
Immediate Post-Procedural and Discharge Assessment of Mitral Valve Function Following Transcatheter Edge-to-Edge Mitral Valve Repair: Correlation and Association with Outcomes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. TEEMr Procedure
2.3. Echocardiography Assessment
2.4. Follow-Up and Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient’s Characteristics
3.2. Procedural Course
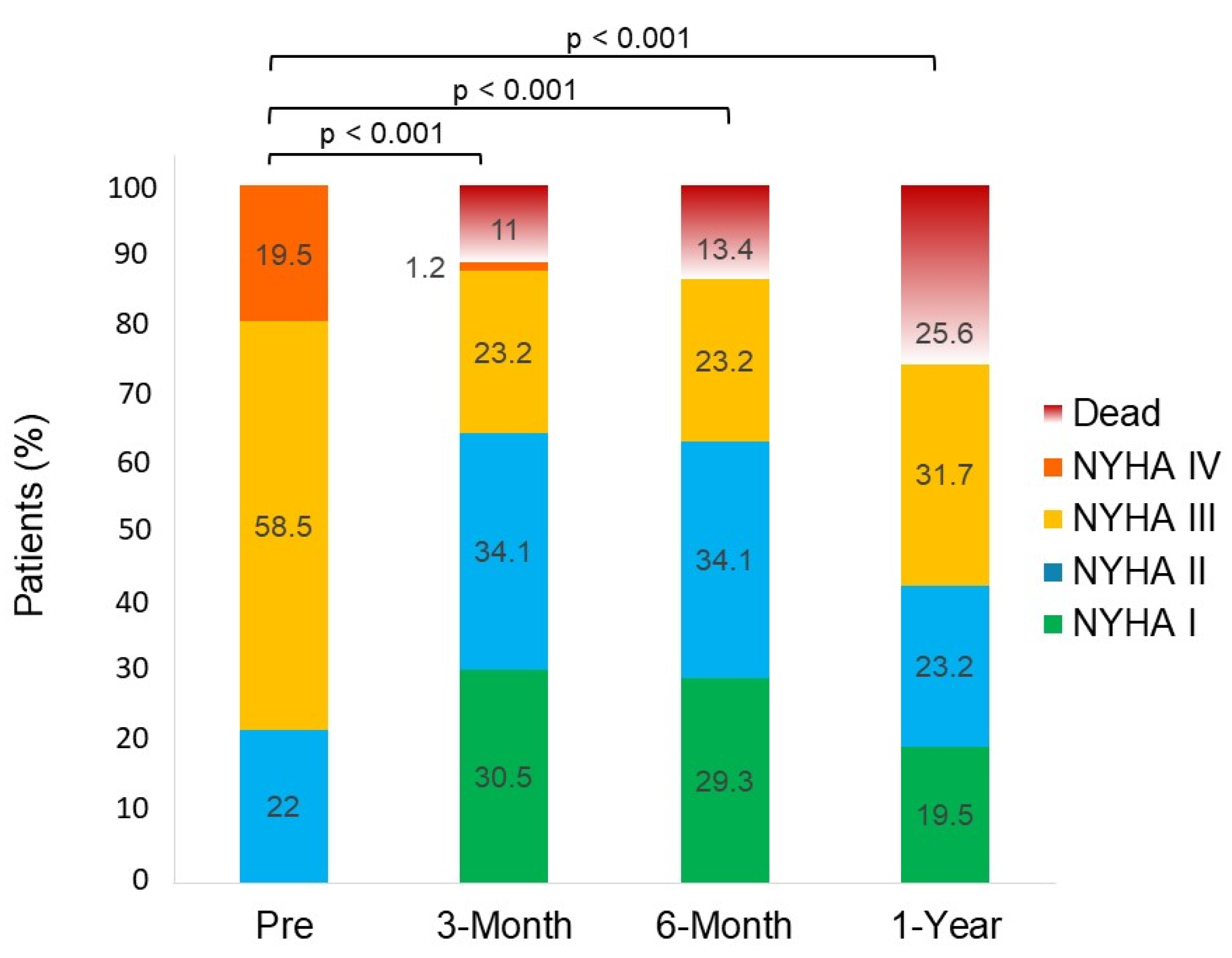
3.3. Clinical Outcomes
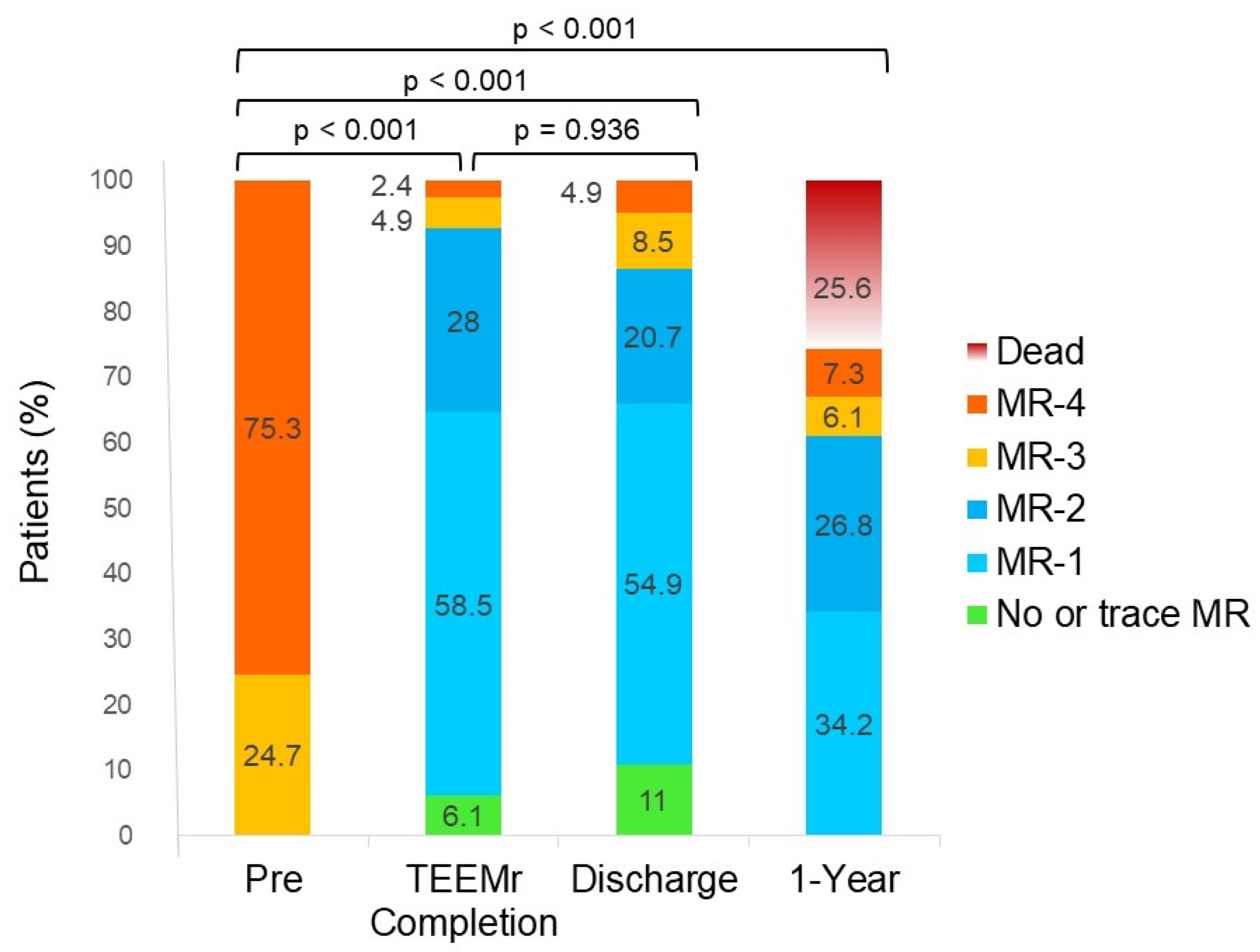
3.4. MR and rMR Assessments
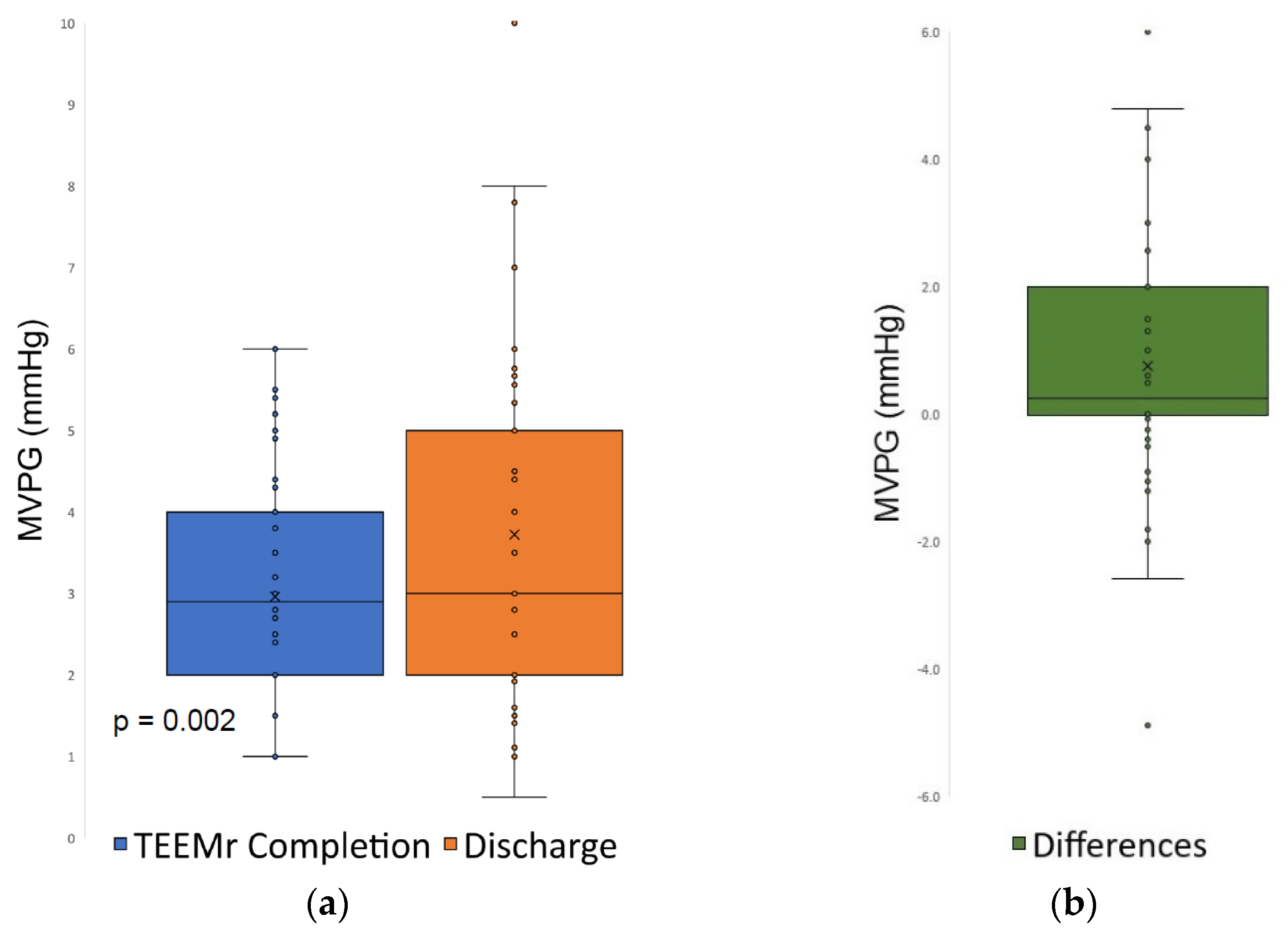
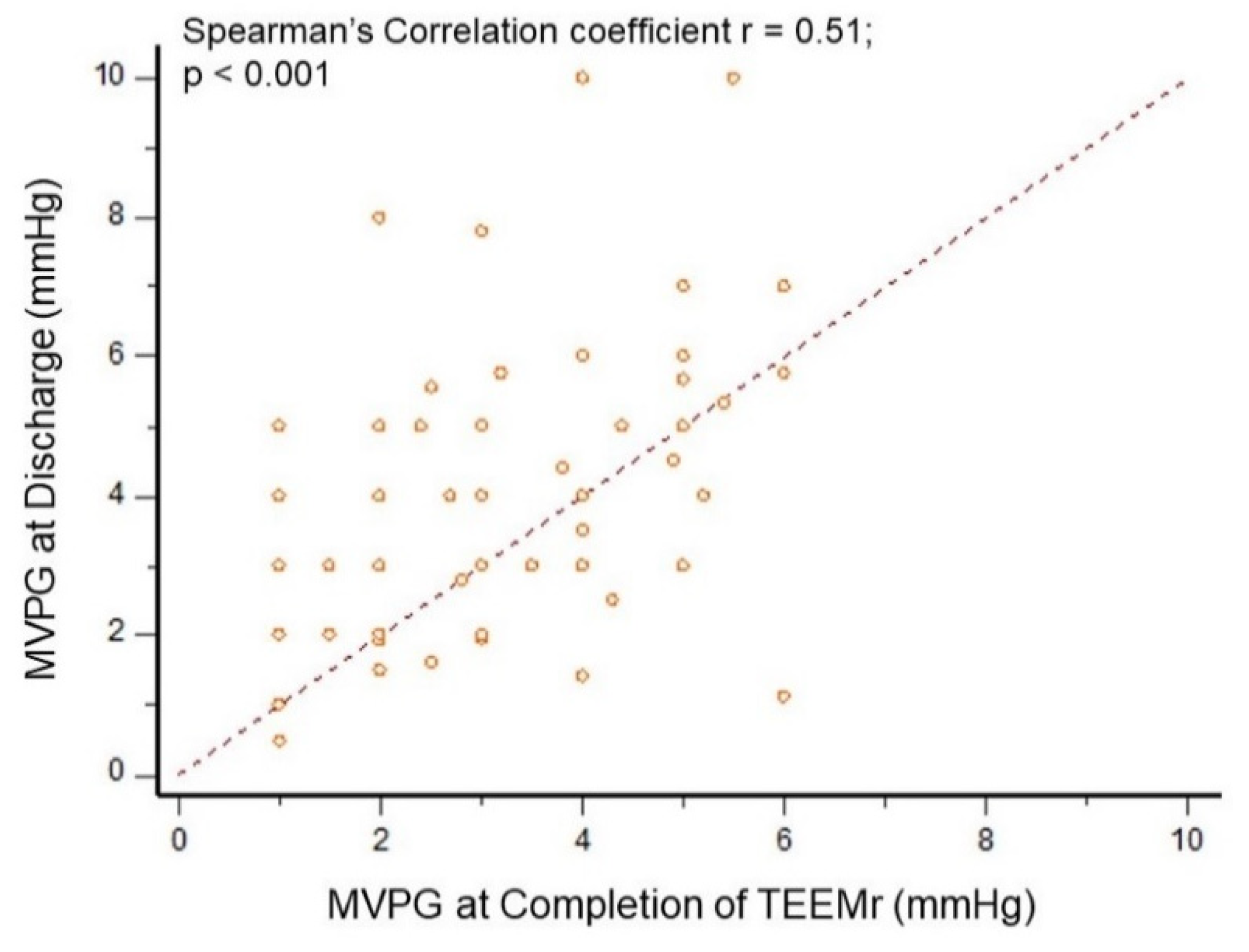
3.5. MVPG Assessments
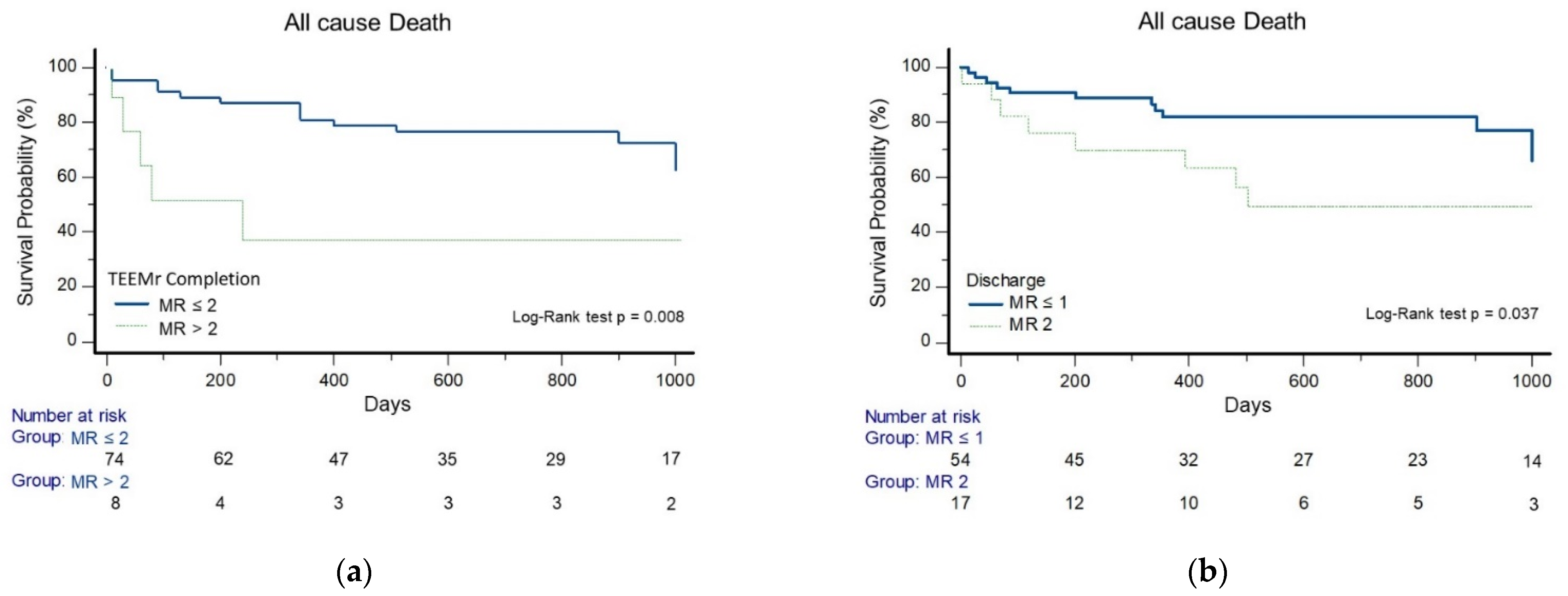
3.6. Event Free Survival Analysis and Predictors of Outcomes
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feldman, T.; Foster, E.; Glower, D.D.; Kar, S.; Rinaldi, M.J.; Fail, P.S.; Smalling, R.W.; Siegel, R.; Rose, G.A.; Engeron, E.; et al. Percutaneous Repair or Surgery for Mitral Regurgitation. N. Engl. J. Med. 2011, 364, 1395–1406. [Google Scholar] [CrossRef] [Green Version]
- Sorajja, P.; Vemulapalli, S.; Feldman, T.; Mack, M.; Holmes, D.R.; Stebbins, A.; Kar, S.; Thourani, V.; Ailawadi, G. Outcomes ith Transcatheter Mitral Valve Repair in the United States: An STS/ACC TVT Registry Report. J. Am. Coll. Cardiol. 2017, 70, 2315–2327. [Google Scholar] [CrossRef] [PubMed]
- Toggweiler, S.; Zuber, M.; Sürder, D.; Biaggi, P.; Gstrein, C.; Moccetti, T.; Pasotti, E.; Gaemperli, O.; Faletra, F.; Petrova-Slater, I.; et al. Two-year outcomes after percutaneous mitral valve repair with the MitraClip system: Durability of the procedure and predictors of outcome. Open Heart 2014, 1, e000056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, H.; Neuss, M.; Weissenborn, J.; Butter, C. Impact of residual mitral regurgitation after MitraClip implantation. Int. J. Cardiol. 2017, 227, 813–819. [Google Scholar] [CrossRef]
- Paranskaya, L.; D’Ancona, G.; Bozdag-Turan, I.; Akin, I.; Kische, S.; Turan, G.R.; Rehders, T.; Ortak, J.; Nienaber, C.A.; Ince, H. Residual mitral valve regurgitation after percutaneous mitral valve repair with the MitraClip® system is a risk factor for adverse one-year outcome. Catheter. Cardiovasc. Interv. 2013, 81, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Reichart, D.; Kalbacher, D.; Rübsamen, N.; Tigges, E.; Thomas, C.; Schirmer, J.; Reichenspurner, H.; Blankenberg, S.; Conradi, L.; Schäfer, U.; et al. The impact of residual mitral regurgitation after MitraClip therapy in functional mitral regurgitation. Eur. J. Heart Fail. 2020, 22, 1840–1848. [Google Scholar] [CrossRef]
