
Same Brain, Different Look?—The Impact of Scanner, Sequence and Preprocessing on Diffusion Imaging Outcome Parameters

 , , ,
, , ,
Abstract
:1. Introduction
- What is the reproducibility of DTI-derived measures across-scanners (with differing upgrade versions) using high-resolution diffusion-weighted MRI on two 3T high-field scanner systems?
- What is the intra-site but across-DWI-sequences comparison of DTI outcome measures from two sequences with matched protocols?
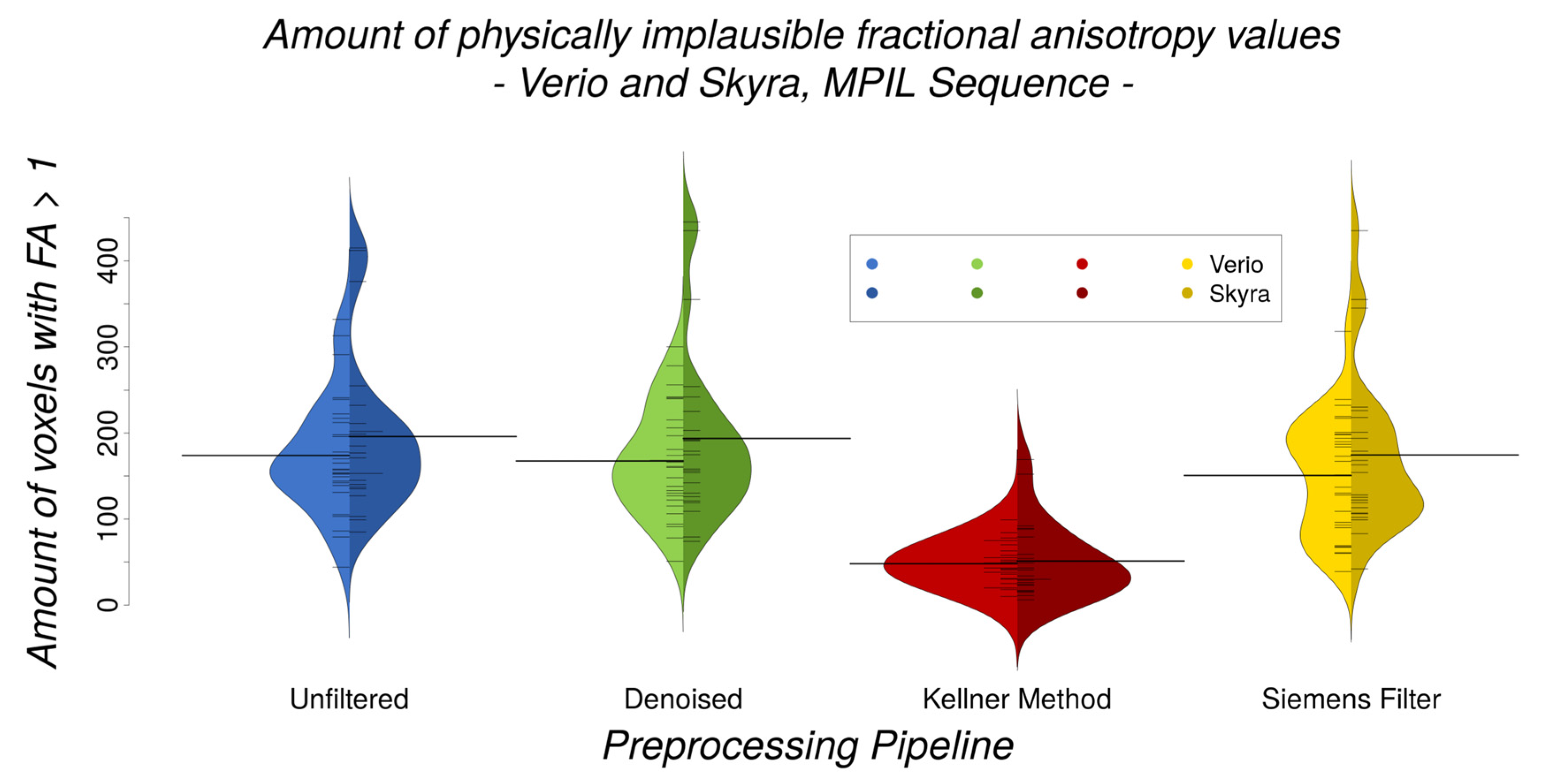
- What is the impact of different preprocessing tools on measurement reproducibility (image denoising, GR artefact reduction, default low-pass window filtering)?
- What are the conclusions to be drawn from the abovementioned results in relation to physiological effects (such as ageing) on white matter FA?
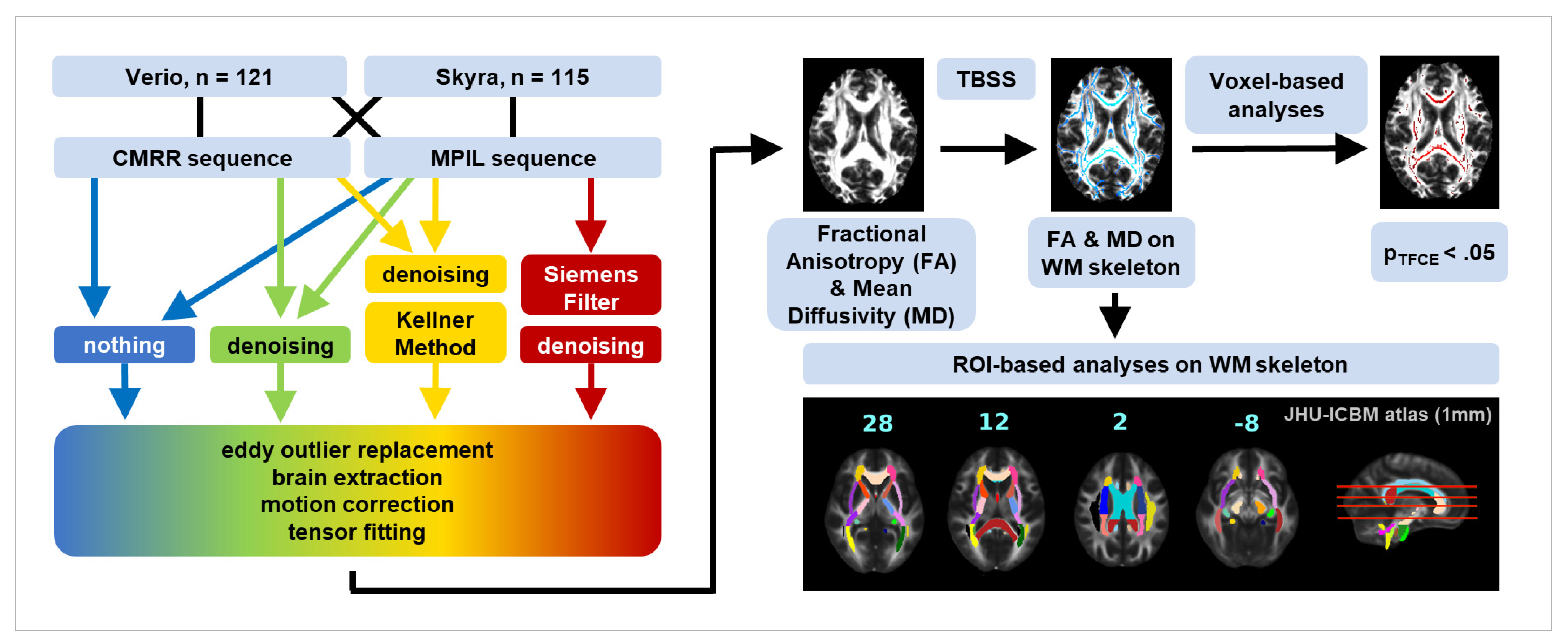
2. Methodology
2.1. Participants
2.2. MR image Acquisition
2.3. Image Processing
2.4. Quality Assessment
2.5. Region of Interest Approach
2.6. Statistical Analysis
2.6.1. Inter-Scanner Variability
2.6.2. Inter-Sequence Variability
2.6.3. Gibbs Ringing (GR) Artefact
2.6.4. Motion Effects
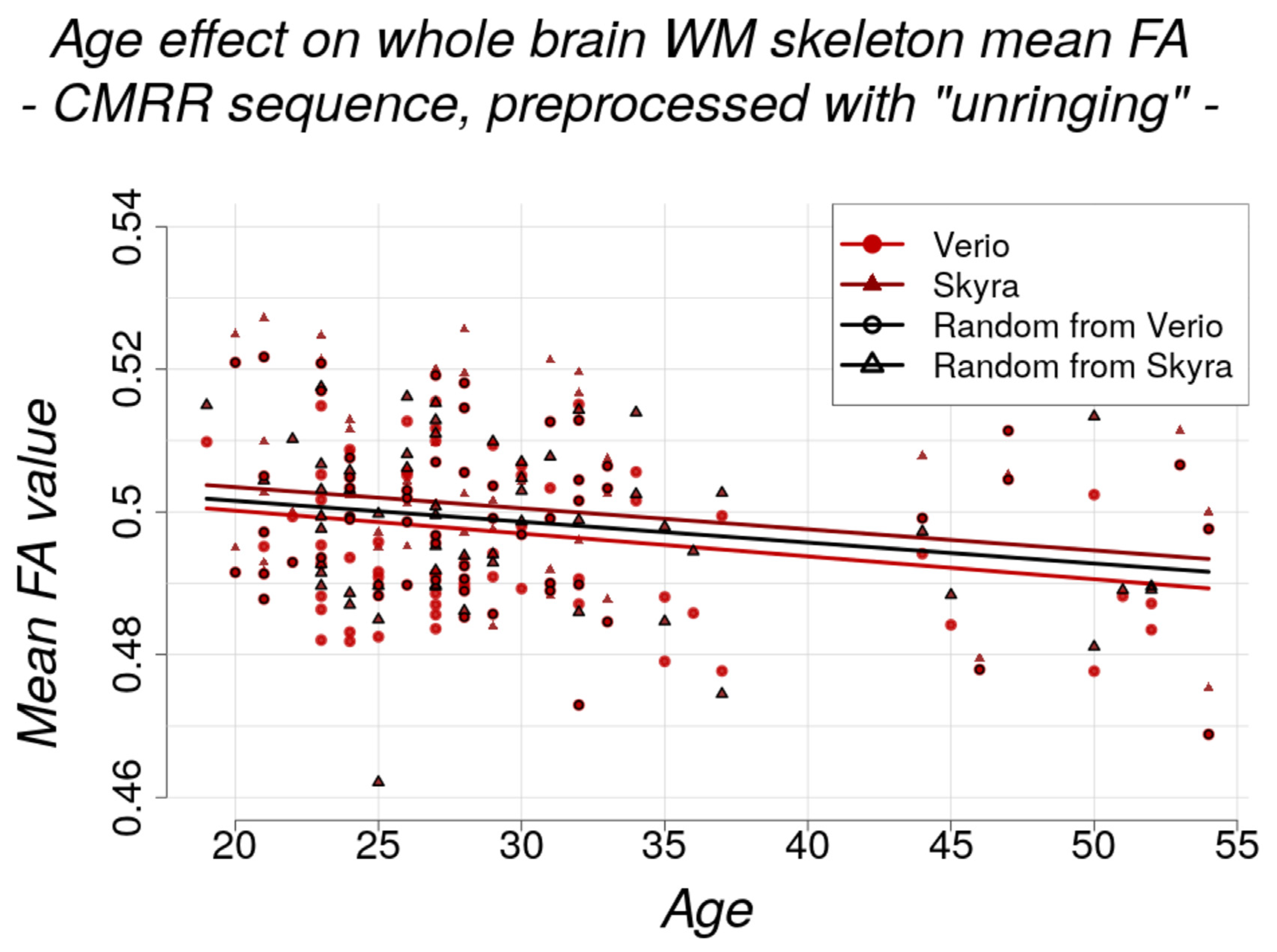
2.6.5. Age Effect
2.6.6. Harmonisation Attempt
2.7. Coefficient of Variance
3. Results
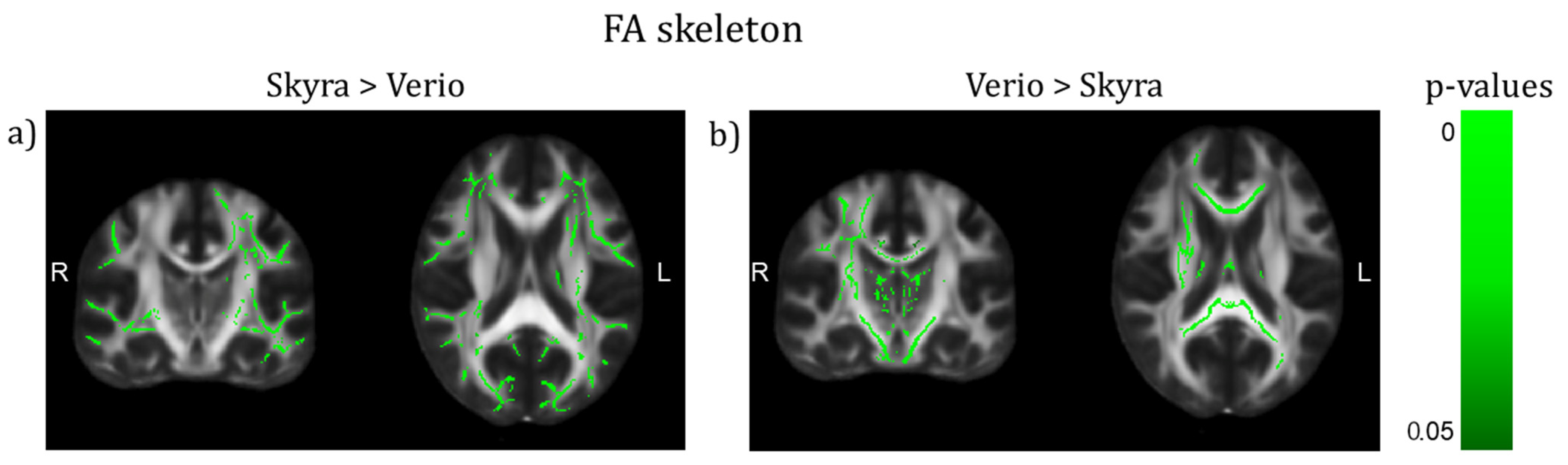
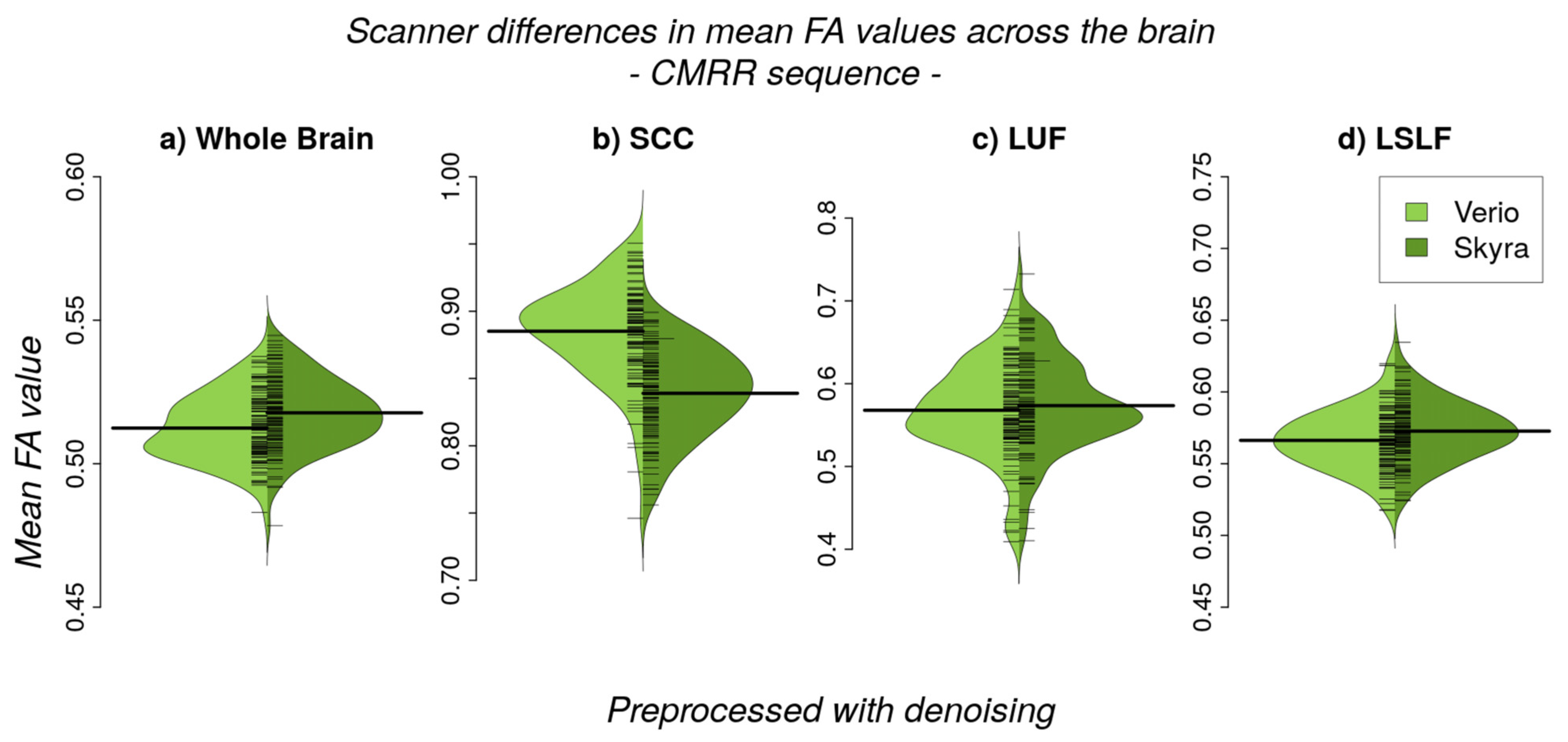
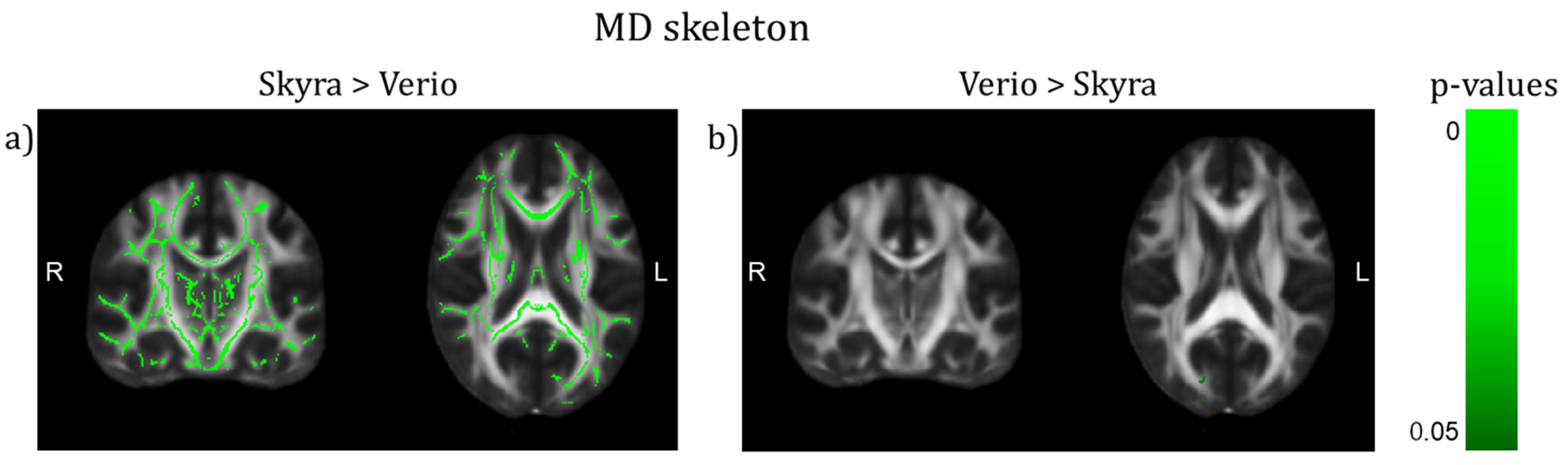
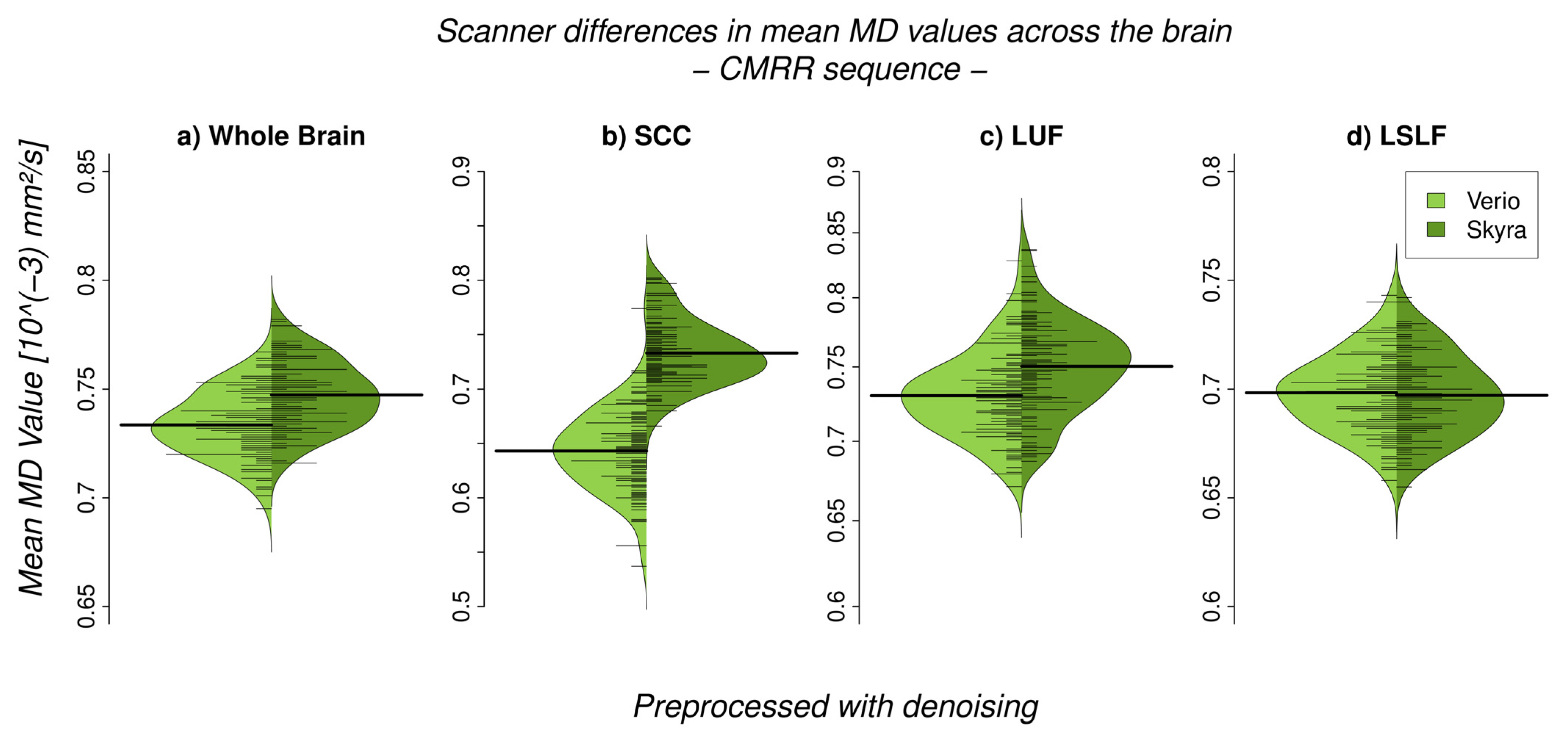
3.1. Inter-Scanner Variability
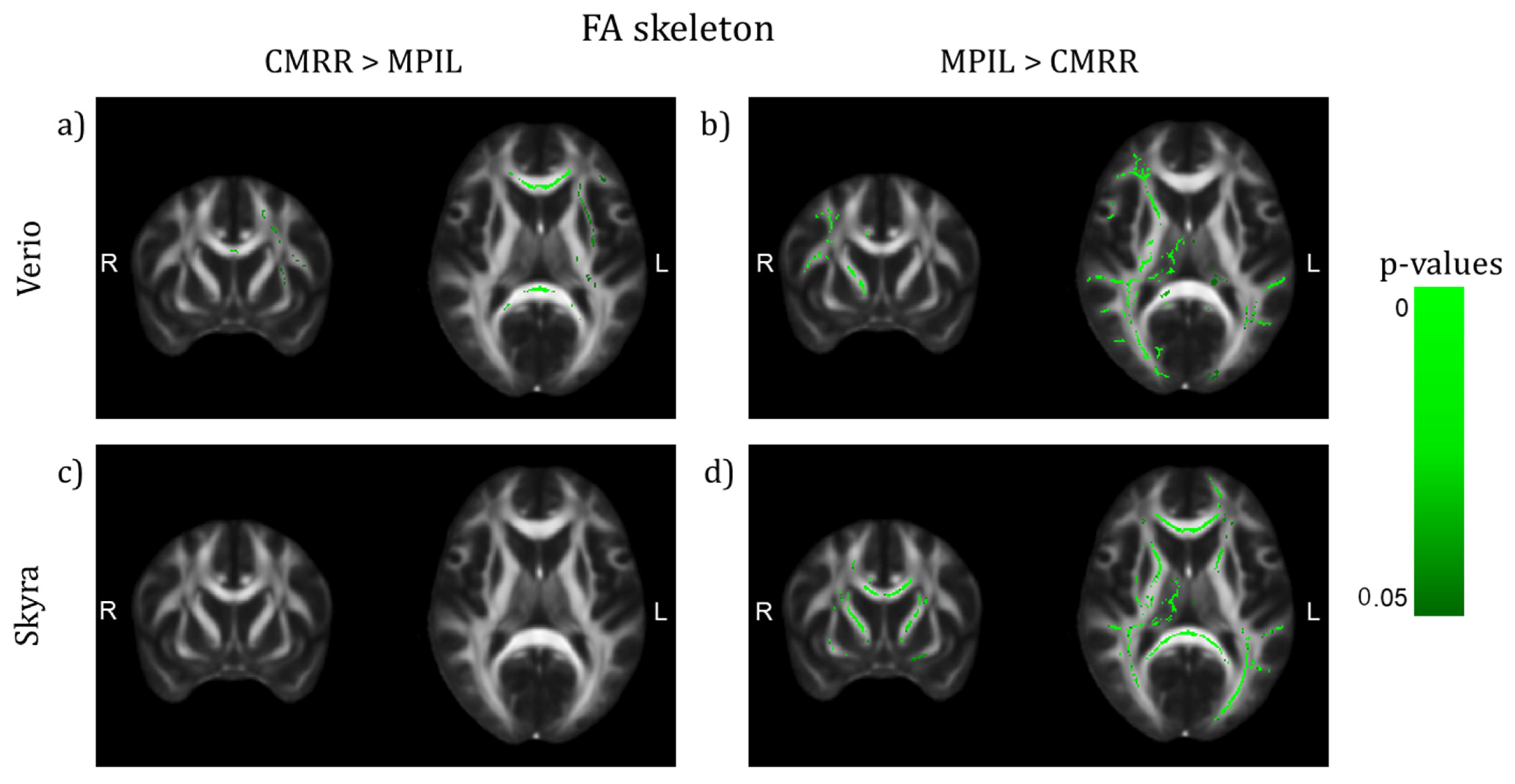
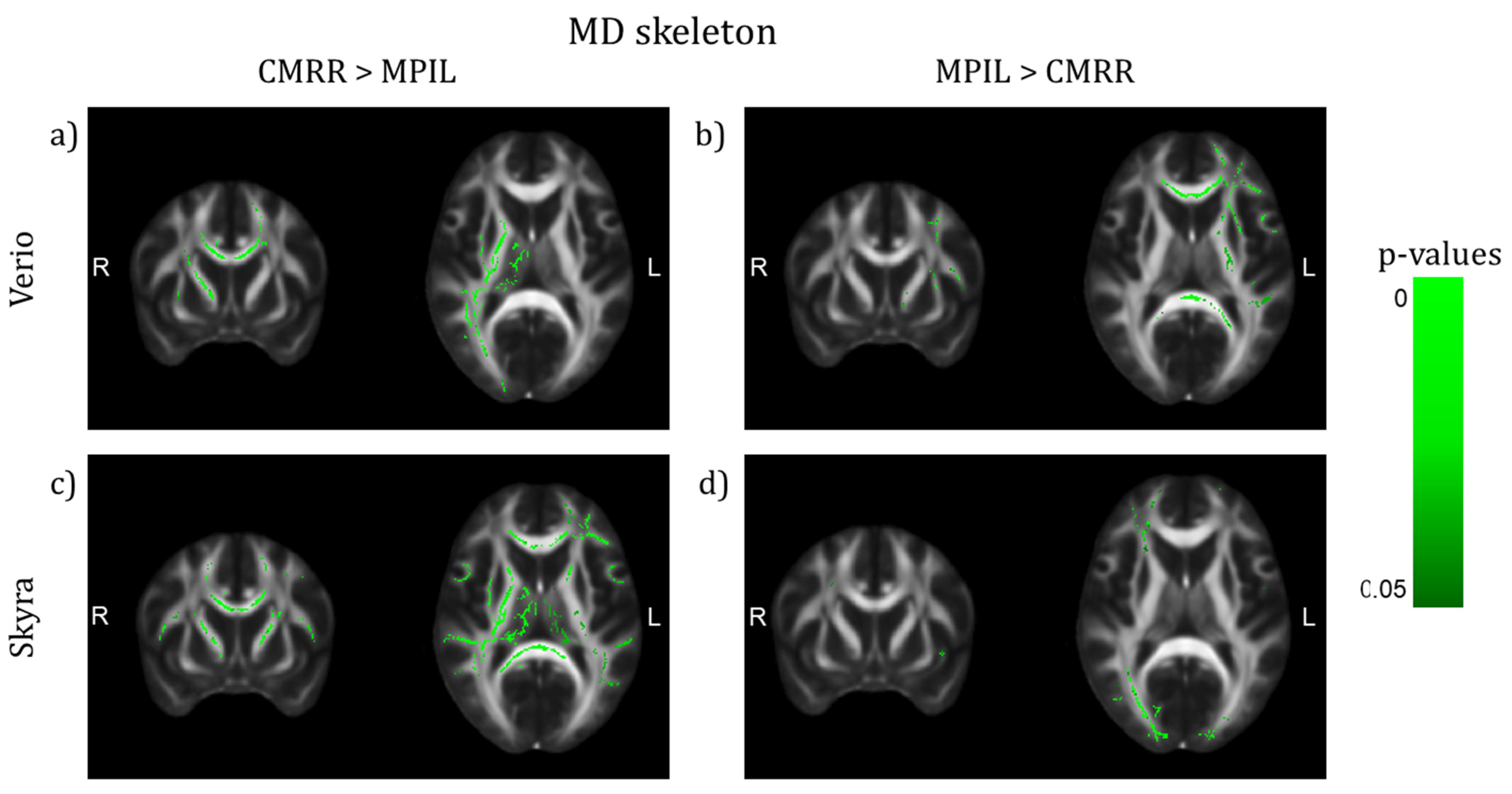
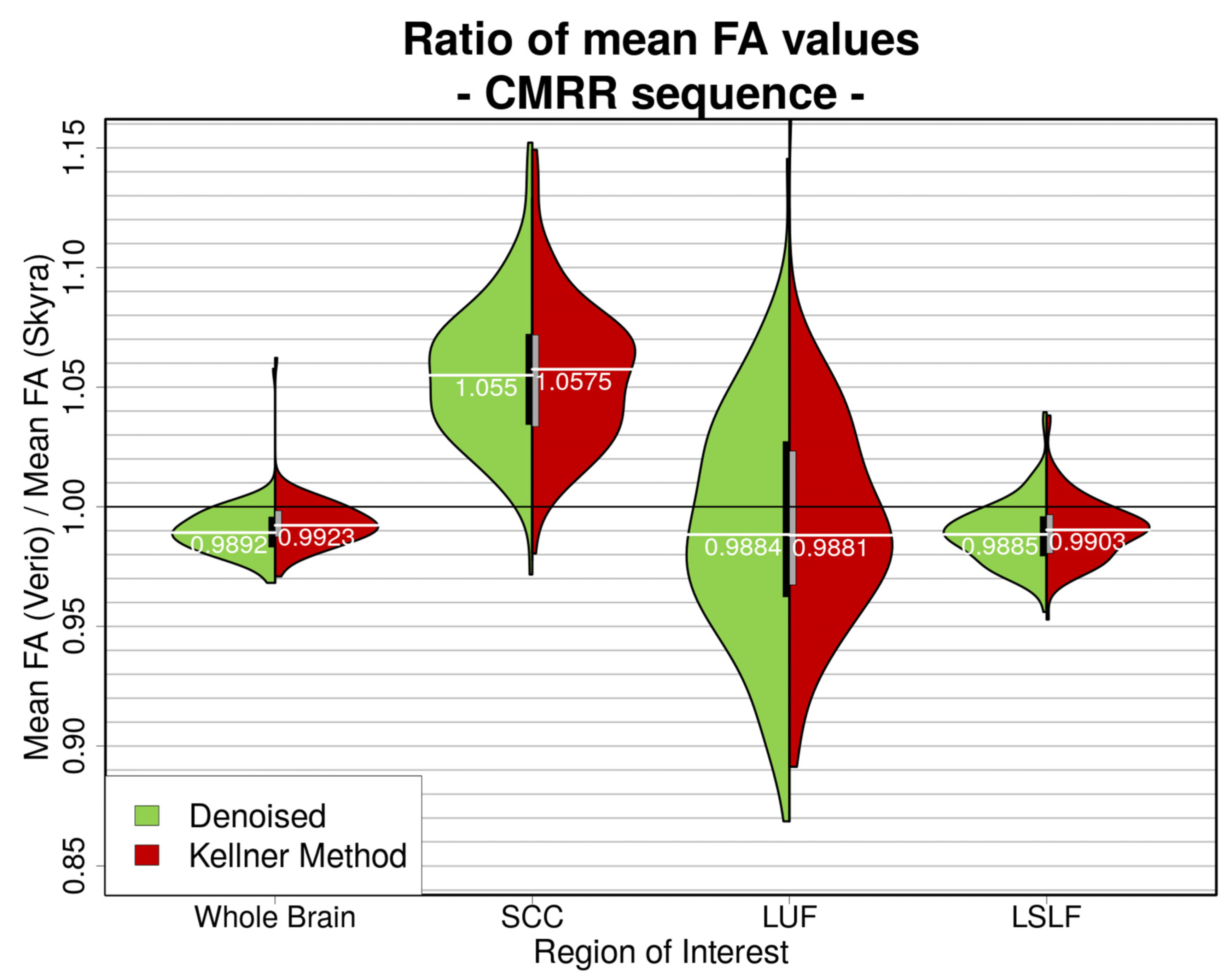
3.2. Inter-Sequence Variability
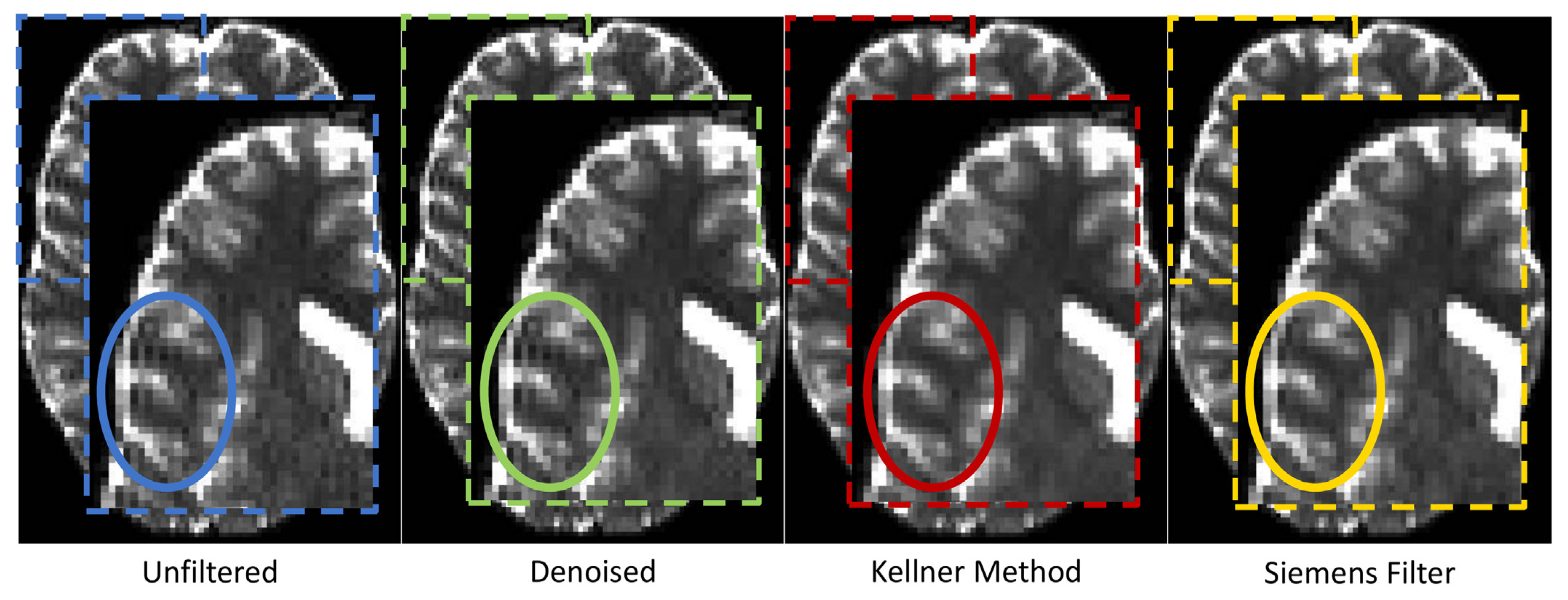
3.3. GR Artefact in DW Images
3.4. Motion Effects
3.5. Physiological Effects of Interest
3.6. Harmonisation Attempt
4. Discussion
4.1. Regional FA and MD Variability Due to Different Scanners and Sequence Parameters
4.2. Gibbs Ringing and Motion Artefacts
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leemans, A. Theory and applications of diffusion MRI. In Proceedings of the 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Rotterdam, The Netherlands, 14–17 April 2010; pp. 628–631. [Google Scholar] [CrossRef]
- Johansen-Berg, H.; Behrens, T.E.J. Diffusion MRI: From Quantitative Measurement to In-Vivo Neuroanatomy; Elsevier Science: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Basser, P.J.; Mattiello, J.; LeBihan, D. MR diffusion tensor spectroscopy and imaging. Biophys. J. 1994, 66, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Basser, P.J.; Jones, D.K. Diffusion-tensor MRI: Theory, experimental design and data analysis-a technical review. NMR Biomed. 2002, 15, 456–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assaf, Y.; Pasternak, O. Diffusion Tensor Imaging (DTI)-based White Matter Mapping in Brain Research: A Review. J. Mol. Neurosci. 2008, 34, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Tournier, J.