
From Basic Mechanisms to Clinical Research: Photodynamic Therapy Applications in Head and Neck Malignancies and Vascular Anomalies

Abstract
:1. Introduction
1.1. Head and Neck and PDT
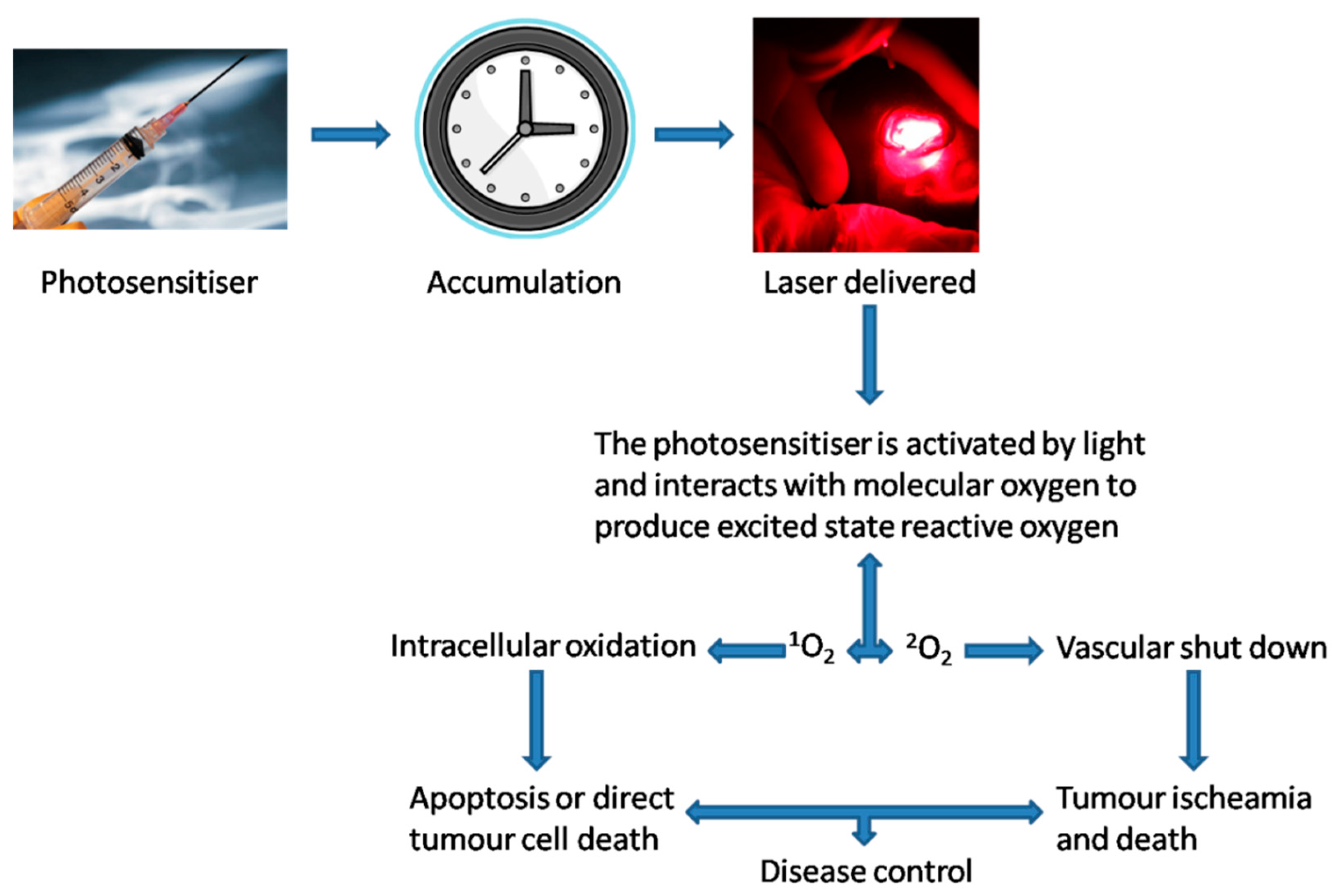
1.2. Theoretical Principles of PDT
1.3. Photosensitisers
1.3.1. First-Generation
1.3.2. Second-Generation
1.3.3. Third-Generation
1.3.4. Specific Type
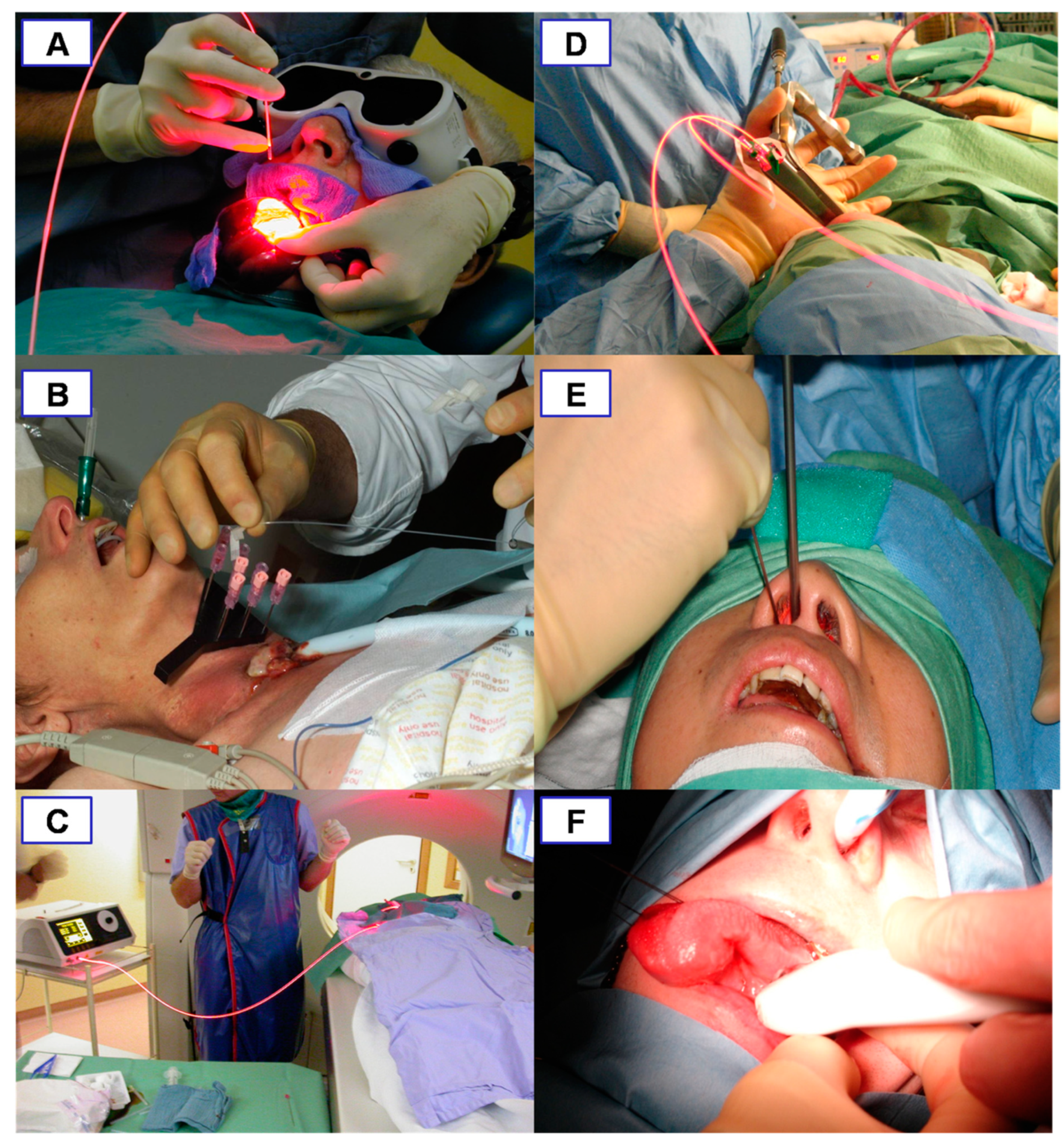
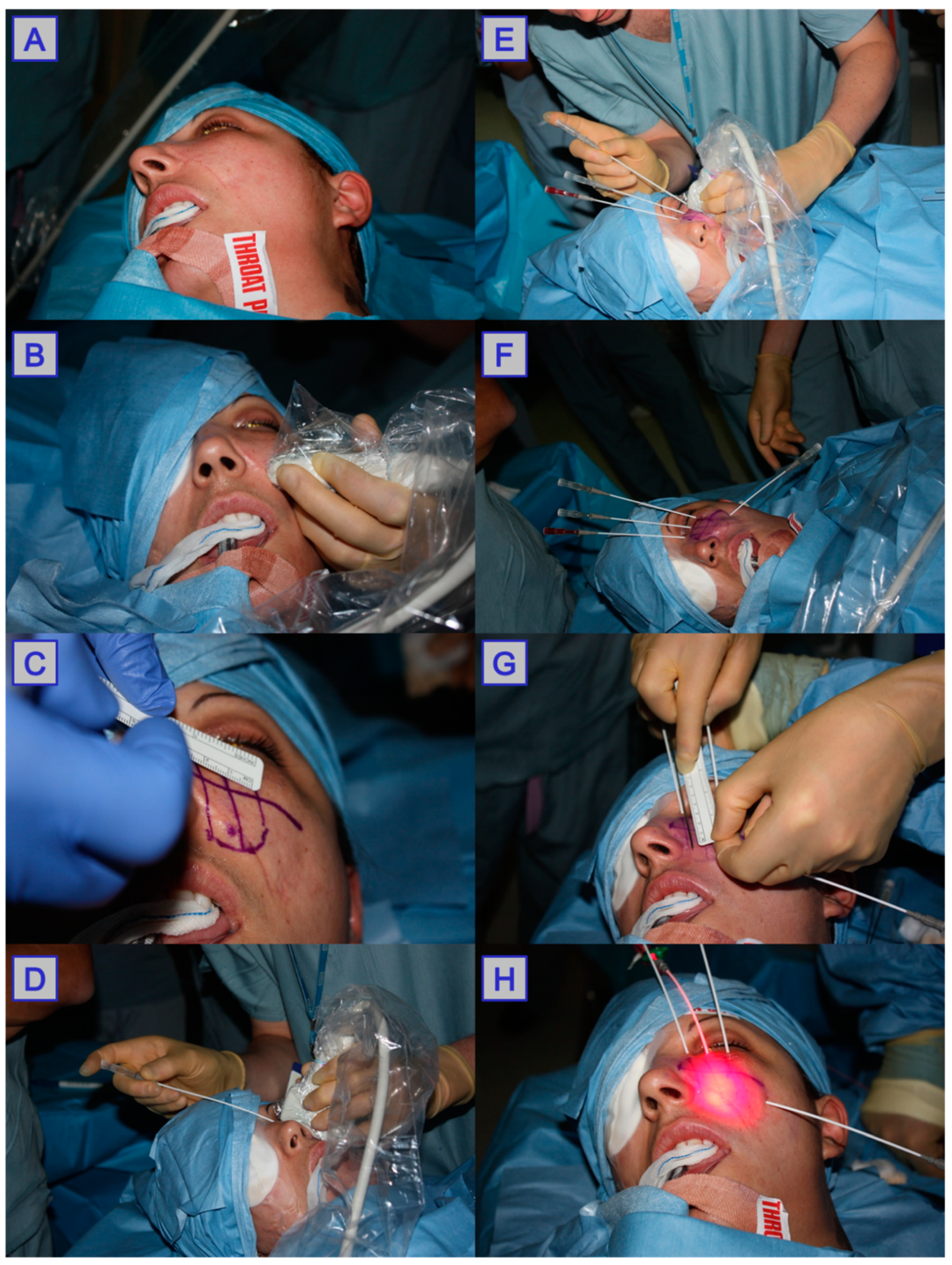
1.4. Delivery of Photodynamic Therapy
1.4.1. Superficial Pathology
1.4.2. Deep-Seated Pathology
1.5. Post Photodynamic Therapy
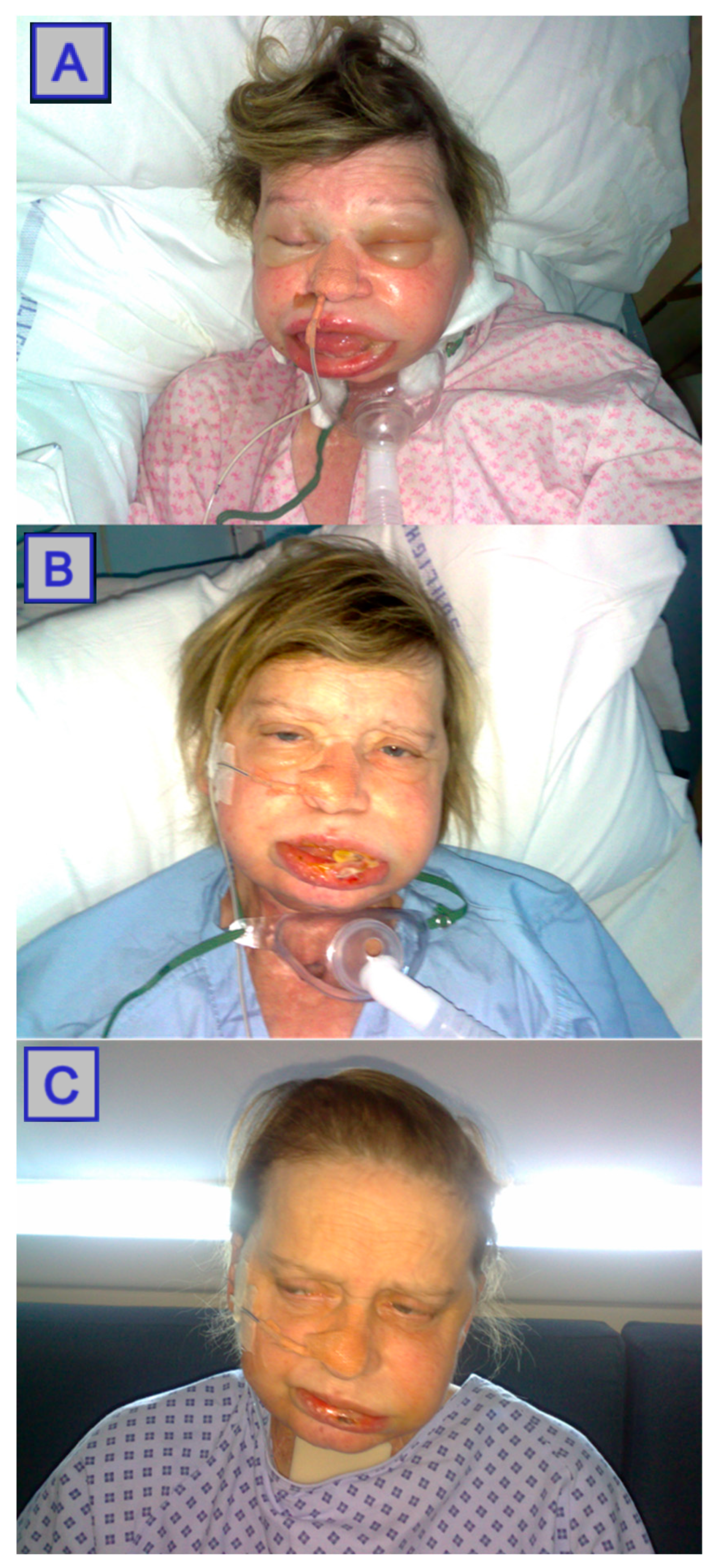
1.5.1. Pain Management and Swelling Control
1.5.2. Residual Systemic Photosensitisation
1.5.3. Assessment of Outcome
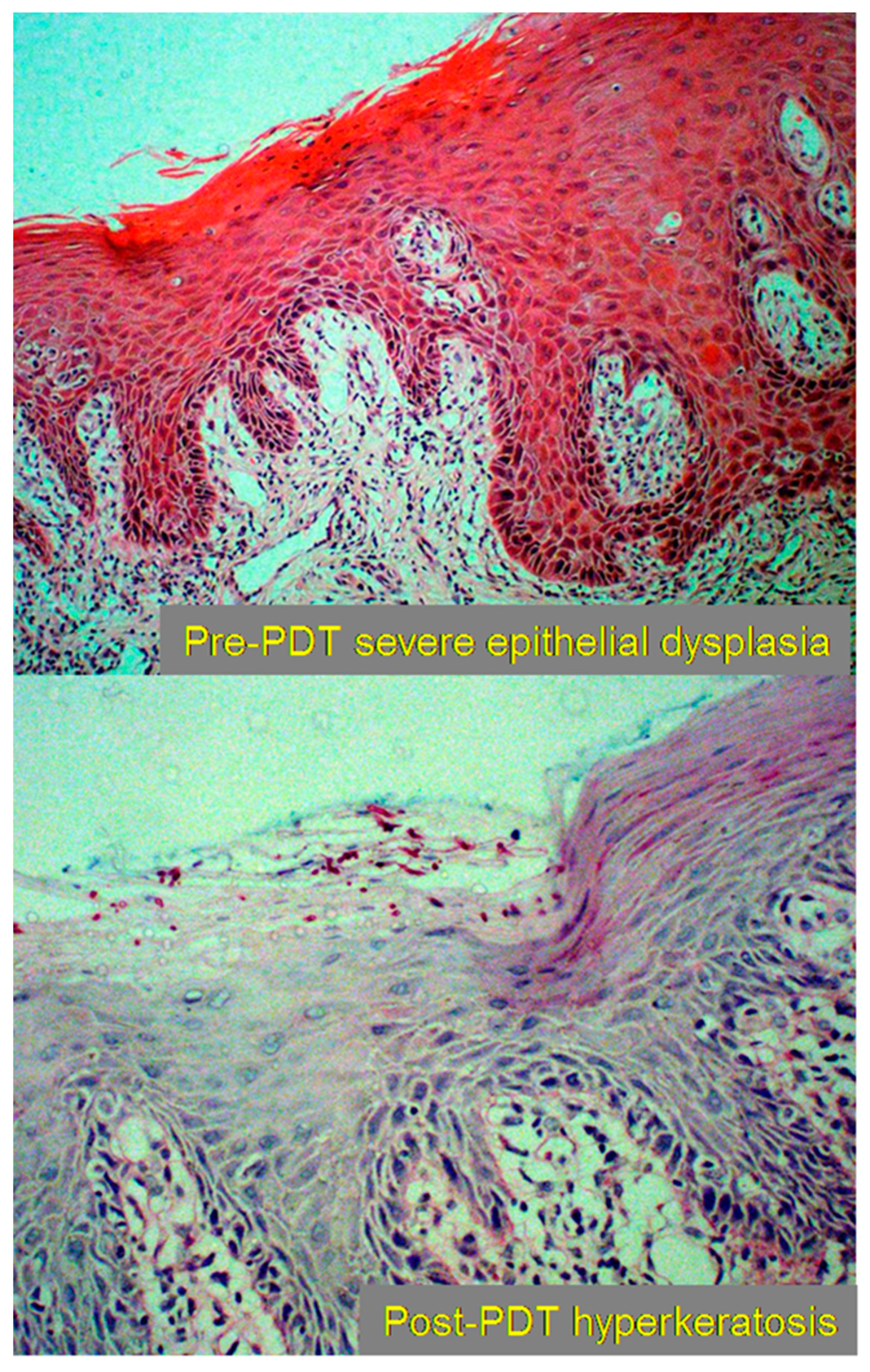
1.6. Tissue Changes
2. Discussion
2.1. Nasopharyngeal Carcinoma
2.2. Oral Cancer
2.3. Oropharyngeal Carcinoma
2.4. Laryngeal Carcinoma
2.5. Vascular Anomalies
3. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patrice, T. (Ed.) Photodynamic Therapy; Royal Society of Chemistry: Cambridge, UK, 2003. [Google Scholar]
- Han, Y.; Chen, Z.; Zhao, H.; Zha, Z.; Ke, W.; Wang, Y.; Ge, Z. Oxygen-independent combined photothermal/photodynamic therapy delivered by tumor acidity-responsive polymeric micelles. J. Control. Release 2018, 284, 15–25. [Google Scholar] [CrossRef]
- Dos Santos, A.; de Almeida, D.; Terra, L.; Baptista, M.; Labriola, L. Photodynamic therapy in cancer treatment-an update review. J. Cancer Metastasis Treat. 2019, 5, 25. [Google Scholar] [CrossRef] [Green Version]
- Horn, M.; Wolf, P.; Wulf, H.; Warloe, T.; Fritsch, C.; Rhodes, L.; Kaufmann, R.; De Rie, M.; Legat, F.; Stender, I.; et al. Topical methyl aminolaevulinate photodynamic therapy in patients with basal cell carcinoma prone to complications and poor cosmetic outcome with conventional treatment. Br. J. Dermatol. 2003, 149, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Nyst, H.; Tan, I.; Stewart, F.; Balm, A. Is photodynamic therapy a good alternative to surgery and radiotherapy in the treatment of head and neck cancer? Photodiagn. Photodyn. Ther. 2009, 6, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Hosokawa, S.; Takebayashi, S.; Takahashi, G.; Okamura, J.; Mineta, H. Photodynamic therapy in patients with head and neck squamous cell carcinoma. Lasers Surg. Med. 2018, 50, 420–426. [Google Scholar] [CrossRef]
