The Effect of Diabetes Mellitus on the Recurrence of Atrial Fibrillation after Ablation

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Periprocedural Management
2.2. Ablation Procedure
2.3. Follow-Up
2.4. Endpoint
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
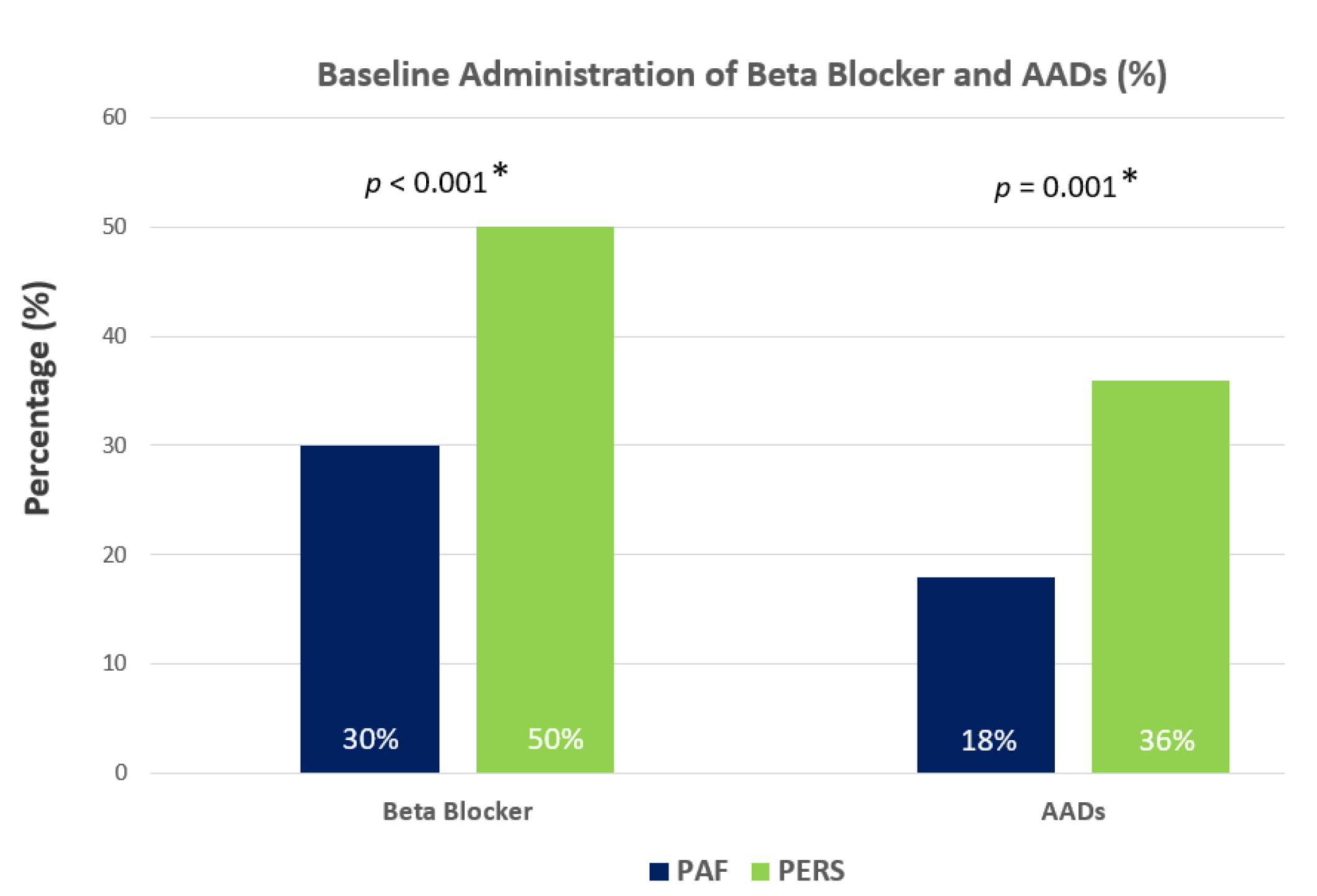
3.2. Baseline Characteristics in PAF and PERS
3.3. Impact of DM on PAF and PERS
3.4. Procedural Data
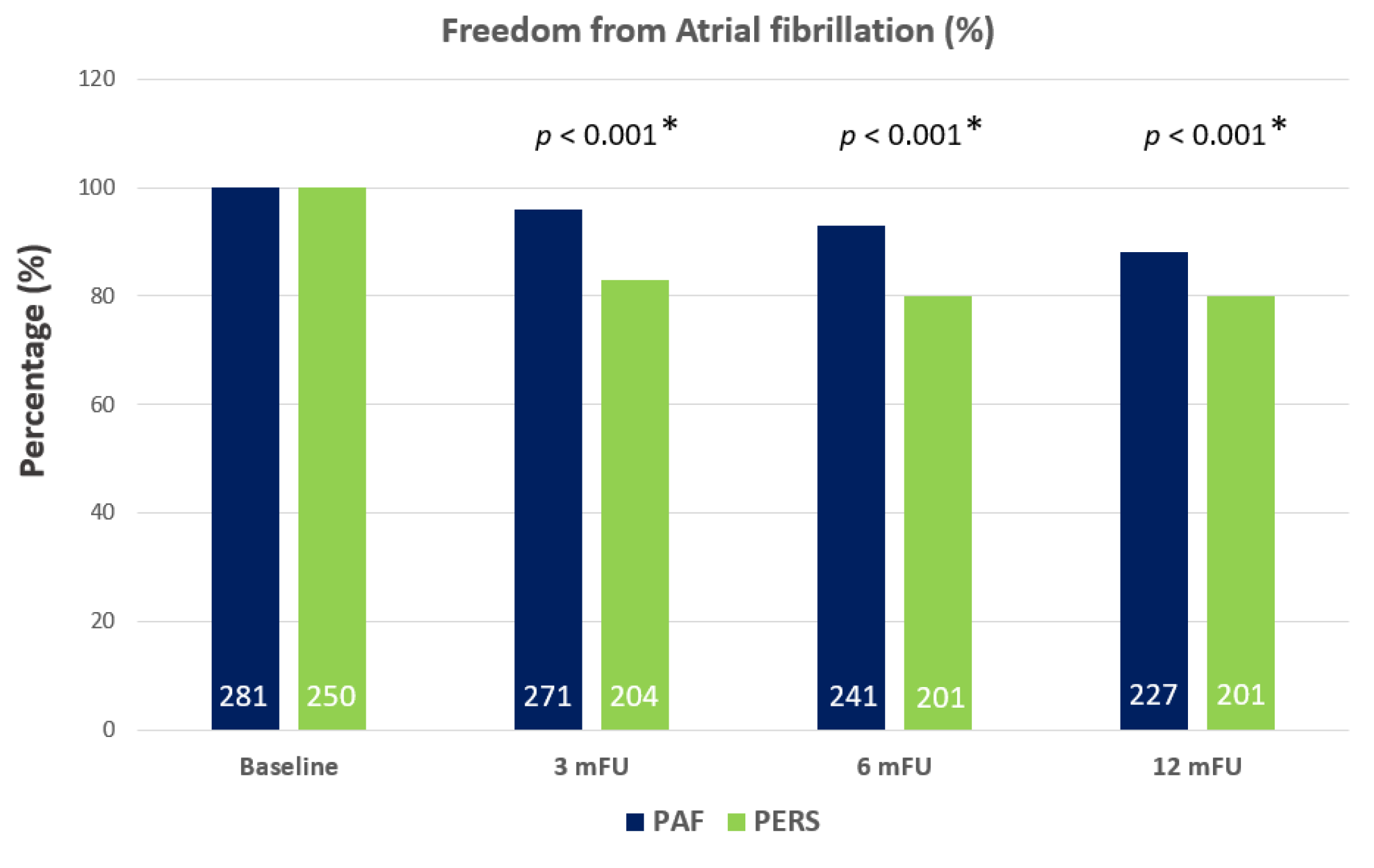
3.5. Clinical Outcome
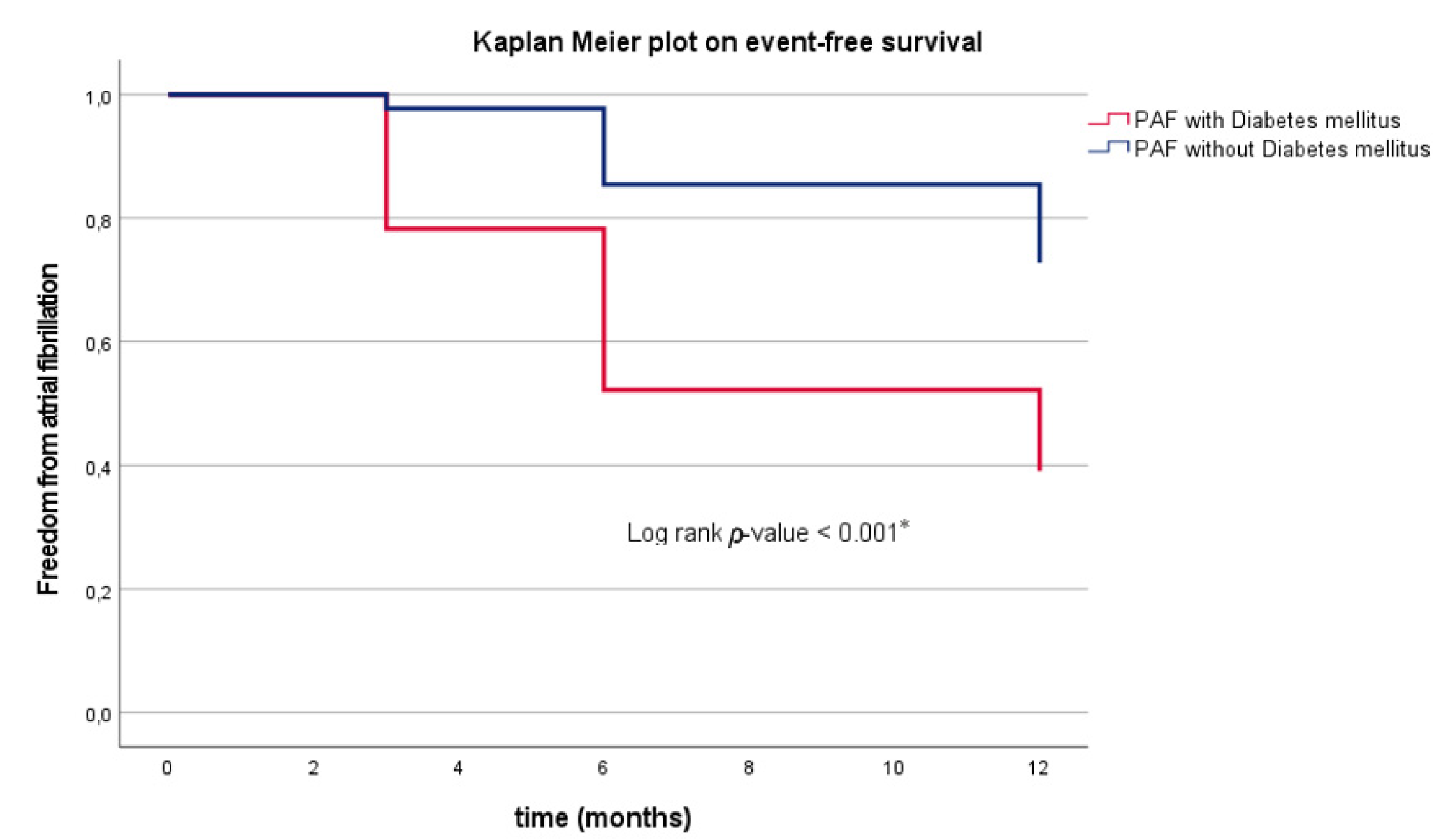
3.6. Clinical Outcome in PAF Depending on DM
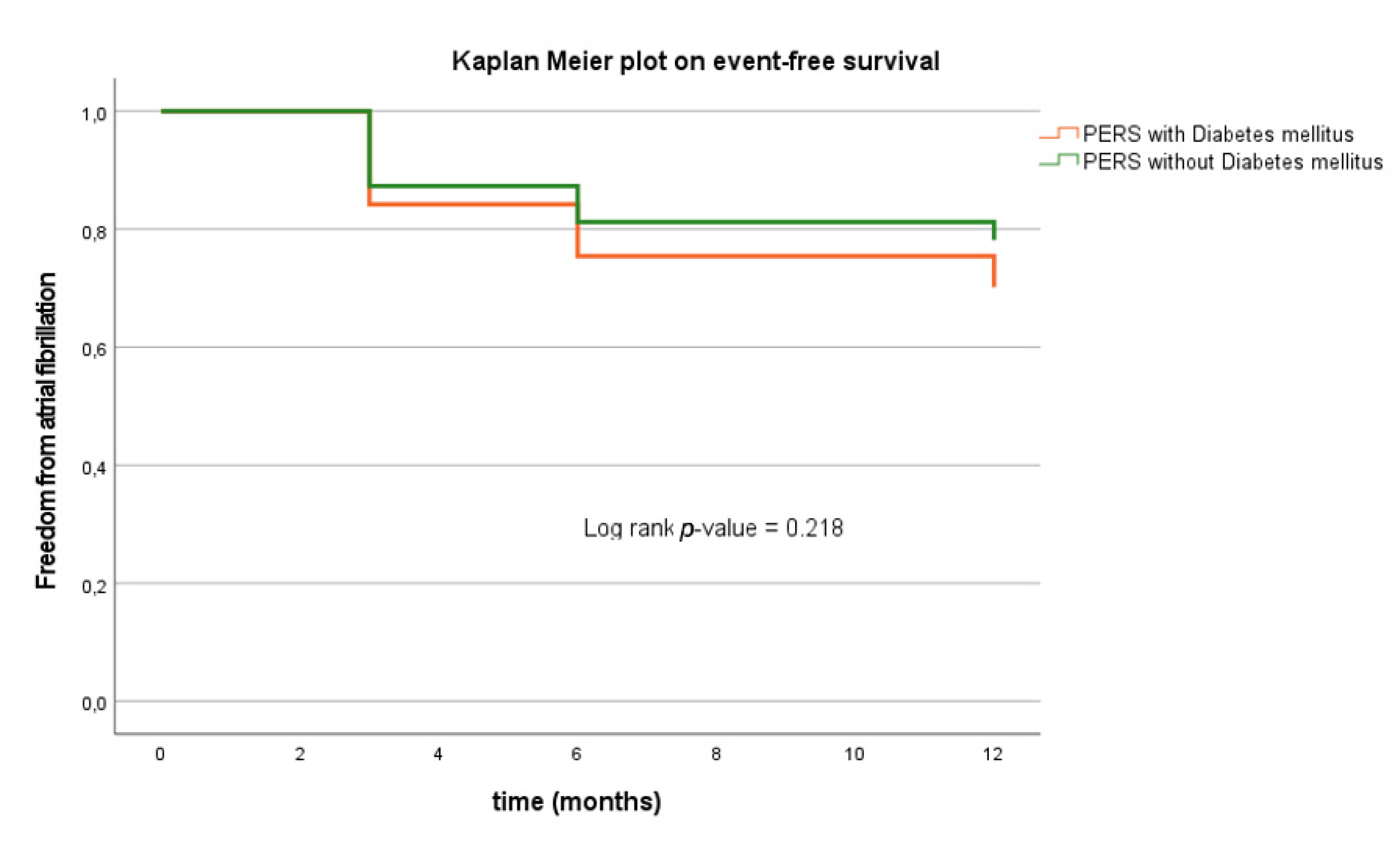
3.7. Clinical Outcome in PERS Depending on DM
3.8. Impact of DM and Other Parameters on AF Recurrence
3.9. Impact of Baseline Parameters on AF Recurrence in DM Patients
4. Complications
5. Discussion
5.1. Main Findings
5.2. Impact of DM on Arrhythmia Recurrence
5.3. Additional Predictors of AF Recurrence
5.3.1. Baseline Characteristics
5.3.2. B-Blocker and Antiarrhythmic Agents
5.3.3. Metabolic Parameters
5.3.4. Gender Disparities and the Autonomic Nervous System
5.3.5. Predictive Value of Baseline Parameters on AF Recurrence in DM Patients
5.4. Clinical Perspective and Translational Outlook
