
Shaft Fractures in Patients Requiring Primary or Revision Total Knee Arthroplasty Can Be Successfully Treated with Long-Stemmed Implants without Additional Fixation

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yoo, J.D.; Kim, N.K. Periprosthetic fractures following total knee arthroplasty. Knee Surg. Relat. Res. 2015, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, M.R.; Mehendale, S. Periprosthetic fractures around the knee: Current concepts and advances in management. Curr. Rev. Musculoskelet. Med. 2014, 7, 136–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alden, K.J.; Duncan, W.H.; Trousdale, R.T.; Pagnano, M.W.; Haidukewych, G.J. Intraoperative fracture during primary total knee arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Canton, G.; Ratti, C.; Fattori, R.; Hoxhaj, B.; Murena, L. Periprosthetic knee fractures. A review of epidemiology, risk factors, diagnosis, management and outcome. Acta Biomed. 2017, 88, 118–128. [Google Scholar]
- Meek, R.M.; Norwood, T.; Smith, R.; Brenkel, I.J.; Howie, C.R. The risk of peri-prosthetic fracture after primary and revision total hip and knee replacement. J. Bone Jt. Surg. Br. 2011, 93, 96–101. [Google Scholar] [CrossRef]
- Kuzyk, P.R.T.; Watts, E.; Backstein, D. Revision Total Knee Arthroplasty for the Management of Periprosthetic Fractures. J. Am. Acad. Orthop. Surg. 2017, 25, 624–633. [Google Scholar] [CrossRef]
- Kamal, A.; Dong, R.J.; Shah, R.; Li, C. Management of periprosthetic fractures of knee arthroplasty with revision surgery. J. Orthop. 2020, 22, 118–123. [Google Scholar] [CrossRef]
- Wallace, S.S.; Bechtold, D.; Sassoon, A. Periprosthetic fractures of the distal femur after total knee arthroplasty: Plate versus nail fixation. Orthop. Traumatol. Surg. Res. 2017, 103, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Yoon, R.S.; Patel, J.N.; Liporace, F.A. Nail and Plate Combination Fixation for Periprosthetic and Interprosthetic Fractures. J. Orthop. Trauma 2019, 33 (Suppl. 6), S18–S20. [Google Scholar] [CrossRef]
- Ebraheim, N.A.; Carroll, T.; Bonaventura, B.; Moral, M.Z.; Jabaly, Y.G.; Liu, J. Challenge of managing distal femur fractures with long-stemmed total knee implants. Orthop. Surg. 2014, 6, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Radke, S.; Radke, J. Total knee arthroplasty in combination with a one-stage tibial osteotomy: A technique for correction of a gonarthrosis with a severe (>15 degrees) tibial extra-articular deformity. J. Arthroplast. 2002, 17, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Grzelecki, D.; Dudek, P.; Kowalczewski, J.; Marczak, D. Złamanie okołoprotezowe dalszego końca kości udowej po całkowitej alloplastyce stawu kolanowego—Opis przypadku. Chir. Narządów Ruchu Ortop. Pol. 2016, 81, 91–95. [Google Scholar]
- Parratte, S.; Ollivier, M.; Argenson, J.N. Primary total knee arthroplasty for acute fracture around the knee. Orthop. Traumatol. Surg. Res. 2018, 104, S71–S80. [Google Scholar] [CrossRef]
