
Lack of Association between Serum Interleukin-23 and Interleukin-27 Levels and Disease Activity in Patients with Active Systemic Lupus Erythematosus


Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnostic Criteria
2.2. Methodology
- Demographic data (age, sex);
- Medical history/clinical data;
- Current treatment;
- Measurements (morphology, biochemistry, urinalysis, daily proteinuria);
- Disease activity measured with the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI 2-K) [35,36], Physician Global Assessment (PGA) [37], and organ damage determined using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index (SDI) [38].
2.3. Immunoassays
2.4. Statistics
2.5. Ethics
3. Results
3.1. Patient Characteristics
3.2. Disease Activity and Laboratory Test Results
3.3. Determinants of Disease Activity and Different Disease Manifestations
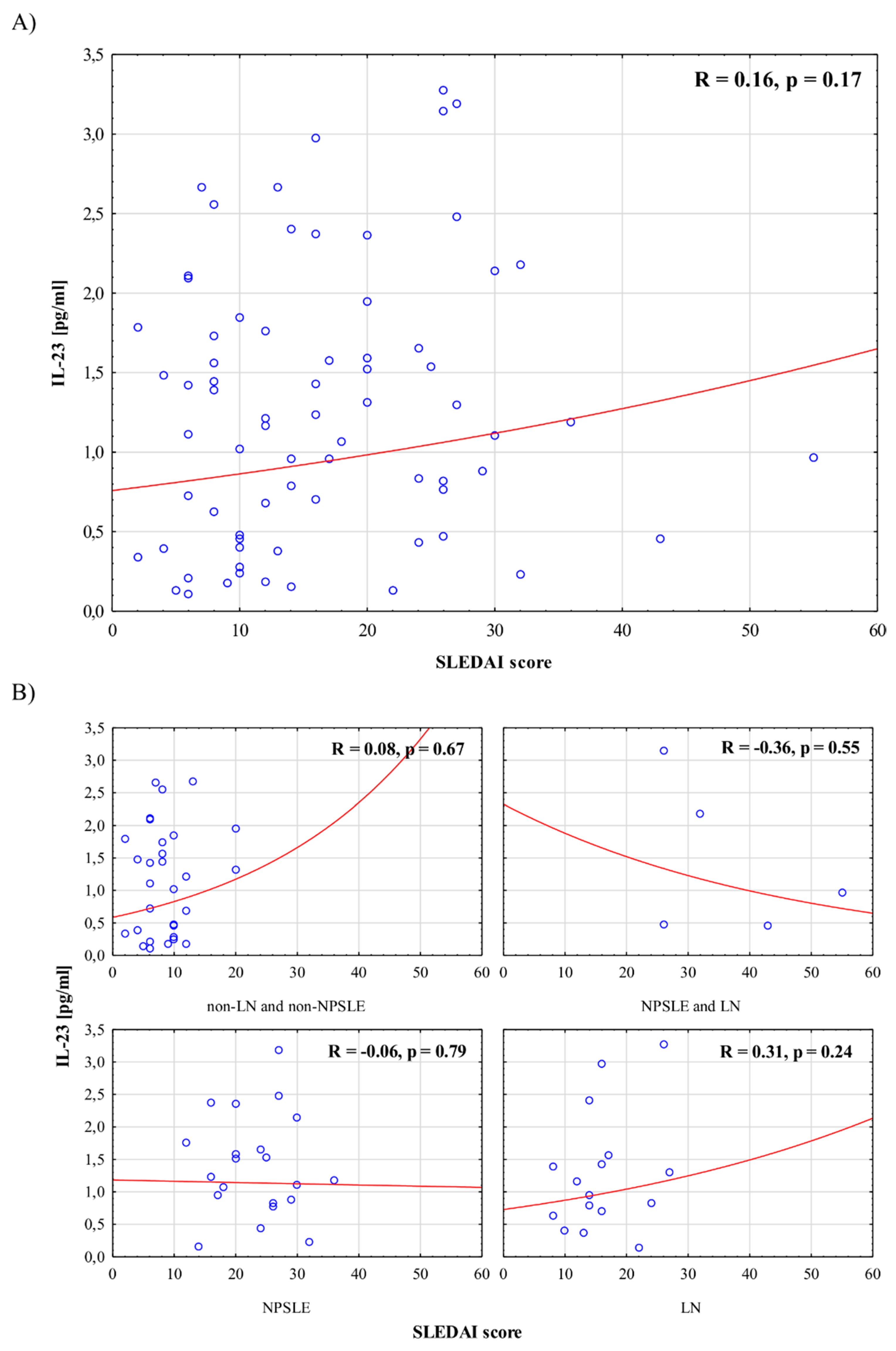
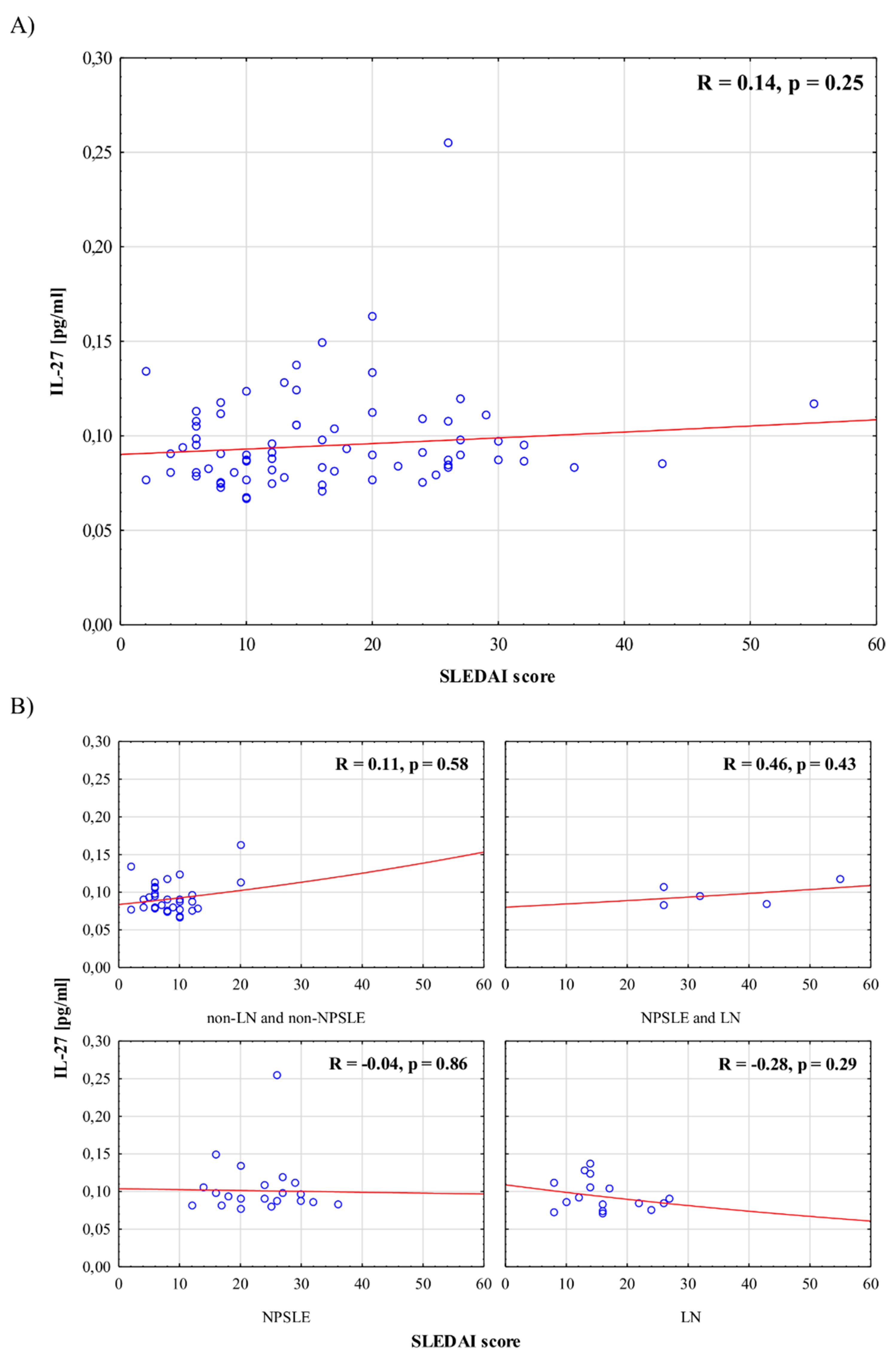
3.4. Association between IL-23/IL-27 Levels and Disease Activity
3.5. Associatiosn between IL-23 Levels, IL-27 Levels, dsDNA, and Complement C3/C4 Components
3.6. Association between IL-23/IL-27 Levels and SLE Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bertsias, G.K.; Pamfil, C.; Fanouriakis, A.; Boumpas, D.T. Diagnostic criteria for systemic lupus erythematosus: Has the time come? Nat. Rev. Rheumatol. 2013, 9, 687–694. [Google Scholar] [CrossRef]
- Tsokos, G.C. Systemic lupus erythematosus. N. Engl. J. Med. 2011, 365, 2110–2121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaul, A.; Gordon, C.; Crow, M.K.; Touma, Z.; Urowitz, M.B.; van Vollenhoven, R.; Ruiz-Irastorza, G.; Hughes, G. Systemic lupus erythematosus. Nat. Rev. Dis. Primers 2016, 2, 16039. [Google Scholar] [CrossRef] [PubMed]
- Furst, D.E.; Clarke, A.; Fernandes, A.W.; Bancroft, T.; Gajria, K.; Greth, W.; Iorga, Ş.R. Medical costs and healthcare resource use in patients with lupus nephritis and neuropsychiatric lupus in an insured population. J. Med. Econ. 2013, 16, 500–509. [Google Scholar] [CrossRef]
- Parikh, S.V.; Almaani, S.; Brodsky, S.; Rovin, B.H. Update on Lupus Nephritis: Core Curriculum 2020. Am. J. Kidney Dis. 2020, 76, 265–281. [Google Scholar] [CrossRef] [PubMed]
- Carrión-Barberà, I.; Salman-Monte, T.C.; Vílchez-Oya, F.; Monfort, J. Neuropsychiatric involvement in systemic lupus erythematosus: A review. Autoimmun. Rev. 2021, 20, 102780. [Google Scholar] [CrossRef]
- Jeltsch-David, H.; Muller, S. Neuropsychiatric systemic lupus erythematosus: Pathogenesis and biomarkers. Nat. Rev. Neurol. 2014, 10, 579–596. [Google Scholar] [CrossRef]
