
Everolimus Reduces Cancer Incidence and Improves Patient and Graft Survival Rates after Kidney Transplantation: A Multi-Center Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
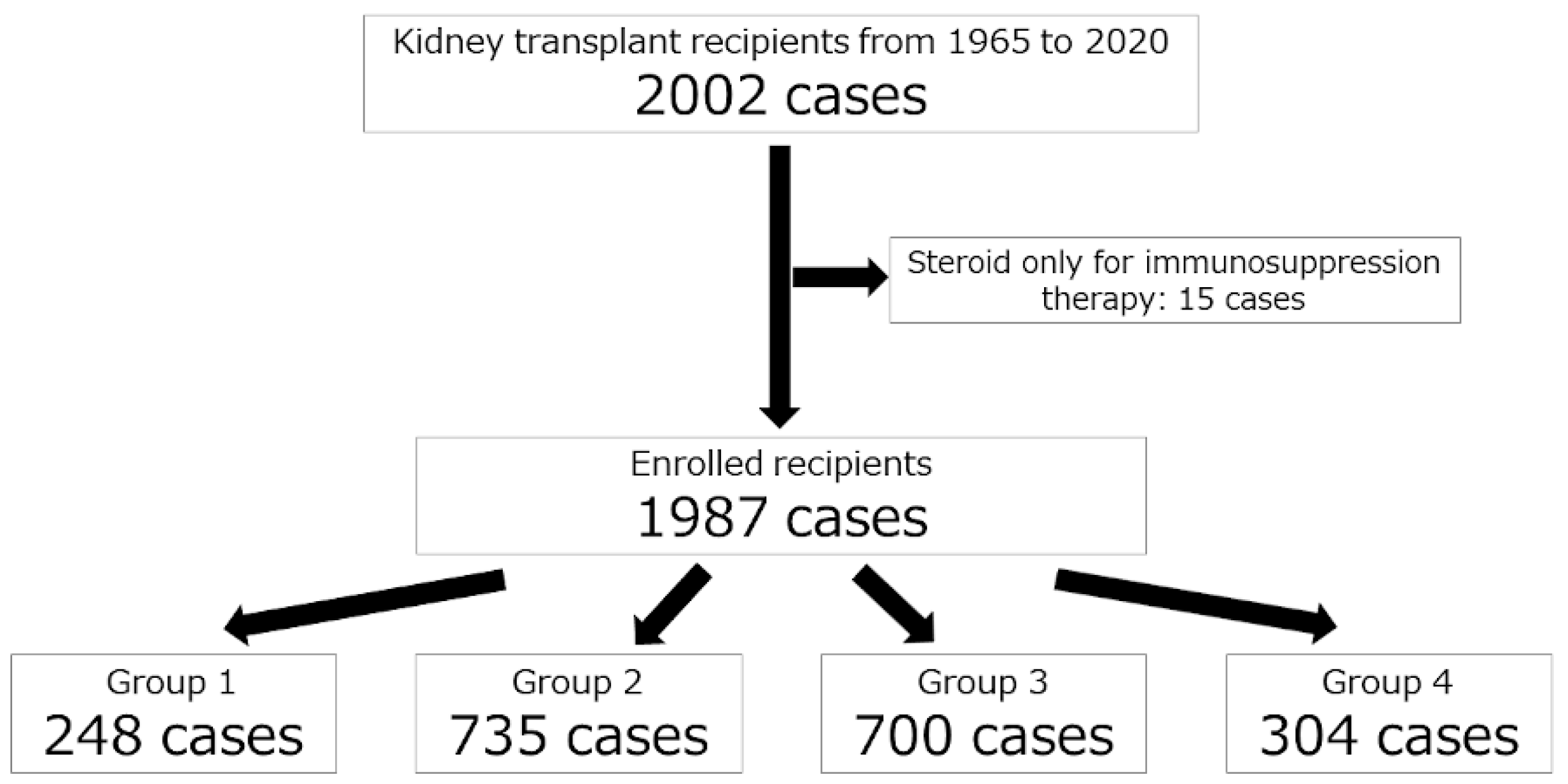
2.1. Patient Characteristics
2.2. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Cumulative de Novo Cancer Incidence Rates after Kidney Transplantation According to the Type of Induction Immunosuppressive Therapy
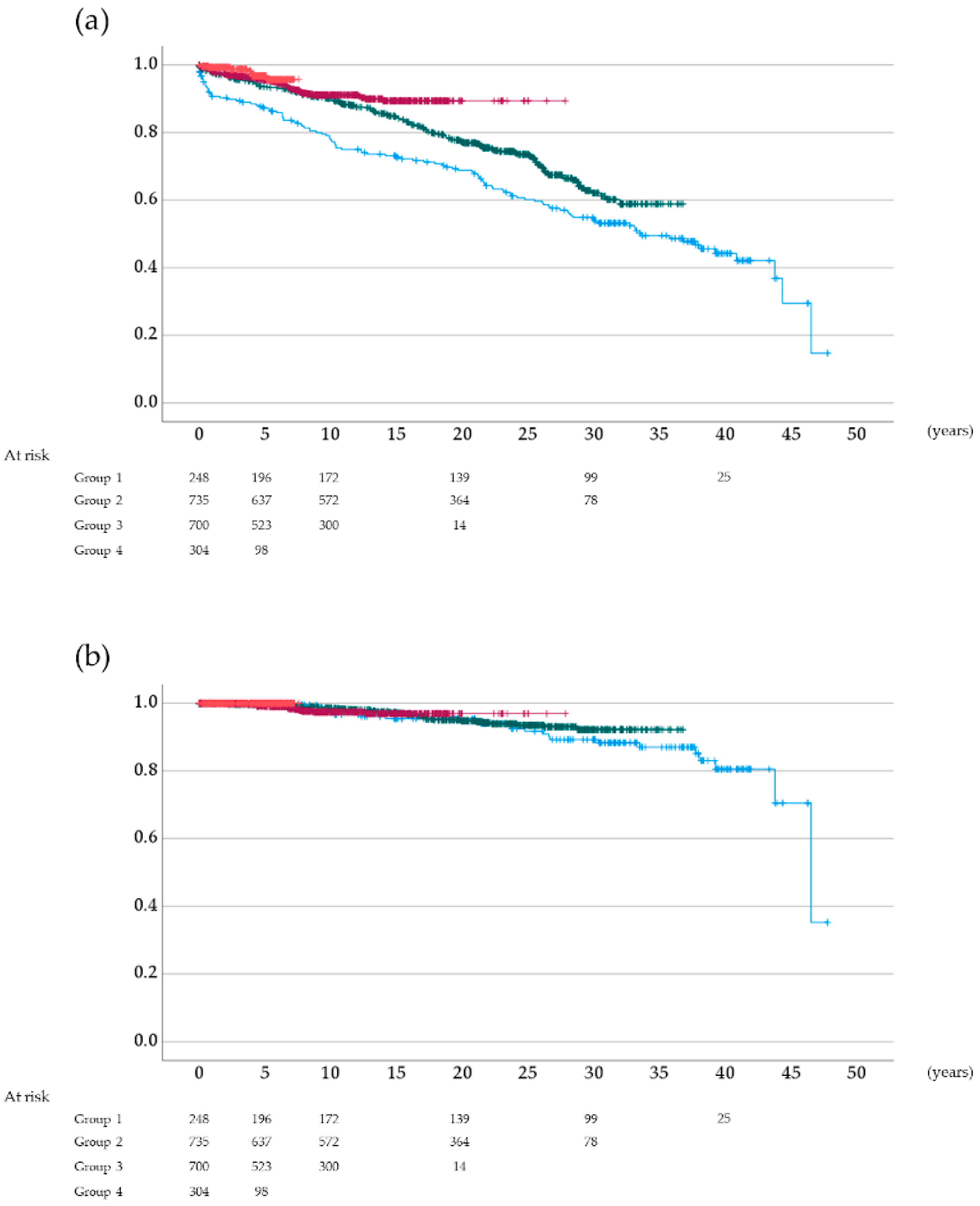
3.3. Overall and Cancer-Specific Survival Rates According to the Type of Induction Immunosuppressive Therapy
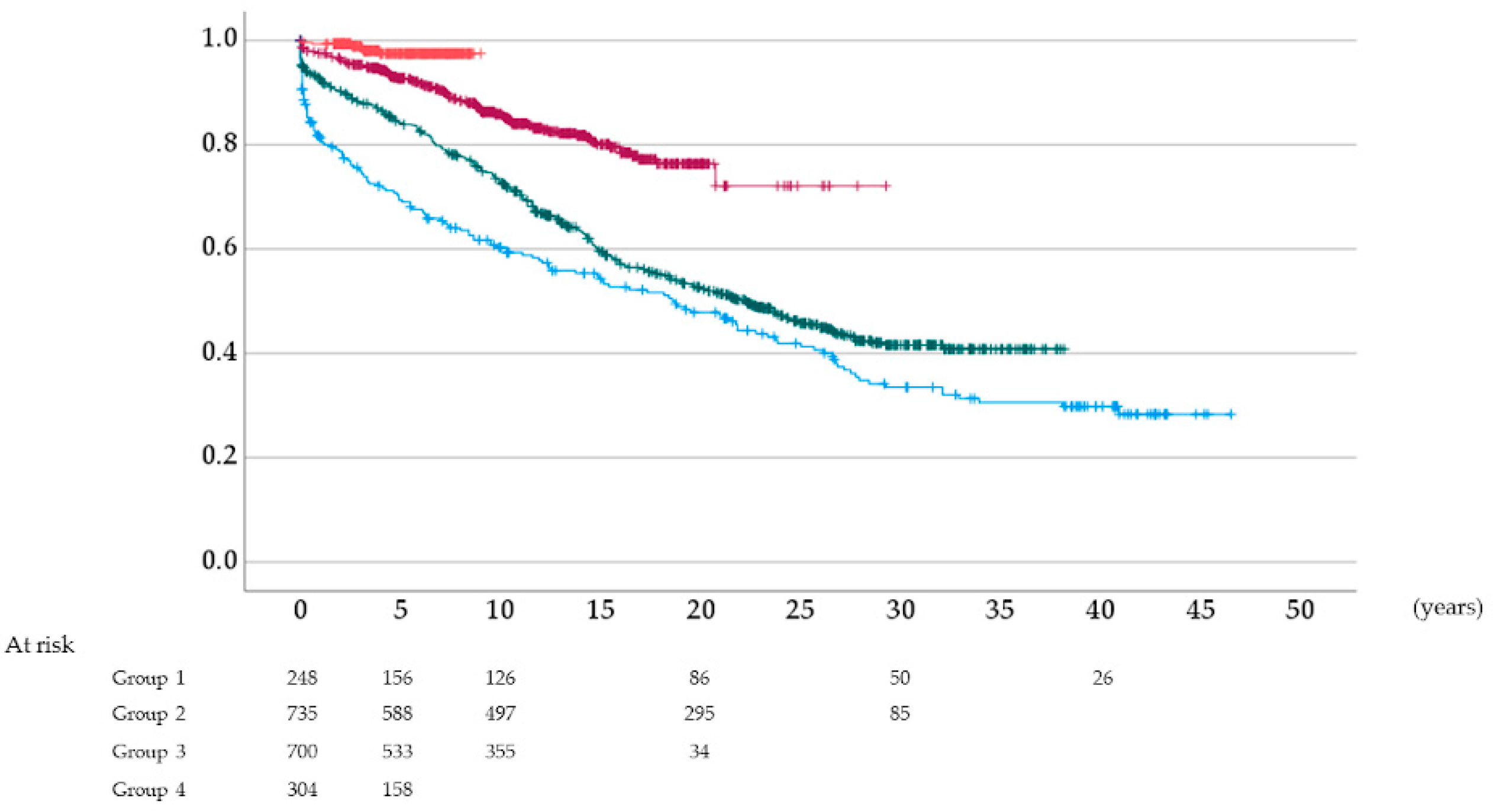
3.4. Graft Survival Rate According to the Type of Induction Immunosuppressive Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abecassis, M.; Bartlett, S.T.; Collins, A.J.; Davis, C.L.; Delmonico, F.L.; Friedewald, J.; Hays, R.; Howard, A.; Jones, E.; Leichtman, A.B.; et al. Kidney Transplantation as Primary Therapy for End-Stage Renal Disease: A National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQI™) Conference. Clin. J. Am. Soc. Nephrol. 2008, 3, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Luan, F.L.; Ding, R.; Sharma, V.K.; Chon, W.J.; Lagman, M.; Suthanthiran, M. Rapamycin is an effective inhibitor of human renal cancer metastasis. Kidney Int. 2003, 63, 917–926. [Google Scholar] [CrossRef] [Green Version]
- Viklicky, O.; Novotny, M.; Hruba, P. Future developments in kidney transplantation. Curr. Opin. Organ Transplant. 2020, 25, 92–98. [Google Scholar] [CrossRef]
- Campistol, J. Minimizing the Risk of Posttransplant Malignancy. Transplant. Proc. 2008, 40, S40–S43. [Google Scholar] [CrossRef]
- Kato, T.; Kakuta, Y.; Abe, T.; Yamanaka, K.; Imamura, R.; Okumi, M.; Ichimaru, N.; Takahara, S.; Nonomura, N. The benefits of cancer screening in kidney transplant recipients: A single-center experience. Cancer Med. 2016, 5, 153–158. [Google Scholar] [CrossRef]
- Bellacosa, A.; Kumar, C.C.; Di Cristofano, A.; Testa, J.R. Activation of AKT Kinases in Cancer: Implications for Therapeutic Targeting. Adv. Cancer Res. 2005, 94, 29–86. [Google Scholar] [CrossRef] [PubMed]