- Neuss, M.; Schau, T.; Isotani, A.; Pilz, M.; Schöpp, M.; Butter, C. Elevated Mitral Valve Pressure Gradient After MitraClip Implantation Deteriorates Long-Term Outcome in Patients With Severe Mitral Regurgitation and Severe Heart Failure. JACC Cardiovasc. Interv. 2017, 10, 931–939. [Google Scholar] [CrossRef]
- Patzelt, J.; Zhang, W.; Sauter, R.; Mezger, M.; Nording, H.; Ulrich, M.; Becker, A.; Patzelt, T.; Rudolph, V.; Eitel, I.; et al. Elevated Mitral Valve Pressure Gradient Is Predictive of Long-Term Outcome After Percutaneous Edge-to-Edge Mitral Valve Repair in Patients With Degenerative Mitral Regurgitation ( MR ), But Not in Functional MR. J. Am. Heart Assoc. 2019, 8, e011366. [Google Scholar] [CrossRef]
- Halaby, R.; Herrmann, H.C.; Gertz, Z.M.; Lim, S.; Kar, S.; Lindenfeld, J.; Abraham, W.T.; Grayburn, P.A.; Naidu, S.; Asch, F.M.; et al. Effect of Mitral Valve Gradient After MitraClip on Outcomes in Secondary Mitral Regurgitation: Results From the COAPT Trial. JACC Cardiovasc. Interv. 2021, 14, 879–889. [Google Scholar] [CrossRef]
- Öztürk, C.; Sprenger, K.; Tabata, N.; Sugiura, A.; Weber, M.; Nickenig, G.; Schueler, R. The predictive value of intraprocedural mitral gradient for outcomes after MitraClip and its peri-interventional dynamics. Echocardiography 2021, 38, 1115–1124. [Google Scholar] [CrossRef]
- Orban, M.; Orban, M.; Lesevic, H.; Braun, D.; Deseive, S.; Sonne, C.; Hutterer, L.; Grebmer, C.; Khandoga, A.; Pache, J.; et al. Predictors for long-term survival after transcatheter edge-to-edge mitral valve repair. J. Intervent. Cardiol. 2017, 30, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.S.; Reynolds, M.R.; Feldman, T.; Kar, S.; Herrmann, H.C.; Wang, A.; Whitlow, P.L.; Gray, W.A.; Grayburn, P.; Mack, M.J.; et al. Improved functional status and quality of life in prohibitive surgical risk patients with degenerative mitral regurgitation after transcatheter mitral valve repair. J. Am. Coll. Cardiol. 2014, 64, 182–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buzzatti, N.; De Bonis, M.; Denti, P.; Barili, F.; Schiavi, D.; Di Giannuario, G.; La Canna, G.; Alfieri, O. What is a ‘good’ result after transcatheter mitral repair? Impact of 2+ residual mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2016, 151, 88–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puls, M.; Tichelbäcker, T.; Bleckmann, A.; Hünlich, M.; Ehe, K.; von der Beuthner, B.E.; Rüter, K.; Beißbarth, T.; Seipelt, R.; Schöndube, F.; et al. Failure of acute procedural success predicts adverse outcome after percutaneous edge-to-edge mitral valve repair with MitraClip. EuroIntervention J. Eur. Collab. Work Group Interv. Cardiol. Eur. Soc. Cardiol. 2014, 9, 1407–1417. [Google Scholar] [CrossRef]
