
Incidence and Practice of Early Prone Positioning in Invasively Ventilated COVID-19 Patients—Insights from the PRoVENT-COVID Observational Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Ethics
2.3. Study Registration
2.4. Inclusion and Exclusion Criteria
2.5. Collected Data, and Patient Classification
2.6. Study Endpoints
2.7. Statistical Analyses
3. Results
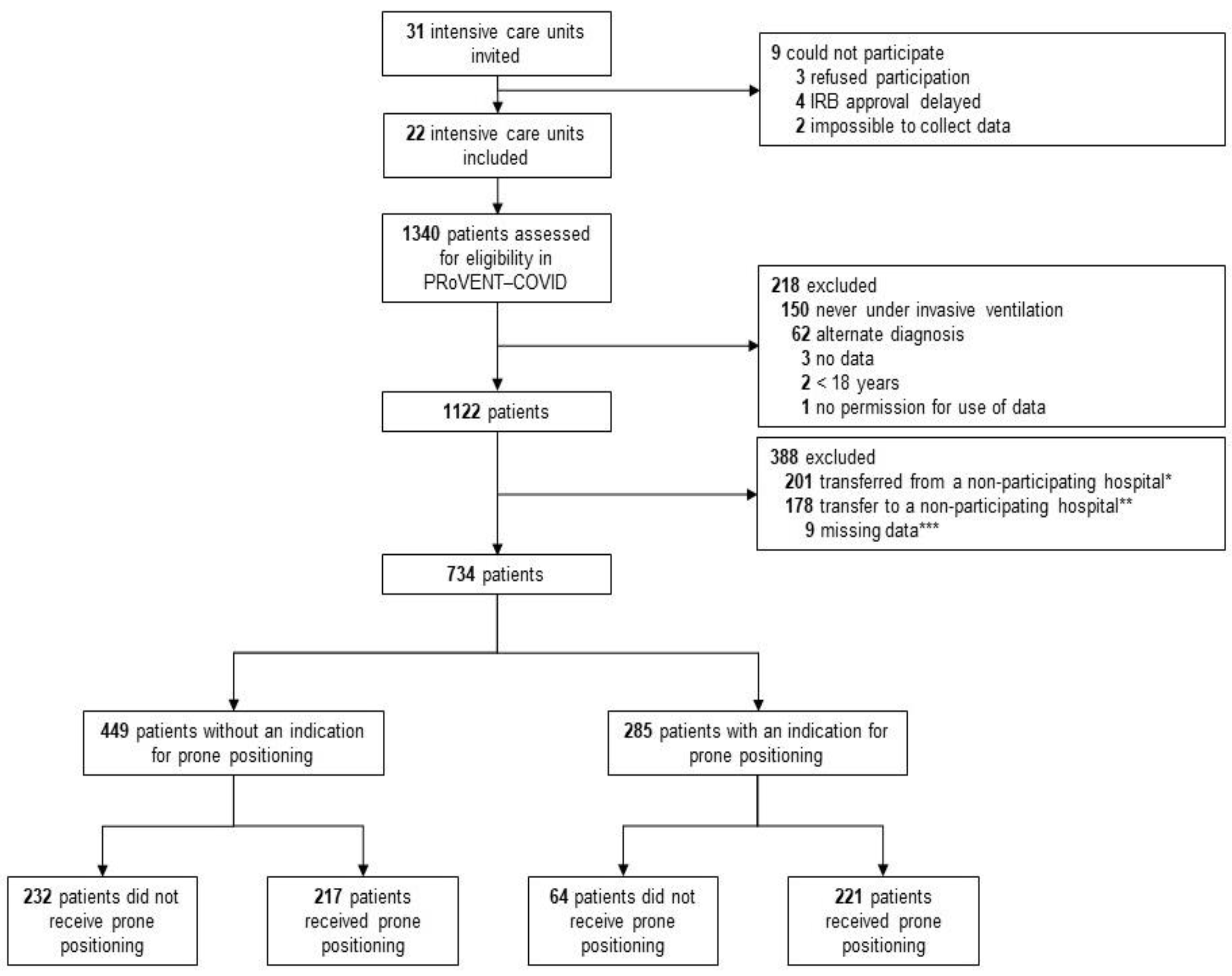
3.1. Patients Enrolled
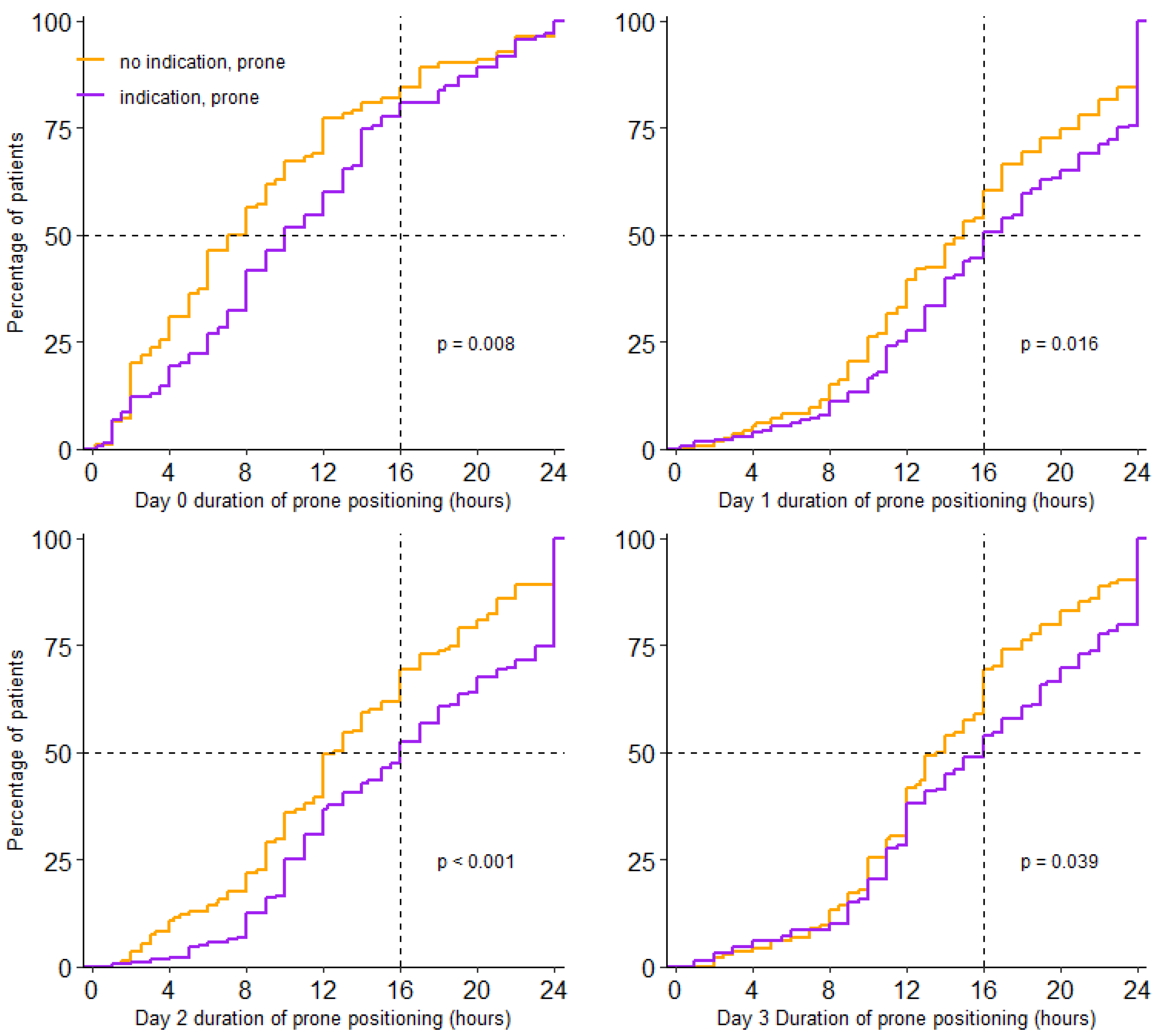
3.2. Incidence of Prone Positioning
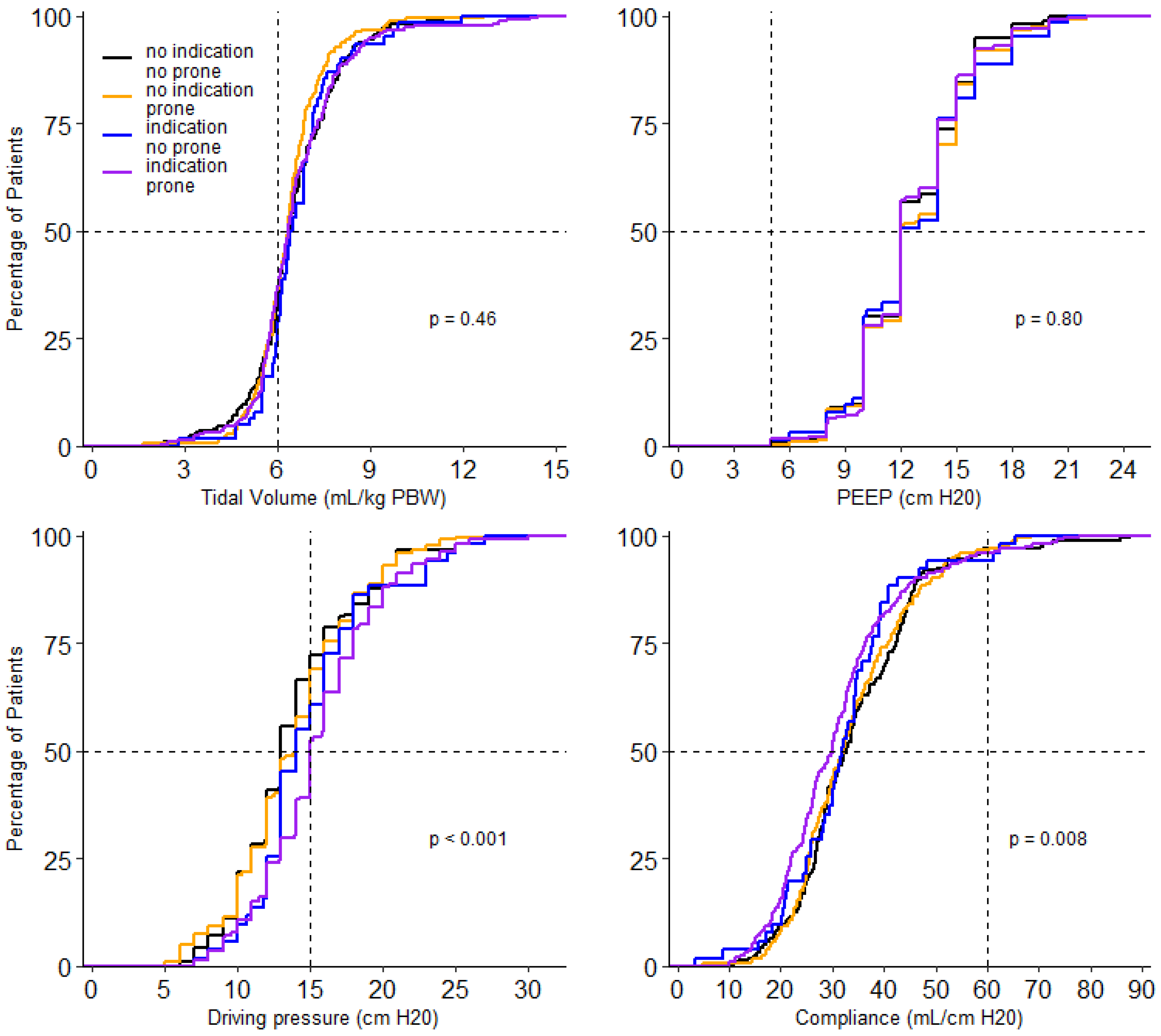
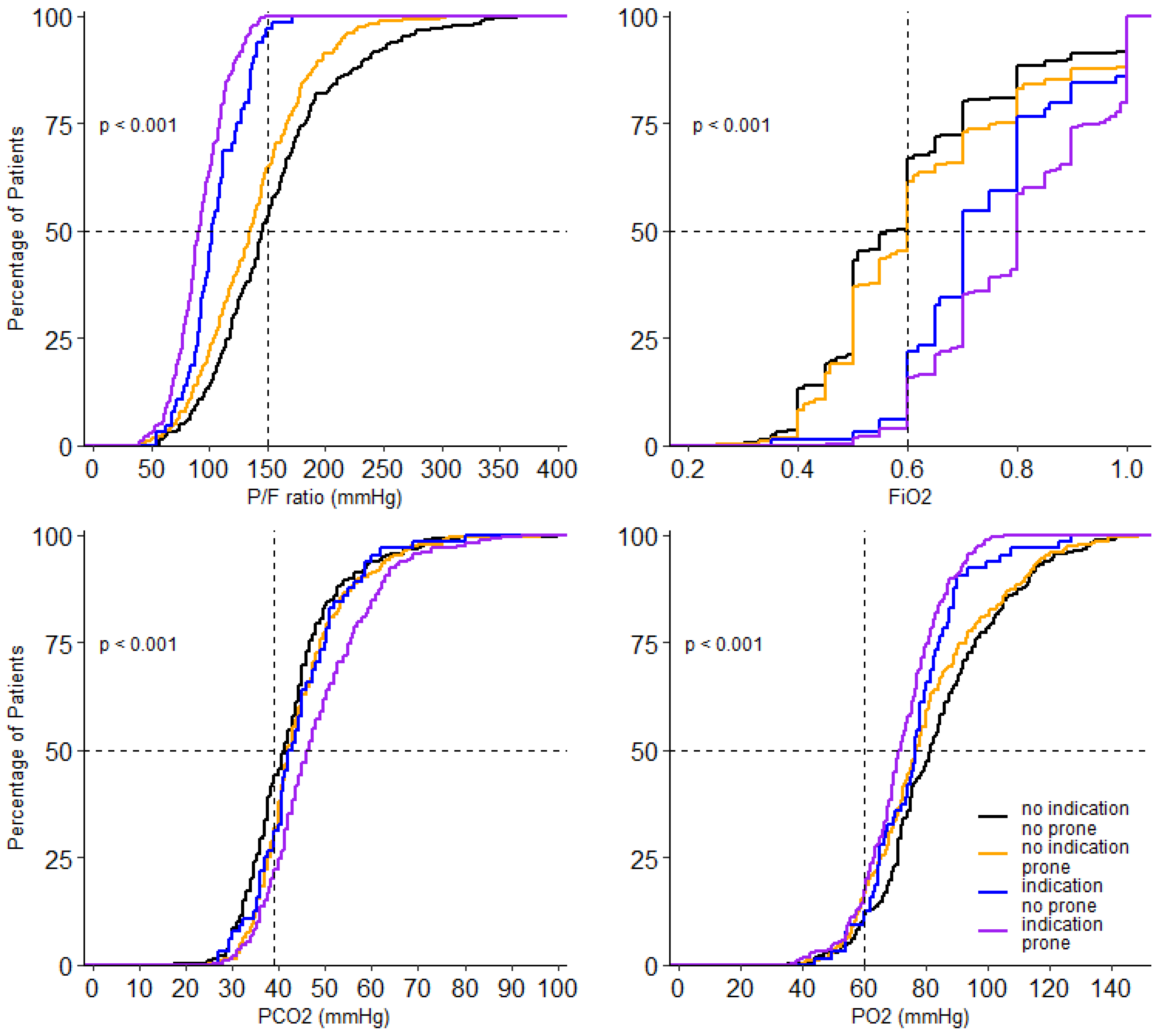
3.3. Ventilation Characteristics in the First 4 Calendar Days of Ventilation
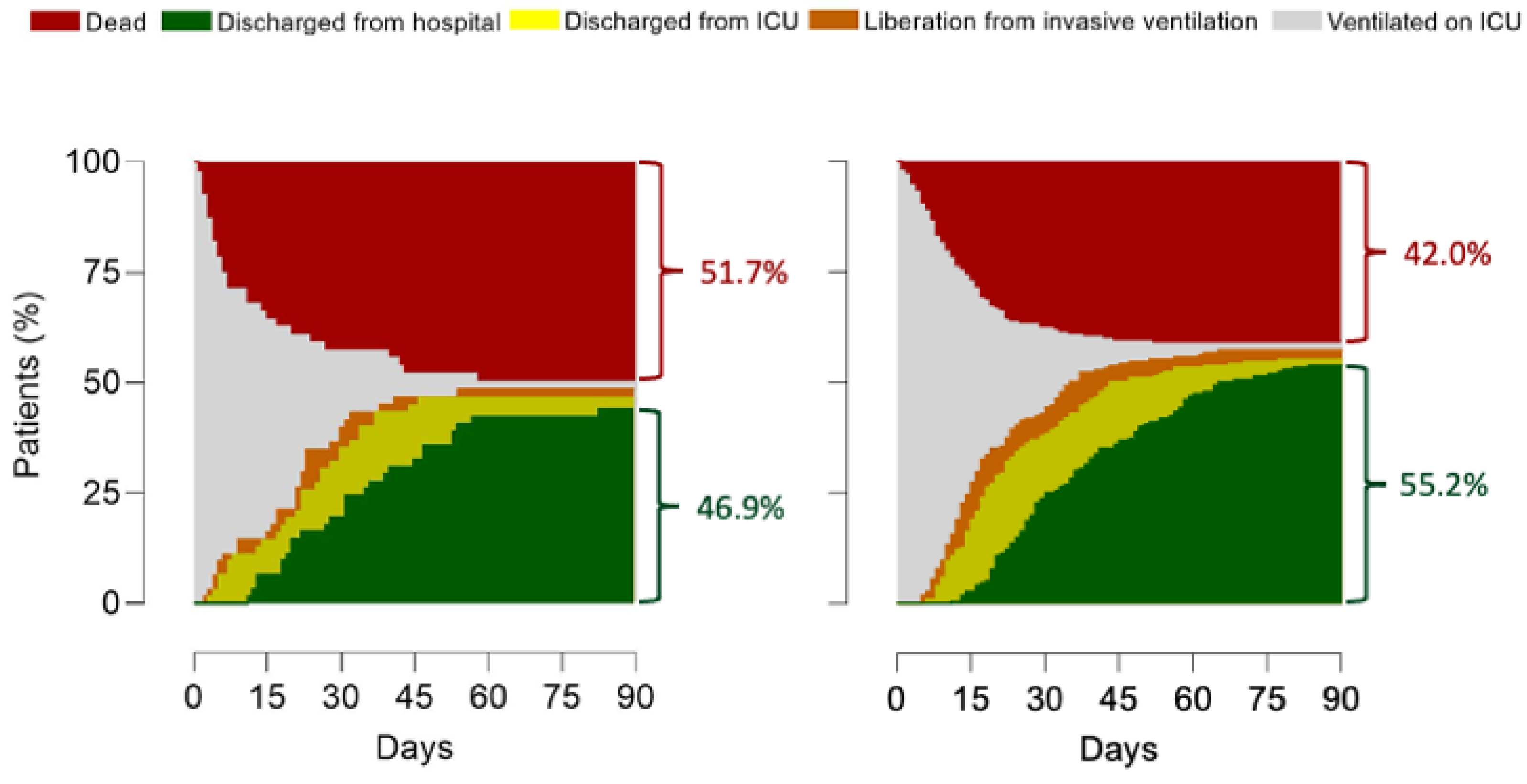
3.4. Patient Outcomes
3.5. Factors That Have an Association with Use of Prone Positioning
3.6. Post Hoc Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Sud, S.; Friedrich, J.; Adhikari, N.K.J.; Taccone, P.; Mancebo, J.; Polli, F.; Latini, R.; Pesenti, A.; Curley, M.; Fernandez, R.; et al. Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: A systematic review and meta-analysis. Can. Med. Assoc. J. 2014, 186, E381–E390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantin, J.-M.; Jabaudon, M.; Lefrant, J.-Y.; Jaber, S.; Quenot, J.-P.; Langeron, O.; Ferrandière, M.; Grelon, F.; Seguin, P.; Ichai, C.; et al. Personalised mechanical ventilation tailored to lung morphology versus low positive end-expiratory pressure for patients with acute respiratory distress syndrome in France (the LIVE study): A multicentre, single-blind, randomised controlled trial. Lancet Respir. Med. 2019, 7, 870–880. [Google Scholar] [CrossRef]
- Duggal, A.; Rezoagli, E.; Pham, T.; McNicholas, B.A.; Fan, E.; Bellani, G.; Rubenfeld, G.; Pesenti, A.M.; Laffey, J.G.; LUNG SAFE Investigators; et al. Patterns of Use of Adjunctive Therapies in Patients with Early Moderate to Severe ARDS: Insights from the LUNG SAFE Study. Chest 2020, 157, 1497–1505. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Beuret, P.; Constantin, J.M.; Bellani, G.; Garcia-Olivares, P.; Roca, O.; Meertens, J.H.; Maia, P.A.; Becher, T.; Peterson, J.; et al. A prospective international observational prevalence study on prone positioning of ARDS patients: The APRONET (ARDS Prone Position Network) study. Intensive Care Med. 2018, 44, 22–37. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, C.; Suarez-Sipmann, F.; Mellado-Artigas, R.; Hernández, M.; Gea, A.; Arruti, E.; Aldecoa, C.; Martínez-Pallí, G.; Martínez-González, M.A.; Slutsky, A.S.; et al. Correction to: Clinical features, ventilatory management, and outcome of ARDS caused by COVID-19 are similar to other causes of ARDS. Intensive Care Med. 2021, 47, 144–146. [Google Scholar] [CrossRef]
- Schultz, M.J. High versus low PEEP in non-recruitable collapsed lung tissue: Possible implications for patients with COVID-19. Lancet Respir. Med. 2020, 8, e44. [Google Scholar] [CrossRef]
- Grasselli, G.; Cattaneo, E.; Florio, G.; Ippolito, M.; Zanella, A.; Cortegiani, A.; Huang, J.; Pesenti, A.; Einav, S. Mechanical ventilation parameters in critically ill COVID-19 patients: A scoping review. Crit. Care 2021, 25, 115. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef]
- COVID-ICU Group on Behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef]
- Boers, N.S.; Botta, M.; Tsonas, A.M.; Algera, A.G.; Pillay, J.; Dongelmans, D.A.; Horn, J.; Vlaar, A.P.J.; Hollmann, M.W.; Bos, L.D.J.; et al. PRactice of VENTilation in Patients with Novel Coronavirus Disease (PRoVENT-COVID): Rationale and protocol for a national multicenter observational study in The Netherlands. Ann. Transl. Med. 2020, 8, 1251. [Google Scholar] [CrossRef]
- Botta, M.; Tsonas, A.M.; Pillay, J.; Boers, L.S.; Algera, A.G.; Bos, L.D.J.; Dongelmans, D.A.; Hollmann, M.W.; Horn, J.; Vlaar, A.P.J.; et al. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): A national, multicentre, observational cohort study. Lancet. Respir. Med. 2021, 9, 139–148. [Google Scholar] [CrossRef]
- PRactice of VENTilation in Patients with Coronavirus Disease 2019 (PRoVENT-COVID)—Rationale, Study Protocol and Statistical Analysis Plans for a National Multicenter Observational Study in The Netherlands. Available online: https://sites.google.com/view/provent-covid/provent-covid (accessed on 19 April 2021).