- Bjornsti, M.-A.; Houghton, P.J. The tor pathway: A target for cancer therapy. Nat. Rev. Cancer 2004, 4, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Hudes, G.; Carducci, M.; Tomczak, P.; Dutcher, J.; Figlin, R.; Kapoor, A.; Staroslawska, E.; Sosman, J.; McDermott, D.; Bodrogi, I.; et al. Temsirolimus, Interferon Alfa, or Both for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2007, 356, 2271–2281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansal, I.; Sellers, W.R. The Biology and Clinical Relevance of the PTEN Tumor Suppressor Pathway. J. Clin. Oncol. 2004, 22, 2954–2963. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; Oudard, S.; Hutson, T.E.; Porta, C.; Bracarda, S.; Grünwald, V.; Thompson, J.A.; Figlin, R.A.; Hollaender, N.; et al. Efficacy of everolimus in advanced renal cell carcinoma: A double-blind, randomised, placebo-controlled phase III trial. Lancet 2008, 372, 449–456. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.; et al. Everolimus for Advanced Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Meric-Bernstam, F.; Gonzalez-Angulo, A.M. Targeting the mTOR Signaling Network for Cancer Therapy. J. Clin. Oncol. 2009, 27, 2278–2287. [Google Scholar] [CrossRef]
- Dantal, J.; Soulillou, J.-P. Immunosuppressive Drugs and the Risk of Cancer after Organ Transplantation. N. Engl. J. Med. 2005, 352, 1371–1373. [Google Scholar] [CrossRef]
- Monaco, A.P. The Role of mTOR Inhibitors in the Management of Posttransplant Malignancy. Transplantation 2009, 87, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, B.; Guillemin, A.; Duvoux, C.; Neuzillet, C.; Tlemsani, C.; Compagnon, P.; Azoulay, D.; Salloum, C.; Laurent, A.; de la Taille, A.; et al. Optimal oncologic management and mTOR inhibitor introduction are safe and improve survival in kidney and liver allograft recipients with de novo carcinoma. Int. J. Cancer 2019, 144, 886–896. [Google Scholar] [CrossRef] [Green Version]
- Imamura, R.; Nakazawa, S.; Yamanaka, K.; Kakuta, Y.; Tsutahara, K.; Taniguchi, A.; Kawamura, M.; Kato, T.; Abe, T.; Uemura, M.; et al. Cumulative cancer incidence and mortality after kidney transplantation in Japan: A long-term multicenter cohort study. Cancer Med. 2021, 10, 2205–2215. [Google Scholar] [CrossRef] [PubMed]
- Farrugia, D.; Mahboob, S.; Cheshire, J.; Begaj, I.; Khosla, S.; Ray, D.; Sharif, A. Malignancy-related mortality following kidney transplantation is common. Kidney Int. 2014, 85, 1395–1403. [Google Scholar] [CrossRef] [Green Version]
- Lim, W.H.; Badve, S.V.; Wong, G. Long-term allograft and patient outcomes of kidney transplant recipients with and without incident cancer-a population cohort study. Oncotarget 2017, 8, 77771–77782. [Google Scholar] [CrossRef] [Green Version]
