
Minor Sphincter Sparing Surgery for Successful Closure of Perianal Fistulas in Patients with Crohn’s Disease

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Perianal Fistula Treatment
2.3. Surgical Management
2.4. Postoperative Standard Care
2.5. Data Collection
2.6. Fistula Healing, Persistence, and Recurrence
2.7. Statistical Analysis
3. Results
3.1. Study Population
3.2. Clinical Appearance of Perianal Fistulas
3.3. Surgical Treatment
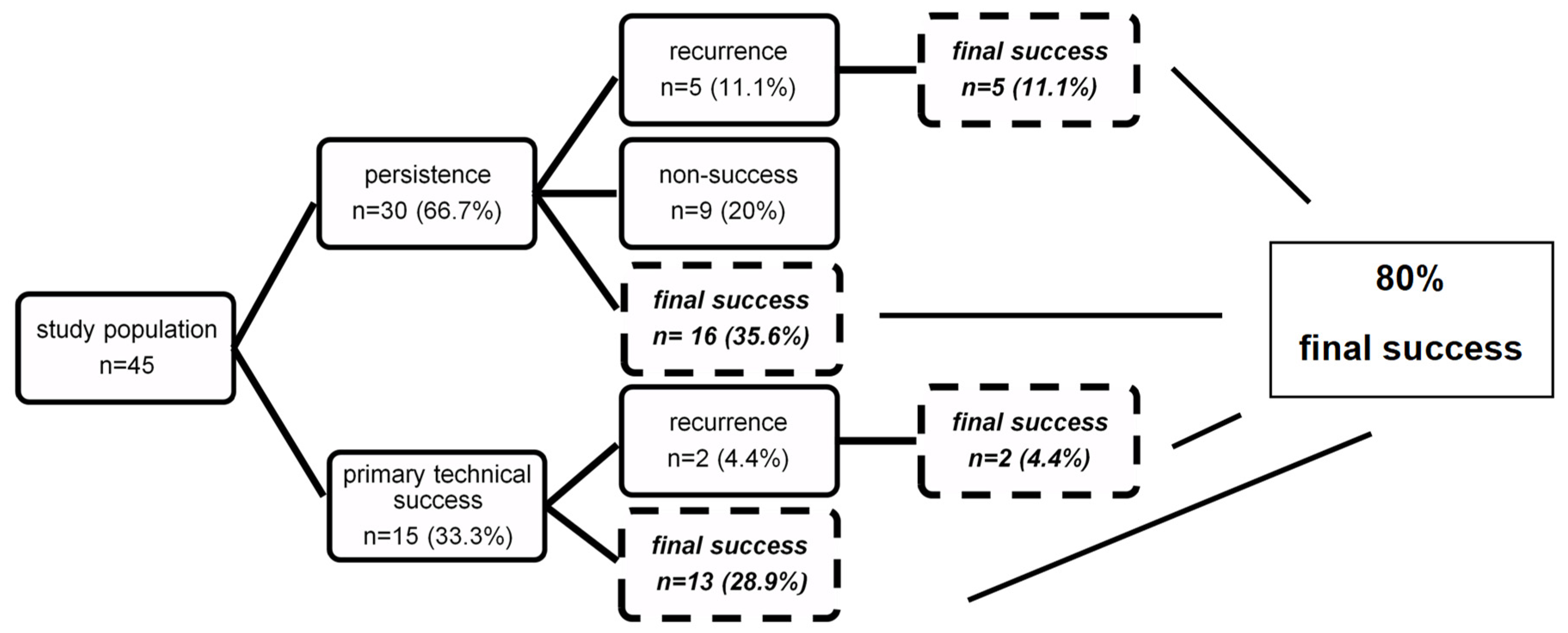
3.4. Surgical Outcome
3.5. Determinants for Successful Treatment, Persistence, and Recurrence
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hellers, G.; Bergstrand, O.; Ewerth, S.; Holmstrom, B. Occurrence and outcome after primary treatment of anal fistulae in Crohn’s disease. Gut 1980, 21, 525–527. [Google Scholar] [CrossRef] [Green Version]
- Burisch, J.; Kiudelis, G.; Kupcinskas, L.; Kievit, H.A.L.; Andersen, K.W.; Andersen, V.; Salupere, R.; Pedersen, N.; Kjeldsen, J.; D’Inca, R.; et al. Natural disease course of Crohn’s disease during the first 5 years after diagnosis in a European population-based inception cohort: An Epi-IBD study. Gut 2019, 68, 423–433. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Loftus, E.V.; Tremaine, W.J.; Panaccione, R.; Harmsen, W.S.; Zinsmeister, A.R.; Sandborn, W.J. The natural history of fistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology 2002, 122, 875–880. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Fazio, V.W.; Feagan, B.G.; Hanauer, S.B.; AGACP Committee. AGA technical review on perianal Crohn’s disease. Gastroenterology 2003, 125, 1508–1530. [Google Scholar] [CrossRef]
- Yassin, N.A.; Askari, A.; Warusavitarne, J.; Faiz, O.D.; Athanasiou, T.; Phillips, R.K.; Hart, A.L. Systematic review: The combined surgical and medical treatment of fistulising perianal Crohn’s disease. Aliment. Pharmacol. Ther. 2014, 40, 741–749. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Ghazi, L.J.; Regueiro, M.; Fichera, A.; Zoccali, M.; Ong, E.M.; Mortelé, K.J.; Crohn’s & Colitis Foundation of America Inc. Guidelines for the multidisciplinary management of Crohn’s perianal fistulas: Summary statement. Inflamm. Bowel Dis. 2015, 21, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, S.; Black, C.; Pugliese, D.; Armuzzi, A.; Sahnan, K.; Elkady, S.M.; Katsanos, K.H.; Christodoulou, D.K.; Selinger, C.; Maconi, G.; et al. The role of multimodal treatment in Crohn’s disease patients with perianal fistula: A multicentre retrospective cohort study. Aliment. Pharmacol. Ther. 2018, 48, 941–950. [Google Scholar] [CrossRef]