- Hosokawa, S.; Takahashi, G.; Sugiyama, K.; Takebayashi, S.; Okamura, J.; Takizawa, Y.; Mineta, H. Porfimer sodium-mediated photodynamic therapy in patients with head and neck squamous cell carcinoma. Photodiagn. Photodyn. Ther. 2020, 29, 101627. [Google Scholar] [CrossRef]
- Ahn, P.; Quon, H.; O’Malley, B.; Weinstein, G.; Chalian, A.; Malloy, K.; Atkins, J.; Sollecito, T.; Greenberg, M.; McNulty, S.; et al. Toxicities and early outcomes in a phase 1 trial of photodynamic therapy for premalignant and early stage head and neck tumors. Oral Oncol. 2016, 55, 37–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, A.; Nees, L.; Nuyts, S.; Clement, P.; Meulemans, J.; Delaere, P.; Poorten, V.V. Photodynamic Therapy as an Alternative Therapeutic Tool in Functionally Inoperable Oral and Oropharyngeal Carcinoma: A Single Tertiary Center Retrospective Cohort Analysis. Front. Oncol. 2021, 11, 518. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Akram, S.; Hopper, C. The surgical palliation of advanced head and neck cancer using photodynamic therapy. Clin. Oncol. 2010, 22, 785–791. [Google Scholar] [CrossRef]
- Van Straten, D.; Mashayekhi, V.; De Bruijn, H.; Oliveira, S.; Robinson, D. Oncologic Photodynamic Therapy: Basic Principles, Current Clinical Status and Future Directions. Cancers 2017, 9, 19. [Google Scholar] [CrossRef]
- Dysart, J.; Patterson, M. Characterization of Photofrin photobleaching for singlet oxygen dose estimation during photodynamic therapy of MLL cells in vitro. Phys. Med. Biol. 2005, 50, 2597. [Google Scholar] [CrossRef] [PubMed]
- Mroz, P.; Yaroslavsky, A.; Kharkwal, G.; Hamblin, M. Cell death pathways in photodynamic therapy of cancer. Cancers 2011, 3, 2516–2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, Y.-J.; Wu, C.-C.; Chang, C.-J.; Yu, J.-S. Subcellular localization of Photofrin® determines the death phenotype of human epidermoid carcinoma A431 cells triggered by photodynamic therapy: When plasma membranes are the main targets. J. Cell. Physiol. 