- Capodanno, D.; Adamo, M.; Barbanti, M.; Giannini, C.; Laudisa, M.L.; Cannata, S.; Curello, S.; Immè, S.; Maffeo, D.; Bedogni, F.; et al. GRASP-IT Investigators. Predictors of clinical outcomes after edge-to-edge percutaneous mitral valve repair. Am. Heart J. 2015, 170, 187–195. [Google Scholar] [CrossRef]
- Sürder, D.; Pedrazzini, G.; Gaemperli, O.; Biaggi, P.; Felix, C.; Rufibach, K.; Maur CA der Jeger, R.; Buser, P.; Kaufmann, B.A.; Moccetti, M.; et al. Predictors for efficacy of percutaneous mitral valve repair using the MitraClip system: The results of the MitraSwiss registry. Heart Br. Card. Soc. 2013, 99, 1034–1040. [Google Scholar] [CrossRef] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713, quiz 786–788. [Google Scholar]
- Zoghbi, W.A.; Asch, F.M.; Bruce, C.; Gillam, L.D.; Grayburn, P.A.; Hahn, R.T.; Inglessis, I.; Islam, A.M.; Lerakis, S.; Little, S.H.; et al. Guidelines for the Evaluation of Valvular Regurgitation After Percutaneous Valve Repair or Replacement: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2019, 32, 431–475. [Google Scholar]
- Foster, E.; Wasserman, H.S.; Gray, W.; Homma, S.; Di Tullio, M.R.; Rodriguez, L.; Stewart, W.J.; Whitlow, P.; Block, P.; Martin, R.; et al. Quantitative assessment of severity of mitral regurgitation by serial echocardiography in a multicenter clinical trial of percutaneous mitral valve repair. Am. J. Cardiol. 2007, 100, 1577–1583. [Google Scholar] [CrossRef]
- Stone, G.W.; Adams, D.H.; Abraham, W.T.; Kappetein, A.P.; Généreux, P.; Vranckx, P.; Mehran, R.; Kuck, K.-H.; Leon, M.B.; Piazza, N.; et al. Mitral Valve Academic Research Consortium (MVARC). Clinical Trial Design Principles and Endpoint Definitions for Transcatheter Mitral Valve Repair and Replacement: Part 2: Endpoint Definitions: A Consensus Document From the Mitral Valve Academic Research Consortium. J. Am. Coll. Cardiol. 2015, 66, 308–321. [Google Scholar] [PubMed]
- Tabata, N.; Weber, M.; Sugiura, A.; Öztürk, C.; Ishii, M.; Tsujita, K.; Nickenig, G.; Sinning, J.-M. Impact of the Leaflet-to-Annulus Index on Residual Mitral Regurgitation in Patients Undergoing Edge-to-Edge Mitral Repair. JACC Cardiovasc. Interv. 2019, 12, 2462–2472. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, H.C.; Rohatgi, S.; Wasserman, H.S.; Block, P.; Gray, W.; Hamilton, A.; Zunamon, A.; Homma, S.; Di Tullio, M.R.; Kraybill, K.; et al. Mitral valve hemodynamic effects of percutaneous edge-to-edge repair with the MitraClip device for mitral regurgitation. Catheter Cardiovasc. Interv. 2006, 68, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Boerlage-van Dijk, K.; van Riel, A.C.M.J.; de Bruin-Bon, R.H.A.C.M.; Wiegerinck, E.M.A.; Koch, K.T.; Vis, M.M.; Meregalli, P.G.; Bindraban, N.R.; Mulder, B.J.M.; Piek, J.J.; et al. Mitral inflow patterns after MitraClip implantation at rest and during exercise. J. Am. Soc. Echocardiogr. 