-D.; Mori, S.; Leemans, A. Diffusion tensor imaging and beyond. Magn. Reson. Med. 2011, 65, 1532–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horsfield, M.A.; Jones, D.K. Applications of diffusion-weighted and diffusion tensor MRI to white matter diseases-a review. NMR Biomed. 2002, 15, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Jellison, B.J.; Field, A.S.; Medow, J.; Lazar, M.; Salamat, M.S.; Alexander, A.L. Diffusion tensor imaging of cerebral white matter: A pictorial review of physics, fiber tract anatomy, and tumor imaging patterns. AJNR. Am. J. Neuroradiol. 2004, 25, 356–369. [Google Scholar]
- Goveas, J.; O’Dwyer, L.; Mascalchi, M.; Cosottini, M.; Diciotti, S.; De Santis, S.; Passamonti, L.; Tessa, C.; Toschi, N.; Giannelli, M. Diffusion-MRI in neurodegenerative disorders. Magn. Reson. Imaging 2015, 33, 853–876. [Google Scholar] [CrossRef]
- De Groot, M.; Cremers, L.G.M.; Ikram, M.A.; Hofman, A.; Krestin, G.P.; van der Lugt, A.; Niessen, W.J.; Vernooij, M.W. White Matter Degeneration with Aging: Longitudinal Diffusion MR Imaging Analysis. Radiology 2016, 279, 532–541. [Google Scholar] [CrossRef] [Green Version]
- De Groot, M.; Ikram, M.A.; Akoudad, S.; Krestin, G.P.; Hofman, A.; van der Lugt, A.; Niessen, W.J.; Vernooij, M.W. Tract-specific white matter degeneration in aging: The Rotterdam Study. Alzheimer’s Dement. 2015, 11, 321–330. [Google Scholar] [CrossRef]
- Branzoli, F.; Ercan, E.; Valabrègue, R.; Wood, E.T.; Buijs, M.; Webb, A.; Ronen, I. Differentiating between axonal damage and demyelination in healthy aging by combining diffusion-tensor imaging and diffusion-weighted spectroscopy in the human corpus callosum at 7 T. Neurobiol. Aging 2016, 47, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Scholz, J.; Klein, M.C.; Behrens, T.E.J.; Johansen-Berg, H. Training induces changes in white-matter architecture. Nat. Neurosci. 2009, 12, 1370–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenfeld-Katzir, T.; Pasternak, O.; Dagan, M.; Assaf, Y. Diffusion MRI of Structural Brain Plasticity Induced by a Learning and Memory Task. PLoS ONE 2011, 6, e20678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatorre, R.J.; Fields, R.D.; Johansen-Berg, H. Plasticity in gray and white: Neuroimaging changes in brain structure during learning. Nat. Neurosci. 2012, 15, 528–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampaio-Baptista, C.; Johansen-Berg, H. White Matter Plasticity in the Adult Brain. Neuron 2017, 96, 1239–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Essen, D.C.; Smith, S.M.; Barch, D.M.; Behrens, T.E.J.; Yacoub, E.; Ugurbil, K.; WU-Minn HCP Consortium. The WU-Minn Human Connectome Project: An overview. NeuroImage 2013, 80, 62–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.L.; Alfaro-Almagro, F.; Bangerter, N.K.; Thomas, D.L.; Yacoub, E.; Xu, J.; Bartsch, A.J.; Jbabdi, S.; Sotiropoulos, S.N.; Andersson, J.L.R.; et al. Multimodal population brain imaging in the UK Biobank prospective epidemiological study. Nat. Neurosci. 