- Bell, S.J.; Williams, A.B.; Wiesel, P.; Wilkinson, K.; Cohen, R.C.; Kamm, M.A. The clinical course of fistulating Crohn’s disease. Aliment. Pharmacol. Ther. 2003, 17, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Ding, N.S.; Mathis, K.L.; Dulai, P.S.; Farrell, A.M.; Pemberton, J.H.; Hart, A.L.; Sandborn, W.J.; Loftus, E.V. Systematic review with meta-analysis: Faecal diversion for management of perianal Crohn’s disease. Aliment. Pharmacol. Ther. 2015, 42, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, M.S.; Satsangi, J.; Ahmad, T.; Arnott, I.D.; Bernstein, C.N.; Brant, S.R.; Caprilli, R.; Colombel, J.F.; Gasche, C.; Geboes, K.; et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: Report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can. J. Gastroenterol. 2005, 19 (Suppl. A), 5A–36A. [Google Scholar] [CrossRef]
- Parks, A.G.; Stitz, R.W. The treatment of high fistula-in-ano. Dis. Colon Rectum 1976, 19, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Irvine, E.J. Usual therapy improves perianal Crohn’s disease as measured by a new disease activity index. McMaster IBD Study Group. J. Clin. Gastroenterol. 1995, 20, 27–32. [Google Scholar] [PubMed]
- Lapidus, A. Crohn’s disease in Stockholm County during 1990–2001: An epidemiological update. World J. Gastroenterol. 2006, 12, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Van Koperen, P.J.; Safiruddin, F.; Bemelman, W.A.; Slors, J.F. Outcome of surgical treatment for fistula in ano in Crohn’s disease. Br. J. Surg. 2009, 96, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Cosnes, J.; Cattan, S.; Blain, A.; Beaugerie, L.; Carbonnel, F.; Parc, R.; Gendre, J.P. Long-term evolution of disease behavior of Crohn’s disease. Inflamm. Bowel Dis. 2002, 8, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Heywood, N.; Sagar, P.M.; Brown, S.R.; Fearnhead, N.S.; pCD Collaborators. Surgical management of fistulating perianal Crohn’s disease: A UK survey. Colorectal Dis. 2017, 19, 266–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotze, P.G.; Shen, B.; Lightner, A.; Yamamoto, T.; Spinelli, A.; Ghosh, S.; Panaccione, R. Modern management of perianal fistulas in Crohn’s disease: Future directions. Gut 2018, 67, 1181–1194. [Google Scholar] [CrossRef] [PubMed]
- Shen, B. Exploring endoscopic therapy for the treatment of Crohn’s disease-related fistula and abscess. Gastrointest. Endosc. 2017, 85, 1133–1143. [Google Scholar] [CrossRef]
- Williams, J.G.; Rothenberger, D.A.; Nemer, F.D.; Goldberg, S.M. Fistula-in-ano in Crohn’s disease. Results of aggressive surgical treatment. Dis. Colon Rectum 1991, 34, 378–384. [Google Scholar] [CrossRef]
- Van der Hagen, S.J.; Baeten, C.G.; Soeters, P.B.; van Gemert, W.G. Long-term outcome following mucosal advancement flap for high perianal fistulas and fistulotomy for low perianal fistulas: Recurrent perianal fistulas: Failure of treatment or recurrent patient disease? Int. J. Colorectal. Dis. 2006, 21, 784–790. [Google Scholar] [CrossRef]