2014, 27, 24–31.e1. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, P.; Felix, C.; Gruner, C.; Herzog, B.A.; Hohlfeld, S.; Gaemperli, O.; Stähli, B.E.; Paul, M.; Held, L.; Tanner, F.C.; et al. Assessment of mitral valve area during percutaneous mitral valve repair using the MitraClip system: Comparison of different echocardiographic methods. Circ. Cardiovasc. Imaging 2013, 6, 1032–1040. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, H.C.; Kar, S.; Siegel, R.; Fail, P.; Loghin, C.; Lim, S.; Hahn, R.; Rogers, J.H.; Bommer, W.J.; Wang, A.; et al. Effect of percutaneous mitral repair with the MitraClip device on mitral valve area and gradient. EuroIntervention J. Eur. Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2009, 4, 437–442. [Google Scholar] [CrossRef]
- Grayburn, P.A.; She, L.; Roberts, B.J.; Golba, K.S.; Mokrzycki, K.; Drozdz, J.; Cherniavsky, A.; Przybylski, R.; Wrobel, K.; Asch, F.M.; et al. Comparison of Transesophageal and Transthoracic Echocardiographic Measurements of Mechanism and Severity of Mitral Regurgitation in Ischemic Cardiomyopathy (from the Surgical Treatment of Ischemic Heart Failure Trial). Am. J. Cardiol. 2015, 116, 913–918. [Google Scholar] [CrossRef] [Green Version]
- Honjo, O.; Kotani, Y.; Osaki, S.; Fujita, Y.; Suezawa, T.; Tateishi, A.; Ishino, K.; Kawada, M.; Akagi, T.; Sano, S. Discrepancy between intraoperative transesophageal echocardiography and postoperative transthoracic echocardiography in assessing congenital valve surgery. Ann. Thorac. Surg. 2006, 82, 2240–2246. [Google Scholar] [CrossRef]
- Saiki, Y.; Kasegawa, H.; Kawase, M.; Osada, H.; Ootaki, E. Intraoperative TEE during mitral valve repair: Does it predict early and late postoperative mitral valve dysfunction? Ann. Thorac. Surg. 1998, 66, 1277–1281. [Google Scholar] [CrossRef]
- Dietl, A.; Prieschenk, C.; Eckert, F.; Birner, C.; Luchner, A.; Maier, L.S.; Buchner, S. 3D vena contracta area after MitraClip© procedure: Precise quantification of residual mitral regurgitation and identification of prognostic information. Cardiovasc. Ultrasound 2018, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Patzelt, J.; Zhang, Y.; Seizer, P.; Magunia, H.; Henning, A.; Riemlova, V.; Patzelt, T.A.E.; Hansen, M.; Haap, M.; Riessen, R.; et al. Effects of Mechanical Ventilation on Heart Geometry and Mitral Valve Leaflet Coaptation During Percutaneous Edge-to-Edge Mitral Valve Repair. JACC Cardiovasc. Interv. 2016, 9, 151–159. [Google Scholar] [CrossRef]