- Ferguson, N.D.; Fan, E.; Camporota, L.; Antonelli, M.; Anzueto, A.; Beale, R.; Brochard, L.; Brower, R.; Esteban, A.; Gattinoni, L.; et al. The Berlin definition of ARDS: An expanded rationale, justification, and supplementary material. Intensive Care Med. 2012, 38, 1573–1582. [Google Scholar] [CrossRef] [PubMed]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Mathews, K.S.; Soh, H.; Shaefi, S.; Wang, W.; Bose, S.; Coca, S.; Gupta, S.; Hayek, S.S.; Srivastava, A.; Brenner, S.K.; et al. Prone Positioning and Survival in Mechanically Ventilated Patients with Coronavirus Disease 2019–Related Respiratory Failure. Crit. Care Med. 2021, 49, 1026–1037. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Morris, Z.; Wooding, S.; Grant, J. The answer is 17 years, what is the question: Understanding time lags in translational research. J. R. Soc. Med. 2011, 104, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Schultz, M.J.; Neto, A.S.; Paulus, F. Battling COVID-19-related mortality: From a fight for ventilators to a cry for oxygen. Lancet Respir. Med. 2021, 9, 939–941. [Google Scholar] [CrossRef]
- Ferrando, C.; Mellado-Artigas, R.; Gea, A.; Arruti, E.; Aldecoa, C.; Bordell, A.; Adalia, R.; Zattera, L.; Ramasco, F.; Monedero, P.; et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: A prospective, cohort, multicentre study. Rev. Esp. Anestesiol. Reanim. 2020, 67, 425–437. [Google Scholar] [CrossRef]
- Chua, E.X.; Zahir, S.M.I.S.M.; Ng, K.T.; Teoh, W.Y.; Bin Hasan, M.S.; Ruslan, S.R.B.; Abosamak, M.F. Effect of prone versus supine position in COVID-19 patients: A systematic review and meta-analysis. J. Clin. Anesth. 2021, 74, 110406. [Google Scholar] [CrossRef]
- Murray, M.J.; DeBlock, H.F.; Erstad, B.L.; Gray, A.W.; Jacobi, J.; Jordan, C.J.; McGee, W.T.; McManus, C.; Meade, M.O.; Nix, S.A.; et al. Clinical practice guidelines for sustained neuromuscular blockade in the adult critically ill patient: 2016 update—executive summary. Am. J. Health Pharm. 2017, 74, 76–78. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss, M.; Huang, D.T.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; Hayden, D.; et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [CrossRef] [PubMed]
