
A Systematic Review of the Safety of Blocking the IL-1 System in Human Pregnancy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources, Search Strategy and Eligibility Criteria
2.2. Data Extraction
2.3. Assessment of Risk of Bias and Methodological Quality
2.4. Data Synthesis
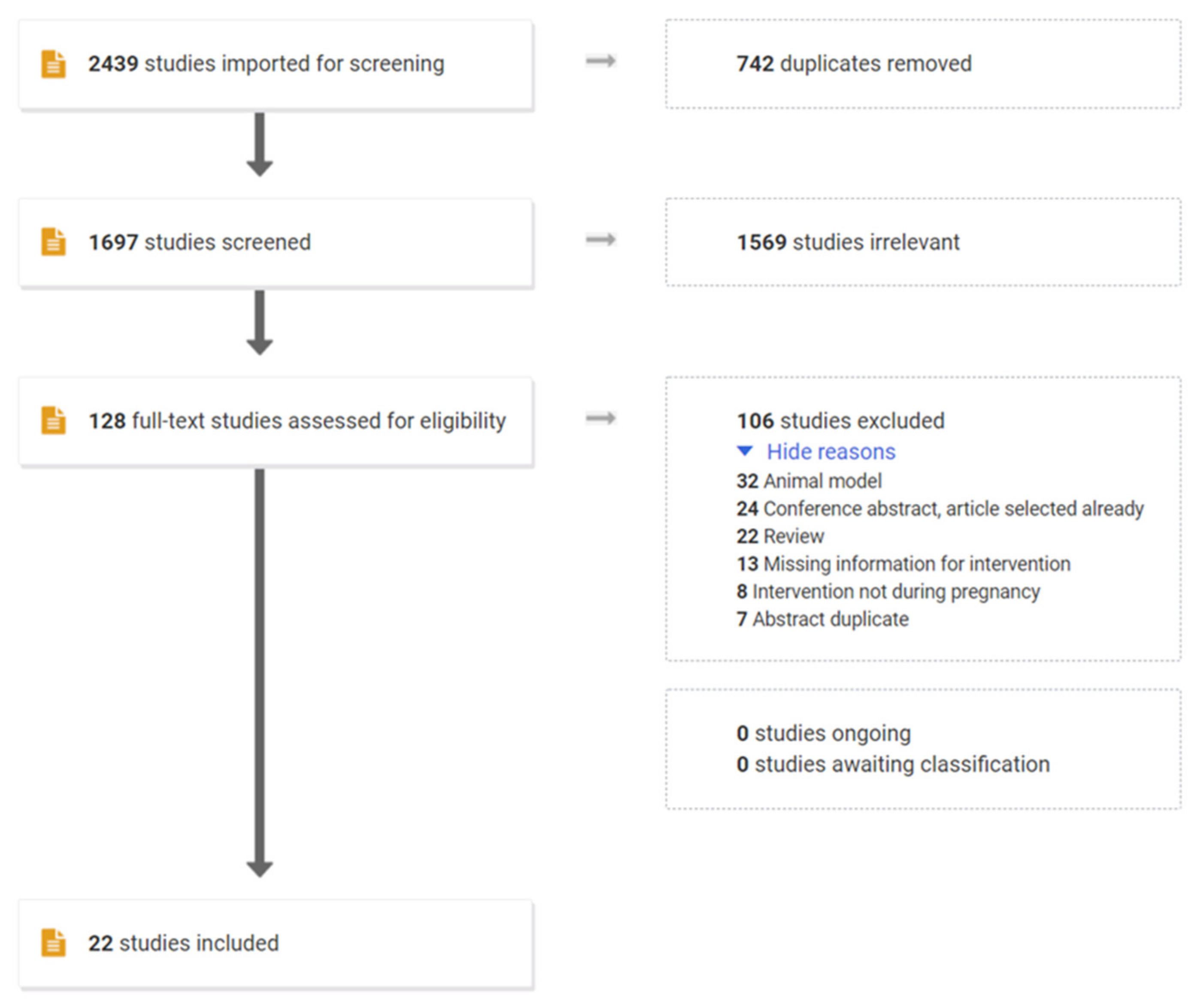
3. Results
3.1. Risk of Bias/Methodological Quality of Included Studies
3.2. Study Characteristics
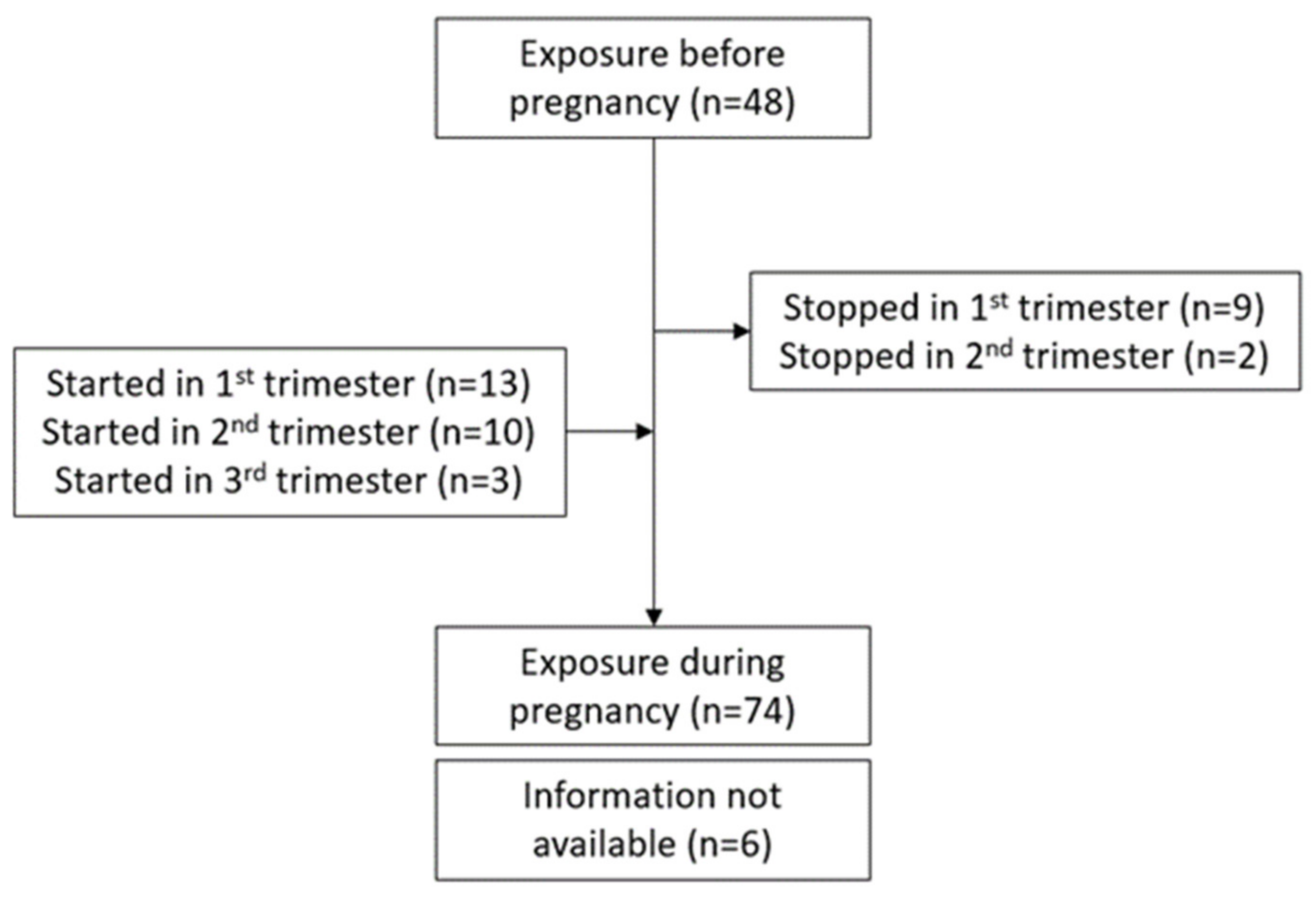
3.3. Duration of Exposure to Drugs during Pregnancy
3.4. Anakinra Use during Pregnancy and Maternal/Fetal Outcome
3.5. Canakinumab Use during Pregnancy and Maternal/Fetal Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aye, I.L.; Jansson, T.; Powell, T.L. Interleukin-1beta inhibits insulin signaling and prevents insulin-stimulated system A amino acid transport in primary human trophoblasts. Mol. Cell. Endocrinol. 2013, 381, 46–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bainbridge, S.A.; Roberts, J.M.; von Versen-Hoynck, F.; Koch, J.; Edmunds, L.; Hubel, C.A. Uric acid attenuates trophoblast invasion and integration into endothelial cell monolayers. Am. J. Physiol. Cell Physiol. 2009, 297, C440–C450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bainbridge, S.A.; von Versen-Höynck, F.; Roberts, J.M. Uric acid inhibits placental system A amino acid uptake. Placenta 2009, 30, 195–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, J.; Vermillion, M.S.; Jia, B.; Xie, H.; Xie, L.; McLane, M.W.; Sheffield, J.S.; Pekosz, A.; Brown, A.; Klein, S.L.; et al. IL-1 receptor antagonist therapy mitigates placental dysfunction and perinatal injury following Zika virus infection. JCI Insight 2019, 4, e122678. [Google Scholar] [CrossRef]
- Mulla, M.J.; Myrtolli, K.; Potter, J.; Boeras, C.; Kavathas, P.B.; Sfakianaki, A.K.; Tadesse, S.; Norwitz, E.R.; Guller, S.; Abrahams, V.M. Uric acid induces trophoblast IL-1beta production via the inflammasome: Implications for the pathogenesis of preeclampsia. Am. J. Reprod. Immunol. 2011, 65, 542–548. [Google Scholar] [CrossRef] [Green Version]
- Brien, M.E.; Duval, C.; Palacios, J.; Boufaied, I.; Hudon-Thibeault, A.A.; Nadeau-Vallee, M.; Vaillancourt, C.; Sibley, C.P.; Abrahams, V.M.; Jones, R.L.; et al. Uric Acid Crystals Induce Placental Inflammation and Alter Trophoblast Function via an IL-1-Dependent Pathway: Implications for Fetal Growth Restriction. J. Immunol. 2017, 198, 443–451. [Google Scholar] [CrossRef] [Green Version]
- Depino, A.M. Perinatal inflammation and adult psychopathology: From preclinical models to humans. Semin. Cell Dev. Biol. 2018, 77, 104–114. [Google Scholar] [CrossRef]
- Hagberg, H.; Gressens, P.; Mallard, C. Inflammation during fetal and neonatal life: Implications for neurologic and neuropsychiatric disease in children and adults. Ann. Neurol. 2012, 71, 444–457. [Google Scholar]
- Van Vliet, E.O.; de Kieviet, J.F.; van der Voorn, J.P.; Been, J.V.; Oosterlaan, J.; van Elburg, R.M. Placental pathology and long-term neurodevelopment of very preterm infants. Am. J. Obstet. Gynecol. 2012, 206, e481–e487. [Google Scholar] [CrossRef] [Green Version]
- Neiger, R. Long-Term Effects of Pregnancy Complications on Maternal Health: A Review. J. Clin. Med. 2017, 6, 76. [Google Scholar] [CrossRef] [Green Version]
- Erlebacher, A. Immunology of the maternal-fetal interface. Annu. Rev. Immunol. 2013, 31, 387–411. [Google Scholar] [CrossRef]
- Moffett, A.; Loke, C. Immunology of placentation in eutherian mammals. Nat. Rev. Immunol. 2006, 6, 584–594. [Google Scholar] [CrossRef]
- Mor, G.; Cardenas, I.; Abrahams, V.; Guller, S. Inflammation and pregnancy: The role of the immune system at the implantation site. Ann. N. Y. Acad. Sci. 2011, 1221, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Menon, R.; Richardson, L.S.; Lappas, M. Fetal membrane architecture, aging and inflammation in pregnancy and parturition. Placenta 2019, 79, 40–45. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Gonçalves, L.F.; Kusanovic, J.P.; Friel, L.A.; Nien, J.K. Inflammation in preterm and term labour and delivery. Semin. Fetal Neonatal Med. 2006, 11, 317–326. [Google Scholar] [CrossRef]
- Brien, M.E.; Boufaied, I.; Bernard, N.; Forest, J.C.; Giguere, Y.; Girard, S. Specific inflammatory profile in each pregnancy complication: A comparative study. Am. J. Reprod. Immunol. 2020, 84, e13316. [Google Scholar] [CrossRef]
- Salazar Garcia, M.D.; Mobley, Y.; Henson, J.; Davies, M.; Skariah, A.; Dambaeva, S.; Gilman-Sachs, A.; Beaman, K.; Lampley, C.; Kwak-Kim, J. Early pregnancy immune biomarkers in peripheral blood may predict preeclampsia. J. Reprod. Immunol. 2018, 125, 25–31. [Google Scholar] [CrossRef]