- Shin, J.H.; Chang, M.J.; Kang, S.-B.; Chang, C.B.; Kim, D.H.; Lee, S.A.; Mok, S.J. Management and clinical outcomes of periprosthetic fractures after total knee arthroplasty with a stem extension. Medicine 2019, 98, e16088. [Google Scholar] [CrossRef] [PubMed]
- Grzelecki, D.; Szneider, J.; Marczak, D.; Kowalczewski, J. Total knee arthroplasty with simultaneous tibial shaft osteotomy in patient with multiple hereditary osteochondromas and multiaxial limb deformity—A case report. BMC Musculoskelet. Disord. 2020, 21, 233. [Google Scholar] [CrossRef] [Green Version]
- Müller, M.; Koch, P.; Nazarian, S.; Schatzker, J. The Comprehensive Classification of Fractures of Long Bones; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Rorabeck, C.H.; Taylor, J.W. Classification of periprosthetic fractures complicating total knee arthroplasty. Orthop. Clin. N. Am. 1999, 30, 209–214. [Google Scholar] [CrossRef]
- Felix, N.A.; Stuart, M.J.; Hanssen, A.D. Periprosthetic fractures of the tibia associated with total knee arthroplasty. Clin. Orthop. Relat. Res. 1997, 345, 113–124. [Google Scholar] [CrossRef]
- Corrales, L.A.; Morshed, S.; Bhandari, M.; Miclau, T. Variability in the assessment of fracture-healing in orthopaedic trauma studies. J. Bone Jt. Surg. Am. 2008, 90, 1862–1868. [Google Scholar] [CrossRef]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the Knee Society clinical rating system. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar] [CrossRef]
- Boureau, F.; Benad, K.; Putman, S.; Dereudre, G.; Kern, G.; Chantelot, C. Does primary total knee arthroplasty for acute knee joint fracture maintain autonomy in the elderly? A retrospective study of 21 cases. Orthop. Traumatol. Surg. Res. 2015, 101, 947–951. [Google Scholar] [CrossRef] [Green Version]
- Marczak, D.; Synder, M.; Sibiński, M.; Okoń, T.; Kowalczewski, J. One-stage total knee arthroplasty with pre-existing fracture deformity: Post-fracture total knee arthroplasty. J. Arthroplast. 2014, 29, 2104–2108. [Google Scholar] [CrossRef]
- Keeney, J.A. Periprosthetic total knee arthroplasty fractures: Revision arthroplasty technique. J. Knee Surg. 2013, 26, 19–25. [Google Scholar] [CrossRef]
- Pannu, T.S.; Villa, J.M.; Cohen, E.M.; Hayda, R.A.; Higuera, C.A.; Deren, M.E. Periprosthetic Tibial Fractures After Total Knee Arthroplasty: Early and Long-Term Clinical Outcomes. J. Arthroplast. 2021, 36, 1429–1436. [Google Scholar] [CrossRef]
- Bauer, C.; Zaharia, B.; Galliot, F.; Parot, J.; Houfani, F.; Mayer, J.; Mainard, D. Management and results in periprosthetic tibial fracture after total knee arthroplasty: Two-center 15-case retrospective series at 2 years’ follow-up. Orthop. Traumatol. Surg. Res. 2020, 106, 449–458. [Google Scholar] [CrossRef]
- Begue, T.; Tricoire, J.-L.; Veillard, D.; Ingels, A.; Thomazeau, H. Periprosthetic fractures around total hip and knee arthroplasty. Therapeutic algorithm for periprosthetic fractures after total knee arthroplasties. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2006, 92 (Suppl. 5), 2S90–2S96. [Google Scholar]