- Mizrahi, N.; Wexner, S.D.; Zmora, O.; Da Silva, G.; Efron, J.; Weiss, E.G.; Vernava, A.M., 3rd; Nogueras, J.J. Endorectal advancement flap: Are there predictors of failure? Dis. Colon Rectum 2002, 45, 1616–1621. [Google Scholar] [CrossRef]
- Sonoda, T.; Hull, T.; Piedmonte, M.R.; Fazio, V.W. Outcomes of primary repair of anorectal and rectovaginal fistulas using the endorectal advancement flap. Dis. Colon Rectum 2002, 45, 1622–1628. [Google Scholar] [CrossRef]
- Sands, B.E.; Anderson, F.H.; Bernstein, C.N.; Chey, W.Y.; Feagan, B.G.; Fedorak, R.N.; Kamm, M.A.; Korzenik, J.R.; Lashner, B.A.; Onken, J.E.; et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N. Engl. J. Med. 2004, 350, 876–885. [Google Scholar] [CrossRef]
- Haennig, A.; Staumont, G.; Lepage, B.; Faure, P.; Alric, L.; Buscail, L.; Bournet, B.; Moreau, J. The results of seton drainage combined with anti-TNFalpha therapy for anal fistula in Crohn’s disease. Colorectal Dis. 2015, 17, 311–319. [Google Scholar] [CrossRef] [PubMed]
- El-Gazzaz, G.; Hull, T.; Church, J.M. Biological immunomodulators improve the healing rate in surgically treated perianal Crohn’s fistulas. Colorectal Dis. 2012, 14, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Schwandner, O.; Stadler, F.; Dietl, O.; Wirsching, R.P.; Fuerst, A. Initial experience on efficacy in closure of cryptoglandular and Crohn’s transsphincteric fistulas by the use of the anal fistula plug. Int. J. Colorectal Dis. 2008, 23, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Van Koperen, P.J.; D’Hoore, A.; Wolthuis, A.M.; Bemelman, W.A.; Slors, J.F. Anal fistula plug for closure of difficult anorectal fistula: A prospective study. Dis. Colon Rectum 2007, 50, 2168–2172. [Google Scholar] [CrossRef]
- Nasseri, Y.; Cassella, L.; Berns, M.; Zaghiyan, K.; Cohen, J. The anal fistula plug in Crohn’s disease patients with fistula-in-ano: A systematic review. Colorectal Dis. 2016, 18, 351–356. [Google Scholar] [CrossRef]
- Senejoux, A.; Siproudhis, L.; Abramowitz, L.; Munoz-Bongrand, N.; Desseaux, K.; Bouguen, G.; Bourreille, A.; Dewit, O.; Stefanescu, C.; Vernier, G.; et al. Fistula Plug in Fistulising Ano-Perineal Crohn’s Disease: A Randomised Controlled Trial. J. Crohns Colitis 2016, 10, 141–148. [Google Scholar] [CrossRef]
- Mennigen, R.; Laukotter, M.; Senninger, N.; Rijcken, E. The OTSC((R)) proctology clip system for the closure of refractory anal fistulas. Tech. Coloproctol. 2015, 19, 241–246. [Google Scholar] [CrossRef]