2016, 19, 1523–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlett, C.; Hendel, T.; Weckbach, S.; Reiser, M.; Kauczor, H.; Nikolaou, K.; Günther, M.; Forsting, M.; Hosten, N.; Völzke, H.; et al. Population-Based Imaging and Radiomics: Rationale and Perspective of the German National Cohort MRI Study. RöFo-Fortschr. Dem Geb. Der Röntgenstrahlen Bildgeb. Verfahr. 2016, 188, 652–661. [Google Scholar] [CrossRef] [Green Version]
- Hasan, K.M.; Parker, D.L.; Alexander, A.L. Comparison of gradient encoding schemes for diffusion-tensor MRI. J. Magn. Reson. Imaging 2001, 13, 769–780. [Google Scholar] [CrossRef] [Green Version]
- Alexander, D.C.; Barker, G.J. Optimal imaging parameters for fibre-orientation estimation in diffusion MRI. NeuroImage 2005, 27, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.; Kavcic, V.; Zhu, T.; Ekholm, S.; Zhong, J. Effects of number of diffusion gradient directions on derived diffusion tensor imaging indices in human brain. AJNR. Am. J. Neuroradiol. 2006, 27, 1776–1781. Available online: http://www.ajnr.org/content/27/8/1776 (accessed on 2 July 2019). [PubMed]
- Giannelli, M.; Cosottini, M.; Michelassi, M.C.; Lazzarotti, G.; Belmonte, G.; Bartolozzi, C.; Lazzeri, M. Dependence of brain DTI maps of fractional anisotropy and mean diffusivity on the number of diffusion weighting directions. J. Appl. Clin. Med. Phys. 2010, 11, 176–190. [Google Scholar] [CrossRef] [PubMed]
- Schilling, K.G.; Nath, V.; Blaber, J.; Harrigan, R.L.; Ding, Z.; Anderson, A.W.; Landman, B.A. Effects of b-Value and Number of Gradient Directions on Diffusion MRI Measures Obtained with Q-ball Imaging. In Proceedings of the Medical Imaging 2017: Image Processing, Orlando, FL, USA, 11–16 February 2017; Styner, M.A., Angelini, E.D., Eds.; NIH Public Access: Bethesda, MA, USA, 2017; Volume 10133, p. 101330N. [Google Scholar] [CrossRef] [Green Version]
- Prohl, A.K.; Scherrer, B.; Tomas-Fernandez, X.; Filip-Dhima, R.; Kapur, K.; Velasco-Annis, C.; Clancy, S.; Carmody, E.; Dean, M.; Valle, M.; et al. Reproducibility of structural and diffusion tensor imaging in the TACERN multi-center study. Front. Integr. Neurosci. 2019, 13, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, D.L.; Tagge, I.; Powers, K.; Ahn, S.; Bakshi, R.; Calabresi, P.A.; Todd Constable, R.; Grinstead, J.; Henry, R.G.; Nair, G.; et al. Multisite reliability and repeatability of an advanced brain MRI protocol. J. Magn. Reson. Imaging 2019, 50, 878–888. [Google Scholar] [CrossRef]
- Tax, C.M.; Grussu, F.; Kaden, E.; Ning, L.; Rudrapatna, U.; John Evans, C.; St-Jean, S.; Leemans, A.; Koppers, S.; Merhof, D.; et al. Cross-scanner and cross-protocol diffusion MRI data harmonisation: A benchmark database and evaluation of algorithms. NeuroImage 2019, 195, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Palacios, E.M.; Martin, A.J.; Boss, M.A.; Ezekiel, F.; Chang, Y.S.; Yuh, E.L.; Vassar, M.J.; Schnyer, D.M.; MacDonald, C.L.; Crawford, K.L.; et al. Toward Precision and Reproducibility of Diffusion Tensor Imaging: A Multicenter Diffusion Phantom and Traveling Volunteer Study. Am. J. Neuroradiol. 2017, 38, 537–545. [Google Scholar] [CrossRef] [Green Version]