- Śliwczyński, A.; Brzozowska, M.; Iltchev, P.; Czeleko, T.; Teter, Z.; Tłustochowicz, W.; Marczak, M.; Tłustochowicz, M. Changes in the morbidity and costs of systemic lupus erythematosus in Poland in the years 2008–2012. Reumatologia 2015, 53, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Lourenço, E.V.; La Cava, A. Cytokines in systemic lupus erythematosus. Curr. Mol. Med. 2009, 9, 242–254. [Google Scholar] [CrossRef] [Green Version]
- Yap, D.Y.; Lai, K.N. Cytokines and their roles in the pathogenesis of systemic lupus erythematosus: From basics to recent advances. J. Biomed. Biotechnol. 2010, 2010, 365083. [Google Scholar] [CrossRef] [Green Version]
- Mikita, N.; Ikeda, T.; Ishiguro, M.; Furukawa, F. Recent advances in cytokines in cutaneous and systemic lupus erythematosus. J. Dermatol. 2011, 38, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Moulton, V.R.; Suárez-Fueyo, A.; Meidan, E.; Li, H.; Mizui, M.; Tsokos, G.C. Pathogenesis of Human Systemic Lupus Erythematosus: A Cellular Perspective. Trends Mol. Med. 2017, 23, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Su, L.; Liu, X.; Wang, J.; Yuan, Z.; Qin, Z.; Zhou, X.; Huang, A. IL-38: A novel cytokine in systemic lupus erythematosus pathogenesis. J. Cell. Mol. Med. 2020, 24, 12379–12389. [Google Scholar] [CrossRef] [PubMed]
- Muhammad Yusoff, F.; Wong, K.K.; Mohd Redzwan, N. Th1, Th2, and Th17 cytokines in systemic lupus erythematosus. Autoimmunity 2020, 53, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Puwipirom, H.; Hirankarn, N.; Sodsai, P.; Avihingsanon, Y.; Wongpiyabovorn, J.; Palaga, T. Increased interleukin-23 receptor+ T cells in peripheral blood mononuclear cells of patients with systemic lupus erythematosus. Arthritis Res. Ther. 2010, 12, R215. [Google Scholar] [CrossRef] [Green Version]
- Curtis, M.M.; Way, S.S.; Wilson, C.B. IL-23 promotes the production of IL-17 by antigen-specific CD8 T cells in the absence of IL-12 and type-I interferons. J. Immunol. 2009, 183, 381–387. [Google Scholar] [CrossRef]
- Sutton, C.E.; Lalor, S.J.; Sweeney, C.M.; Brereton, C.F.; Lavelle, E.C.; Mills, K.H. Interleukin-1 and IL-23 induce innate IL-17 production from gammadelta T cells, amplifying Th17 responses and autoimmunity. Immunity 2009, 31, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Doodes, P.D.; Glant, T.T.; Finnegan, A. IL-27 induces a Th1 immune response and susceptibility to experimental arthritis. J. Immunol. 2008, 180, 922–930. [Google Scholar] [CrossRef]
- Su, Y.; Yao, H.; Wang, H.; Xu, F.; Li, D.; Li, D.; Zhang, X.; Yin, Y.; Cao, J. IL-27 enhances innate immunity of human pulmonary fibroblasts and epithelial cells through upregulation of TLR4 expression. Am. J. Physiol. Lung Cell. Mol. Physiol. 2016, 310, L133–L141. [Google Scholar] [CrossRef] [Green Version]