- Rahimtoola, S.H.; Durairaj, A.; Mehra, A.; Nuno, I. Current Evaluation and Management of Patients With Mitral Stenosis; American Heart Association. Circulation 2002, 106, 1183–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Evangelista, A.; Griffin, B.P.; Iung, B.; Otto, C.M.; Pellikka, P.A.; Quiñones, M. American Society of Echocardiography, European Association of Echocardiography. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J. Am. Soc. Echocardiogr. 2009, 22, 1–23, quiz 101–102. [Google Scholar] [CrossRef]
- Lin, B.A.; Forouhar, A.S.; Pahlevan, N.M.; Anastassiou, C.A.; Grayburn, P.A.; Thomas, J.D.; Gharib, M. Color Doppler jet area overestimates regurgitant volume when multiple jets are present. J. Am. Soc. Echocardiogr. 2010, 23, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Voelker, W.; Regele, B.; Dittmann, H.; Mauser, M.; Ickrath, O.; Schmid, K.M.; Karsch, K.R. Effect of heart rate on transmitral flow velocity profile and Doppler measurements of mitral valve area in patients with mitral stenosis. Eur. Heart. J. 1992, 13, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Gorlin, R.; Gorlin, S.G. Hydraulic formula for calculation of the area of the stenotic mitral valve, other cardiac valves, and central circulatory shunts. I. Am. Heart J. 1951, 41, 1–29. [Google Scholar] [CrossRef]
- Hoffmann, R.; Altiok, E.; Reith, S.; Brehmer, K.; Almalla, M. Functional effect of new atrial septal defect after percutaneous mitral valve repair using the MitraClip device. Am. J. Cardiol. 2014, 113, 1228–1233. [Google Scholar] [CrossRef]
- Smith, T.; McGinty, P.; Bommer, W.; Low, R.I.; Lim, S.; Fail, P.; Rogers, J.H. Prevalence and echocardiographic features of iatrogenic atrial septal defect after catheter-based mitral valve repair with the MitraClip system. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2012, 80, 678–685. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TEEMr Completion (TEE) | Pre-Discharge (TTE) | ||||||
|---|---|---|---|---|---|---|---|
| rMR ≤ 2 (n = 74) | rMR > 2 (n = 8) | p Value | rMR ≤ 1 (n = 54) | rMR > 1 (n = 28) | p Value | ||
| Age (years) | 75.2 ± 8.8 | 75.5 ± 7.5 | 0.921 | 75.2 ± 11.3 | 75.3 ± 9.3 | 0.982 | |
| Male | 40 (54.1%) | 6 (75%) | 0.456 | 29 (53.7%) | 17 (60.7%) | 0.641 | |
| Body Mass Index (kg/m2) | 27.8 ± 4.7 | 26.2 ± 4.4 | 0.39 | 28.2 ± 5.2 | 25.6 ± 4.6 | 0.119 | |
| Diabetes Mellitus | 34 (45.9%) | 3 (37.5%) | 0.724 | 25 (46.3%) | 13 (46.4%) | 1 | |
| Hyperlipidemia | 61 (82.4%) | 7 (87.5%) | 1 | 44 (81.5%) | 24 (85.7%) | 0.762 | |
| Hypertension | 63 (85.1%) | 5 (62.5%) | 0.132 | 45 (83.3%) | 23 (82.1%) | 1 | |
| Smoking History | 22 (29.7%) | 2 (25%) | 1 | 14 (25.9%) | 10 (35.7%) | 0.444 | |
| Ischemic Heart Disease | 49 (66.2%) | 5 (62.5%) | 1 | 35 (64.8%) | 19 (67.9%) | 0.812 | |
| Past Myocardial Infraction | 40 (54.1%) | 5 (62.5%) | 0.724 | 27 (50%) | 18 (64.3%) | 0.249 | |
| Past Coronary Intervention | PCI | 37 (50%) | 4 (50%) | 1 | 25 (46.3%) | 16 (57.1%) | 0.485 |