- Badve, S.V.; Pascoe, E.; Burke, M.; Clayton, P.A.; Campbell, S.B.; Hawley, C.; Lim, W.H.; McDonald, S.P.; Wong, G.; Johnson, D.W. Mammalian Target of Rapamycin Inhibitors and Clinical Outcomes in Adult Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2016, 11, 1845–1855. [Google Scholar] [CrossRef] [Green Version]
- Campbell, S.B.; Walker, R.; Tai, S.S.; Jiang, Q.; Russ, G.R. Randomized Controlled Trial of Sirolimus for Renal Transplant Recipients at High Risk for Nonmelanoma Skin Cancer. Arab. Archaeol. Epigr. 2012, 12, 1146–1156. [Google Scholar] [CrossRef]
- Lim, W.H.; Eris, J.; Kanellis, J.; Pussell, B.; Wiid, Z.; Witcombe, D.; Russ, G.R. A Systematic Review of Conversion from Calcineurin Inhibitor to Mammalian Target of Rapamycin Inhibitors for Maintenance Immunosuppression in Kidney Transplant Recipients. Arab. Archaeol. Epigr. 2014, 14, 2106–2119. [Google Scholar] [CrossRef] [PubMed]
- Ying, T.; Wong, G.; Lim, W.; Kanellis, J.; Pilmore, H.; Campbell, S.; Masterson, R.; Walker, R.; O’Connell, P.; Russ, G.; et al. De novo or early conversion to everolimus and long-term cancer outcomes in kidney transplant recipients: A trial-based linkage study. Arab. Archaeol. Epigr. 2018, 18, 2977–2986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kauffman, H.M.; Cherikh, W.S.; Cheng, Y.; Hanto, D.W.; Kahan, B.D. Maintenance Immunosuppression with Target-of-Rapamycin Inhibitors is Associated with a Reduced Incidence of De Novo Malignancies. Transplantation 2005, 80, 883–889. [Google Scholar] [CrossRef]
- Basu, A.; Liu, T.; Banerjee, P.; Flynn, E.; Zurakowski, D.; Datta, D.; Viklicky, O.; Gasser, M.; Waaga-Gasser, A.M.; Yang, J.; et al. Effectiveness of a combination therapy using calcineurin inhibitor and mTOR inhibitor in preventing allograft rejection and post-transplantation renal cancer progression. Cancer Lett. 2012, 321, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Andrassy, J.; Graeb, C.; Rentsch, M.; Jauch, K.-W.; Guba, M. mTOR Inhibition and its Effect on Cancer in Transplantation. Transplantation 2005, 80, S171–S174. [Google Scholar] [CrossRef]