- Li, T.-T.; Zhang, T.; Chen, G.-M.; Zhu, Q.-Q.; Tao, J.-H.; Pan, H.-F.; Ye, D.-Q. Low level of serum interleukin 27 in patients with systemic lupus erythematosus. J. Investig. Med. 2010, 58, 737–739. [Google Scholar] [CrossRef]
- Lee, M.H.; Gallo, P.M.; Hooper, K.M.; Corradetti, C.; Ganea, D.; Caricchio, R.; Gallucci, S. The cytokine network Type I Interferon, IL-27 and IL-10 is augmented in murine and human lupus. J. Leukoc. Biol. 2019, 106, 967–975. [Google Scholar] [CrossRef]
- Leng, R.-X.; Pan, H.-F.; Chen, G.-M.; Wang, C.; Qin, W.-Z.; Chen, L.-L.; Tao, J.-H.; Ye, D.-Q. IL-23: A Promising Therapeutic Target for Systemic Lupus Erythematosus. Arch. Med. Res. 2010, 41, 221–225. [Google Scholar] [CrossRef]
- Gaber, W.; Sayed, S.; Rady, H.M.; Mohey, A.M. Interleukin-27 and its relation to disease parameters in SLE patients. Egypt. Rheumatol. 2012, 34, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Hegab, D.S.; Saudi, W.M.; Ammo, D.E.A.; El Bedewy, M.M.; Elhabian, N.F.; Gamei, M.M. Role of interleukin-23 in the immunopathogenesis of systemic lupus erythematosus. Egypt. J. Dermatol. Venerol. 2014, 34, 120. [Google Scholar] [CrossRef]
- Du, J.; Li, Z.; Shi, J.; Bi, L. Associations between serum interleukin-23 levels and clinical characteristics in patients with systemic lupus erythematosus. J. Int. Med. Res. 2014, 42, 1123–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, L.P.; Li, B.F.; Shen, H.; Lu, J. Interleukin-27 and interleukin-23 in patients with systemic lupus erythematosus: Possible role in lupus nephritis. Scand. J. Rheumatol. 2015, 44, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Przepiera-Bedzak, H.; Sawicki, M.; Walecka, A.; Brzosko, I.; Brzosko, M. Serum Interleukin-23 in Polish Patients with Systemic Lupus Erythematosus: Association with Lupus Nephritis, Obesity, and Peripheral Vascular Disease. Mediat. Inflamm. 2017, 2017, 9401432. [Google Scholar] [CrossRef]
- Vukelic, M.; Laloo, A.; Kyttaris, V.C. Interleukin 23 is elevated in the serum of patients with SLE. Lupus 2020, 29, 1943–1947. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 EULAR/ACR classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef] [Green Version]
- Leuchten, N.; Hoyer, A.; Brinks, R.; Schoels, M.; Schneider, M.; Smolen, J.; Johnson, S.R.; Daikh, D.; Dörner, T.; Aringer, M.; et al. Performance of Antinuclear Antibodies for Classifying Systemic Lupus Erythematosus: A Systematic Literature Review and Meta-Regression of Diagnostic Data. Arthritis Rheum. 2018, 70, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Fox, B.J.; Hockley, J.; Rigsby, P.; Dolman, C.; Meroni, P.L.; Rönnelid, J. A WHO Reference Reagent for lupus (anti-dsDNA) antibodies: International collaborative study to evaluate a candidate preparation. Ann. Rheum. Dis. 2019, 78, 1677–1680. [Google Scholar] [CrossRef] [Green Version]