2003, 194, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Castano, A.; Mroz, P.; Hamblin, M. Photodynamic therapy and anti-tumour immunity. Nat. Rev. Cancer 2006, 6, 535–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, H.; Nakamura, H.; Fang, J. The EPR effect for macromolecular drug delivery to solid tumors: Improvement of tumor uptake, lowering of systemic toxicity, and distinct tumor imaging in vivo. Adv. Drug Deliv. Rev. 2013, 65, 71–79. [Google Scholar] [CrossRef]
- Grant, W.E.; Speight, P.M.; Hopper, C.; Bown, S.G. Photodynamic therapy: An effective, but non-selective treatment for superficial cancers of the oral cavity. Int. J. Cancer 1997, 71, 937–942. [Google Scholar] [CrossRef]
- Kubler, A.; Hasse, T.; Staff, C.; Kahle, B.; Rheinwald, M.; Muhling, J. Photodynamic therapy of primary nonmelanomatous skin tumours of the head and neck. Lasers Surg. Med. 1999, 25, 60–68. [Google Scholar] [CrossRef]
- Hopper, C. Photodynamic therapy: A clinical reality in the treatment of cancer. Lancet Oncol. 2000, 1, 212–219. [Google Scholar] [CrossRef]
- Li, X.; Lovell, J.F.; Yoon, J.; Chen, X. Clinical development and potential of photothermal and photodynamic therapies for cancer. Nat. Rev. Clin. Oncol. 2020, 17, 657–674. [Google Scholar] [CrossRef]
- Triesscheijn, M.; Baas, P.; Schellens, J.; Stewart, F. Photodynamic Therapy in Oncology. Oncologist 2006, 11, 1034–1044. [Google Scholar] [CrossRef]
- Chilakamarthi, U.; Giribabu, L. Photodynamic Therapy: Past, Present and Future. Chem. Rec. 2017, 17, 775–802. [Google Scholar] [CrossRef]
- Minnich, D.J.; Bryant, A.; Dooley, A.; Cerfolio, R. Photodynamic Laser Therapy for Lesions in the Airway. Ann. Thorac. Surg. 2010, 89, 1744–1749. [Google Scholar] [CrossRef]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kedzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy—Mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef]
- Kataoka, H.; Nishie, H.; Hayashi, N.; Tanaka, M.; Nomoto, A.; Yano, S.; Joh, T. New photodynamic therapy with next-generation photosensitizers. Ann. Transl. Med. 2017, 5, 183. [Google Scholar] [CrossRef] [Green Version]