- Bassi, G.L.; Gibbons, K.; Suen, J.; Dalton, H.; White, N.; Barnett, A.; Fraser, J. COVID-19 Critical Care Consortium Neuromuscular Blocking Agents in Critically-Ill COVID-19 Patients Requiring Mechanical Ventilation. In TP48. TP048 COVID: ARDS CLINICAL STUDIES; American Thoracic Society: New York, NY, USA, 2021; p. A2489. [Google Scholar]
- Scaramuzzo, G.; Gamberini, L.; Tonetti, T.; Zani, G.; Ottaviani, I.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Reggiani, M.L.B.; Bertellini, E.; et al. Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: A cohort study. Ann. Intensive Care 2021, 11, 63. [Google Scholar] [CrossRef] [PubMed]
- Cour, M.; Bussy, D.; Stevic, N.; Argaud, L.; Guérin, C. Differential effects of prone position in COVID-19-related ARDS in low and high recruiters. Intensive Care Med. 2021, 47, 1044–1046. [Google Scholar] [CrossRef]
- Kallet, R.H. A Comprehensive Review of Prone Position in ARDS. Respir. Care 2015, 60, 1660–1687. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Huerta, M.D.; Diez-Fernandez, A.; Rodriguez-Alonso, M.J.; Robles-Gonzalez, M.; Martin-Rodriguez, M.; Gonzalez-Garcia, A. Nursing care and prevalence of adverse events in prone position: Characteristics of mechanically ventilated patients with severe SARS-CoV-2 pulmonary infection. Nurs. Crit. Care 2021. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Without an Indication for Prone Positioning | With an Indication for Prone Positioning | |||||
|---|---|---|---|---|---|---|
| No Prone Positioning (N = 232) | Prone Positioning (N = 217) | p Value | No Prone Positioning (N = 64) | Prone Positioning (N = 221) | p Value | |
| Age, years (median, IQR) | 64.2 (11.4) | 65.0 (10.3) | 0.430 | 66.6 (9.1) | 62.6 (11.2) | 0.008 |
| Male gender, N (%) | 171 (73.7) | 164 (73.2) | 0.916 | 46 (71.9) | 154 (69.1) | 0.758 |
| BMI, kg/m2 (median, IQR) | 28.5 (7.8) | 28.1 (4.0) | 0.490 | 29.2 (6.3) | 29.3 (5.3) | 0.841 |
| Chest CT performed, N (%) | 93 (40.1) | 82 (36.6) | 0.500 | 17 (26.6) | 92 (41.3) | 0.040 |
| Affected lung parenchyma (%) | 5 (5.3) | 2 (2.4) | 0.212 | 0 (0.0) | 2 (2.2) | 0.967 |
| ≤25% | 28 (29.8) | 28 (34.1) | 6 (35.3) | 27 (29.0) | ||
| 50% | 34 (36.2) | 19 (23.2) | 5 (29.4) | 30 (32.3) | ||