- Burke, J.P. Role of Fecal Diversion in Complex Crohn’s Disease. Clin. Colon Rectal Surg. 2019, 32, 273–279. [Google Scholar] [CrossRef]
- Bafford, A.C.; Latushko, A.; Hansraj, N.; Jambaulikar, G.; Ghazi, L.J. The Use of Temporary Fecal Diversion in Colonic and Perianal Crohn’s Disease Does Not Improve Outcomes. Digest. Dis. Sci. 2017, 62, 2079–2086. [Google Scholar] [CrossRef]
- Mennigen, R.; Heptner, B.; Senninger, N.; Rijcken, E. Temporary fecal diversion in the management of colorectal and perianal Crohn’s disease. Gastroenterol. Res. Pract. 2015, 2015, 286315. [Google Scholar] [CrossRef] [Green Version]
- Thornton, M.; Solomon, M.J. Long-term indwelling seton for complex anal fistulas in Crohn’s disease. Dis. Colon Rectum 2005, 48, 459–463. [Google Scholar] [CrossRef]
- Van Koperen, P.J.; Wind, J.; Bemelman, W.A.; Bakx, R.; Reitsma, J.B.; Slors, J.F. Long-term functional outcome and risk factors for recurrence after surgical treatment for low and high perianal fistulas of cryptoglandular origin. Dis. Colon Rectum 2008, 51, 1475–1481. [Google Scholar] [CrossRef] [Green Version]
- Makowiec, F.; Jehle, E.C.; Starlinger, M. Clinical course of perianal fistulas in Crohn’s disease. Gut 1995, 37, 696–701. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Heywood, N.; Adegbola, S.; Tozer, P.; Sahnan, K.; Fearnhead, N.S.; Brown, S.R.; Collaborators, E.N. Systematic review of surgical interventions for Crohn’s anal fistula. BJS Open 2017, 1, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.F.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombel, J.F.; Schwartz, D.A.; Sandborn, W.J.; Kamm, M.A.; D’Haens, G.; Rutgeerts, P.; Enns, R.; Panaccione, R.; Schreiber, S.; Li, J.; et al. Adalimumab for the treatment of fistulas in patients with Crohn’s disease. Gut 2009, 58, 940–948. [Google Scholar] [CrossRef] [Green Version]
- Thia, K.T.; Mahadevan, U.; Feagan, B.G.; Wong, C.; Cockeram, A.; Bitton, A.; Bernstein, C.N.; Sandborn, W.J. Ciprofloxacin or metronidazole for the treatment of perianal fistulas in patients with Crohn’s disease: A randomized, double-blind, placebo-controlled pilot study. Inflamm. Bowel Dis. 2009, 15, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, G.; Halligan, S.; Williams, A.; Cohen, C.R.; Tarroni, D.; Phillips, R.K.; Bartram, C.I. Effect of MRI on clinical outcome of recurrent fistula-in-ano. Lancet 2002, 360, 1661–1662. [Google Scholar] [CrossRef]
- Beets-Tan, R.G.; Beets, G.L.; van der Hoop, A.G.; Kessels, A.G.; Vliegen, R.F.; Baeten, C.G.; van Engelshoven, J.M. Preoperative MR imaging of anal fistulas: Does it really help the surgeon? Radiology 2001, 218, 75–84. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n (%) * | ||
|---|---|---|
| age at initial fistula appearance | median | 27 (16–71) ** |