- Freeman, D.J.; McManus, F.; Brown, E.A.; Cherry, L.; Norrie, J.; Ramsay, J.E.; Clark, P.; Walker, I.D.; Sattar, N.; Greer, I.A. Short- and long-term changes in plasma inflammatory markers associated with preeclampsia. Hypertension 2004, 44, 708–714. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, K.K.; Meeker, J.D.; McElrath, T.F.; Mukherjee, B.; Cantonwine, D.E. Repeated measures of inflammation and oxidative stress biomarkers in preeclamptic and normotensive pregnancies. Am. J. Obstet. Gynecol. 2017, 216, e521–e527. [Google Scholar] [CrossRef] [Green Version]
- Redman, C.W.; Staff, A.C. Preeclampsia, biomarkers, syncytiotrophoblast stress, and placental capacity. Am. J. Obstet. Gynecol. 2015, 213, S9.e1–S9.e4. [Google Scholar] [CrossRef]
- Taylor, B.D.; Ness, R.B.; Klebanoff, M.A.; Zoh, R.; Bass, D.; Hougaard, D.M.; Skogstrand, K.; Haggerty, C.L. First and second trimester immune biomarkers in preeclamptic and normotensive women. Pregnancy Hypertens. 2016, 6, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Taylor, B.D.; Tang, G.; Ness, R.B.; Olsen, J.; Hougaard, D.M.; Skogstrand, K.; Roberts, J.M.; Haggerty, C.L. Mid-pregnancy circulating immune biomarkers in women with preeclampsia and normotensive controls. Pregnancy Hypertens. 2016, 6, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Ronzoni, S.; Steckle, V.; D’Souza, R.; Murphy, K.E.; Lye, S.; Shynlova, O. Cytokine Changes in Maternal Peripheral Blood Correlate With Time-to-Delivery in Pregnancies Complicated by Premature Prelabor Rupture of the Membranes. Reprod. Sci. 2018, 26, 1266–1276. [Google Scholar] [CrossRef]
- Giguere, Y.; Masse, J.; Theriault, S.; Bujold, E.; Lafond, J.; Rousseau, F.; Forest, J.C. Screening for pre-eclampsia early in pregnancy: Performance of a multivariable model combining clinical characteristics and biochemical markers. BJOG 2015, 122, 402–410. [Google Scholar] [CrossRef]
- Kuc, S.; Wortelboer, E.J.; van Rijn, B.B.; Franx, A.; Visser, G.H.; Schielen, P.C. Evaluation of 7 serum biomarkers and uterine artery Doppler ultrasound for first-trimester prediction of preeclampsia: A systematic review. Obstet. Gynecol. Surv. 2011, 66, 225–239. [Google Scholar] [CrossRef] [Green Version]
- Yu, N.; Cui, H.; Chen, X.; Chang, Y. First trimester maternal serum analytes and second trimester uterine artery Doppler in the prediction of preeclampsia and fetal growth restriction. Taiwan J. Obstet. Gynecol. 2017, 56, 358–361. [Google Scholar] [CrossRef]
- Bianchi, M.E. DAMPs, PAMPs and alarmins: All we need to know about danger. J. Leukoc. Biol. 2007, 81, 1–5. [Google Scholar] [CrossRef]
- Matzinger, P. The danger model: A renewed sense of self. Science 2002, 296, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Brien, M.E.; Baker, B.; Duval, C.; Gaudreault, V.; Jones, R.L.; Girard, S. Alarmins at the maternal-fetal interface: Involvement of inflammation in placental dysfunction and pregnancy complications (1). Can. J. Physiol. Pharmacol. 2019, 97, 206–212. [Google Scholar] [CrossRef]
- Nadeau-Vallee, M.; Obari, D.; Palacios, J.; Brien, M.E.; Duval, C.; Chemtob, S.; Girard, S. Sterile inflammation and pregnancy complications: A review. Reproduction 2016, 152, R277–R292. [Google Scholar] [CrossRef]
- Sharps, M.C.; Baker, B.C.; Guevara, T.; Bischof, H.; Jones, R.L.; Greenwood, S.L.; Heazell, A.E.P. Increased placental macrophages and a pro-inflammatory profile in placentas and maternal serum in infants with a decreased growth rate in the third trimester of pregnancy. Am. J. Reprod. Immunol. 2020, 84, e13267. [Google Scholar] [CrossRef] [PubMed]
- Saji, F.; Samejima, Y.; Kamiura, S.; Sawai, K.; Shimoya, K.; Kimura, T. Cytokine production in chorioamnionitis. J. Reprod. Immunol. 2000, 47, 185–196. [Google Scholar] [CrossRef]
- Russo, R.C.; Garcia, C.C.; Teixeira, M.M. Anti-inflammatory drug development: Broad or specific chemokine receptor antagonists? Curr. Opin. Drug Discov. Dev. 2010, 13, 414–427. [Google Scholar]
- Grainger, D.J.; Reckless, J. Broad-spectrum chemokine inhibitors (BSCIs) and their anti-inflammatory effects in vivo. Biochem. Pharmacol. 2003, 65, 1027–1034. [Google Scholar] [CrossRef]
- Bandoli, G.; Palmsten, K.; Forbess Smith, C.J.; Chambers, C.D. A Review of Systemic Corticosteroid Use in Pregnancy and the Risk of Select Pregnancy and Birth Outcomes. Rheum. Dis. Clin. N. Am. 2017, 43, 489–502. [Google Scholar] [CrossRef]
- Shanks, A.L.; Grasch, J.L.; Quinney, S.K.; Haas, D.M. Controversies in antenatal corticosteroids. Semin. Fetal Neonatal Med. 2019, 24, 182–188. [Google Scholar] [CrossRef]
- Wapner, R.J.; Sorokin, Y.; Mele, L.; Johnson, F.; Dudley, D.J.; Spong, C.Y.; Peaceman, A.M.; Leveno, K.J.; Malone, F.; Caritis, S.N.; et al. Long-term outcomes after repeat doses of antenatal corticosteroids. N. Engl. J. Med. 2007, 357, 1190–1198. [Google Scholar] [CrossRef]
- Bandyopadhyay, A.; Slaven, J.E.; Evrard, C.; Tiller, C.; Haas, D.M.; Tepper, R.S. Antenatal corticosteriods decrease forced vital capacity in infants born fullterm. Pediatr. Pulmonol. 2020, 55, 2630–2634. [Google Scholar] [CrossRef]