| 75% | 21 (22.3) | 28 (34.1) | 5 (29.4) | 29 (31.2) | ||
| 100% | 6 (6.4) | 5 (6.1) | 1 (5.9) | 5 (5.4) | ||
| Chest X-ray performed, N (%) | 127 (91.4) | 135 (93.8) | 0.501 | 44 (93.6) | 113 (85.6) | 0.199 |
| Number of quadrants affected (%) | 0.760 | 0.790 | ||||
| 1 | 10 (7.9) | 10 (7.4) | 2 (4.5) | 8 (7.0) | ||
| 2 | 27 (21.4) | 36 (26.7) | 9 (20.5) | 27 (23.7) | ||
| 3 | 31 (24.6) | 34 (25.2) | 16 (36.4) | 32 (28.1) | ||
| 4 | 58 (46.0) | 55 (40.7) | 17 (38.6) | 47 (41.2) | ||
| Pneumothorax, N (%) | 0 (0.0) | 0 (0.0) | 1.000 | 0 (0.0) | 1 (16.7) | 1.000 |
| Severity of illness | ||||||
| SAPS II (median, IQR) | 35.7 (11.7) | 36.9 (12.8) | 0.562 | 35.9 (16.1) | 37.1 (12.8) | 0.726 |
| APACHE II (median, IQR) | 16.6 (11.3) | 18.9 (8.5) | 0.230 | 16.1 (8.0) | 19.6 (9.3) | 0.295 |
| APACHE IV (median, IQR) | 55.2 (20.5) | 59.6 (22.9) | 0.197 | 67.2 (25.0) | 58.6 (20.6) | 0.086 |
| SOFA (median, IQR) | 8.1 (3.2) | 9.1 (4.4) | 0.066 | 8.6 (3.2) | 8.1 (3.8) | 0.512 |
| Severity class ARDS (%) | 0.002 | 0.607 | ||||
| Mild | 82 (36.3) | 51 (23.5) | 0 (0.0) | 2 (0.9) | ||
| Moderate | 142 (62.8) | 157 (72.4) | 49 (76.6) | 154 (69.4) | ||
| Severe | 2 (0.9) | 9 (4.1) | 15 (23.4) | 66 (29.7) | ||
| PaO2/FiO2 ≤ 150 mm Hg, N (%) | 90 (38.8) | 104 (47.9) | 0.024 | 56 (87.5) | 189 (85.5) | 0.600 |
| Medical history | ||||||
| None | 57 (24.6) | 46 (20.5) | 0.315 | 14 (21.9) | 60 (26.9) | 0.517 |
| Hypertension, N (%) | 75 (32.3) | 75 (33.5) | 0.842 | 26 (40.6) | 73 (32.7) | 0.296 |
| Heart failure, N (%) | 13 (5.6) | 12 (5.4) | 1.000 | 4 (6.2) | 7 (3.1) | 0.271 |
| Diabetes, N (%) | 43 (18.5) | 57 (25.4) | 0.089 | 12 (18.8) | 52 (23.3) | 0.499 |
| Chronic kidney disease (%) | 9 (3.9) | 9 (4.0) | 1.000 | 2 (3.1) | 7 (3.1) | 1.000 |
| Baseline creatinine, µmol/L (median, IQR) | 81.1 (37.2) | 96.2 (79.7) | 0.021 | 93.2 (48.1) | 82.5 (39.8) | 0.121 |
| Liver cirrhosis, N (%) | 1 (0.4) | 0 (0.0) | 1.000 | 1 (1.6) | 0 (0.0) | 0.223 |
| COPD, N (%) | 16 (6.9) | 17 (7.6) | 0.857 | 5 (7.8) | 24 (10.8) | 0.640 |
| Active hematological neoplasia, N (%) | 5 (2.2) | 4 (1.8) | 1.000 | 2 (3.1) | 0 (0.0) | 0.049 |
| Active solid neoplasia, N (%) | 6 (2.6) | 9 (4.0) | 0.440 | 0 (0.0) | 5 (2.2) | 0.590 |