- Hashemolhosseini, S.; Nagamine, Y.; Morley, S.J.; Desrivières, S.; Mercep, L.; Ferrari, S. Rapamycin inhibition of the G1 to S transition is mediated by effects on cyclin D1 mRNA and protein stability. J. Biol. Chem. 1998, 273, 14424–14429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motzer, R.J.; Escudier, B.; Oudard, S.; Hutson, T.E.; Porta, C.; Bracarda, S.; Grünwald, V.; Thompson, J.A.; Figlin, R.A.; Hollaender, N.; et al. Phase 3 trial of everolimus for metastatic renal cell carcinoma: Final results and analysis of prognostic factors. Cancer 2010, 116, 4256–4265. [Google Scholar] [CrossRef]
- Franz, D.N.; Belousova, E.; Sparagana, S.; Bebin, E.M.; Frost, M.; Kuperman, R.; Witt, O.; Kohrman, M.H.; Flamini, J.R.; Wu, J.Y.; et al. Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet 2013, 381, 125–132. [Google Scholar] [CrossRef]
- Ekberg, H.; Tedesco-Silva, H.; Demirbas, A.; Vítko, Š.; Nashan, B.; Guerkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced Exposure to Calcineurin Inhibitors in Renal Transplantation. N. Engl. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponticelli, C.; Scolari, M. Calcineurin Inhibitors in Renal Transplantation Still Needed but in Reduced Doses: A Review. Transplant. Proc. 2010, 42, 2205–2208. [Google Scholar] [CrossRef]
- Croze, L.E.; Tetaz, R.; Roustit, M.; Malvezzi, P.; Janbon, B.; Jouve, T.; Pinel, N.; Masson, D.; Quesada, J.L.; Bayle, F.; et al. Conversion to mammalian target of rapamycin inhibitors increases risk of de novo donor-specific antibodies. Transpl. Int. 2014, 27, 775–783. [Google Scholar] [CrossRef]
- Lederer, S.R.; Friedrich, N.; Banas, B.; Welser, G.; Albert, E.D.; Sitter, T. Effects of mycophenolate mofetil on donor-specific antibody formation in renal transplantation. Clin. Transplant. 2005, 19, 168–174. [Google Scholar] [CrossRef]
- Terasaki, P.I.; Ozawa, M. Predicting Kidney Graft Failure by HLA Antibodies: A Prospective Trial. Arab. Archaeol. Epigr. 2004, 4, 438–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.; Turner, R.M.; Chapman, J.R.; Howell, M.; Lim, W.H.; Webster, A.C.; Craig, J.C. Time on Dialysis and Cancer Risk After Kidney Transplantation. Transplantation 2013, 95, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Andrés, V.; Castro, C.; Campistol, J.M. Potential role of proliferation signal inhibitors on atherosclerosis in renal transplant patients. Nephrol. Dial. Transplant. 2006, 21, iii14–iii17. [Google Scholar] [CrossRef] [Green Version]