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R. Heart Disease and Stroke Statistics—2019 Update: A Report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Costard-Jäckle, A.; Tschope, D.; Meinertz, T. Cardiovascular outcome in type 2 diabetes and atrial fibrillation. Herz 2018, 44, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Stegmann, C.; Jahnke, C.; Paetsch, I.; Hilbert, S.; Arya, A.; Bollmann, A.; Hindricks, G.; Sommer, P. Association of left ventricular late gadolinium en-hancement with left atrial low voltage areas in patients with atrial fibrillation. Europace 2018, 20, 1606–1611. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Ninomiya, T.; de Galan, B.; Abadir, E.; Chalmers, J.; Pillai, A.; Woodward, M.; Cooper, M.; Harrap, S.; Hamet, P.; et al. Risks of cardiovascular events and effects of routine blood pressure lowering among patients with type 2 diabetes and atrial fibrillation: Results of the ADVANCE study. Eur. Heart J. 2009, 30, 1128–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chao, T.-F.; Suenari, K.; Chang, S.-L.; Lin, Y.-J.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; Tai, C.-T.; Tsao, H.-M.; Li, C.-H.; et al. Atrial Substrate Properties and Outcome of Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation Associated with Diabetes Mellitus or Impaired Fasting Glucose. Am. J. Cardiol. 2010, 106, 1615–1620. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Green, J.B.; Halperin, J.L.; Piccini, J.P., Sr. Atrial Fibrillation and Diabetes Mellitus: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Kowallick, J.T.; Staab, W.; Schuster, A.; Backhaus, S.J.; Weber-Krüger, M.; Bauer, L.; Sohns, C.; Lotz, J.; Hasenfuß, G.; Lüthje, L.; et al. Reverse left ventricular structural remodeling after catheter ablation of atrial fibrillation in patients with preserved left ventricular function: Insights from cardio-vascular magnetic resonance native T1 mapping. Heart Rhythm 2019, 16, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Sohns, C.; Marrouche, N.F. Atrial fibrillation and cardiac fibrosis. Eur. Heart J. 2019, 41, 1123–1131. [Google Scholar] [CrossRef]
- Ostgren, C.J.; Merlo, J.; Rastam, L.; Lindblad, U. Atrial fibrillation and its association with type 2 diabetes and hypertension in a Swedish community. Diabetes Obes. Metab. 2004, 6, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Chan, Y.-H.; Chang, G.-J.; Lai, Y.-J.; Chen, W.-J.; Chang, S.-H.; Hung, L.-M.; Kuo, C.-T.; Yeh, Y.-H. Atrial fibrillation and its arrhythmogenesis associated with insulin resistance. Cardiovasc. Diabetol. 2019, 18, 125. [Google Scholar] [CrossRef] [Green Version]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef]
- Akoum, N.; Wilber, D.; Hindricks, G.; Jais, P.; Cates, J.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. MRI Assessment of Ablation-Induced Scarring in Atrial Fibrillation: Analysis from the DECAAF Study. J. Cardiovasc. Electrophysiol. 