- Fortin, J.P.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. Harmonization of multi-site diffusion tensor imaging data. NeuroImage 2017, 161, 149–170. [Google Scholar] [CrossRef]
- Mirzaalian, H.; Ning, L.; Savadjiev, P.; Pasternak, O.; Bouix, S.; Michailovich, O.; Grant, G.; Marx, C.; Morey, R.A.; Flashman, L.A.; et al. Inter-site and inter-scanner diffusion MRI data harmonization. NeuroImage 2016, 135, 311–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belli, G.; Busoni, S.; Ciccarone, A.; Coniglio, A.; Esposito, M.; Giannelli, M.; Mazzoni, L.N.; Nocetti, L.; Sghedoni, R.; Tarducci, R.; et al. Quality assurance multicenter comparison of different MR scanners for quantitative diffusion-weighted imaging. J. Magn. Reson. Imaging 2016, 43, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, T.; Gullett, J.M.; Nguyen, P.; Boutzoukas, A.E.; Ford, A.; Colon-Perez, L.M.; Triplett, W.; Carney, P.R.; Mareci, T.H.; Price, C.C.; et al. Test-retest reliability of high angular resolution diffusion imaging acquisition within medial temporal lobe connections assessed via tract based spatial statistics, probabilistic tractography and a novel graph theory metric. Brain Imaging Behav. 2016, 10, 533–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, C.R.; Pernet, C.R.; Gorgolewski, K.J.; Storkey, A.J.; Bastin, M.E. Test–retest reliability of structural brain networks from diffusion MRI. NeuroImage 2014, 86, 231–243. [Google Scholar] [CrossRef] [Green Version]
- Zhan, L.; Jahanshad, N.; Jin, Y.; Nir, T.M.; Leonardo, C.D.; Bernstein, M.A.; Borowski, B.; Jack, C.R.; Thompson, P.M. Understanding scanner upgrade effects on brain integrity andamp; connectivity measures. In Proceedings of the 2014 IEEE 11th International Symposium on Biomedical Imaging (ISBI), Beijing, China, 29 April–2 May 2014; pp. 234–237. [Google Scholar] [CrossRef]
- Malyarenko, D.; Galbán, C.J.; Londy, F.J.; Meyer, C.R.; Johnson, T.D.; Rehemtulla, A.; Ross, B.D.; Chenevert, T.L. Multi-system repeatability and reproducibility of apparent diffusion coefficient measurement using an ice-water phantom. J. Magn. Reson. Imaging JMRI 2013, 37, 1238–1246. [Google Scholar] [CrossRef] [Green Version]
- Fox, R.J.; Sakaie, K.; Lee, J.-C.; Debbins, J.P.; Liu, Y.; Arnold, D.L.; Melhem, E.R.; Smith, C.H.; Philips, M.D.; Lowe, M.; et al. A validation study of multicenter diffusion tensor imaging: Reliability of fractional anisotropy and diffusivity values. AJNR. Am. J. Neuroradiol. 2012, 33, 695–700. [Google Scholar] [CrossRef] [Green Version]