- Quinzi, D.A.; Childs, S.; Lipof, J.; Soin, S.; Ricciardi, B.F. The Treatment of Periprosthetic Distal Femoral Fractures after Total Knee Replacement: A Critical Analysis Review. JBJS Rev. 2020, 8, e2000003. [Google Scholar] [CrossRef] [PubMed]
- Gausden, E.B.; Lim, P.K.; Rabonivich, A.; Shaath, M.K.; Mitchell, P.M.; Hartline, B.; Achor, T.S.; Warner, S.J. Outcomes of periprosthetic distal femur fractures following total knee arthroplasty: Intramedullary nailing versus plating. Injury 2021, 52, 1875–1879. [Google Scholar] [CrossRef] [PubMed]
- Gondalia, V.; Choi, D.H.; Lee, S.C.; Nam, C.H.; Hwang, B.H.; Ahn, H.S.; Ong, A.C.; Park, H.Y.; Jung, K.A. Periprosthetic supracondylar femoral fractures following total knee arthroplasty: Clinical comparison and related complications of the femur plate system and retrograde-inserted supracondylar nail. J. Orthop. Traumatol. 2014, 15, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darrith, B.; Bohl, D.; Karadsheh, M.S.; Sporer, S.M.; Berger, R.A.; Levine, B.R. Periprosthetic Fractures of the Distal Femur: Is Open Reduction and Internal Fixation or Distal Femoral Replacement Superior? J. Arthroplast. 2020, 35, 1402–1406. [Google Scholar] [CrossRef]
- Tian, Z.-J.; Liu, Y.-J.; Chen, B.-J.; Wang, J.; Niu, C.-L.; Feng, E.-H.; Mai, X.-J.; Huang, Y.-M. Failure of Less-Invasive Stabilization System (LISS) plating for periprosthetic distal femur fractures: Three case reports. Medicine 2020, 99, e19195. [Google Scholar] [CrossRef] [PubMed]
- Bohm, E.R.; Tufescu, T.V.; Marsh, J.P. The operative management of osteoporotic fractures of the knee: To fix or replace? J. Bone Jt. Surg. Br. 2012, 94, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Parratte, S.; Bonnevialle, P.; Pietu, G.; Saragaglia, D.; Cherrier, B.; Lafosse, J. Primary total knee arthroplasty in the management of epiphyseal fracture around the knee. Orthop. Traumatol. Surg. Res. 2011, 97 (Suppl. 6), S87–S94. [Google Scholar] [CrossRef] [Green Version]
- Yoshino, N.; Takai, S.; Watanabe, Y.; Fujiwara, H.; Ohshima, Y.; Hirasawa, Y. Primary total knee arthroplasty for supracondylar/condylar femoral fracture in osteoarthritic knees. J. Arthroplast. 2001, 16, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Marczak, D.; Marczak, D.; Kowalczewski, J.; Czubak, J.; Okoń, T.; Synder, M. Short and mid term results of revision total knee arthroplasty with Global Modular Replacement System. Indian J. Orthop. 2017, 51, 324–329. [Google Scholar]
- Tampere, T.; Ollivier, M.; Jacquet, C.; Fabre-Aubrespy, M.; Parratte, S. Knee arthroplasty for acute fractures around the knee. EFORT Open Rev. 2020, 5, 713–723.37. [Google Scholar] [CrossRef] [PubMed]
- Wui, N.B.; Anuar, M.A.A.; Wahid, A.M.A. Short-Term Outcome of Early Primary Total Knee Arthroplasty for Fractures Around the Knee in the Elderly Population: The Experience of a Secondary Healthcare Centre in Malaysia. Malays. J. Med. Sci. 2020, 27, 64–71. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Periprosthetic Fractures (n = 12) | Fractures with Knee OA (n = 13) | |
|---|---|---|
| Constrained condylar knee(CCK) | ||
| Triathlon TS (Stryker, Mahwah, NJ, USA) | 5 | 7 |