2015, 26, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Teh, A.W.; Kistler, P.; Lee, G.; Medi, C.; Heck, P.M.; Spence, S.J.; Sparks, P.B.; Morton, J.B.; Kalman, J.M. Electroanatomic Remodeling of the Left Atrium in Paroxysmal and Persistent Atrial Fibrillation Patients Without Structural Heart Disease. J. Cardiovasc. Electrophysiol. 2011, 23, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; Van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Omran, H.; Gutleben, K.-J.; Molatta, S.; Fischbach, T.; Wellmann, B.; Horstkotte, D.; Körber, B.; Nölker, G. Second generation cryoballoon ablation for persistent atrial fibrillation: An updated meta-analysis. Clin. Res. Cardiol. 2017, 107, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Guckel, D.; Schmidt, A.; Gutleben, K.J.; Körber, B.; Fischbach, T.; Horstkotte, D.; Nölker, G. Pulmonary vein isolation and be-yond: Predictive value of vagal reactions in second-generation cryoballoon ablation for the outcome of persistent atrial fibrillation. Heart Rhythm 2020, 17, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.-H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018, 20, e1–e160. [Google Scholar] [CrossRef] [PubMed]
- Roney, C.; Williams, S.E.; Cochet, H.; Mukherjee, R.K.; O’Neill, L.; Sim, I.; Whitaker, J.; Razeghi, O.; Klein, G.J.; Vigmond, E.J.; et al. Patient-specific simulations predict efficacy of ablation of interatrial connections for treatment of persistent atrial fibrillation. Europace 2018, 20, iii55–iii68. [Google Scholar] [CrossRef] [PubMed]