| CABG | 14 (18.9%) | 3 (37.5%) | 0.353 | 11 (20.4%) | 6 (21.4%) | 1 | |
| Past CVA or TIA | 17 (23%) | 2 (25%) | 1 | 13 (24.1%) | 6 (21.4%) | 1 | |
| COPD | 12 (16.2%) | 3 (37.5%) | 0.157 | 7 (13%) | 8 (28.6%) | 0.13 | |
| NYHA FC | II | 17 (23%) | 1 (12.5%) | 0.117 | 15 (27.8%) | 4 (14.3%) | 0.353 |
| III | 45 (60.8%) | 3 (37.5%) | 29 (53.7%) | 19 (67.9%) | |||
| IV | 14 (18.9%) | 4 (50%) | 10 (18.5%) | 5 (17.9%) | |||
| Past Year Heart Failure Admission (s) | 53 (71.6%) | 3 (37.5%) | 0.102 | 38 (70.4%) | 18 (64.3%) | 0.622 | |
| Atrial Fibrillation | 35 (47.3%) | 4 (50%) | 1 | 27 (50%) | 12 (42.9%) | 0.643 | |
| Pacemaker or Defibrillator | 21 (28.4%) | 2 (25%) | 1 | 17 (31.5%) | 6 (21.4%) | 0.44 | |
| eGFR (mL/min/1.73 mr2) ① | 56.1 ± 21.5 | 52.7 ± 22.7 | 0.69 | 55 ± 21.6 | 48.9 ± 23.6 | 0.247 | |
| Chronic Kidney Disease ② | 44 (59.5%) | 5 (62.5%) | 0.719 | 29 (53.7%) | 20 (71.4%) | 0.156 | |
| Hemoglobin (g/dL) | 11.3 ± 1.5 | 10.2 ± 1.8 | 0.06 | 11.4 ± 1.5 | 10.9 ± 1.7 | 0.211 | |
| Albumin (g/dL) | 3.7 ± 0.5 | 3.5 ± 0.6 | 0.3 | 3.7 ± 0.5 | 3.6 ± 0.5 | 0.442 | |
| Medications | SAPT | 23 (31.1%) | 3 (37.5%) | 0.704 | 15 (27.8%) | 11 (39.3%) | 0.324 |
| DAPT | 17 (23%) | 1 (12.5%) | 0.678 | 12 (22.2%) | 6 (21.4%) | 1 | |
| Oral Anticoagulant | 36 (48.6%) | 5 (62.5%) | 0.712 | 28 (51.9%) | 13 (46.4%) | 0.816 | |
| ACE-I/ARB/ARNI | 44 (59.5%) | 2 (25%) | 0.13 | 37 (68.5%) | 14 (50%) | 0.149 | |
| Beta Blockers | 62 (83.8%) | 7 (87.5%) | 1 | 44 (81.5%) | 25 (89.3%) | 0.527 | |
| Spironolactone | 33 (44.6%) | 3 (37.5%) | 1 | 26 (48.1%) | 10 (35.7%) | 0.351 | |
| Loop Diuretic | 66 (89.2%) | 7 (87.5%) | 1 | 49 (90.7%) | 24 (85.7%) | 0.483 | |
| Urgency of Procedure ③ | Urgent | 9 (12.2%) | 2 (25%) | 0.199 | 7 (13%) | 4 (14.3%) | 0.469 |
| Expedited | 2 (2.7%) | 1 (12.5%) | 1 (1.8%) | 2 (7.1%) | |||
| Elective | 63 (85.1%) | 5 (62.5%) | 46 (85.2%) | 22 (78.6%) | |||
| Cardiogenic Shock Within 30 Days | 7 (9.5%) | 2 (25%) | 0.211 | 6 (11.1%) | 3 (10.7%) | 1 | |
| ACS Within 90 Days | 11 (14.9%) | 2 (25%) | 0.607 | 8 (14.8%) | 5 (17.9%) | 0.756 | |
| PCI Within 30 Days | 7 (9.5%) | 2 (25%) | 0.211 | 5 (9.3%) | 4 (14.3%) | 0.483 | |
| Surgical Risk | STS Score (%) ④ | 5.2 (2.8–9.0) | 12.7 (4.1–17.6) | 0.136 | 4.3 (2.6–9.2) | 6.2 (3.8–11.4) | 0.18 |
| EuroSCORE II (%)⑤ | 6.8 (4.0–12.4) | 10.7 (6.1–13.8) | 0.368 | 6.2 (3.2–11.9) | 9.3 (5.6–13.5) | 0.103 | |
| TEEMr Completion (TEE) | Pre-Discharge (TTE) | ||||||
|---|---|---|---|---|---|---|---|
| rMR ≤ 2 (n = 74) | rMR > 2 (n = 8) | p Value | rMR ≤ 1 (n = 54) | rMR > 1 (n = 28) | p Value | ||
| Left Ventricle End Diastolic Volume (mL) | 135.9 ± 45.3 | 151.2 ± 38.8 | 0.434 | 130 ± 42.3 | 152.7 ± 45.7 | 0.046 | |