| Neuromuscular disease, N (%) | 1 (0.4) | 0 (0.0) | 1.000 | 0 (0.0) | 5 (2.2) | 0.590 |
| Immunosuppression, N (%) | 10 (4.3) | 5 (2.2) | 0.295 | 1 (1.6) | 5 (2.2) | 1.000 |
| Home medication | ||||||
| Systemic steroids, N (%) | 13 (5.6) | 9 (4.0) | 0.515 | 3 (4.7) | 5 (2.2) | 0.383 |
| Inhalation steroids, N (%) | 26 (11.2) | 24 (10.7) | 0.882 | 7 (10.9) | 29 (13.0) | 0.831 |
| ACE inhibitor, N (%) | 44 (19.0) | 48 (21.4) | 0.560 | 7 (10.9) | 38 (17.0) | 0.329 |
| Angiotensin II receptor blocker, N (%) | 22 (9.5) | 29 (12.9) | 0.298 | 9 (14.1) | 21 (9.4) | 0.352 |
| Beta blocker, N (%) | 44 (19.0) | 43 (19.2) | 1.000 | 18 (28.1) | 43 (19.3) | 0.165 |
| Insulin, N (%) | 17 (7.3) | 21 (9.4) | 0.499 | 1 (1.6) | 9 (4.0) | 0.467 |
| Metformin, N (%) | 32 (13.8) | 44 (19.6) | 0.103 | 7 (10.9) | 36 (16.1) | 0.426 |
| Statin, N (%) | 63 (27.2) | 76 (33.9) | 0.127 | 18 (28.1) | 76 (34.1) | 0.450 |
| Calcium channel blockers, N (%) | 31 (13.4) | 49 (21.9) | 0.019 | 15 (23.4) | 39 (17.5) | 0.281 |
| No Indication for Prone Positioning (N = 217) | Indication for Prone Positioning (N = 221) | p Value | |
|---|---|---|---|
| Day 0 | |||
| n/N (%) | 110/217 (51) | 130/221 (59) | |
| absolute time in a prone position, hours (median, IQR) | 7.5 (3.6–12.0) | 10.0 (6.0–14.4) | 0.008 |
| relative time in a prone position, % of total hours * | 75% (65–75) | 100% (80–100) | <0.001 |
| Day 1 | |||
| n/N (%) | 167/217 (77) | 180/221 (81) | |
| absolute time in a prone position, hours (median, IQR) | 15 (10.0–20.5) | 16 (11.9–23.1) | 0.016 |
| relative time in a prone position, % of total hours | 63% (42–85) | 67% (50–96) | 0.016 |
| Day 2 | |||
| n/N (%) | 147/217 (68) | 175/221 (79) | |
| absolute time in a prone position, hours (median, IQR) | 12.5 (9.0–18.8) | 16 (10.5–23.5) | <0.001 |
| relative time in a prone position, % of total hours * | 52% (38–78) | 67% (44–98) | <0.001 |
| Day 3 | |||
| n/N (%) | 143/217 (66) | 152/221 (66) | |
| absolute time in a prone position, hours (median, IQR) | 13.8 (10.3–18.0) | 16.0 (11.0–22.0) | 0.039 |
| relative time in a prone position, % of total hours * | 58% (43–75) | 67% (46–92) | 0.039 |
| Total | |||