- Liang, M.H.; Corzillius, M.; Bae, S.C.; Lew, R.A.; Fortin, P.R.; Gordon, C.; Isenberg, D.; Alarcón, G.S.; Straaton, K.V.; Denburg, J.; et al. The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. 1999, 42, 599–608. [Google Scholar]
- Rekvig, O.P. Anti-dsDNA antibodies as a classification criterion and a diagnostic marker for systemic lupus erythematosus: Critical remarks. Clin. Exp. Immunol. 2015, 179, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar]
- Mikdashi, J.; Nived, O. Measuring disease activity in adults with systemic lupus erythematosus: The challenges of administrative burden and responsiveness to patient concerns in clinical research. Arthritis Res. Ther. 2015, 17, 183. [Google Scholar] [CrossRef] [Green Version]
- Chessa, E.; Piga, M.; Floris, A.; Devilliers, H.; Cauli, A.; Arnaud, L. Use of Physician Global Assessment in systemic lupus erythematosus: A systematic review of its psychometric properties. Rheumatology 2020, 59, 3622–3632. [Google Scholar] [CrossRef]
- Gladman, D.D.; Urowitz, M.B. The SLICC/ACR damage index: Progress report and experience in the field. Lupus 1999, 8, 632–637. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Kyttaris, V.C.; Tsokos, G.C. The role of IL-23/IL-17 axis in lupus nephritis. J. Immunol. 2009, 183, 3160–3169. [Google Scholar] [CrossRef] [PubMed]
- Argollo, M.C.; Allocca, M.; Furfaro, F.; Peyrin-Biroulet, L.; Danese, S. Interleukin-23 Blockers: Born to be First-line Biologic Agents in Inflammatory Bowel Disease? Curr. Pharm. Des. 2019, 25, 25–31. [Google Scholar] [CrossRef]
- Chen, Y.; Langrish, C.L.; McKenzie, B.; Joyce-Shaikh, B.; Stumhofer, J.S.; McClanahan, T.; Blumenschein, W.; Churakovsa, T.; Low, J.; Presta, L. Anti–IL-23 therapy inhibits multiple inflammatory pathways and ameliorates autoimmune encephalomyelitis. J. Clin. Investig. 2006, 116, 1317–1326. [Google Scholar] [CrossRef] [Green Version]
- Kyttaris, V.C.; Kampagianni, O.; Tsokos, G.C. Treatment with anti-interleukin 23 antibody ameliorates disease in lupus-prone mice. BioMed Res. Int. 2013, 2013, 861028. [Google Scholar] [CrossRef]
- Janssen Announces Discontinuation of Phase 3 LOTUS Study Evaluating Ustekinumab in Systemic Lupus Erythematosus. Available online: https://www.janssen.com/janssen-announces-discontinuation-phase-3-lotus-study-evaluating-ustekinumab-systemic-lupus (accessed on 12 October 2021).