- Quadri, R.; Maule, S.; Chiandussi, L.; Fonzo, D. Diabete, obesità, ipertensione e sistema nervoso vegetativo [Diabetes, obesity, hypertension and the autonomic nervous system]. Minerva Endocrinol. 1994, 19, 105–111. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PAF (n = 258) | PERS (n = 193) | p-Value |
|---|---|---|---|
| Age (years) | 51.0 ± 23.2 | 65.0 ± 10.0 | <0.01 * |
| Gender, female | 66 (26%) | 57 (30%) | 0.02 * |
| BMI (kg/m2) | 26.8 ± 3.8 | 29.0 ± 5.3 | <0.01 * |
| LVEF (%) | 54.1 ± 4.4 | 54.3 ± 2.8 | 0.06 |
| LA diameter (mm) | 38.2 ± 6.5 | 43.6 ± 8.5 | <0.01 * |
| CMP | 22 (9%) | 21 (11%) | 0.06 |
| CAD | 14 (4%) | 11 (6%) | 0.09 |
| Hypertensive CMP | 8 (3%) | 7 (4%) | 0.11 |
| H(O)CM | 0 (0%) | 2 (1%) | 0.40 |
| Valvular CMP | 0 (0%) | 1 (1%) | 0.64 |
| Hypertension | 98 (38%) | 122 (63%) | <0.01 * |
| Smoking | 26 (10%) | 38 (20%) | <0.01 * |
| Beta blocker BL | 86 (30%) | 124 (50%) | <0.01 * |
| AADs BL | 51 (18%) | 89 (36%) | <0.01 * |
| Characteristics | DM (n = 23) | No DM (n = 258) | p-Value |
|---|---|---|---|
| Age (years) | 58.1 ± 28.3 | 50.8 ± 22.9 | 0.03 * |
| Gender, female | 7 (30%) | 66 (26%) | 0.01 * |
| BMI (kg/m2) | 30.0 ± 5.1 | 27.0 ± 3.8 | <0.01 * |
| LVEF (%) | 52.1 ± 5.7 | 54.1 ± 4.4 | 0.13 |