- Zeier, M.; van der Giet, M. Calcineurin inhibitor sparing regimens using m-target of rapamycin inhibitors: An opportunity to improve cardiovascular risk following kidney transplantation? Transpl. Int. 2010, 24, 30–42. [Google Scholar] [CrossRef]
- Nashan, B.; Curtis, J.; Ponticelli, C.; Mourad, G.; Jaffe, J.; Haas, T. Everolimus and Reduced-Exposure Cyclosporine in de novo Renal-Transplant Recipients: A Three-Year Phase II, Randomized, Multicenter, Open-Label Study. Transplantation 2004, 78, 1332–1340. [Google Scholar] [CrossRef]
- Silva, H.T., Jr.; Cibrik, D.; Johnston, T.; Lackova, E.; Mange, K.; Panis, C.; Walker, R.; Wang, Z.; Zibari, G.B.; Kim, Y.S. Everolimus Plus Reduced-Exposure CsA versus Mycophenolic Acid Plus Standard-Exposure CsA in Renal-Transplant Recipients. Arab. Archaeol. Epigr. 2010, 10, 1401–1413. [Google Scholar] [CrossRef] [PubMed]
- Vítko, Š.; Margreiter, R.; Weimar, W.; Dantal, J.; Kuypers, D.; Winkler, M.; Øyen, O.; Viljoen, H.G.; Filiptsev, P.; Sadek, S.; et al. Three-Year Efficacy and Safety Results from a Study of Everolimus Versus Mycophenolate Mofetil in de novo Renal Transplant Patients. Arab. Archaeol. Epigr. 2005, 5, 2521–2530. [Google Scholar] [CrossRef] [PubMed]
- Kahwaji, J.; Bunnapradist, S.; Hsu, J.-W.; Idroos, M.L.; Dudek, R. Cause of Death With Graft Function Among Renal Transplant Recipients in an Integrated Healthcare System. Transplantation 2011, 91, 225–230. [Google Scholar] [CrossRef]
- Sánchez-Fructuoso, A.; Ruiz, J.; Pérez-Flores, I.; Alamillo, C.G.; Romero, N.C.; Arias, M. Comparative Analysis of Adverse Events Requiring Suspension of mTOR Inhibitors: Everolimus versus Sirolimus. Transplant. Proc. 2010, 42, 3050–3052. [Google Scholar] [CrossRef] [PubMed]
- Eertwegh, A.J.V.D.; Karakiewicz, P.; Bavbek, S.; Rha, S.Y.; Bracarda, S.; Bahl, A.; Ou, Y.-C.; Kim, D.; Panneerselvam, A.; Anak, O.; et al. Safety of Everolimus by Treatment Duration in Patients With Advanced Renal Cell Cancer in an Expanded Access Program. Urology 2013, 81, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Ventura-Aguiar, P.; Campistol, J.M.; Diekmann, F. Safety of mTOR inhibitors in adult solid organ transplantation. Expert Opin. Drug Saf. 2016, 15, 303–319. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 | Group 3 | Group 4 | p-Value | ||
|---|---|---|---|---|---|---|
| The Number of Patients | 248 | 735 | 700 | 304 | ||
| Follow-up duration (yr) | 21.6 (15.0) | 18.8 (10.0) | 10.7 (5.8) | 4.9 (2.2) | <0.001 | |