- Bérard, A.; Sheehy, O.; Girard, S.; Zhao, J.P.; Bernatsky, S. Risk of preterm birth following late pregnancy exposure to NSAIDs or COX-2 inhibitors. Pain 2018, 159, 948–955. [Google Scholar] [CrossRef]
- Daniel, S.; Matok, I.; Gorodischer, R.; Koren, G.; Uziel, E.; Wiznitzer, A.; Levy, A. Major malformations following exposure to nonsteroidal antiinflammatory drugs during the first trimester of pregnancy. J. Rheumatol. 2012, 39, 2163–2169. [Google Scholar] [CrossRef]
- Kenyon, S.; Pike, K.; Jones, D.R.; Brocklehurst, P.; Marlow, N.; Salt, A.; Taylor, D.J. Childhood outcomes after prescription of antibiotics to pregnant women with spontaneous preterm labour: 7-year follow-up of the ORACLE II trial. Lancet 2008, 372, 1319–1327. [Google Scholar] [CrossRef] [Green Version]
- Kenyon, S.; Pike, K.; Jones, D.R.; Brocklehurst, P.; Marlow, N.; Salt, A.; Taylor, D.J. Childhood outcomes after prescription of antibiotics to pregnant women with preterm rupture of the membranes: 7-year follow-up of the ORACLE I trial. Lancet 2008, 372, 1310–1318. [Google Scholar] [CrossRef] [Green Version]
- Muanda, F.T.; Sheehy, O.; Bérard, A. Use of antibiotics during pregnancy and risk of spontaneous abortion. CMAJ 2017, 189, E625–E633. [Google Scholar] [CrossRef] [Green Version]
- Muanda, F.T.; Sheehy, O.; Bérard, A. Use of antibiotics during pregnancy and the risk of major congenital malformations: A population based cohort study. Br. J. Clin. Pharmacol. 2017, 83, 2557–2571. [Google Scholar] [CrossRef] [Green Version]
- Reis, A.S.; Barboza, R.; Murillo, O.; Barateiro, A.; Peixoto, E.P.M.; Lima, F.A.; Gomes, V.M.; Dombrowski, J.G.; Leal, V.N.C.; Araujo, F.; et al. Inflammasome activation and IL-1 signaling during placental malaria induce poor pregnancy outcomes. Sci. Adv. 2020, 6, eaax6346. [Google Scholar] [CrossRef] [Green Version]
- Equils, O.; Kellogg, C.; McGregor, J.; Gravett, M.; Neal-Perry, G.; Gabay, C. The role of the IL-1 system in pregnancy and the use of IL-1 system markers to identify women at risk for pregnancy complications. Biol. Reprod. 2020, 103, 684–694. [Google Scholar] [CrossRef]
- Southcombe, J.H.; Redman, C.W.; Sargent, I.L.; Granne, I. Interleukin-1 family cytokines and their regulatory proteins in normal pregnancy and pre-eclampsia. Clin. Exp. Immunol. 2015, 181, 480–490. [Google Scholar] [CrossRef] [Green Version]
- Licini, C.; Tossetta, G.; Avellini, C.; Ciarmela, P.; Lorenzi, T.; Toti, P.; Gesuita, R.; Voltolini, C.; Petraglia, F.; Castellucci, M.; et al. Analysis of cell-cell junctions in human amnion and chorionic plate affected by chorioamnionitis. Histol. Histopathol. 2016, 31, 759–767. [Google Scholar]
- Tossetta, G.; Paolinelli, F.; Avellini, C.; Salvolini, E.; Ciarmela, P.; Lorenzi, T.; Emanuelli, M.; Toti, P.; Giuliante, R.; Gesuita, R.; et al. IL-1β and TGF-β weaken the placental barrier through destruction of tight junctions: An in vivo and in vitro study. Placenta 2014, 35, 509–516. [Google Scholar] [CrossRef]
- Girard, S.; Heazell, A.E.; Derricott, H.; Allan, S.M.; Sibley, C.P.; Abrahams, V.M.; Jones, R.L. Circulating cytokines and alarmins associated with placental inflammation in high-risk pregnancies. Am. J. Reprod. Immunol. 2014, 72, 422–434. [Google Scholar] [CrossRef] [Green Version]
- Girard, S.; Sébire, H.; Brochu, M.E.; Briota, S.; Sarret, P.; Sébire, G. Postnatal administration of IL-1Ra exerts neuroprotective effects following perinatal inflammation and/or hypoxic-ischemic injuries. Brain Behav. Immun. 2012, 26, 1331–1339. [Google Scholar] [CrossRef] [Green Version]
- Girard, S.; Tremblay, L.; Lepage, M.; Sebire, G. IL-1 receptor antagonist protects against placental and neurodevelopmental defects induced by maternal inflammation. J. Immunol. 2010, 184, 3997–4005. [Google Scholar] [CrossRef]
- Leitner, K.; Al Shammary, M.; McLane, M.; Johnston, M.V.; Elovitz, M.A.; Burd, I. IL-1 receptor blockade prevents fetal cortical brain injury but not preterm birth in a mouse model of inflammation-induced preterm birth and perinatal brain injury. Am. J. Reprod. Immunol. 2014, 71, 418–426. [Google Scholar] [CrossRef] [Green Version]
- Nadeau-Vallee, M.; Chin, P.Y.; Belarbi, L.; Brien, M.E.; Pundir, S.; Berryer, M.H.; Beaudry-Richard, A.; Madaan, A.; Sharkey, D.J.; Lupien-Meilleur, A.; et al. Antenatal Suppression of IL-1 Protects against Inflammation-Induced Fetal Injury and Improves Neonatal and Developmental Outcomes in Mice. J. Immunol. 2017, 198, 2047–2062. [Google Scholar] [CrossRef]
- Nadeau-Vallee, M.; Quiniou, C.; Palacios, J.; Hou, X.; Erfani, A.; Madaan, A.; Sanchez, M.; Leimert, K.; Boudreault, A.; Duhamel, F.; et al. Novel Noncompetitive IL-1 Receptor-Biased Ligand Prevents Infection- and Inflammation-Induced Preterm Birth. J. Immunol. 2015, 195, 3402–3415. [Google Scholar] [CrossRef] [Green Version]