- Teipel, S.J.; Reuter, S.; Stieltjes, B.; Acosta-Cabronero, J.; Ernemann, U.; Fellgiebel, A.; Filippi, M.; Frisoni, G.; Hentschel, F.; Jessen, F.; et al. Multicenter stability of diffusion tensor imaging measures: A European clinical and physical phantom study. Psychiatry Res. Neuroimaging 2011, 194, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Vollmar, C.; O’Muircheartaigh, J.; Barker, G.J.; Symms, M.R.; Thompson, P.; Kumari, V.; Duncan, J.S.; Richardson, M.P.; Koepp, M.J. Identical, but not the same: Intra-site and inter-site reproducibility of fractional anisotropy measures on two 3.0 T scanners. NeuroImage 2010, 51, 1384–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfefferbaum, A.; Adalsteinsson, E.; Sullivan, E.V. Replicability of diffusion tensor imaging measurements of fractional anisotropy and trace in brain. J. Magn. Reson. Imaging 2003, 18, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Pohl, K.M.; Sullivan, E.V.; Rohlfing, T.; Chu, W.; Kwon, D.; Nichols, B.N.; Zhang, Y.; Brown, S.A.; Tapert, S.F.; Cummins, K.; et al. Harmonizing DTI measurements across scanners to examine the development of white matter microstructure in 803 adolescents of the NCANDA study. NeuroImage 2016, 130, 194–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovicich, J.; Marizzoni, M.; Bosch, B.; Bartrés-Faz, D.; Arnold, J.; Benninghoff, J.; Wiltfang, J.; Roccatagliata, L.; Picco, A.; Nobili, F.; et al. Multisite longitudinal reliability of tract-based spatial statistics in diffusion tensor imaging of healthy elderly subjects. NeuroImage 2014, 101, 390–403. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. NeuroImage 2006, 31, 1487–1505. [Google Scholar] [CrossRef] [PubMed]
- Zavaliangos-Petropulu, A.; Nir, T.M.; Thomopoulos, S.I.; Reid, R.I.; Bernstein, M.A.; Borowski, B.; Jack, C.R.; Weiner, M.W.; Jahanshad, N.; Thompson, P.M. Diffusion MRI indices and their relation to cognitive impairment in brain aging: The updated multi-protocol approach in ADNI3. Front. Neuroinform. 2019, 13, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.J.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage 2004, 23, S208–S219. [Google Scholar] [CrossRef] [Green Version]
- Woolrich, M.W.; Jbabdi, S.; Patenaude, B.; Chappell, M.; Makni, S.; Behrens, T.; Beckmann, C.; Jenkinson, M.; Smith, S.M. Bayesian analysis of neuroimaging data in FSL. NeuroImage 2009, 45, S173–S186. [Google Scholar] [CrossRef] [PubMed]
- Andersson, J.L.R.; Sotiropoulos, S.N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. NeuroImage 2016, 125, 1063–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, D.; Aelterman, J.; Pižurica, A.; Jeurissen, B.; Philips, W.; Leemans, A. The effect of Gibbs ringing artifacts on measures derived from diffusion MRI. NeuroImage 2015, 120, 441–455. [Google Scholar] [CrossRef] [PubMed]