- Sbidian, E.; Chaimani, A.; Garcia-Doval, I.; Do, G.; Hua, C.; Mazaud, C.; Droitcourt, C.; Hughes, C.; Ingram, J.R.; Naldi, L.; et al. Systemic pharmacological treatments for chronic plaque psoriasis: A network meta-analysis. Cochrane Database Syst. Rev. 2017, 12, CD011535. [Google Scholar] [CrossRef]
- Youn, S.W.; Tsai, T.-F.; Theng, C.; Choon, S.-E.; Wiryadi, B.E.; Pires, A.; Tan, W.; Lee, M.-G.; MARCOPOLO Investigators. The MARCOPOLO Study of Ustekinumab Utilization and Efficacy in a Real-World Setting: Treatment of Patients with Plaque Psoriasis in Asia-Pacific Countries. Ann. Dermatol. 2016, 28, 222–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biemans, V.B.C.; Van Der Woude, C.J.; Dijkstra, G.; Jong, A.E.V.D.M.-D.; Löwenberg, M.; de Boer, N.; Oldenburg, B.; Srivastava, N.; Jansen, J.M.; Bodelier, A.G.L.; et al. Ustekinumab is associated with superior effectiveness outcomes compared to vedolizumab in Crohn’s disease patients with prior failure to anti-TNF treatment. Aliment. Pharmacol. Ther. 2020, 52, 123–134. [Google Scholar] [CrossRef]
- Blauvelt, A.; Leonardi, C.L.; Gooderham, M.; Papp, K.A.; Philipp, S.; Wu, J.J.; Igarashi, A.; Flack, M.; Geng, Z.; Wu, T.; et al. Efficacy and Safety of Continuous Risankizumab Therapy vs Treatment Withdrawal in Patients with Moderate to Severe Plaque Psoriasis: A Phase 3 Randomized Clinical Trial. JAMA Dermatol. 2020, 156, 649–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papp, K.A.; de Vente, S.; Zeng, J.; Flack, M.; Padilla, B.; Tyring, S.K. Long-Term Safety and Efficacy of Risankizumab in Patients with Moderate-to-Severe Chronic Plaque Psoriasis: Results from a Phase 2 Open-Label Extension Trial. Dermatol. Ther. 2021, 11, 487–497. [Google Scholar] [CrossRef] [PubMed]
- McKeage, K.; Duggan, S. Risankizumab: First Global Approval. Drugs 2019, 79, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Khorrami, S.; Ginard, D.; Marín-Jiménez, I.; Chaparro, M.; Sierra, M.; Aguas, M.; Sicilia, B.; García-Sánchez, V.; Suarez, C.; Villoria, A.; et al. Ustekinumab for the Treatment of Refractory Crohn’s Disease: The Spanish Experience in a Large Multicentre Open-label Cohort. Inflamm. Bowel Dis. 2016, 22, 1662–1669. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Orlando, A.; Cottone, M. Anti-interleukin-12 and anti-interleukin-23 agents in Crohn’s disease. Expert Opin. Biol. Ther. 2019, 19, 89–98. [Google Scholar] [CrossRef]
- Berman, H.S.; Villa, N.M.; Shi, V.Y.; Hsiao, J.L. Guselkumab in the treatment of concomitant hidradenitis suppurativa, psoriasis, and Crohn’s disease. J. Dermatol. Treat. 2021, 32, 261–263. [Google Scholar] [CrossRef]
- Jørgensen, A.R.; Holm, J.G.; Thomsen, S.F. Guselkumab for hidradenitis suppurativa in a patient with concomitant Crohn’s disease: Report and systematic literature review of effectiveness and safety. Clin. Case Rep. 2020, 8, 2874–2877. [Google Scholar] [CrossRef]