| LA diameter (mm) | 40.2 ± 7.7 | 38.2 ± 6.5 | 0.07 |
| CMP | 2 (9%) | 22 (9%) | 0.25 |
| CAD | 2 (9%) | 14 (4%) | 0.26 |
| Hypertensive CMP | 0 (0%) | 8 (3%) | 0.44 |
| H(O)CM | 0 (0%) | 0 (0%) | 1.00 |
| Valvular CMP | 0 (0%) | 0 (0%) | 1.00 |
| Hypertension | 19 (83%) | 98 (38%) | <0.01 * |
| Smoking | 8 (35%) | 26 (10%) | <0.01 * |
| Beta blocker BL | 4 (17%) | 82 (32%) | <0.01 * |
| AADs BL | 5 (22%) | 46 (18%) | 0.02 * |
| HbA1c (%) | 6.2 ± 0.4 | 5.7 ± 0.7 | 0.01 * |
| Cholesterol (mg/dL) | 179.3 ± 36.0 | 207.4 ± 40.9 | 0.06 |
| Triglyceride (mg/dL) | 187.25 ± 77.8 | 148.7 ± 94.8 | 0.21 |
| LDL (mg/dL) | 114.5 ± 18.5 | 127.6 ± 34.1 | 0.15 |
| HDL (mg/dL) | 60.0 ± 37.8 | 53.4 ± 28.7 | 0.64 |
| CRP (mg/dL) | 0.6 ± 0.8 | 0.5 ± 0.9 | 0.59 |
| Characteristics | DM (n = 57) | No DM (n = 193) | p-Value |
|---|---|---|---|
| Age (years) | 70.4 ± 9.9 | 65.3 ± 9.8 | <0.01 * |
| Gender, female | 18 (32%) | 57 (30%) | 0.09 |
| BMI (kg/m2) | 30.7 ± 4.7 | 28.9 ± 5.3 | 0.03 * |
| LVEF (%) | 53.2 ± 3.6 | 54.3 ± 2.8 | 0.04 * |
| LA diameter (mm) | 44.3 ± 4.5 | 43.7 ± 8.5 | 0.43 |
| CMP | 15 (26%) | 4 (11%) | <0.01 * |
| CAD | 9 (16%) | 11 (6%) | 0.03 * |
| Hypertensive CMP | 6 (11%) | 7 (4%) | 0.05 * |
| H(O)CM | 0 (0%) | 2 (1%) | 0.66 |
| Valvular CMP | 0 (0%) | 1 (1%) | 0.81 |
| Hypertension | 49 (86%) | 122 (63%) | <0.01 * |
| Smoking | 17 (30%) | 38 (20%) | 0.05 * |
| Beta blocker BL | 46 (82%) | 146 (76%) | 0.07 |