- Kellner, E.; Dhital, B.; Kiselev, V.G.; Reisert, M. Gibbs-ringing artifact removal based on local subvoxel-shifts. Magn. Reson. Med. 2016, 76, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Veraart, J.; Fieremans, E.; Jelescu, I.O.; Knoll, F.; Novikov, D.S. Gibbs ringing in diffusion MRI. Magn. Reson. Med. 2016, 76, 301–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Ruan, G.; Yang, W.; Liu, Y.; Zhao, K.; Feng, Q.; Chen, W.; Wu, E.X.; Feng, Y. MRI Gibbs-ringing artifact reduction by means of machine learning using convolutional neural networks. Magn. Reson. Med. 2019, 82, 2133–2145. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhang, H.; Zhou, Y.; Bian, W.; Zhang, T.; Zou, X. Gibbs-ringing artifact suppression with knowledge transfer from natural images to MR images. Multimed. Tools Appl. 2020, 79, 33711–33733. [Google Scholar] [CrossRef]
- Muckley, M.J.; Ades-Aron, B.; Papaioannou, A.; Lemberskiy, G.; Solomon, E.; Lui, Y.W.; Sodickson, D.K.; Fieremans, E.; Novikov, D.S.; Knoll, F. Training a neural network for Gibbs and noise removal in diffusion MRI. Magn. Reson. Med. 2021, 85, 413–428. [Google Scholar] [CrossRef] [PubMed]
- Constable, R.T.; Henkelman, R.M. Data extrapolation for truncation artifact removal. Magn. Reson. Med. 1991, 17, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Pan, C. Gibbs phenomenon removal and digital filtering directly through the fast Fourier transform. IEEE Trans. Signal Process. 2001, 49, 444–448. [Google Scholar] [CrossRef]
- Gelb, A.; Archibald, R. Reducing the Gibbs ringing artifact in MRI scans while maintaining tissue boundary integrity. In Proceedings of the IEEE International Symposium on Biomedical Imaging, Washington, DC, USA, 7–10 July 2002; pp. 923–926. [Google Scholar] [CrossRef]
- Veraart, J.; Fieremans, E.; Novikov, D.S. Diffusion MRI noise mapping using random matrix theory. Magn. Reson. Med. 2016, 76, 1582–1593. [Google Scholar] [CrossRef]
- Moeller, S.; Yacoub, E.; Olman, C.A.; Auerbach, E.; Strupp, J.; Harel, N.; Uǧurbil, K. Multiband multislice GE-EPI at 7 tesla, with 16-fold acceleration using partial parallel imaging with application to high spatial and temporal whole-brain FMRI. Magn. Reson. Med. 2010, 63, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Morgan, P.S.; Ashburner, J.; Smith, J.; Rorden, C. The first step for neuroimaging data analysis: DICOM to NIfTI conversion. J. Neurosci. Methods 2016, 264, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.M. Fast robust automated brain extraction. Hum. Brain Mapp. 2002, 17, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, G.; Müller, K.; Bosch, V.; Mentzel, H.; Hessler, S.; Chen, L.; Zysset, S.; von Cramon, D.Y. Lipsia—A new software system for the evaluation of functional magnetic resonance images of the human brain. Comput. Med. Imaging Graph. 2001, 25, 449–457. [Google Scholar] [CrossRef]
- Power, J.D.; Barnes, K.A.; Snyder, A.Z.; Schlaggar, B.L.; Petersen, S.E. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. NeuroImage 2012, 59, 2142–2154. [Google Scholar] [CrossRef] [Green Version]