- McDuffie, R.S., Jr.; Davies, J.K.; Leslie, K.K.; Lee, S.; Sherman, M.P.; Gibbs, R.S. A randomized controlled trial of interleukin-1 receptor antagonist in a rabbit model of ascending infection in pregnancy. Infect. Dis. Obstet. Gynecol. 2001, 9, 233–237. [Google Scholar] [CrossRef] [Green Version]
- Presicce, P.; Park, C.W.; Senthamaraikannan, P.; Bhattacharyya, S.; Jackson, C.; Kong, F.; Rueda, C.M.; DeFranco, E.; Miller, L.A.; Hildeman, D.A.; et al. IL-1 signaling mediates intrauterine inflammation and chorio-decidua neutrophil recruitment and activation. JCI Insight 2018, 3, e98306. [Google Scholar] [CrossRef]
- Karisnan, K.; Bakker, A.J.; Song, Y.; Noble, P.B.; Pillow, J.J.; Pinniger, G.J. Interleukin-1 receptor antagonist protects against lipopolysaccharide induced diaphragm weakness in preterm lambs. PLoS ONE 2015, 10, e0124390. [Google Scholar]
- Nadeau-Vallee, M.; Obari, D.; Quiniou, C.; Lubell, W.D.; Olson, D.M.; Girard, S.; Chemtob, S. A critical role of interleukin-1 in preterm labor. Cytokine Growth Factor Rev. 2016, 28, 37–51. [Google Scholar] [CrossRef]
- Prieto-Peña, D.; Dasgupta, B. Biologic agents and small-molecule inhibitors in systemic autoimmune conditions: An update. Pol. Arch. Intern. Med. 2020, 131, 171–181. [Google Scholar] [CrossRef]
- Soh, M.C.; Moretto, M. The use of biologics for autoimmune rheumatic diseases in fertility and pregnancy. Obstet. Med. 2020, 13, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Götestam Skorpen, C.; Hoeltzenbein, M.; Tincani, A.; Fischer-Betz, R.; Elefant, E.; Chambers, C.; da Silva, J.; Nelson-Piercy, C.; Cetin, I.; Costedoat-Chalumeau, N.; et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann. Rheum. Dis. 2016, 75, 795–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuki, G.; Bresnihan, B.; Bear, M.B.; McCabe, D. Long-term safety and maintenance of clinical improvement following treatment with anakinra (recombinant human interleukin-1 receptor antagonist) in patients with rheumatoid arthritis: Extension phase of a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2002, 46, 2838–2846. [Google Scholar] [CrossRef] [PubMed]
- Buckley, L.F.; Viscusi, M.M.; Van Tassell, B.W.; Abbate, A. Interleukin-1 blockade for the treatment of pericarditis. Eur. Heart J. Cardiovasc. Pharmacother. 2018, 4, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Kary, S.; Burmester, G.R. Anakinra: The first interleukin-1 inhibitor in the treatment of rheumatoid arthritis. Int. J. Clin. Pract. 2003, 57, 231–234. [Google Scholar]
- Ramírez, J.; Cañete, J.D. Anakinra for the treatment of rheumatoid arthritis: A safety evaluation. Expert Opin. Drug Saf. 2018, 17, 727–732. [Google Scholar] [CrossRef]
- Dinarello, C.A.; van der Meer, J.W. Treating inflammation by blocking interleukin-1 in humans. Semin. Immunol. 2013, 25, 469–484. [Google Scholar] [CrossRef] [Green Version]
- Vastert, S.J.; Jamilloux, Y.; Quartier, P.; Ohlman, S.; Osterling Koskinen, L.; Kullenberg, T.; Franck-Larsson, K.; Fautrel, B.; de Benedetti, F. Anakinra in children and adults with Still’s disease. Rheumatology 2019, 58, vi9–vi22. [Google Scholar] [CrossRef]
- Church, L.D.; McDermott, M.F. Canakinumab, a fully-human mAb against IL-1beta for the potential treatment of inflammatory disorders. Curr. Opin. Mol. Ther. 2009, 11, 81–89. [Google Scholar]
- Savic, S.; McDermott, M.F. Inflammation: Canakinumab for the cryopyrin-associated periodic syndromes. Nat. Rev. Rheumatol. 2009, 5, 529–530. [Google Scholar] [CrossRef]
- Ortona, E.; Pierdominici, M.; Maselli, A.; Veroni, C.; Aloisi, F.; Shoenfeld, Y. Sex-based differences in autoimmune diseases. Ann. Ist. Super. Sanita 2016, 52, 205–212. [Google Scholar]
- Fischer-Betz, R.; Specker, C. Pregnancy in systemic lupus erythematosus and antiphospholipid syndrome. Best Pract. Res. Clin. Rheumatol. 2017, 31, 397–414. [Google Scholar] [CrossRef]
- Ugurlu, S.; Ergezen, B.; Egeli, B.H.; Selvi, O.; Ozdogan, H. Anakinra treatment in patients with familial Mediterranean fever: A single-centre experience. Rheumatology 2021, 60, 2327–2332. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Sfriso, P.; Bindoli, S.; Doria, A.; Feist, E.; Galozzi, P. Canakinumab for the treatment of adult-onset Still’s disease. Expert Rev. Clin. Immunol. 2020, 16, 129–138. [Google Scholar] [CrossRef]
- Egawa, M.; Imai, K.; Mori, M.; Miyasaka, N.; Kubota, T. Placental Transfer of Canakinumab in a Patient with Muckle-Wells Syndrome. J. Clin. Immunol. 2017, 37, 339–341. [Google Scholar] [CrossRef]
- Mijatovic, V.; Hompes, P.G.; Wouters, M.G. Familial Mediterranean fever and its implications for fertility and pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 108, 171–176. [Google Scholar] [CrossRef]