| Recipient age (yr) | <30 | 141 (63.2) | 248 (36.1) | 108 (16.3) | 25 (9.5) | <0.001 |
| 30–45 | 100 (34.2) | 367 (47.6) | 265 (33.8) | 89 (30.4) | ||
| 46–60 | 7 (2.6) | 113 (15.5) | 234 (35.7) | 128 (36.7) | ||
| >61 | 0 (0.0) | 7 (0.8) | 93 (14.2) | 62 (23.4) | ||
| Recipient sex | Female | 89 (35.9) | 294 (40.0) | 268 (38.3) | 113 (37.2) | 0.648 |
| Male | 159 (64.1) | 441 (60.0) | 432 (61.7) | 191 (62.8) | ||
| Donor type | living | 214 (86.3) | 539 (73.3) | 615 (87.9) | 273 (89.8) | <0.001 |
| deceased | 34 (13.7) | 196 (26.7) | 85 (12.1) | 31 (10.2) | ||
| Blood relation | Yes | 214 (86.3) | 530 (72.1) | 432 (61.7) | 146 (48.0) | <0.001 |
| ABO blood-type | compatible | 248 (100.0) | 715 (97.3) | 548 (78.3) | 201 (66.1) | <0.001 |
| incompatible | 0 (0.0) | 20 (2.7) | 152 (21.7) | 103 (33.9) | ||
| Number of HLA mismatches | A, B, DR | 0.64 (1.01) | 1.39 (1.06) | 1.80 (1.26) | 1.79 (1.29) | <0.001 |
| Body mass index (kg/m2) | 21.5 (1.47) | 21.3 (1.55) | 21.3 (2.57) | 21.4 (3.33) | 0.417 | |
| Dialysis duration (yr) | 0 | 7 (3.1) | 17 (2.6) | 109 (18.6) | 89 (26.6) | <0.001 |
| <1, ≤1 | 91 (36.8) | 202 (27.0) | 153 (21.7) | 59 (20.3) | ||
| 1–3, ≤3 | 92 (25.0) | 215 (17.1) | 147 (12.3) | 61 (16.5) | ||
| 3–5, ≤5 | 38 (27.6) | 111 (28.0) | 69 (16.3) | 23 (17.7) | ||
| 5–10, ≤10 | 19 (7.0) | 130 (17.3) | 86 (12.3) | 31 (7.0) | ||
| 10–20, ≤20 | 1 (0.4) | 51 (6.8) | 94 (13.1) | 29 (8.2) | ||
| >20 | 0 (0.0) | 9 (1.1) | 42 (5.7) | 12 (3.8) | ||
| Calcineulin inhibitors | Cyclosporine | 0 (0.0) | 552 (75.1) | 212 (30.3) | 17 (5.6) | <0.001 |
| Tacrolimus | 0 (0.0) | 183 (24.9) | 488 (69.7) | 287 (94.4) | ||
| none | 248 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Antiproliferative agents | Azathioprine | 248 (100.0) | 361 (49.1) | 0 (0.0) | 1 (0.3) | <0.001 |
| Mizoribine | 0 (0.0) | 321 (43.7) | 0 (0.0) | 3 (1.0) | ||
| Mycophenolate mofetil | 0 (0.0) | 0 (0.0) | 700 (100.0) | 300 (98.7) | ||
| none | 0 (0.0) | 53 (7.2) | 0 (0.0) | 0 (0.0) | ||
| mTOR inhibitor (everolimus) | induction therapy | 0 (0.0) | 0 (0.0) | 0 (0.0) | 155 (51.0) | <0.001 |
| add-on within 3 months | 0 (0.0) | 0 (0.0) | 0 (0.0) | 149 (49.0) | ||
| History of rejection | Yes | 145 (58.5) | 519 (70.6) | 165 (23.6) | 31 (10.2) | <0.001 |
| History of transplantation | Yes | 6 (2.4) | 17 (2.3) | 42 (6.0) | 21 (7.6) | <0.001 |