- Selbo, P.; Bostad, M.; Olsen, C.; Edwards, V.; Hogset, A.; Weyergang, A.; Berg, K. Photochemical internalisation, a minimally invasive strategy for light-controlled endosomal escape of cancer stem cell-targeting therapeutics. Photochem. Photobiol. Sci. 2015, 14, 1433–1450. [Google Scholar] [CrossRef]
- Lou, P.; Jäger, H.; Jones, L.; Theodossy, T.; Bown, S.; Hopper, C. Interstitial photodynamic therapy as salvage treatment for recurrent head and neck cancer. Br. J. Cancer 2004, 91, 441–446. [Google Scholar] [CrossRef]
- Gubarkova, E.; Feldchtein, F.; Zagaynova, E.; Gamayunov, S.; Sirotkina, M.; Sedova, E.; Kuznetsov, S.; Moiseev, A.; Matveev, L.; Zaitsev, V.; et al. Optical coherence angiography for pre-treatment assessment and treatment monitoring following photodynamic therapy: A basal cell carcinoma patient study. Sci. Rep. 2019, 9, 18670. [Google Scholar] [CrossRef]
- Navarrete-Dechent, C.; Aleissa, S.; Cordova, M.; Liopyris, K.; Sahu, A.; Rossi, A.; Lee, E.; Nehal, K. Management of complex head-and-neck basal cell carcinomas using a combined reflectance confocal microscopy/optical coherence tomography: A descriptive study. Arch. Dermatol. Res. 2021, 313, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Sirotkina, M.A.; Matveev, L.; Shirmanova, M.V.; Zaitsev, V.; Buyanova, N.L.; Elagin, V.; Gelikonov, G.V.; Kuznetsov, S.S.; Kiseleva, E.B.; Moiseev, A.A.; et al. Photodynamic therapy monitoring with optical coherence angiography. Sci. Rep. 2017, 7, 41506. [Google Scholar] [CrossRef] [Green Version]
- Jerjes, W.; Hamdoon, Z.; Hopper, C. Photodynamic therapy in the management of potentially malignant and malignant oral disorders. Head Neck Oncol. 2012, 4, 16. [Google Scholar] [CrossRef] [Green Version]
- D’Cruz, A.K.; Robinson, M.H.; Biel, M.A. mTHPC-mediated photodynamic therapy in patients with advanced, incurable head and neck cancer: A multicenter study of 128 patients. Head Neck 2004, 26, 232–240. [Google Scholar] [CrossRef]
- Civantos, F.J.; Karakullukcu, B.; Biel, M.; Silver, C.E.; Rinaldo, A.; Saba, N.F.; Takes, R.P.; Poorten, V.V.; Ferlito, A. A Review of Photodynamic Therapy for Neoplasms of the Head and Neck. Adv. Ther. 2018, 35, 324–340. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Mosse, C.A.; Hamdoon, Z.; Morcos, M.; Morley, S.; Hopper, C. Prospective evaluation of 110 patients following ultrasound-guided photodynamic therapy for deep seated pathologies. Photodiagn. Photodyn. Ther. 2011, 8, 297–306. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Mosse, C.A.; Akram, S.; Morley, S.; Hopper, C. Interstitial PDT for vascular anomalies. Lasers Surg. Med. 2011, 43, 357–365. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Mosse, C.A.; Morcos, M.; Hopper, C. Photodynamic therapy outcome for T1/T2 N0 oral squamous cell carcinoma. Lasers Surg. Med. 2011, 43, 463–469. [Google Scholar] [CrossRef]
- Karakullukcu, B.; Nyst, H.; van Veen, R.; Hoebers, F.; Hamming-Vrieze, O.; Witjes, M.; de Visscher, S.; Burlage, F.; Levendag, P.; Sterenborg, H.; et al. mTHPC mediated interstitial photodynamic therapy of recurrent nonmetastatic base of tongue cancers: Development of a new method. Head Neck 2012, 34, 1597–1606. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Abbas, S.; Vincent, A.; Hopper, C. The developing role of photodynamic therapy in multidisciplinary oncological care. Oncol. News. 2008, 3, 12–15. [Google Scholar]
- Abbas, S.; Jerjes, W.; Upile, T.; Vaz, F.; Hopper, C. The palliative role of PDT in recurrent advanced nasopharyngeal carcinoma: Case series. Photodiagn. Photodyn. Ther. 2012, 9, 142–147. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Nhembe, F.; Bhandari, R.; Mackay, S.; Shah, P.; Mosse, C.A.; As Brookes, J.; Morley, S.; et al. Ultrasound-guided photodynamic therapy for deep seated pathologies: Prospective study. Lasers Surg. Med. 2009, 41, 612–621. [Google Scholar] [CrossRef]
- Weymuller, E.; Yueh, B.; Deleyiannis, F.; Kuntz, A.; Alsarraf, R.; Coltrera, M. Quality of life in patients with head and neck cancer: Lessons learned from 549 prospectively evaluated patients. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 329–335. [Google Scholar] [CrossRef] [Green Version]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Abbas, S.; Akram, S.; Mosse, C.A.; Morley, S.; Hopper, C. Photodynamic therapy: The minimally invasive surgical intervention for advanced and/or recurrent tongue base carcinoma. Lasers Surg. Med. 2011, 43, 283–292. [Google Scholar] [CrossRef]