- Yasar, O.; Iskender, C.; Kaymak, O.; Taflan Yaman, S.; Uygur, D.; Danisman, N. Retrospective evaluation of pregnancy outcomes in women with familial Mediterranean fever. J. Matern. Fetal Neonatal Med. 2014, 27, 733–736. [Google Scholar] [CrossRef]
- Chang, Z.; Spong, C.Y.; Jesus, A.A.; Davis, M.A.; Plass, N.; Stone, D.L.; Chapelle, D.; Hoffmann, P.; Kastner, D.L.; Barron, K.; et al. Anakinra use during pregnancy in patients with cryopyrin-associated periodic syndromes (CAPS). Arthritis Rheum. 2014, 66, 3227–3232. [Google Scholar] [CrossRef] [Green Version]
- De Lorenzo, R.; Ramirez, G.A.; Punzo, D.; Lorioli, L.; Rovelli, R.; Canti, V.; Barera, G.; Rovere-Querini, P. Neonatal outcomes of children born to mothers on biological agents during pregnancy: State of the art and perspectives. Pharmacol. Res. 2020, 152, 104583. [Google Scholar] [CrossRef]
- Ben-Chetrit, E.; Ben-Chetrit, A.; Berkun, Y.; Ben-Chetrit, E. Pregnancy outcomes in women with familial Mediterranean fever receiving colchicine: Is amniocentesis justified? Arthritis Care Res. 2010, 62, 143–148. [Google Scholar] [CrossRef]
- Mok, M.Y.; Lo, Y.; Leung, P.Y.; Lau, C.S. Pregnancy outcome in patients with adult onset Still’s disease. J. Rheumatol. 2004, 31, 2307–2309. [Google Scholar]
- García-Fernández, A.; Gerardi, M.C.; Crisafulli, F.; Filippini, M.; Fredi, M.; Gorla, R.; Lazzaroni, M.G.; Lojacono, A.; Nalli, C.; Ramazzotto, F.; et al. Disease course and obstetric outcomes of pregnancies in juvenile idiopathic arthritis: Are there any differences among disease subtypes? A single-centre retrospective study of prospectively followed pregnancies in a dedicated pregnancy clinic. Clin. Rheum. 2021, 40, 239–244. [Google Scholar] [CrossRef]
- Bakalianou, K.; Salakos, N.; Iavazzo, C.; Danilidou, K.; Papadias, K.; Kondi-Pafiti, A. A rare case of uneventful pregnancy in a woman with Cogan’s syndrome. Clin. Exp. Obstet. Gynecol. 2008, 35, 301–302. [Google Scholar]
- Currie, C.; Wax, J.R.; Pinette, M.G.; Blackstone, J.; Cartin, A. Cogan’s syndrome complicating pregnancy. J. Matern. Fetal Neonatal Med. 2009, 22, 928–930. [Google Scholar] [CrossRef]
- Deliveliotou, A.; Moustakarias, T.; Argeitis, J.; Vaggos, G.; Vitoratos, N.; Hassiakos, D. Successful full-term pregnancy in a woman with Cogan’s syndrome: A case report. Clin. Rheum. 2007, 26, 2181–2183. [Google Scholar] [CrossRef]
- Riboni, F.; Cosma, S.; Perini, P.G.; Benedetto, C. Successful Pregnancy in a Patient with Atypical Cogan’s Syndrome. Isr. Med. Assoc. J. 2016, 18, 495–496. [Google Scholar]
- Tarney, C.M.; Wilson, K.; Sewell, M.F. Cogan syndrome in pregnancy. Obstet. Gynecol. 2014, 124, 428–431. [Google Scholar] [CrossRef]
- Venhoff, N.; Thiel, J.; Schramm, M.A.; Jandova, I.; Voll, R.E.; Glaser, C. Case Report: Effective and Safe Treatment with Certolizumab Pegol in Pregnant Patients With Cogan’s Syndrome: A Report of Three Pregnancies in Two Patients. Front. Immunol. 2020, 11, 616992. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Chou, D.; Oestergaard, M.; Say, L.; Moller, A.B.; Kinney, M.; Lawn, J. Born too soon: The global epidemiology of 15 million preterm births. Reprod. Health 2013, 10 (Suppl. 1), S2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venhoff, N.; Voll, R.E.; Glaser, C.; Thiel, J. IL-1-blockade with Anakinra during pregnancy: Retrospective analysis of efficacy and safety in female patients with familial Mediterranean fever. Z. Rheum. 2018, 77, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- Smith, C.J.F.; Chambers, C.D. Five successful pregnancies with antenatal anakinra exposure. Rheumatology 2018, 57, 1271–1275. [Google Scholar] [CrossRef] [Green Version]
- Youngstein, T.; Hoffmann, P.; Gül, A.; Lane, T.; Williams, R.; Rowczenio, D.M.; Ozdogan, H.; Ugurlu, S.; Ryan, J.; Harty, L.; et al. International multi-centre study of pregnancy outcomes with interleukin-1 inhibitors. Rheumatology 2017, 56, 2102–2108. [Google Scholar] [CrossRef] [Green Version]
- Rider, R.A.; Stevenson, D.A.; Rinsky, J.E.; Feldkamp, M.L. Association of twinning and maternal age with major structural birth defects in Utah, 1999 to 2008. Birth Defects Res. A Clin. Mol. Teratol. 2013, 97, 554–563. [Google Scholar] [CrossRef]
- Viktil, K.K.; Engeland, A.; Furu, K. Use of antirheumatic drugs in mothers and fathers before and during pregnancy-a population-based cohort study. Pharmacoepidemiol. Drug Saf. 2009, 18, 737–742. [Google Scholar] [CrossRef]
- Drechsel, P.; Stüdemann, K.; Niewerth, M.; Horneff, G.; Fischer-Betz, R.; Seipelt, E.; Spähtling-Mestekemper, S.; Aries, P.; Zink, A.; Klotsche, J.; et al. Pregnancy outcomes in DMARD-exposed patients with juvenile idiopathic arthritis-results from a JIA biologic registry. Rheumatology 2020, 59, 603–612. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Study Design | Year of Publication | Population | Number of Pregnancies Included in This Study | Indication for Treatment | Treatment; Doses | Outcome | Notes |