| <20 | 5 (11.1) | |
| 21–30 | 23 (51.1) | |
| 31–40 | 7 (15.6) | |
| 41–50 | 4 (8.9) | |
| 51–60 | 4 (8.9) | |
| >61 | 2 (4.4) | |
| sex | female | 17 (37.8) |
| male | 28 (62.2) | |
| BMI (kg/m2) | median | 24 (17.1–33.2) ** |
| <18.5 | 6 (13.3) | |
| 18.5–24.9 | 24 (53.3) | |
| 25–29.9 | 11 (24.5) | |
| 30–34.9 | 4 (8.9) | |
| >35 | 0 (0) | |
| ASA | ASA 1 | 13 (28.9) |
| ASA 2 | 32 (71.1) | |
| >ASA 3 | 0 (0) | |
| smoking history | yes no | 8 (17.8) 37 (82.2) |
| medication history | steroids | 13 (28.9) |
| azathioprine | 18 (40) | |
| biologicals | 28 (62.2) | |
| surgical history | abdominal IBD surgery | 16 (35.6) |
| proctosurgery | 23 (51.1) | |
| Montreal classification for CD | age at diagnosis (A) | |
| A1, 16 years or younger | 2 (4.4) | |
| A2, 17–40 years | 35 (77.8) | |
| A3, >40 years | 8 (17.8) | |
| location (L) | ||
| L1, terminal ileum | 14 (31.1) | |
| L2, colon | 11 (24.4) | |
| L3, ileocolon | 18 (40.0) | |
| L4, upper GI | 2 (4.4) | |
| behavior (B) | ||
| B1, non-stricturing/penetrating | 0 (0) | |
| B2, stricturing | 0 (0) | |
| B3, penetrating | 0 (0) | |
| perianal disease modifier (p) | ||
| B3p, penetrating + perianal | 45 (100) |
| time interval | n (%) * | months *** |
|---|---|---|
| diagnosis of CD—first fistula surgery | 27 (60) ** | 72 (0–391) |
| first—last fistula surgery | 45 (100) | 18 (0–182) |
| fistula seton drainage—fistula closure surgery | 40 (88.9) | 5 (1–54) |
| last surgery—last follow-up | 45 (100) | 90 (15–200) |
| last fistula closure surgery—surgery for recurrence | 7 (15.5) | 45 (17–111) |
| n (%) * | ||
|---|---|---|
| preoperative examination | perianal abscess | 26 (57.8) |
| anal fissure | 5 (11.1) | |
| proctitis | 5 (11.1) | |
| anorectal stricture | 5 (11.1) | |
| Park´s classification | superficial | 4 (8.9) |
| transsphincteric (low) | 19 (42.2) | |
| transsphincteric (high) | 11 (24.4) | |
| intersphincteric | 3 (6.7) | |
| suprasphincteric | 3 (6.7) | |
| extrasphincteric | 5 (11.1) | |
| AGA classification | complex | 22 (48.9) |
| simple | 23 (51.1) | |
| localization | ventral (10°°–2°°) | 9 (20) |
| dorsal (4°°–8°°) | 27 (60) | |
| horizontal (9°° + 3°°) | 9 (20) | |
| number of fistulas | 1 | 29 (64.4) |
| ≥2 | 16 (35.6) |
| surgical procedures in total | abscess incision | 50 |
| fistula seton drainage | 77 | |
| fistulotomy | 34 | |
| AFP | 18 | |
| OTSC | 7 | |
| mucosa advancement flap | 3 | |
| n (%) * | ||
| surgery for infection control | abscess incision | 26 (57.8) |
| fistula seton drainage | 40 (88.9) | |
| last fistula closure surgery | fistulotomy | 14 (31.1) |
| biologicals + seton removal | 12 (26.7) | |
| AFP | 8 (17.8) | |
| OTSC | 5 (11.1) | |