- Beyer, F.; Kharabian Masouleh, S.; Huntenburg, J.M.; Lampe, L.; Luck, T.; Riedel-Heller, S.G.; Loeffler, M.; Schroeter, M.L.; Stumvoll, M.; Villringer, A.; et al. Higher body mass index is associated with reduced posterior default mode connectivity in older adults. Hum. Brain Mapp. 2017, 38, 3502–3515. [Google Scholar] [CrossRef] [Green Version]
- Loeffler, M.; Engel, C.; Ahnert, P.; Alfermann, D.; Arelin, K.; Baber, R.; Beutner, F.; Binder, H.; Brähler, E.; Burkhardt, R.; et al. The LIFE-Adult-Study: Objectives and design of a population-based cohort study with 10,000 deeply phenotyped adults in Germany. BMC Public Health 2015, 15, 691. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Beyer, F.; Lampe, L.; Luck, T.; Riedel-Heller, S.G.; Loeffler, M.; Schroeter, M.L.; Stumvoll, M.; Villringer, A.; Witte, A.V. White matter microstructural variability mediates the relation between obesity and cognition in healthy adults. NeuroImage 2018, 172, 239–249. [Google Scholar] [CrossRef]
- Medawar, E.; Thieleking, R.; Manuilova, I.; Paerisch, M.; Villringer, A.; Witte, A.V.; Beyer, F. Estimating the effect of a scanner upgrade on measures of grey matter structure for longitudinal designs. PLoS ONE 2021, 16, e0239021. [Google Scholar] [CrossRef]
- Holdsworth, S.; Bammer, R. Magnetic Resonance Imaging Techniques: fMRI, DWI, and PWI. Semin. Neurol. 2008, 28, 395–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madhyastha, T.; Mérillat, S.; Hirsiger, S.; Bezzola, L.; Liem, F.; Grabowski, T.; Jäncke, L. Longitudinal reliability of tract-based spatial statistics in diffusion tensor imaging. Hum. Brain Mapp. 2014, 35, 4544–4555. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Fedeli, L.; Belli, G.; Ciccarone, A.; Coniglio, A.; Esposito, M.; Giannelli, M.; Mazzoni, L.N.; Nocetti, L.; Sghedoni, R.; Tarducci, R.; et al. Dependence of apparent diffusion coefficient measurement on diffusion gradient direction and spatial position–A quality assurance intercomparison study of forty-four scanners for quantitative diffusion-weighted imaging. Phys. Med. 2018, 55, 135–141. [Google Scholar] [CrossRef]
- Koay, C.G.; Carew, J.D.; Alexander, A.L.; Basser, P.J.; Meyerand, M.E. Investigation of anomalous estimates of tensor-derived quantities in diffusion tensor imaging. Magn. Reson. Med. 2006, 55, 930–936. [Google Scholar] [CrossRef]
- Tan, E.T.; Marinelli, L.; Slavens, Z.W.; King, K.F.; Hardy, C.J. Improved correction for gradient nonlinearity effects in diffusion-weighted imaging. J. Magn. Reson. Imaging 2013, 38, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Fedeli, L.; Benelli, M.; Busoni, S.; Belli, G.; Ciccarone, A.; Coniglio, A.; Esposito, M.; Nocetti, L.; Sghedoni, R.; Tarducci, R.; et al. On the dependence of quantitative diffusion-weighted imaging on scanner system characteristics and acquisition parameters: A large multicenter and multiparametric phantom study with unsupervised clustering analysis. Phys. Med. 2021, 85, 98–106. [Google Scholar] [CrossRef]