|---|---|---|---|---|---|---|---|---|
| 1 | Case report | 2009 | 1 | 1 | AOSD | Anakinra; 100 mg/day | Healthy term baby | |
| 2 | Case report | 2011 | 2 | 2 | AOSD | Anakinra; 100 mg/day | Two healthy babies, one PTB 36 weeks | |
| 3 | Retrospective cohort study | 2013 | 51 | 1 | SOJIA | Anakinra; NA | Term baby | Big cohort of SOJIA patients but only one pregnant |
| 4 | Prospective cohort study | 2014 | 9 | 9 | FCAS (6) NOMID (1) MWS/NOMID (1) | Anakinra; mostly 100 mg/day but also 239–300 mg/day | All term babies, three with FCAS, one with MWS and one twin pregnancy resulted in one death at 30 weeks | |
| 5 | Prospective cohort study | 2015 | 4 | 0 | FMF | Anakinra; 100 mg/day | All healthy babies, one PTB 36 weeks | Data in another study already included |
| 6 | Prospective cohort study | 2015 | 6 | 3 | FMF | Anakinra; 100 mg/day or NA | All healthy babies, one PTB 36 weeks | Data in another study already included |
| 7 | Prospective cohort study | 2015 | 79 | 1 | Chronic inflammatory rheumatic disease | Anakinra; NA | Voluntary pregnancy termination | Big cohort of biological drug during pregnancy, only one took anakinra |
| 8 | Case report | 2017 | 1 | 1 | FMF | Anakinra; 100 mg/day | Healthy term baby | |
| 9 | Prospective cohort study | 2018 | 5 | 5 | AOSD (3) SOJIA (2) | Anakinra; 100 mg/day | All healthy term babies but one with right hydrocele, heart murmur and resolved low birthweight | |
| 10 | Retrospective cohort study | 2018 | 4 | 4 | FMF | Anakinra; 100 mg/day–2 days | All healthy babies but one PTB at 33 weeks with hypotrophic, respiratory distress syndrome, hyperbilirubinemia and poor drinking | |
| 11 | Prospective cohort study | 2019 | 13 | 12 | FMF | Anakinra; 100 mg/day or NA | One miscarriage, two PTB, one stillbirth but overall healthy babies | Two pregnancies still ongoing, no obstetrical information and two pregnancies with data in another study already included |
| 12 | Case report | 2019 | 1 | 1 | FMF | Anakinra; 100 mg/day | Term healthy baby | Cohort of four patients with FMF, only one pregnant |
| 13 | Prospective cohort study | 2019 | 54 | 1 | FMF | Anakinra; 100 mg/day | Obstetrical and neonatal information NA | Cohort of patient with FMF, only one pregnant |
| 14 | Case report | 2019 | 1 | 1 | HLH | Anakinra; 200 mg/twice daily | Healthy but had anaemia and marrow suppression | |
| 15 | Retrospective cohort study | 2020 | 16 | 3 | AOSD | Anakinra; NA | All healthy babies but one had PTB at 28 weeks | Cohort of child exposed to DMARDs, only 3 exposed to anakinra during pregnancy |
| 16 | Case report | 2020 | 1 | 1 | HLH | Anakinra; NA | PTB at 31 weeks and IUGR but overall healthy | |
| 17 | Case report | 2017 | 1 | 1 | MWS | Canakinumab; 150 mg/ 4–8 weeks | Healthy term baby | |
| 18 | Case report | 2018 | 1 | 1 | SOJIA | Canakinumab; NA | Healthy term baby | |
| 19 | Retrospective cohort study | 2020 | 23 | 1 | FMF | Canakinumab; 150 mg/ 6–8 weeks | One healthy term pregnancy and one without information | Cohort of patient with FMF, only 2 pregnant |
| 20 | Retrospective cohort study | 2013 | 7 | 7 | AOSD (1) CAPS (3) TRAPS (1) FMF (1) Idiopathic pericarditis (1) | Anakinra; NA (6), Canakinumab; NA (1) | All healthy babies, one PTB 36 weeks and one with unilateral reduced hearing at 6 weeks | Two pregnancies still ongoing, no obstetrical information |
| 21 | Case report | 2015 | 1 | 1 | MWS | Canakinumab; NA and Anakinra; NA | Healthy but with CAPS | |
| 22 | Retrospective cohort study | 2017 | 43 | 31 | AOSD (4) CAPS (16) Cogan syndrome (2) FMF (5) Idiopathic pericarditis (1) TRAPS (2) Un-SAID (1) | Anakinra; mostly 100 mg/day but also 50–300 mg/day Canakinumab; 150 mg/ 4–8 weeks | Two miscarriage (same women), two PTB, all healthy babies but one with left renal agenesis and ectopic neurohypophysis with hormone deficiency | 43 pregnancies exposed to IL-1 inhibitor but 11 were male exposure |
| Pregnancy ID | Pregnancy from Study | Indication for Treatment | Treatment | Doses | Exposure Time | Mode of Delivery | GA at Delivery (Weeks) | Birth Weight (g) | Obstetric Complication | Child Sex | Child Wellbeing | Breasfeeding |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 14 | HLH | Anakinra | 200 mg/ twice daily | 22 w–B | C- section | NA | NA | None | NA | Anaemia and bone marrow suppression | NA |
| 2 | 19 | FMF + amyloidosis | Canakinumab | 150 mg/6 weeks | PC–8 w | NA | Term | NA | None | NA | Healthy | NA |
| 3 | 19 | FMF | Canakinumab | 150 mg/8 weeks | PC–PPT | NA | NA | NA | NA | NA | NA | NA |
| 4 * | 7 | Chronic inflammatory rheumatic disease | Anakinra | NA | NA | Vaginal | NA | NA | Voluntary abortion | NA | NA | NA |