| Duration of prone positioning per full calendar day (median, IQR) | 14.0 (10.0–19.0) | 16.0 (11.0–23.0) | <0.001 |
| Without an Indication for Prone Positioning | With an Indication for Prone Positioning | |||||
|---|---|---|---|---|---|---|
| No Prone Positioning (N = 232) | Prone Positioning (N = 217) | p Value | No Prone Positioning (N = 64) | Prone Positioning (N = 221) | p Value | |
| Mode of ventilation | 232 | 217 | 64 | 221 | ||
| Volume Control | 23 (10.0) | 51 (22.8) | 6 (9.4) | 32 (14.5) | ||
| Pressure Control | 127 (55.5) | 116 (51.8) | 33 (51.6) | 131 (59.3) | ||
| Pressure Support | 7 (3.1) | 4 (1.8) | 0 (0.0) | 8 (3.6) | ||
| SIMV | 17 (7.4) | 24 (10.7) | 11 (17.2) | 19 (8.6) | ||
| APRV | 6 (2.6) | 7 (3.1) | 0 (0.0) | 9 (4.1) | ||
| Intellivent-ASV | 11 (4.8) | 6 (2.7) | 3 (4.7) | 5 (2.3) | ||
| other | 38 (16.6) | 16 (7.1) | 11 (17.2) | 17 (7.7) | ||
| Vt, mL/kg PBW (median, IQR) | 6.2 (5.7–6.9) | 6.2 (5.7, 6.8) | 0.561 | 6.3 (5.9–7.1) | 6.2 (5.7–7.0) | 0.295 |
| PEEP (median, IQR) | 12.0 (10.0–15.0) | 12.0 (10.0–15.0) | 0.419 | 12.0 (10.0–14.0) | 12.0 (10.0–14.8) | 0.848 |
| Ppeak (median, IQR) | 25.5 (23.0–29.0) | 27.0 (24.0–30.0) | 0.022 | 27.0 (24.0–30.0) | 28.0 (25.0–32.0) | 0.106 |
| Driving pressure (median, IQR) | 13.3 (12.0–16.0) | 15.0 (12.0–16.8) | 0.059 | 14.0 (13.0–16.2) | 15.7 (13.0–18.2) | 0.030 |
| Mechanical power (median, IQR) | 17.0 (13.2–19.8) | 16.4 (13.6–19.8) | 0.861 | 17.7 (13.9–21.4) | 18.1 (14.8–22.6) | 0.418 |
| Compliance (median, IQR) | 31.8 (26.1–40.6) | 29.5 (24.1–38.2) | 0.120 | 32.3 (26.0–38.2) | 28.7 (22.3–34.5) | 0.039 |
| Total respiratory rate (median, IQR) | 20.0 (18.0–22.8) | 20.0 (20.0–24.0) | 0.136 | 20.0 (18.0–21.5) | 21.0 (18.0–25.0) | 0.014 |
| FiO2 (median, IQR) | 0.6 (0.5–0.8) | 0.6 (0.5–0.8) | 0.127 | 0.7 (0.6–0.8) | 0.8 (0.7–1.0) | 0.016 |
| SpO2/FiO2 ratio (median, IQR) | 158.3 (125.5–192.1) | 153.3 (116.7–180.0) | 0.022 | 129.0 (109.1–141.5) | 115.1 (96.2–136.5) | 0.012 |
| End tidal CO2 mmHg (median, IQR) | 4.8 (4.3–5.5) | 4.8 (4.2–5.5) | 0.889 | 4.7 (4.3–5.6) | 4.9 (4.3–5.7) | 0.291 |
| NMBA | 89 (38.4) | 116 (51.8) | 0.005 | 27 (42.2) | 133 (59.6) | 0.015 |
| Vital signs | ||||||