| Left Ventricle End Systolic Volume (mL) | 79.8 ± 37.5 | 82.8 ± 23.8 | 0.847 | 77.3 ± 36.9 | 86 ± 34.2 | 0.347 | |
| Left Ventricle End Diastolic Diameter (mm) | 59.6 ± 8.1 | 58 ± 7.9 | 0.622 | 59 ± 8.3 | 60.4 ± 7.7 | 0.448 | |
| Left Ventricle End Systolic Diameter (mm) | 46.4 ± 10.2 | 44.7 ± 9.2 | 0.688 | 45.7 ± 10.2 | 47.1 ± 10.1 | 0.56 | |
| Left Ventricle Ejection Fraction (%) | 44.3 ± 15.1 | 46.3 ± 9.2 | 0.725 | 44.2 ± 14.6 | 45.1 ± 14.7 | 0.786 | |
| Left Atrium Volume (mL) | 98.3 ± 32.5 | 63.8 ± 19.1 | 0.014 | 94.9 ± 33.1 | 97 ± 32.7 | 0.794 | |
| Left Atrium Volume Index (mL/mr2) | 54.8 ± 16.6 | 37.2 ± 13.4 | 0.015 | 52.3 ± 16.8 | 55.7 ± 17.3 | 0.437 | |
| Mitral Regurgitation Mechanism | Primary | 23 (31.1%) | 3 (37.5%) | 0.873 | 17 (31.5%) | 9 (28.6%) | 0.385 |
| Secondary | 44 (59.4%) | 4 (50%) | 30 (55.5%) | 18 (67.8%) | |||
| Mixed | 7 (9.5%) | 1 (12.5%) | 7 (13%) | 1 (3.6%) | |||
| Mitral Regurgitation Grade ① | Moderate to Severe | 21 (28.4%) | 2 (25%) | 1 | 15 (27.8%) | 8 (28.6%) | 1 |
| Severe | 53 (71.6%) | 6 (75%) | 39 (72.2%) | 20 (71.4%) | |||
| Mitral Valve EROA (cm2) | 0.4 ± 0.21 | 0.64 ± 0.3 | 0.007 | 0.39 ± 0.18 | 0.5 ± 0.29 | 0.045 | |
| Mitral Valve Regurgitant Volume (mL) | 56.4 ± 23.3 | 73.7 ± 35.1 | 0.086 | 55.3 ± 22.9 | 62.9 ± 28.3 | 0.227 | |
| Severe Tricuspid Regurgitation or Worse ② | 9 (12.2%) | 2 (25%) | 0.291 | 8 (14.8%) | 3 (10.7%) | 0.741 | |
| Systolic Pulmonary Artery Pressure (mmHg) | 49.4 ± 14.4 | 44.6 ± 15 | 0.411 | 48.2 ± 14.2 | 50.4 ± 15.1 | 0.533 | |
| (a) | ||||||
| Univariable Analysis | Multivariable Analysis | |||||
| Variable | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Diabetes Mellitus | 3.18 | 1.76–5.73 | <0.001 | 4.28 | 1.66–11.06 | 0.003 |
| eGFR | 0.97 | 0.95–0.99 | 0.004 | 0.95 | 0.92–0.98 | <0.001 |
| Past MI | 2.67 | 0.82–8.7 | 0.104 | |||
| NYHA FC | 2.03 | 0.99–3.98 | 0.111 | |||
| Age | 1.02 | 0.97–1.08 | 0.382 | |||
| Gender | 1.06 | 0.46–2.46 | 0.891 | |||
| Hypertension | 2.04 | 0.47–8.78 | 0.336 | |||
| IHD | 1.65 | 0.61–4.49 | 0.323 | |||
| Atrial fibrillation | 0.84 | 0.35–1.97 | 0.695 | |||
| Hemoglobin | 0.77 | 0.59–1.02 | 0.112 | |||
| Albumin | 0.52 | 0.22–1.17 | 0.115 | |||
| Urgency of procedure | 1.77 | 0.60–5.19 | 0.296 | |||
| ACS within 90 days | 0.82 | 0.24–2.82 | 0.762 | |||
| STS score | 1.02 | 0.99–1.07 | 0.147 | |||
| LVEDV | 1 | 0.99–1.01 | 0.767 | |||
| LVESV | 1 | 0.99–1.01 | 0.695 | |||
| LVEF | 0.98 | 0.96–0.99 | 0.05 | 0.93 | 0.87–0.99 | 0.018 |
| rMR ≤ 1 vs. rMR-2; TEEMr Completion | 0.59 | 0.21–1.65 | 0.316 | |||
| rMR ≤ 2 vs. rMR > 2; TEEMr Completion | 0.21 | 0.07–0.6 | 0.004 | 0.08 | 0.01–0.83 | 0.035 |
| MVPG; TEEMr Completion | 1.04 | 0.77–1.4 | 0.8 | |||