- Fiorino, G.; Allocca, M.; Correale, C.; Roda, G.; Furfaro, F.; Loy, L.; Zilli, A.; Peyrin-Biroulet, L.; Danese, S. Positioning ustekinumab in moderate-to-severe ulcerative colitis: New kid on the block. Expert Opin. Biol. Ther. 2020, 20, 421–427. [Google Scholar] [CrossRef]
- Hanžel, J.; D’Haens, G.R. Anti-interleukin-23 agents for the treatment of ulcerative colitis. Expert Opin. Biol. Ther. 2020, 20, 399–406. [Google Scholar] [CrossRef]
- Chiricozzi, A.; Costanzo, A.; Fargnoli, M.C.; Malagoli, P.; Piaserico, S.; Amerio, P.; Argenziano, G.; Balato, N.; Bardazzi, F.; Bianchi, L.; et al. Guselkumab: An anti-IL-23 antibody for the treatment of moderate-to-severe plaque psoriasis. Eur. J. Dermatol. 2021, 31, 3–16. [Google Scholar]
- Leszczyński, P.; Pawlak-Buś, K. New treatment strategy including biological agents in patients with systemic lupus erythematosus. Pol. Arch. Med. Wewn 2013, 123, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Murugaiyan, G.; Mittal, A.; Lopez-Diego, R.; Maier, L.M.; Anderson, D.E.; Weiner, H.L. IL-27 Is a Key Regulator of IL-10 and IL-17 Production by Human CD4+ T Cells. J. Immunol. 2009, 183, 2435–2443. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | All Patients | Non-LN and Non-NPSLE | NPSLE | LN | NPSLE + LN | p |
|---|---|---|---|---|---|---|
| n | 72 | 30 | 21 | 16 | 5 | - |
| Sex (♂/♀) | 4/68 | 2/28 | 2/19 | 0/16 | 0/5 | 0.39 |
| Age (mean ± SD) (years) | 42.9 ± 13.3 | 47.7 ± 12.2 | 38.3 ± 11.4 | 42.1 ± 14.6 | 36.4 ± 16.9 | <0.05 |
| Age at disease onset (mean ± SD) (years) | 36.5 ± 12.6 | 41.9 ± 10.8 | 32.5 ± 10.7 | 33.6 ± 14.4 | 29.4 ± 14.8 | <0.05 |
| Disease duration (median, min–max) (years) | 5, 1–20 | 5, 1–12 | 4, 1–15 | 5, 1–20 | 7, 1–12 | 0.78 |
| Fever (yes/no) | 4/68 | 0/30 | 1/20 | 2/14 | 1/4 | 0.12 |
| Lupus rash (yes/no) | 53/19 | 22/8 | 5/16 | 4/12 | 2/3 | 0.91 |
| Alopecia (yes/no) | 45/27 | 19/11 | 12/9 | 12/4 | 2/3 | 0.49 |
| Mucosal ulcers (yes/no) | 5/67 | 0/30 | 2/19 | 2/14 | 1/4 | 0.11 |
| Arthritis (yes/no) | 53/19 | 21/9 | 15/6 | 13/3 | 4/1 | 0.83 |
| Myositis (yes/no) | 0/72 | 0/30 | 0/21 | 0/16 | 0/5 | - |
| Psychosis (yes/no) | 4/68 | 0/30 | 4/17 | 0/16 | 5/0 | <0.05 |
| Organic brain syndrome (yes/no) | 25/47 | 0/30 | 21/0 | 0/16 | 4/1 | <0.001 |
| Cranial nerves disorder (yes/no) | 1/71 | 0/30 | 1/20 | 0/16 | 0/5 | 0.48 |
| Vision disturbances (yes/no) | 1/71 | 0/30 | 1/20 | 0/16 | 0/5 | 0.48 |
| Lupus headache (yes/no) | 6/66 | 0/30 | 5/16 | 0/16 | 1/4 | <0.01 |
| Cerebrovascular accident (yes/no) | 2/70 | 0/30 | 1/20 | 0/16 | 1/4 | 0.16 |
| Vasculitis (yes/no) | 11/61 | 2/28 | 4/17 | 3/13 | 2/3 | 0.24 |
| Pleuritis (yes/no) | 4/68 | 0/30 | 2/19 | 0/16 | 2/3 | <0.05 |
| Pericarditis (yes/no) | 2/70 | 0/30 | 0/21 | 1/15 | 1/4 | 0.12 |
| Active urinary sediment (yes/no) | 3/69 | 0/30 | 0/21 | 1/15 | 2/3 | <0.05 |
