A Randomized Controlled Pilot Study. Anesth. Analg. 2020, 130, 1264–1273. [Google Scholar] [CrossRef] [PubMed]
- Gruenewald, M.; Willms, S.; Broch, O.; Kott, M.; Steinfath, M.; Bein, B. Sufentanil administration guided by surgical pleth index vs standard practice during sevoflurane anaesthesia: A randomized controlled pilot study. Br. J. Anaesth. 2014, 112, 898–905. [Google Scholar] [CrossRef] [Green Version]
- Meijer, F.; Honing, M.; Roor, T.; Toet, S.; Calis, P.; Olofsen, E.; Martini, C.; van Velzen, M.; Aarts, L.; Niesters, M.; et al. Reduced postoperative pain using Nociception Level-guided fentanyl dosing during sevoflurane anaesthesia: A randomised controlled trial. Br. J. Anaesth. 2020, 125, 1070–1078. [Google Scholar] [CrossRef]
- El Hachem, L.; Small, E.; Chung, P.; Moshier, E.L.; Friedman, K.; Fenske, S.S.; Gretz, H.F. Randomized controlled double-blind trial of transversus abdominis plane block versus trocar site infiltration in gynecologic laparoscopy. Am. J. Obstet. Gynecol. 2015, 212, 182.e1–182.e9. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ANI (n = 38) | Standard (n = 40) | |
|---|---|---|
| Age (years) | 39 ± 10 | 40 ± 7 |
| Weight (kg) | 68 ± 10 | 68 ± 11 |
| Body Mass Index (kg/m2) | 24.9 ± 3.4 | 24.9 ± 3.2 |
| Baseline SBP (mmHg) | 100 ± 14 | 104 ± 14 |
| Baseline HR (bpm) | 70 ± 11 | 70 ± 12 |
| Laparoscopy (n) | 19 | 19 |
| Laparotomy (n) | 19 | 21 |
| ANI (n = 38) | Standard (n = 40) | |
|---|---|---|
| Per-operative data | ||
| Propofol consumption (mg kg−1 h−1) | 8.4 ± 1.7 | 8.1 ± 1.6 |
| Changes in Remifentanil Ce (Total number) | 5 (4; 7) | 5.0 (2; 7) |
| Time to emergence (min) | 13.5 (7.0; 21.0) | 15.5 (10.0; 26.0) |
| Duration of anesthesia (min) | 133 (114; 161) | 168 (135; 212) |
| Patients requiring atropine (n) | 2 | 2 |
| Patients requiring ephedrine (n) | 1 | 2 |
| Patients requiring nicardipine (n) | 1 | 0 |
| Postoperative data | ||
| 12 h cumulative morphine (mg kg−1) | 0.22 (0.17; 0.25) | 0.23 (0.19; 0.32) |
| 24 h cumulative morphine (mg kg−1) | 0.25 (0.21; 0.31) | 0.29 (0.21; 0.39) |
| Proportion of patients requiring nefopam (%) | 73.5% (55.6%; 87.1%) | 75.7% (58.8%; 88.2%) |
| Proportion of patients requiring ketoprofen (%) | 35.3% (19.7%; 53.5%) | 19.4% (8.2%; 36.0%) |
| Nausea/Vomiting (n (%)) | 8 (25%) | 8 (21.6%) |
| Itching (n (%)) | 1 (3.1%) | 0 |
| Urinary retention (n (%)) | 0 | 2 (5.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabourdin, N.; Burey, J.; Tuffet, S.; Thomin, A.; Rousseau, A.; Al-Hawari, M.; Taconet, C.; Louvet, N.; Constant, I. Analgesia Nociception Index-Guided Remifentanil versus Standard Care during Propofol Anesthesia: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 333. https://doi.org/10.3390/jcm11020333
Sabourdin N, Burey J, Tuffet S, Thomin A, Rousseau A, Al-Hawari M, Taconet C, Louvet N, Constant I. Analgesia Nociception Index-Guided Remifentanil versus Standard Care during Propofol Anesthesia: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(2):333. https://doi.org/10.3390/jcm11020333
Chicago/Turabian StyleSabourdin, Nada, Julien Burey, Sophie Tuffet, Anne Thomin, Alexandra Rousseau, Mossab Al-Hawari, Clementine Taconet, Nicolas Louvet, and Isabelle Constant. 2022. "Analgesia Nociception Index-Guided Remifentanil versus Standard Care during Propofol Anesthesia: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 2: 333. https://doi.org/10.3390/jcm11020333