| rMR ≤ 1 vs. rMR-2; Discharge | 0.49 | 0.18–1.34 | 0.165 | |||
| rMR ≤ 2 vs. rMR > 2; Discharge | 0.95 | 0.28–3.24 | 0.937 | |||
| MVPG; Discharge | 1.08 | 0.88–1.33 | 0.448 | |||
| (b) | ||||||
| Univariable Analysis | Multivariable Analysis | |||||
| Variable | HR | 95% CI | p Value | HR | 95% CI | p Value |
| Diabetes Mellitus | 2.76 | 1.74–4.36 | 0.001 | 2.37 | 1.34–4.18 | 0.003 |
| eGFR | 0.98 | 0.97–1.00 | 0.122 | |||
| Past MI | 2.42 | 1.16–5.05 | 0.019 | 2.39 | 0.77–7.08 | 0.133 |
| NYHA | 1.5 | 1.01–2.67 | 0.05 | 2.12 | 0.97–4.61 | 0.059 |
| Age | 0.98 | 0.94–1.02 | 0.355 | |||
| Gender | 0.78 | 0.39–1.55 | 0.49 | |||
| Hypertension | 1.34 | 0.51–3.46 | 0.545 | |||
| IHD | 1.85 | 0.83–4.08 | 0.127 | |||
| Atrial fibrillation | 0.54 | 0.27–1.10 | 0.091 | |||
| Hemoglobin | 0.96 | 0.77–1.19 | 0.731 | |||
| Albumin | 0.52 | 0.26–1.06 | 0.072 | |||
| Urgency of procedure | 0.96 | 0.57–1.62 | 0.897 | |||
| ACS within 90 days | 1.39 | 0.60–3.24 | 0.437 | |||
| STS score | 1.0 | 0.96–1.04 | 0.913 | |||
| LVEDV | 1.0 | 0.99–1.01 | 0.186 | |||
| LVESV | 1.0 | 0.99–1.01 | 0.348 | |||
| LVEF | 0.98 | 0.95–1 | 0.095 | |||
| rMR ≤ 1 vs. rMR-2; TEEMr Completion | 0.68 | 0.41–2 | 0.804 | |||
| rMR ≤ 2 vs. rMR > 2; TEEMr Completion | 0.35 | 0.12–1 | 0.06 | |||
| MVPG; TEEMr Completion | 1.08 | 0.85–1.37 | 0.53 | |||
| rMR ≤ 1 vs. rMR-2; Discharge | 0.48 | 0.2–0.98 | 0.045 | 0.24 | 0.08–0.73 | 0.012 |
| rMR ≤ 2 vs. rMR > 2; Discharge | 1.35 | 0.48–3.85 | 0.57 | |||
| MVPG; Discharge | 1.09 | 0.93–1.28 | 0.272 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sudarsky, D.; Kusniec, F.; Grosman-Rimon, L.; Lubovich, A.; Kinany, W.; Hazanov, E.; Gelbstein, M.; Birati, E.Y.; Carasso, S. Immediate Post-Procedural and Discharge Assessment of Mitral Valve Function Following Transcatheter Edge-to-Edge Mitral Valve Repair: Correlation and Association with Outcomes. J. Clin. Med. 2021, 10, 5448. https://doi.org/10.3390/jcm10225448
Sudarsky D, Kusniec F, Grosman-Rimon L, Lubovich A, Kinany W, Hazanov E, Gelbstein M, Birati EY, Carasso S. Immediate Post-Procedural and Discharge Assessment of Mitral Valve Function Following Transcatheter Edge-to-Edge Mitral Valve Repair: Correlation and Association with Outcomes. Journal of Clinical Medicine. 2021; 10(22):5448. https://doi.org/10.3390/jcm10225448
Chicago/Turabian StyleSudarsky, Doron, Fabio Kusniec, Liza Grosman-Rimon, Ala Lubovich, Wadia Kinany, Evgeni Hazanov, Michael Gelbstein, Edo Y. Birati, and Shemy Carasso. 2021. "Immediate Post-Procedural and Discharge Assessment of Mitral Valve Function Following Transcatheter Edge-to-Edge Mitral Valve Repair: Correlation and Association with Outcomes" Journal of Clinical Medicine 10, no. 22: 5448. https://doi.org/10.3390/jcm10225448