| History of transfusion | Yes | 87 (35.1) | 116 (15.8) | 148 (21.1) | 70 (23.0) | <0.001 |
| Group 1 | Group 2 | Group 3 | Group 4 | p-Value | ||
|---|---|---|---|---|---|---|
| The Number of Patients | 42 (16.9) | 119 (16.2) | 80 (11.7) | 1 (0.3) | ||
| Number of yrs from KTP to diagnosis of cancer (yr) | 21.9 (9.7) | 14.5 (7.2) | 6.9 (4.6) | 1.2 (-) | <0.001 | |
| Recipient age (yr) | <30 | 20 (47.6) | 23 (19.3) | 10 (12.5) | 0 (0.0) | <0.001 |
| 30–45 | 19 (45.2) | 72 (60.5) | 25 (31.2) | 0 (0.0) | ||
| 46–60 | 3 (7.2) | 23 (19.3) | 32 (40.0) | 1 (100.0) | ||
| >61 | 0 (0.0) | 1 (0.9) | 13 (16.3) | 0 (0.0) | ||
| Recipient sex | Female | 15 (35.7) | 52 (43.7) | 38 (47.5) | 0 (0.0) | 0.501 |
| Male | 27 (64.3) | 67 (56.3) | 42 (52.5) | 1 (100.0) | ||
| Donor type | living | 36 (85.7) | 81 (68.1) | 72 (90.0) | 1 (100.0) | 0.02 |
| deceased | 6 (14.3) | 38 (31.9) | 8 (10.0) | 0 (0.0) | ||
| Blood relation | Yes | 36 (85.7) | 81 (67.8) | 48 (60.0) | 1 (100.0) | 0.028 |
| ABO blood-type | compatible | 42 (100.0) | 117 (98.3) | 59 (73.8) | 1 (100.0) | <0.001 |
| incompatible | 0 (0.0) | 2 (1.7) | 21 (26.2) | 0 (0.0) | ||
| Number of HLA mismatches | A, B, DR | 1.17 (1.32) | 2.02 (1.02) | 2.99 (1.51) | 3.00 (-) | <0.001 |
| Body mass index (kg/m2) | 21.8 (1.28) | 21.3 (1.58) | 21.3 (2.36) | 27.64 (-) | 0.11 | |
| Dialysis duration (yr) | 0 | 2 (4.8) | 3 (2.5) | 6 (7.5) | 1 (100.0) | 0.02 |
| ≤1 | 9 (21.4) | 22 (18.5) | 13 (16.3) | 0 (0.0) | ||
| 1<, ≤2 | 10 (23.8) | 18 (15.1) | 9 (11.3) | 0 (0.0) | ||
| 2<, ≤5 | 13 (31.0) | 32 (26.9) | 20 (25.0) | 0 (0.0) | ||
| 5<, ≤10 | 6 (14.3) | 23 (19.3) | 13 (16.3) | 0 (0.0) | ||
| 10<, ≤20 | 0 (0.0) | 12 (10.1) | 13 (16.3) | 0 (0.0) | ||
| >20 | 0 (0.0) | 3 (2.5) | 6 (7.5) | 0 (0.0) | ||
| Calcineulin inhibitors | Cyclosporine | 0 (0.0) | 88 (73.9) | 34 (41.4) | 0 (0.0) | <0.001 |
| Tacrolimus | 0 (0.0) | 31 (26.1) | 46 (58.5) | 1 (100.0) | ||
| none | 42 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Antiproliferative agents | Azathioprine | 42 (100.0) | 69 (58.0) | 0 (0.0) | 0 (0.0) | <0.001 |
| Mizoribine | 0 (0.0) | 44 (42.0) | 0 (0.0) | 0 (0.0) | ||
| Mcophenolatemofetil | 0 (0.0) | 0 (0.0) | 80 (100.0) | 1 (100.0) | ||
| none | 0 (0.0) | 6 (5.1) | 0 (0.0) | 0 (0.0) | ||
| mTOR inhibitor | everolimus | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | |
| History of rejection | Yes | 24 (57.1) | 85 (71.4) | 24 (30.5) | 0 (0.0) | <0.001 |