| fistula seton drainage | 4 (8.9) | |
| mucosa advancement flap | 2 (4.4) | |
| number of attempts to close internal ostium | 0 (=fistulotomy, fistula seton drainage) | 25 (55.6) |
| 1 | 15 (33.3) | |
| 2 | 4 (8.9) | |
| 3 | 1 (2.2) | |
| number of all surgical procedures | mean | 4.2 (1–14) ** |
| surgery under fecal diversion | 2 (4.4) | |
| PDAI before last fistula surgery | median | 8 (1–16) ** |
| n (%) * | ||
|---|---|---|
| persistence | 30 (66.7) * | |
| low fistula | 14 (46.7) | |
| high fistula | 16 (53.3) | |
| complex | 16 (53.3) | |
| ventral (10°°–2°°) | 7 (56.7) | |
| dorsal (4°°–8°°) | 16 (53.3) | |
| horizontal (9°° + 3°°) | 7 (56.7) | |
| multiple fistulas | 13 (43.3) | |
| recurrence | 7 (15.5) * | |
| low fistula | 1 (14.3) | |
| high fistula | 6 (85.7) | |
| complex | 6 (85.7) | |
| ventral (10°°–2°°) | 4 (57.1) | |
| dorsal (4°°–8°°) | 3 (42.9) | |
| multiple fistulas | 2 (28.6) | |
| surgery before recurrence | biologicals + seton removal | 3 (42.9) |
| AFP | 3 (42.9) | |
| fistulotomy | 1 (14.2) | |
| number of surgical procedures after recurrence | mean | 1.86 (1–2) ** |
| final fistula closure surgery after recurrence | OTSC | 4 (57.1) |
| fistulotomy | 1 (14.3) | |
| mucosa advancement flap | 1 (14.3) | |
| biologicals + seton removal | 1 (14.3) | |
| non-success | 9 (20) * | |
| low fistula | 6 (66.7) | |
| high fistula | 3 (33.3) | |
| complex | 3 (33.3) | |
| dorsal (4°°–8°°) | 7 (77.8) | |
| horizontal (9°° + 3°°) | 2 (22.2) | |
| multiple fistulas | 4 (44.4) | |
| last surgery before non-success | fistula seton drainage | 4 (44.4) |
| biologicals + seton removal | 2 (22.2) | |
| fistulotomy | 1 (11.1) | |
| AFP | 1 (11.1) | |
| OTSC | 1 (11.1) | |
| postoperative complications | 3 (6.7) | |
| final success | 36 (80) * | |
| last surgery before success | fistulotomy | 13 (28.9) |
| biologicals + seton removal | 10 (22.2) | |
| AFP | 7 (15.7) | |
| OTSC | 4 (8.9) | |
| mucosa advancement flap | 2 (4.4) |
| factor | persistence n (%) * | p-value | recurrence n (%) * | p-value | primary success n (%) * | p-value | |||
|---|---|---|---|---|---|---|---|---|---|
| yes | no | yes | no | yes | no | ||||
| sex female | 10 (58.8) | 7 (41.2) | 0.384 | 5 (29.4) | 12 (70.6) | 0.046 | 12 (70.6) | 5 (29.4) | 0.219 |
| male | 20 (71.4) | 8 (28.6) | 2 (7.1) | 26 (92.9) | 24 (85.7) | 4 (14.3) | |||
| age at first appearance ≤20 | 1 (20) | 4 (80) | 0.037 | 0 (0) | 5 (100) | 0.812 | 5 (100) | 0 (0) | 0.197 |
| 21–30 | 14 (60.9) | 9 (39.1) | 5 (21.7) | 18 (78.3) | 20 (86.9) | 3 (13.1) | |||
| 31–40 | 7 (100) | 0 (0) | 1 (14.3) | 6 (85.7) | 3 (42.9) | 4 (57.1) | |||
| 41–50 | 3 (75) | 1 (25) | 1 (25) | 3 (75) | 3 (75) | 1 (25) | |||
| 51–60 | 4 (100) | 0 (0) | 0 (0) | 4 (100) | 3 (75) | 1 (25) | |||