| Mean arterial pressure, mmHg (median, IQR) | 82.5 (72.0–98.0) | 86.0 (75.0–101.0) | 0.106 | 87.0 (74.0–97.2) | 88.5 (75.0–105.2) | 0.386 |
| Heart rate, beats per min (median, IQR) | 89.0 (77.0–105.5) | 91.0 (78.0–105.0) | 0.380 | 88.5 (76.5–100.2) | 96.0 (83.0–112.0) | 0.002 |
| Laboratory tests | ||||||
| pH (median, IQR) | 7.4 (7.3–7.4) | 7.4 (7.3–7.4) | 0.083 | 7.4 (7.3–7.4) | 7.3 (7.3–7.4) | 0.224 |
| PaO2 (median, IQR) | 12.3 (10.1–15.6) | 11.2 (9.5–13.8) | 0.001 | 10.4 (9.3–11.8) | 10.1 (8.9–11.4) | 0.173 |
| PaO2/FiO2 ratio (median, IQR) | 161.5 (118.8–212.9) | 143.8 (106.5–181.3) | 0.005 | 108.8 (92.2–132.0) | 96.4 (79.2–119.2) | 0.005 |
| PaCO2 (median, IQR) | 5.5 (4.7–6.1) | 5.6 (4.9–6.5) | 0.037 | 5.9 (5.0–6.7) | 6.2 (5.3–7.3) | 0.031 |
| Lactate (median, IQR) | 1.2 (0.9–1.5) | 1.2 (0.9–1.5) | 0.713 | 1.2 (1.0–1.6) | 1.2 (0.9–1.5) | 0.466 |
| Creatinine, µmol/L (median, IQR) | 72.0 (58.0–91.0) | 74.0 (62.0–100.0) | 0.111 | 80.0 (68.0–96.0) | 74.0 (57.0–91.2) | 0.086 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stilma, W.; van Meenen, D.M.P.; Valk, C.M.A.; de Bruin, H.; Paulus, F.; Serpa Neto, A.; Schultz, M.J.; on behalf of the PRoVENT-COVID Collaborative Group. Incidence and Practice of Early Prone Positioning in Invasively Ventilated COVID-19 Patients—Insights from the PRoVENT-COVID Observational Study. J. Clin. Med. 2021, 10, 4783. https://doi.org/10.3390/jcm10204783
Stilma W, van Meenen DMP, Valk CMA, de Bruin H, Paulus F, Serpa Neto A, Schultz MJ, on behalf of the PRoVENT-COVID Collaborative Group. Incidence and Practice of Early Prone Positioning in Invasively Ventilated COVID-19 Patients—Insights from the PRoVENT-COVID Observational Study. Journal of Clinical Medicine. 2021; 10(20):4783. https://doi.org/10.3390/jcm10204783
Chicago/Turabian StyleStilma, Willemke, David M. P. van Meenen, Christel M. A. Valk, Hendrik de Bruin, Frederique Paulus, Ary Serpa Neto, Marcus J. Schultz, and on behalf of the PRoVENT-COVID Collaborative Group. 2021. "Incidence and Practice of Early Prone Positioning in Invasively Ventilated COVID-19 Patients—Insights from the PRoVENT-COVID Observational Study" Journal of Clinical Medicine 10, no. 20: 4783. https://doi.org/10.3390/jcm10204783