| 5 | 1 | AOSD | Anakinra | 100 mg/ day | PC–B | Vaginal | 40.7 | 2700 | Placental retention requiring manual abruption | F | Healthy | Yes |
| 6 | 4 | FCAS | Anakinra | 100 mg/ day | PC–B | Vaginal | 41.0 | 3742 | None | NA | Healthy | No |
| 7 | 4 | FCAS | Anakinra | 100 mg/ day | PC–B | Vaginal | 41.0 | 3629 | None | NA | FCAS | No |
| 8 | 4 | FCAS | Anakinra | 100 mg/ day | PC–B | Vaginal | 38.0 | 3402 | None | NA | FCAS | Yes |
| 9 | 4 | FCAS | Anakinra | 100 mg/ day | PC–B | Vaginal | 37.0 | 3459 | None | NA | Healthy | No |
| 10 | 4 | FCAS | Anakinra | 100 mg/ day | PC–B | Vaginal | 37.7 | 2977 | None | NA | FCAS | No |
| 11 | 4 | FCAS | Anakinra | 100 mg/ day | PC–B | Vaginal | 39.0 | 3345 | None | NA | Healthy | No |
| 12 | 4 | NOMID | Anakinra | 300 mg/ day | PC–B | C- section | 40.0 | 4139 | Chronic hypertension | NA | Healthy | Yes |
| 13 | 4 | NOMID | Anakinra | 239–300 mg/ day | PC–B | Vaginal | A: 38.7 B: 30.0 | A: 2637 B: NA | A: None B: PTB | NA | A: Healthy B: Renal agenesis (death) | A: Yes B: No |
| 14 | 4 | MWS/NOMID | Anakinra | 100 mg/ day | PC–B | C- section | Term | 3515 | None | NA | MWS | No |
| 15 | 15 | AOSD | Anakinra | NA | PC–B | C- section | 28.0 | 1175 | PTB | F | Healthy | NA |
| 16 | 15 | AOSD | Anakinra | NA | PC–B | Vaginal | 40.0 | 3480 | None | M | Healthy | NA |
| 17 | 15 | AOSD | Anakinra | NA | PC–B | Vaginal | 38.0 | 3450 | None | M | Healthy | NA |
| 19 | 12 | FMF | Anakinra | 100 mg/ day | 6 w–B | C- section | Term | 3340 | None | F | Healthy | Yes |
| 20 | 17 | MWS | Canakinumab | 150 mg/ 8 weeks, then every 4–5 weeks | PC–34 w | C- section | 39.0 | 2994 | None | F | Healthy with NLRP3 mutation | NA |
| 22 | 11 | FMF | Anakinra | 100 mg/ day | PC–29 w + 33 w–B | C- section | 38.0 | NA | Incision site infection in postpartum | M | Healthy | NA |
| 24 | 11 | FMF | Anakinra | NA | 16 w–B | C- section | 31.0 | NA | PTB | F-F twins | Healthy | NA |
| 25 | 11 | FMF | Anakinra | NA | 23 w–B | C- section | 37.0 | NA | NA | F | Healthy | NA |
| 26 | 11 | FMF | Anakinra | NA | 32 w–B | C- section | 40.0 | NA | NA | F | Healthy | NA |
| 27 | 11 | FMF | Anakinra | NA | PC–B with 1 month interruption | C- section | 38.0 | NA | NA | F | Healthy | NA |
| 28 | 11 | FMF | Anakinra | NA | 34 w–B | Vaginal | 37.0 | NA | Stillbirth | M | NA | |
| 29 | 11 | FMF | Anakinra | NA | 6 w–B | C- section | 36.0 | NA | PTB | F | Healthy | NA |
| 30 | 11 | FMF | Anakinra | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| 31 * | 11 | FMF | Anakinra | NA | 5 w–8 w (ongoing) | NA | NA | NA | NA | NA | NA | NA |
| 32 * | 11 | FMF | Anakinra | NA | PC–8 w (ongoing) | NA | NA | NA | NA | NA | NA | NA |
| 33 | 2 | AOSD | Anakinra | 100 mg/ day | PC–B | Vaginal | 39.0 | 3100 | None | M | Healthy | No |
| 34 | 2 | AOSD | Anakinra | NA | 12 w–B | C- section | 36.0 | 2800 | PTB | M | Healthy | No |
| 35 | 18 | sJIA | Canakinumab | NA | PC–35 w | Vaginal | 39.0 | NA | Forceps + minor episiotomy wound infection | M | Healthy | NA |
| 36 | 21 | MWS | Canakinumab and Ana kinra | NA | PC–B | NA | NA | NA | NA | M | Healthy with CAPS | Yes |
| 37 | 8 | FMF | Anakinra | 100 mg/ day | PC–B | C- section | 38.0 | 2700 | None | NA | Healthy | Yes |
| 38 * | 20 | CAPS | Anakinra | NA | PC–NA (ongoing) | NA | NA | NA | NA | NA | NA | NA |
| 39 * | 20 | CAPS | Canakinumab | NA | PC–8 w (ongoing) | NA | NA | NA | NA | NA | NA | NA |
| 40 | 20 | CAPS | Anakinra | NA | PC–B | Vaginal | NA | NA | None | M | Healthy | No |
| 41 | 20 | TRAPS | Anakinra | NA | PC–B | Vaginal | NA | NA | None | M | Unilateral reduced hearing at 6 weeks | No |
| 42 | 20 | FMF | Anakinra | 100 mg/ day | 21 w–B | C- section | 36.0 | NA | Vaginal bleeding, PTB | M | Healthy | Yes |
| 43 | 20 | idiopathic pericarditis | Anakinra | NA | PC–B | Vaginal | NA | NA | None | M | Healthy | No |
| 44 | 20 | AOSD | Anakinra | NA | 22 w–33 w | Vaginal | NA | NA | None | M | Healthy | No |
| 50 | 6 | FMF | Anakinra | 100 mg/ day | 12 w–B | Vaginal | 40.0 | NA | None | F | Healthy | Yes |
| 52 | 6 | FMF | Anakinra | NA | 15 w–B | Vaginal | 38.0 | NA | None | M | Low thrombocyte count treated by IVIG | NA |
| 54 | 3 | sJIA | Anakinra | NA | P–B | NA | Term | NA | NA | NA | NA | NA |
| 55 | 13 | FMF | Anakinra | 100 mg/ day | P–B | NA | NA | NA | None | NA | NA | NA |
| 56 | 9 | sJIA | Anakinra | 100 mg/ day | PC–20.4 w | C- section | 37.1 | 2419 | Hypertension, oligohydramnios, breech presentation | M | Jaundice, right hydrocele and heart murmur | No |
| 57 | 9 | AOSD | Anakinra | 100 mg/ day | 20 w–38.1 w | Vaginal | 40.1 | 2940 | None | M | Jaundice | NA |
| 58 | 9 | AOSD | Anakinra | 100 mg/ day | PC– 16.6 w + 19.4 w– 37.3 w | C- section | 39.4 | 3632 | None | M | Jaundice | Yes |
| 59 | 9 | AOSD | Anakinra | 100 mg/ day | PC– 2 w + 9.6 w– 36.7 w | Vaginal | 38.7 | 3519 | None | M | Tongue-tied | Yes |