| ≥61 | 1 (50) | 1 (50) | 0 (0) | 2 (100) | 2 (100) | 0 (0) | |||
| BMI (kg/m2) ≤18.5 | 3 (50) | 3 (50) | 0.532 | 2 (33.3) | 4 (66.7) | 0.466 | 4 (66.7) | 2 (33.3) | 0.020 |
| 18.5–24.9 | 15 (62.5) | 9 (37.5) | 4 (16.7) | 20 (83.3) | 21 (87.5) | 3 (12.5) | |||
| 25–29.9 | 9 (81.8) | 2 (18.2) | 1 (9.1) | 10 (90.9) | 10 (90.9) | 1 (9.1) | |||
| 30–34.9 | 3 (75) | 1 (25) | 0 (0) | 4 (100) | 1 (25) | 3 (75) | |||
| ≥35 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |||
| Park’s classification superficial | 1 (25) | 3 (75) | 0.032 | 0 (0) | 4 (100) | 0.004 | 3 (75) | 1 (25) | 0.190 |
| low transsphincteric | 13 (68.4) | 6 (31.6) | 1 (5.3) | 18 (94.7) | 14 (73.7) | 5 (26.3) | |||
| high transsphincteric | 9 (81.8) | 2 (18.2) | 6 (54.5) | 5 (45.5) | 10 (90.9) | 1 (9.1) | |||
| intersphincteric | 0 (0) | 3 (100) | 0 (0) | 3 (100) | 3 (100) | 0 (0) | |||
| suprasphincteric | 3 (100) | 0 (0) | 0 (0) | 3 (100) | 1 (33.3) | 2 (66.7) | |||
| extrasphincteric | 4 (80) | 1 (20) | 0 (0) | 5 (100) | 5 (100) | 0 (0) | |||
| AGA classification simple | 14 (60.9) | 9 (39.1) | 0.399 | 1 (4.3) | 22 (95.7) | 0.034 | 17 (73.9) | 6 (26.1) | 0.297 |
| complex | 16 (72.7) | 6 (27.3) | 6 (27.3) | 16 (72.7) | 19 (86.4) | 3 (13.6) | |||
| localization of fistula ventral (10°°–2°°) | 7 (77.8) | 2 (22.2) | 0.435 | 4 (44.4) | 5 (55.6) | 0.020 | 9 (100) | 0 (0) | 0.238 |
| dorsal (4°°–8°°) | 16 (59.3) | 11 (40.7) | 3 (11.1) | 24 (88.9) | 20 (74.1) | 7 (25.9) | |||
| horizontal (9°° + 3°°) | 7 (77.8) | 2 (22.2) | 0 (0) | 9 (100) | 7 (77.8) | 2 (22.2) | |||
| leukocytes at last fistula closure surgery ≤12.680/μL ≥12.680/μL | 23 (63.9) 7 (78.2) | 13 (36.1) 2 (22.2) | 0.429 | 5 (13.9) 2 (22.2) | 31 (86.1) 7 (77.8) | 0.537 | 31 (86.1) 5 (55.6) | 5 (13.9) 4 (44.4) | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merten, J.; Eichelmann, A.-K.; Mennigen, R.; Flammang, I.; Pascher, A.; Rijcken, E. Minor Sphincter Sparing Surgery for Successful Closure of Perianal Fistulas in Patients with Crohn’s Disease. J. Clin. Med. 2021, 10, 4721. https://doi.org/10.3390/jcm10204721
Merten J, Eichelmann A-K, Mennigen R, Flammang I, Pascher A, Rijcken E. Minor Sphincter Sparing Surgery for Successful Closure of Perianal Fistulas in Patients with Crohn’s Disease. Journal of Clinical Medicine. 2021; 10(20):4721. https://doi.org/10.3390/jcm10204721
Chicago/Turabian StyleMerten, Jennifer, Ann-Kathrin Eichelmann, Rudolf Mennigen, Isabelle Flammang, Andreas Pascher, and Emile Rijcken. 2021. "Minor Sphincter Sparing Surgery for Successful Closure of Perianal Fistulas in Patients with Crohn’s Disease" Journal of Clinical Medicine 10, no. 20: 4721. https://doi.org/10.3390/jcm10204721