| Hematuria (yes/no) | 2/70 | 0/30 | 0/21 | 0/16 | 2/3 | <0.01 |
| Proteinuria (yes/no) | 18/54 | 0/30 | 0/21 | 13/3 | 5/0 | <0.001 |
| Leukocyturia (yes/no) | 7/65 | 0/30 | 0/21 | 5/11 | 2/3 | <0.001 |
| Leukopenia (yes/no) | 11/61 | 4/26 | 5/16 | 1/15 | 1/4 | 0.48 |
| Thrombocytopenia (yes/no) | 9/63 | 4/26 | 1/20 | 2/14 | 2/3 | 0.28 |
| Variables | All Patients | Non-LN and Non-NPSLE | NPSLE | LN | NPSLE + LN | p |
|---|---|---|---|---|---|---|
| SLEDAI (median, min–max) (points) | 14, 2–55 | 8, 2–20 | 24, 12–36 | 15, 8–27 | 32, 26–55 | <0.001 |
| PGA (median, min–max) (points) | 1, 0–3 | 1, 0–3 | 2, 0–3 | 1, 0–3 | 3, 0–3 | <0.05 |
| SDI (yes/no) | 30/42 | 11/19 | 8/13 | 9/7 | 2/3 | 0.61 |
| Low C3/C4 (yes/no) | 36/36 | 13/17 | 11/10 | 11/5 | 1/4 | 0.19 |
| Elevated anti-dsDNA (yes/no) | 49/23 | 16/14 | 16/5 | 12/4 | 5/0 | 0.05 |
| Elevated anti-dsDNA and low C3/C4 (yes/no) | 33/39 | 11/19 | 10/11 | 10/6 | 2/3 | 0.41 |
| IL-23 (median, min–max) (pg/mL) | 1.18, 0.11–3.28 | 1.16, 0.11–2.67 | 1.23, 0.16–3.19 | 1.06, 0.14–3.28 | 0.96, 0.46–3.15 | 0.70 |
| IL-27 (median, min–max) (pg/mL) | 0.09, 0.07–0.26 | 0.09, 0.07–0.16 | 0.09, 0.08–0.26 | 0.09, 0.07–0.14 | 0.10, 0.08–0.12 | 0.47 |
| SLEDAI Score (Points) | Odds Ratio | |||||
|---|---|---|---|---|---|---|
| Determinant | n | 1–11, n = 27 n (%) | ≥12, n = 45 n (%) | OR | 95% CI | p |
| Disease duration (years) | 72 | 0.33 | ||||
| [1, 4] | 9 (33%) | 23 (51%) | — | — | ||
| (4, 7.57] | 7 (26%) | 9 (20%) | 0.50 | 0.14, 1.78 | ||
| (7.57, 20] | 11 (41%) | 13 (29%) | 0.46 | 0.15, 1.40 | ||
| Age at disease onset (years) median (IQR) | 72 | 42 (39, 50) | 35 (22, 43) | 0.94 | 0.90, 0.98 | <0.01 |
| IL-27 (pg/mL) | 72 | 0.29 | ||||
| [0.067, 0.0837] | 12 (44%) | 12 (27%) | — | — | ||
| (0.0837, 0.0983] | 7 (26%) | 17 (38%) | 2.43 | 0.75, 8.31 | ||
| (0.0983, 0.255] | 8 (30%) | 16 (36%) | 2.00 | 0.63, 6.62 | ||
| IL-23 (pg/mL) | 72 | 0.10 | ||||
| [0.112, 0.776] | 13 (48%) | 11 (24%) | — | — | ||
| (0.776, 1.55] | 6 (22%) | 18 (40%) | 3.55 | 1.08, 12.8 | ||
| (1.55, 3.28] | 8 (30%) | 16 (36%) | 2.36 | 0.75, 7.87 | ||
| Decreased C3/C4 | 72 | <0.01 | ||||
| No | 19 (70%) | 17 (38%) | — | — | ||
| Yes | 8 (30%) | 28 (62%) | 3.91 | 1.45, 11.4 | ||
| Anti-dsDNA | 72 | <0.001 | ||||
| No | 15 (56%) | 8 (18%) | — | — | ||
| Yes | 12 (44%) | 37 (82%) | 5.78 | 2.03, 17.8 | ||
| LN | Odds Ratio | |||||
|---|---|---|---|---|---|---|
| Determinant | n | 0, n = 51 n (%) | 1, n = 21 n (%) | OR | 95% CI | p |
| Disease duration (years) | 72 | 0.84 | ||||
| [1, 4] | 23 (45%) | 9 (43%) | — | — | ||
| (4, 7.57] | 12 (24%) | 4 (19%) | 0.85 | 0.20, 3.23 | ||
| (7.57, 20] | 16 (31%) | 8 (38%) | 1.28 | 0.40, 4.06 | ||
| Age at disease onset (years) median (IQR) | 72 | 40 (31, 44) | 28 (21, 45) | 0.97 | 0.92, 1.01 | 0.09 |
| IL-27 (pg/mL) | 72 | 0.82 | ||||
| [0.067, 0.0837] | 18 (35%) | 6 (29%) | — | — | ||