- Hamdoon, Z.; Jerjes, W.; Upile, T.; Akram, S.; Hopper, C. Metastatic renal cell carcinoma to the orofacial region: A novel method to alleviate symptoms and control disease progression. Photodiagn. Photodyn. Ther. 2010, 7, 246–250. [Google Scholar] [CrossRef]
- Biel, M.A. Photodynamic therapy treatment of early oral and laryngeal cancers. Photochem. Photobiol. 2007, 83, 1063–1068. [Google Scholar] [CrossRef]
- Truchuelo, M.; Fernández-Guarino, M.; Fleta, B.; Alcántara, J.; Jaén, P. Effectiveness of photodynamic therapy in Bowen’s disease: An observational and descriptive study in 51 lesions. J. Eur. Acad. Dermatol. Venereol. 2011, 26, 868–887. [Google Scholar] [CrossRef]
- Busch, T.M. Local physiological changes during photodynamic therapy. Lasers Surg. Med. 2006, 38, 494–499. [Google Scholar] [CrossRef]
- Jerjes, W.; Hopper, C. Guidelines on Clinical Management. In Biomedical Optics in Otorhinolaryngology; Springer: New York, NY, USA, 2016; pp. 337–358. [Google Scholar]
- Bobrov, N.; Čavarga, I.; Longauer, F.; Rybárová, S.; Fedoročko, P.; Brezáni, P.; Miškovský, P.; Mirossay, L.; Štubňa, J. Histomorphological changes in murine fibrosarcoma after hypericin-based photodynamic therapy. Phytomedicine 2007, 14, 172–178. [Google Scholar] [CrossRef]
- Biel, M. Photodynamic therapy and the treatment of neoplastic diseases of the larynx. Laryngoscope 1994, 104, 399–403. [Google Scholar] [CrossRef]
- Jerjes, W.; Upile, T.; Hamdoon, Z.; Mosse, C.A.; Akram, S.; Hopper, C. Photodynamic therapy outcome for oral dysplasia. Lasers Surg. Med. 2011, 43, 192–199. [Google Scholar] [CrossRef]
- Cao, S.-M.; Simons, M.J.; Qian, C.-N. The prevalence and prevention of nasopharyngeal carcinoma in China. Chin. J. Cancer 2011, 30, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.C.; Yuan, J.-M. Epidemiology of nasopharyngeal carcinoma. Semin. Cancer Biol. 2002, 12, 421–429. [Google Scholar] [CrossRef]
- Sun, L.; Wang, Y.; Shi, J.; Zhu, W.; Wang, X. Association of Plasma Epstein-Barr Virus LMP1 and EBER1 with Circulating Tumor Cells and the Metastasis of Nasopharyngeal Carcinoma. Pathol. Oncol. Res. 2020, 26, 1893–1901. [Google Scholar] [CrossRef]
- Shah, A.B.; Zulfiqar, H.; Nagalli, S. Nasopharyngeal Carcinoma. January 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554588/ (accessed on 1 August 2021).