| 60 | 9 | sJIA | Anakinra | 100 mg/ day | PC– 37.3 w | Vaginal | 39.4 | 2640 | Oligohydramnios | F | Healthy | No |
| 61 | 10 | FMF | Anakinra | 100 mg/ day | P–B | C- section | 40.6 | 4025 | None | NA | Healthy | Yes |
| 62 | 10 | FMF | Anakinra | 100 mg/ day | 2e trimester–B | C- section | 33.7 | 3320 | PTB | NA | Healthy, hypotrophic, respiratory distress syndrome, hyperbilirubinemia and poor drinking | No |
| 63 | 10 | FMF | Anakinra | 100 mg/2 days | P–B | C- section | 39.3 | 4030 | Premature bleeding | NA | Healthy | NA |
| 64 | 10 | FMF | Anakinra | 100 mg/2 days | P–B | C- section | 36.4 | 3320 | PTB | NA | Healthy | NA |
| 66 | 16 | HLH | Anakinra | NA | 22 w–B | C- section | 31.7 | NA | PTB, IUGR, abnormal umbilical artery Doppler and subsequent cardiotocography was abnormal | M | Neonatal unit briefly but healthy | NA |
| 67 | 22 | CAPS | Canakinumab | 150 mg/ 8 weeks | PC–8 w | C- section | 38.0 | 3540 | Gestationnal diabetes | M | Healthy | No |
| 68 | 22 | CAPS | Canakinumab | 150 mg/ 8 weeks | PC–12 w | Vaginal | 40.0 | 4480 | None | F | Healthy | Yes |
| 69 | 22 | CAPS | Canakinumab | 150 mg/ 8 weeks | 1 w–36 w | NA | 40.0 | 3570 | None | M | Healthy | NA |
| 70 | 22 | CAPS | Canakinumab | 120 mg (single dose) | P | NA | 38.0 | 3290 | None | M | Healthy | Yes |
| 71 | 22 | Un-SAID | Canakinumab | 300 mg/ 8 weeks | PC–B | Vaginal | 39.0 | NA | None | M | Healthy | NA |
| 72 | 22 | FMF | Canakinumab | 150 mg/ 4 weeks | PC–B | C- section | 37.0 | 3300 | None | M | Healthy | Yes |
| 73 | 22 | FMF | Canakinumab | 150 mg/ 8 weeks | PC–4 w | C- section | 40.0 | 3300 | None | F | Healthy | Yes |
| 74 * | 22 | Cogan syndrome | Canakinumab | 150 mg/ 4 weeks | PC–4 w | Vaginal | 4.0 | NA | Miscarriage | NA | NA | |
| 75 | 22 | CAPS | Anakinra | 50 mg/ day | PC–B | Vaginal | 39.0 | 3940 | None | M | Healthy | No |
| 76 | 22 | CAPS | Anakinra | 50 mg/ day | PC–B | Vaginal | 39.0 | NA | None | F | Healthy | No |
| 77 | 22 | CAPS | Anakinra | 100 mg/ day | PC–B | Vaginal | 41.1 | 3600 | None | M | Healthy | Yes |
| 78 | 22 | CAPS | Anakinra | 100 mg/ day | PPT–B | Vaginal | 40.0 | 4480 | None | F | Healthy | Yes |
| 79 | 22 | CAPS | Anakinra | 100 mg/ day | 36 w–B | NA | 40.0 | 3570 | None | M | Healthy | NA |
| 80 | 22 | CAPS | Anakinra | 100 mg/ day | 1 w–PPT | NA | 36.9 | 2830 | PTB | M | Healthy | No |
| 81 | 22 | CAPS | Anakinra | 100 mg/ day | PC–B | C- section | 38.9 | NA | C-section due to failure to progress | NA | Healthy | NA |
| 82 | 22 | CAPS | Anakinra | 100 mg/ day | PC–6 w | C- section | 40.0 | NA | None | M | Healthy | NA |
| 83 | 22 | CAPS | Anakinra | 100 mg/ day | PC–B | NA | NA | NA | None | M | Healthy | Yes |
| 84 | 22 | CAPS | Anakinra | 100 mg/ day | NA | NA | 40.1 | NA | None | F | Healthy | NA |
| 85 | 22 | CAPS | Anakinra | 100 mg/ day | NA | NA | NA | NA | None | F | Healthy | NA |
| 86 | 22 | CAPS | Anakinra | 100 mg/ day | NA | NA | NA | NA | None | F | Healthy | NA |
| 87 | 22 | FMF | Anakinra | 100 mg/ day | PC–B | C- section | 36.1 | 2170 | Vaginal bleeding, PTB | M | Healthy | Yes |
| 88 | 22 | FMF | Anakinra | 100 mg/ day | 12 w–B | Vaginal | 40.0 | 3170 | None | F | Healthy | Yes |
| 89 | 22 | FMF | Anakinra | 100 mg/ day | PC–B | Vaginal | 36.0 | 1600 | PTB | F | Healthy | Yes |
| 90 | 22 | idiopathic pericarditis | Anakinra | 100 mg/ day | PC–PPT | Vaginal | 38.3 | 2930 | None | M | Healthy | No |
| 91 | 22 | AOSD | Anakinra | 200–300 mg/ day | PC–16 w | NA | 37.0 | 2450 | None | F | Healthy | No |
| 92 | 22 | AOSD | Anakinra | 100 mg/ day | 22 w– 33 w | NA | 35.1 | 2020 | PTB | M | Healthy | Yes |
| 93 | 22 | AOSD | Anakinra | 100 mg/ day | 9 w–B | C- section | 38.1 | NA | None | M | Left renal agenesis | Yes |
| 94 | 22 | AOSD | Anakinra | 100 mg/ day | NA | Vaginal | 38.0 | 3060 | None | F | Healthy | Yes |
| 95 | 22 | TRAPS | Anakinra | 100 mg/ day | PC–B | Vaginal | 41.0 | 3230 | None | M | Healthy | Yes |
| 96 | 22 | TRAPS | Anakinra | 100 mg/ day | PC–B | NA | NA | NA | None | F | Healthy | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brien, M.-E.; Gaudreault, V.; Hughes, K.; Hayes, D.J.L.; Heazell, A.E.P.; Girard, S. A Systematic Review of the Safety of Blocking the IL-1 System in Human Pregnancy. J. Clin. Med. 2022, 11, 225. https://doi.org/10.3390/jcm11010225
Brien M-E, Gaudreault V, Hughes K, Hayes DJL, Heazell AEP, Girard S. A Systematic Review of the Safety of Blocking the IL-1 System in Human Pregnancy. Journal of Clinical Medicine. 2022; 11(1):225. https://doi.org/10.3390/jcm11010225
Chicago/Turabian StyleBrien, Marie-Eve, Virginie Gaudreault, Katia Hughes, Dexter J. L. Hayes, Alexander E. P. Heazell, and Sylvie Girard. 2022. "A Systematic Review of the Safety of Blocking the IL-1 System in Human Pregnancy" Journal of Clinical Medicine 11, no. 1: 225. https://doi.org/10.3390/jcm11010225