| (0.0837, 0.0983] | 17 (33%) | 7 (33%) | 1.24 | 0.34, 4.56 | ||
| (0.0983, 0.255] | 16 (31%) | 8 (38%) | 1.50 | 0.43, 5.46 | ||
| IL-23 (pg/mL) | 72 | 0.82 | ||||
| [0.112, 0.776] | 17 (33%) | 7 (33%) | — | — | ||
| (0.776, 1.55] | 16 (31%) | 8 (38%) | 1.21 | 0.36, 4.22 | ||
| (1.55, 3.28] | 18 (35%) | 6 (29%) | 0.81 | 0.22, 2.92 | ||
| Decreased C3/C4 | 72 | 0.44 | ||||
| No | 27 (53%) | 9 (43%) | — | — | ||
| Yes | 24 (47%) | 12 (57%) | 1.50 | 0.54, 4.27 | ||
| Anti-dsDNA | 72 | 0.12 | ||||
| No | 19 (37%) | 4 (19%) | — | — | ||
| Yes | 32 (63%) | 17 (81%) | 2.52 | 0.79, 9.76 | ||
| NPSLE | Odds Ratio | |||||
|---|---|---|---|---|---|---|
| Determinant | n | 0, n = 46 n (%) | 1, n = 26 n (%) | OR | 95% CI | p |
| Disease duration (years) | 72 | 0.55 | ||||
| [1, 4] | 19 (41%) | 13 (50%) | — | — | ||
| (4, 7.57] | 12 (26%) | 4 (15%) | 0.49 | 0.12, 1.76 | ||
| (7.57, 20] | 15 (33%) | 9 (35%) | 0.88 | 0.29, 2.59 | ||
| Age at disease onset (years) median (IQR) | 72 | 42 (31, 48) | 32 (22, 39) | 0.95 | 0.91, 0.99 | <0.05 |
| IL-27 (pg/mL) | 72 | 0.31 | ||||
| [0.067, 0.0837] | 18 (39%) | 6 (23%) | — | — | ||
| (0.0837, 0.0983] | 13 (28%) | 11 (42%) | 2.54 | 0.76, 9.09 | ||
| (0.0983, 0.255] | 15 (33%) | 9 (35%) | 1.80 | 0.53, 6.49 | ||
| IL-23 (pg/mL) | 72 | 0.37 | ||||
| [0.112, 0.776] | 18 (39%) | 6 (23%) | — | — | ||
| (0.776, 1.55] | 14 (30%) | 10 (38%) | 2.14 | 0.64, 7.69 | ||
| (1.55, 3.28] | 14 (30%) | 10 (38%) | 2.14 | 0.64, 7.69 | ||
| Decreased C3/C4 | 72 | 0.62 | ||||
| No | 22 (48%) | 14 (54%) | — | — | ||
| Yes | 24 (52%) | 12 (46%) | 0.79 | 0.30, 2.06 | ||
| Anti-dsDNA | 72 | 0.08 | ||||
| No | 18 (39%) | 5 (19%) | — | — | ||
| Yes | 28 (61%) | 21 (81%) | 2.70 | 0.91, 9.24 | ||
| Elevated Anti-dsDNA and Low C3/C4 No (n = 39) | Elevated Anti-dsDNA and Low C3/C4 Yes (n = 33) | p | |
|---|---|---|---|
| IL-23 (pg/mL) | 0.96, 0.11–3.28 | 1.30, 0.14–3.19 | 0.31 |
| IL-27 (pg/mL) | 0.09, 0.07–0.16 | 0.09, 0.07–0.26 | 0.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pawlak-Buś, K.; Schmidt, W.; Leszczyński, P. Lack of Association between Serum Interleukin-23 and Interleukin-27 Levels and Disease Activity in Patients with Active Systemic Lupus Erythematosus. J. Clin. Med. 2021, 10, 4788. https://doi.org/10.3390/jcm10204788
Pawlak-Buś K, Schmidt W, Leszczyński P. Lack of Association between Serum Interleukin-23 and Interleukin-27 Levels and Disease Activity in Patients with Active Systemic Lupus Erythematosus. Journal of Clinical Medicine. 2021; 10(20):4788. https://doi.org/10.3390/jcm10204788
Chicago/Turabian StylePawlak-Buś, Katarzyna, Wiktor Schmidt, and Piotr Leszczyński. 2021. "Lack of Association between Serum Interleukin-23 and Interleukin-27 Levels and Disease Activity in Patients with Active Systemic Lupus Erythematosus" Journal of Clinical Medicine 10, no. 20: 4788. https://doi.org/10.3390/jcm10204788