| History of transplantation | Yes | 1 (2.4) | 4 (3.4) | 6 (8.5) | 1 (100.0) | <0.001 |
| History of transfusion | Yes | 23 (54.8) | 26 (21.8) | 15 (23.2) | 1 (100.0) | <0.001 |
| Group 1 | Group 2 | Group 3 | Group 4 | |
|---|---|---|---|---|
| The number of recipients | 248 | 735 | 700 | 304 |
| Total cancer-positive recipients | 42 (16.9) | 119 (16.2) | 80 (11.7) | 1 (0.3) |
| Double cancer-positive recipients | 6 | 12 | 9 | 0 |
| Triple cancer-positive recipients | 4 | 1 | 0 | 0 |
| Type of cancer | ||||
| PTLD | 3 | 21 | 13 | 1 |
| renal cell carcinoma | 2 | 12 | 13 | 0 |
| breast cancer | 4 | 13 | 13 | 0 |
| skin cancer (melanoma) | 0 | 0 | 1 | 0 |
| skin cancer (non-melanoma) | 10 | 12 | 9 | 0 |
| prostate cancer | 1 | 5 | 5 | 0 |
| colorectal cancer | 5 | 7 | 6 | 0 |
| uterus cancer | 2 | 10 | 5 | 0 |
| gastric cancer | 5 | 8 | 5 | 0 |
| urothelial cancer | 2 | 6 | 4 | 0 |
| thyroid cancer | 1 | 6 | 3 | 0 |
| tongue cancer | 3 | 7 | 2 | 0 |
| pancreas cancer | 0 | 2 | 2 | 0 |
| hepatocellular carcinoma | 5 | 7 | 1 | 0 |
| lung cancer | 2 | 1 | 0 | 0 |
| ovarian cancer | 1 | 1 | 0 | 0 |
| vaginal cancer | 0 | 1 | 0 | 0 |
| anal cancer | 0 | 1 | 0 | 0 |
| others | 10 | 13 | 7 | 0 |
| Total | 56 | 133 | 89 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, R.; Tanaka, R.; Taniguchi, A.; Nakazawa, S.; Kato, T.; Yamanaka, K.; Namba-Hamano, T.; Kakuta, Y.; Abe, T.; Tsutahara, K.; et al. Everolimus Reduces Cancer Incidence and Improves Patient and Graft Survival Rates after Kidney Transplantation: A Multi-Center Study. J. Clin. Med. 2022, 11, 249. https://doi.org/10.3390/jcm11010249
Imamura R, Tanaka R, Taniguchi A, Nakazawa S, Kato T, Yamanaka K, Namba-Hamano T, Kakuta Y, Abe T, Tsutahara K, et al. Everolimus Reduces Cancer Incidence and Improves Patient and Graft Survival Rates after Kidney Transplantation: A Multi-Center Study. Journal of Clinical Medicine. 2022; 11(1):249. https://doi.org/10.3390/jcm11010249
Chicago/Turabian StyleImamura, Ryoichi, Ryo Tanaka, Ayumu Taniguchi, Shigeaki Nakazawa, Taigo Kato, Kazuaki Yamanaka, Tomoko Namba-Hamano, Yoichi Kakuta, Toyofumi Abe, Koichi Tsutahara, and et al. 2022. "Everolimus Reduces Cancer Incidence and Improves Patient and Graft Survival Rates after Kidney Transplantation: A Multi-Center Study" Journal of Clinical Medicine 11, no. 1: 249. https://doi.org/10.3390/jcm11010249