| AADs BL | 23 (40%) | 66 (34%) | 0.04 * |
| HbA1c (mg/dL) | 6.7 ± 1.2 | 5.5 ± 0.3 | <0.01 * |
| Cholesterol (mg/dL) | 179.4 ± 44.8 | 208.2 ± 44.5 | 0.05 * |
| Triglyceride (mg/dL) | 181.08 ± 91.8 | 150.9 ± 85.9 | <0.01 * |
| LDL (mg/dL) | 105.6 ± 36.4 | 130.1 ± 35.9 | <0.01 * |
| HDL (mg/dL) | 47.6 ± 21.1 | 52.2 ± 16.4 | <0.01 * |
| CRP (mg/dL) | 0.6 ± 0.8 | 0.5 ± 0.9 | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guckel, D.; Isgandarova, K.; Bergau, L.; Piran, M.; El Hamriti, M.; Imnadze, G.; Braun, M.; Khalaph, M.; Fink, T.; Sciacca, V.; et al. The Effect of Diabetes Mellitus on the Recurrence of Atrial Fibrillation after Ablation. J. Clin. Med. 2021, 10, 4863. https://doi.org/10.3390/jcm10214863
Guckel D, Isgandarova K, Bergau L, Piran M, El Hamriti M, Imnadze G, Braun M, Khalaph M, Fink T, Sciacca V, et al. The Effect of Diabetes Mellitus on the Recurrence of Atrial Fibrillation after Ablation. Journal of Clinical Medicine. 2021; 10(21):4863. https://doi.org/10.3390/jcm10214863
Chicago/Turabian StyleGuckel, Denise, Khuraman Isgandarova, Leonard Bergau, Misagh Piran, Mustapha El Hamriti, Guram Imnadze, Martin Braun, Moneeb Khalaph, Thomas Fink, Vanessa Sciacca, and et al. 2021. "The Effect of Diabetes Mellitus on the Recurrence of Atrial Fibrillation after Ablation" Journal of Clinical Medicine 10, no. 21: 4863. https://doi.org/10.3390/jcm10214863