- Streitbuerger, D.-P.; Möller, H.E.; Tittgemeyer, M.; Hund-Georgiadis, M.; Schroeter, M.L.; Mueller, K. Investigating Structural Brain Changes of Dehydration Using Voxel-Based Morphometry. PLoS ONE 2012, 7, e44195. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| WM Skeleton (After Denoising) | Scanner | Mean FA Value | SD | CoV |Verio—Skyra|(%) | Linear Model Bayes Factor (Mean FA Value ~ Scanner, n = 115) |
|---|---|---|---|---|---|
| whole brain | Verio | 0.5124 | 0.0112 | 7.1 | 33.9 |
| Skyra | 0.5177 | 0.0121 | |||
| SCC | Verio | 0.7796 | 0.0168 | 30.7 | 1.1 × 1032 |
| Skyra | 0.7631 | 0.0172 | |||
| LUF | Verio | 0.5679 | 0.0566 | 31.5 | 1.1 |
| Skyra | 0.5735 | 0.0571 | |||
| LSLF | Verio | 0.5663 | 0.0204 | 11.1 | 3.3 × 1012 |
| Skyra | 0.5727 | 0.0208 |
| WM Skeleton (After Denoising) | Scanner | Mean MD Value [10−3 mm/s2] | SD [10−3 mm/s2] | CoV |Verio − Skyra| (%) | Linear Model Bayes Factor (Mean MD value ~ Scanner, n = 115) |
|---|---|---|---|---|---|
| whole brain | Verio | 0.7336 | 0.0149 | 11.1 | 1.4 × 108 |
| Skyra | 0.7474 | 0.0155 | |||
| SCC | Verio | 0.6431 | 0.0370 | 27.4 | 1.3 × 1050 |
| Skyra | 0.7330 | 0.0289 | |||
| LUF | Verio | 0.7310 | 0.0285 | 28.3 | 1.4 × 104 |
| Skyra | 0.7511 | 0.0321 | |||
| LSLF | Verio | 0.6983 | 0.0173 | 13.9 | 0.16 |
| Skyra | 0.6972 | 0.0186 |
| Contrast of Preprocessing Pipelines | Bayes Factor of Paired t-Test on Mean FD Values (n = 115) | CoV |Preprocessing Step − Preprocessing Step| (%) | |
|---|---|---|---|
| Verio | Skyra | ||
| unfiltered ~ denoised | > 2 × 109 | 20.5 | 27.4 |
| unfiltered ~ Kellner Method | > 5 × 106 | 27.8 | 40.2 |
| denoised ~ Kellner Method | 0.241 | 61.6 | 71.8 |
| Preprocessing Pipeline | Mean FD Value ± SD (mm) | CoV (%) |Verio − Skyra| | |
|---|---|---|---|
| Verio | Skyra | ||
| unfiltered | 0.417 ± 0.061 | 0.293 ± 0.064 | 41.9 |
| denoised | 0.355 ± 0.066 | 0.263 ± 0.066 | 47.3 |
| Kellner Method | 0.364 ± 0.067 | 0.269 ± 0.067 | 46.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thieleking, R.; Zhang, R.; Paerisch, M.; Wirkner, K.; Anwander, A.; Beyer, F.; Villringer, A.; Witte, A.V. Same Brain, Different Look?—The Impact of Scanner, Sequence and Preprocessing on Diffusion Imaging Outcome Parameters. J. Clin. Med. 2021, 10, 4987. https://doi.org/10.3390/jcm10214987
Thieleking R, Zhang R, Paerisch M, Wirkner K, Anwander A, Beyer F, Villringer A, Witte AV. Same Brain, Different Look?—The Impact of Scanner, Sequence and Preprocessing on Diffusion Imaging Outcome Parameters. Journal of Clinical Medicine. 2021; 10(21):4987. https://doi.org/10.3390/jcm10214987
Chicago/Turabian StyleThieleking, Ronja, Rui Zhang, Maria Paerisch, Kerstin Wirkner, Alfred Anwander, Frauke Beyer, Arno Villringer, and A. Veronica Witte. 2021. "Same Brain, Different Look?—The Impact of Scanner, Sequence and Preprocessing on Diffusion Imaging Outcome Parameters" Journal of Clinical Medicine 10, no. 21: 4987. https://doi.org/10.3390/jcm10214987