- Blanchard, P.; Nguyen, F.; Moya-Plana, A.; Pignon, J.P.; Even, C.; Bidault, F.; Temam, S.; Ruffier, A.; Tao, Y. New developments in the management of nasopharyngeal carcinoma. Cancer Radiother. 2018, 22, 492–495. [Google Scholar] [CrossRef]
- Liu, J.; Yu, H.; Sun, X.; Wang, D.; Gu, Y.; Liu, Q.; Wang, H.; Han, W.; Fry, A. Salvage endoscopic nasopharyngectomy for local recurrent or residual nasopharyngeal carcinoma: A 10-year experience. Int. J. Clin. Oncol. 2017, 22, 834–842. [Google Scholar] [CrossRef]
- Sun, Z. Photodynamic therapy of nasopharyngeal carcinoma by argon or dye laser—An analysis of 137 cases. Zhonghua Zhong Liu Za Zhi 1992, 14, 290–292. [Google Scholar]
- Nyst, H.; Wildeman, M.; Indrasari, S.; Karakullukcu, B.; van Veen, R.; Adham, M.; Stewart, F.; Levendag, P.; Sterenborg, H.; Tan, I. Temoporfin mediated photodynamic therapy in patients with local persistent and recurrent nasopharyngeal carcinoma after curative radiotherapy: A feasibility study. Photodiagn. Photodyn. Ther. 2012, 9, 274–281. [Google Scholar] [CrossRef]
- Succo, G.; Rosso, S.; Fadda, G.L.; Fantini, M.; Crosetti, E. Salvage photodynamic therapy for recurrent nasopharyngeal carcinoma. Photodiagn. Photodyn. Ther. 2014, 11, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Stoker, S.; Indrasari, S.; Herdini, C.; Hariwiyanto, B.; Dhamiyati, W.; Widayati, K.; Romdhoni, A.; Fles, R.; Haryana, S.; Wildeman, M.A.M.; et al. Photodynamic therapy as salvage therapy for patients with nasopharyngeal carcinoma experiencing local failures following definitive radiotherapy. Photodiagn. Photodyn. Ther. 2015, 12, 519–525. [Google Scholar] [CrossRef]
- Yow, C.M.N.; Chen, J.Y.; Mak, N.K.; Cheung, N.H.; Leung, A.W.N. Cellular uptake, subcellular localization and photodamaging effect of temoporfin (mTHPC) in nasopharyngeal carcinoma cells: Comparison with hematoporphyrin derivative. Cancer Lett. 2000, 157, 123–131. [Google Scholar] [CrossRef]
- Feller, L.; Lemmer, J. Oral squamous cell carcinoma: Epidemiology, clinical presentation and treatment. J. Cancer Ther. 2012, 3, 263–268. [Google Scholar] [CrossRef] [Green Version]
- Markopoulos, A.K. Current Aspects on Oral Squamous Cell Carcinoma. Open Dent. J. 2012, 6, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Bagan, J. Oral squamous cell carcinoma overview. Oral Oncol. 2009, 45, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Pagedar, N.A.; Gilbert, R.W. Selective neck dissection: A review of the evidence. Oral Oncol. 2009, 45, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S. Quality of life for head and neck cancer patients–has treatment planning altered? Oral Oncol. 2009, 45, 435–439. [Google Scholar] [CrossRef]
- Wang, X.; Li, N.; Meng, J.; Wen, N. The use of topical ALA-photodynamic therapy combined with induction chemotherapy for locally advanced oral squamous cell carcinoma. Am. J. Otolaryngol. 2021, 42, 103112. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, H.; Tobita, T.; Ohba, S.; Uehara, M.; Asahina, I. Treatment outcome of Photofrin-based photodynamic therapy for T1 and T2 oral squamous cell carcinoma and dysplasia. Photodiagn. Photodyn. Ther. 2013, 10, 229–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Ni, G.; Ding, T.; Lei, S.; Zhong, L.; Liu, N.; Pan, K.; Chen, T.; Zeng, X.; Xu, H.; et al. Photodynamic Therapy for Oral Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Int. J. Photoenergy 2021, 2021, 1–14. [Google Scholar] [CrossRef]
- de Visscher, S.A.H.J.; Melchers, L.J.; Dijkstra, P.U.; Karakullukcu, B.; Tan, I.B.; Hopper, C.; Roodenburg, J.L.N.; Witjes, M.J.H. mTHPC-mediated photodynamic therapy of early stage oral squamous cell carcinoma: A comparison to surgical treatment. Ann. Surg. Oncol. 2013, 20, 3076–3082. [Google Scholar] [CrossRef]
- Alekseeva, P.; Efendiev, K.; Shiryaev, A.; Rusakov, M.; Simonova, M.; Samoylova, S.; Fatyanova, A.; Reshetov, I.; Loschenov, V. Sublingual administration of 5-aminolevulinic acid for laser-induced photodiagnostics and photodynamic therapy of oral cavity and larynx cancers. Photodiagn. Photodyn. Ther. 2021, 34, 102289. [Google Scholar] [CrossRef]
- Cohan, D.; Popat, S.; Kaplan, S.; Rigual, N.; Loree, T.; Hicks, W.L., Jr. Oropharyngeal cancer: Current understanding and management. Curr. Opin. Otolaryngol. Head Neck Surg. 2009, 17, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- Machiels, J.; Leemans, C.R.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef]
- D’souza, G.; McNeel, T.; Fakhry, C. Understanding personal risk of oropharyngeal cancer: Risk-groups for oncogenic oral HPV infection and oropharyngeal cancer. Ann. Oncol. 2017, 28, 3065–3069. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Issaeva, N.; Yarbrough, W. HPV-driven oropharyngeal cancer: Current knowledge of molecular biology and mechanisms of carcinogenesis. Cancers Head Neck 2018, 3, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baskin, R.; Boyce, B.; Amdur, R.; Mendenhall, W.; Hitchcock, K.; Silver, N.; Dziegielewski, P. Transoral robotic surgery for oropharyngeal cancer: Patient selection and special considerations. Cancer Manag. Res. 2018, 10, 839. [Google Scholar] [CrossRef] [Green Version]