| PFC Sigma TC3 (DePuy Synthes, Raynham, MA, USA) | 1 | 2 |
| Vanguard 360 (Zimmer Biomet, Warsaw, IN, USA) | 1 | - |
| Scorpio TS (Stryker, Mahwah, NJ, USA) | - | 1 |
| Constrained rotating-hinge(RH) | ||
| MRH (Stryker, Mahwah, NJ, USA) | 5 | 3 |
| Periprosthetic Fractures | Fractures with Knee OA | p-Value | |
|---|---|---|---|
| No. | 12 | 13 | - |
| Gender (M/F) | 1/11 | 1/12 | 0.95 * |
| Age (years) | 74.2 (±7.4) | 69.9 (±8.9) | 0.12 ** |
| Prosthesis type | 0.32 * | ||
| semi-constrained (CCK) | 7 | 10 | |
| constrained (RH) | 5 | 3 | |
| Fracture level (shaft) | 0.07 * | ||
| middle 1/3 femur | 2 | 0 | |
| distal 1/3 femur | 5 | 4 | |
| proximal 1/3 tibia | 3 | 9 | |
| middle 1/3 tibia | 2 | 0 | |
| Type of fracture | 0.06 * | ||
| acute fracture | 6 | 2 | |
| pseudarthrosis | 6 | 11 | |
| Bone union rate | 0.61 * | ||
| total | 11 | 11 | |
| partial | 1 | 1 | |
| non-union | 0 | 1 | |
| Hardware in situ before TKA | 0.89 * | ||
| Yes | 4 | 4 | |
| No | 8 | 9 | |
| Concomitant diseases | |||
| Rheumatoid arthritis | 2 | 1 | 0.59 * |
| Diabetes | 1 | 2 | 0.59 * |
| Stem length (above or below the fracture level) (mm) | |||
| Femur | 109.3 (±31.1) | 123.7 (±55.2) | 0.6 ** |
| Tibia | 124.6 (±24.2) | 125.5 (±22.9) | 0.94 ** |
| Stem diameter (% of filling the medullary canal in the narrowest point) | |||
| Femur | 95.5 (±4.4) | 85 (±14.4) | 0.1 ** |
| Tibia | 93.7 (±10.1) | 90 (±8.4) | 0.46 ** |
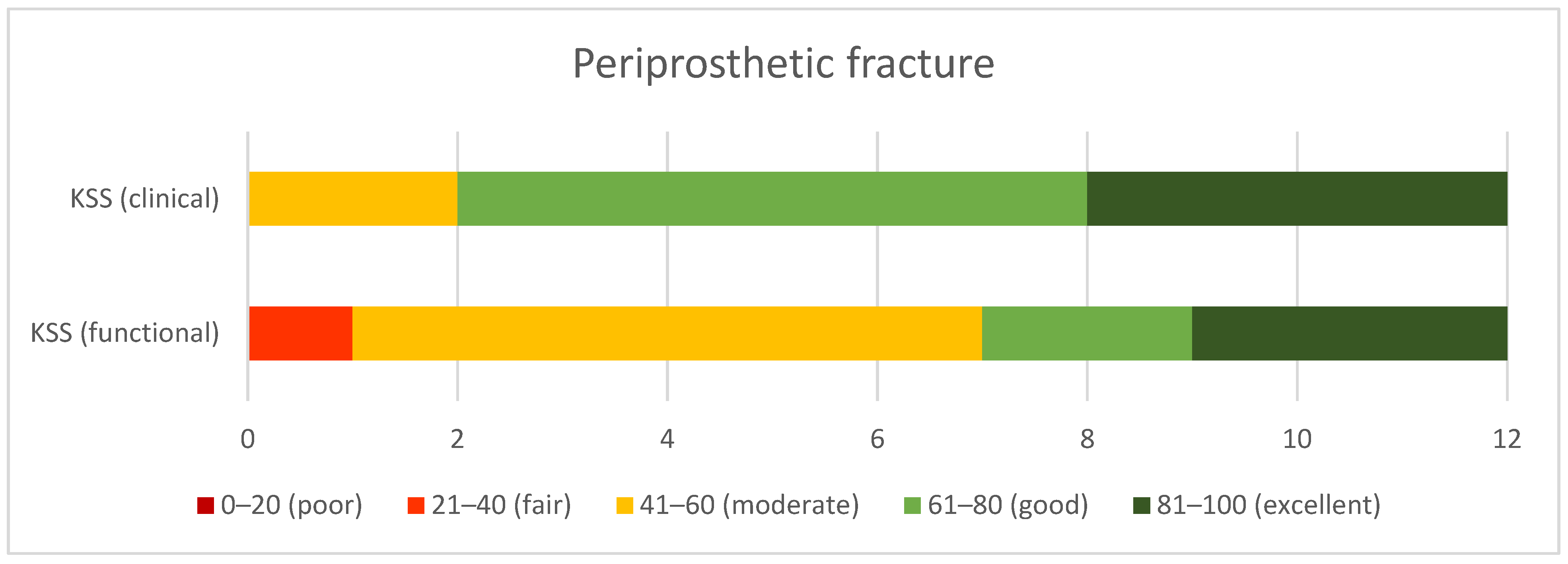
| KSS (clinical) | 73.1 (±13.3) | 84.1 (±11) | 0.03 ** |
| KSS (functional) | 59.2 (±18.8) | 76.2 (±20.6) | 0.04 ** |
| ROM (mean, range) | |||
| Extension | 0° | 0.77° (±2.8°) From 0° to −10° | 0.35 ** |
| Flexion | 96.7° (±26°) From 25° to 120° | 93.6° (±26.3°) From 30° to 120° | 0.85 ** |
| Complications | |||
| Surgical site infection | 2 | 1 | 0.59 * |
| Arthrofibrosis | 1 | 1 | 0.95 * |
| Delayed union | 1 | 2 | 0.59 * |
| Non-union | 1 | 0 | 0.33 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grzelecki, D.; Marczak, D.; Kwolek, K.; Dudek, P.; Tyrakowski, M.; Olewnik, Ł.; Czubak-Wrzosek, M.; Kowalczewski, J. Shaft Fractures in Patients Requiring Primary or Revision Total Knee Arthroplasty Can Be Successfully Treated with Long-Stemmed Implants without Additional Fixation. J. Clin. Med. 2021, 10, 4926. https://doi.org/10.3390/jcm10214926
Grzelecki D, Marczak D, Kwolek K, Dudek P, Tyrakowski M, Olewnik Ł, Czubak-Wrzosek M, Kowalczewski J. Shaft Fractures in Patients Requiring Primary or Revision Total Knee Arthroplasty Can Be Successfully Treated with Long-Stemmed Implants without Additional Fixation. Journal of Clinical Medicine. 2021; 10(21):4926. https://doi.org/10.3390/jcm10214926
Chicago/Turabian StyleGrzelecki, Dariusz, Dariusz Marczak, Kamil Kwolek, Piotr Dudek, Marcin Tyrakowski, Łukasz Olewnik, Maria Czubak-Wrzosek, and Jacek Kowalczewski. 2021. "Shaft Fractures in Patients Requiring Primary or Revision Total Knee Arthroplasty Can Be Successfully Treated with Long-Stemmed Implants without Additional Fixation" Journal of Clinical Medicine 10, no. 21: 4926. https://doi.org/10.3390/jcm10214926