- Golusiński, W.; Golusińska-Kardach, E. Current role of surgery in the management of oropharyngeal cancer. Front. Oncol. 2019, 9, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karakullukcu, B.; Van Oudenaarde, K.; Copper, M.P.; Klop, W.M.C.; Van Veen, R.; Wildeman, M.; Tan, I.B. Photodynamic therapy of early stage oral cavity and oropharynx neoplasms: An outcome analysis of 170 patients. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerjes, W.; Upile, T.; Vincent, A.; Abbas, S.; Shah, P.; Mosse, C.A.; McCarthy, E.; El-Maaytah, M.; Topping, W.; Morley, S.; et al. Management of deep-seated malformations with photodynamic therapy: A new guiding imaging modality. Lasers Med. Sci. 2009, 24, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Hamdoon, Z.; Jerjes, W.; Upile, T.; Hoonjan, P.; Hopper, C. Endoluminal carotid stenting prior to photodynamic therapy to pericarotid malignant disease: Technical advance. Photodiagnosis Photodyn. Ther. 2010, 7, 126–128. [Google Scholar] [CrossRef]
- Baird, B.J.; Sung, C.K.; Beadle, B.M.; Divi, V. Treatment of early-stage laryngeal cancer: A comparison of treatment options. Oral Oncol. 2018, 87, 8–16. [Google Scholar] [CrossRef]
- Rigual, N.R.; Thankappan, K.; Cooper, M.; Sullivan, M.A.; Dougherty, T.; Popat, S.R.; Loree, T.R.; Biel, M.A.; Henderson, B. Photodynamic Therapy for Head and Neck Dysplasia and Cancer. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 784–788. [Google Scholar] [CrossRef] [Green Version]
- Von Beckerath, M.P.; Reizenstein, J.A.; Berner, A.L.; Nordqvist, K.W.; Landström, F.J.; Löfgren, A.L.; Möller, C.G. Outcome of primary treatment of early laryngeal malignancies using photodynamic therapy. Acta Oto-Laryngol. 2014, 134, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Shafirstein, G.; Rigual, N.R.; Arshad, H.; Cooper, M.T.; Bellnier, D.A.; Wilding, G.; Tan, W.; Merzianu, M.; Henderson, B.W. Photodynamic therapy with 3-(1′-hexyloxyethyl) pyropheophorbide-a for early-stage cancer of the larynx: Phase Ib study. Head Neck 2016, 38, e377–e383. [Google Scholar] [CrossRef] [PubMed]
- Nhembe, F.; Jerjes, W.; Upile, T.; Hamdoon, Z.; Vaz, F.; Hopper, C. Subglottic carcinoma treated with surgery and adjuvant photodynamic therapy. Photodiagnosis Photodyn. Ther. 2010, 7, 284–287. [Google Scholar] [CrossRef]
- Cox, J.A.; Bartlett, E.; Lee, E.I. Vascular Malformations: A Review. Semin. Plast. Surg. 2014, 28, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Hamdoon, Z.; Jerjes, W.; Upile, T.; Akram, S.; Hopper, C. Cystic hygroma treated with ultrasound guided interstitial photodynamic therapy: Case study. Photodiagnosis Photodyn. Ther. 2010, 7, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Gao, K.; Huang, Z.; Yuan, K.-H.; Zhang, B.; Hu, Z.-Q. Side-by-side comparison of photodynamic therapy and pulsed-dye laser treatment of port-wine stain birthmarks. Br. J. Dermatol. 2013, 168, 1040–1046. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhou, Z.; Zhou, G.; Tu, P.; Zheng, Q.; Tao, J.; Gu, Y.; Zhu, X. Efficacy and safety of hemoporfin in photodynamic therapy for port-wine stain: A multicenter and open-labeled phase IIa study. Photodermatol. Photoimmunol. Photomed. 2011, 27, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Tu, P.; Zhou, G.; Yang, H.; Zhou, Z.; Zhao, Y.; Zheng, Q.; Gu, Y.; Tao, J.; Zhu, X. A dose-finding study for hemoporfin in photodynamic therapy for port-wine stain: A multicenter randomized double-blind phase IIb trial. Photodermatol. Photoimmunol. Photomed. 2018, 34, 314–321. [Google Scholar] [CrossRef]
- Zhao, Y.; Tu, P.; Zhou, G.; Zhou, Z.; Lin, X.; Yang, H.; Lu, Z.; Gao, T.; Tu, Y.; Xie, H.; et al. Hemoporfin Photodynamic Therapy for Port-Wine Stain: A Randomized Controlled Trial. PLoS ONE 2016, 11, e0156219. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Year of Publication | Number of Patients | Photo-Sensitiser | Photosensitiser Dose | Results at the End of Follow Up (Mean Follow-Up Time) |
|---|---|---|---|---|
| Abbas et al., 2012 [39] | 7 (2 stage III, 5 stage IV) | m-THPC | 0.15 mg/kg, drug-light interval 96 h | 5 died (3 tumour related), 2 alive (36 months) |
| Nyst et al., 2012 [58] | 22 | m-THPC | n = 8: 0.15 mg/kg, drug-light interval 96 h n = 7: 0.10 mg/kg, drug-light interval 48 h n = 7 0.075 mg/kg, drug-light interval 24 h | 7 out of 8 patients who received the recommended dose survived (37.8 months) (1 died of pneumonia 2 days post-PDT). 6 out of 7 who received 0.1 mg/kg PS died (3 related to disease, 1 of unknown cause and 2 unrelated to disease). 3 out of 7 receiving 0.075 mg/kg PS died (all due to disease). Overall survival 55% at 3 years 100% complete response *. |
| Succo et al., 2014 [59] | 6 | m-THPC | 0.15 mg/kg, drug-light interval 96 h | 2 died (disease-related), 1 alive with disease, 3 disease-free (24–71 months of follow-up). |
| Stoker et al., 2015 [60] | 21 | m-THPC | 0.15 mg/kg, drug-light interval 96 h | 10 died, 2 alive with disease and 9 alive and disease-free (32 months). |
| Study | Number of Patients | Photosensitiser | Dose | Response (At the End of Follow-Up) | ||
|---|---|---|---|---|---|---|
| CR | PR | NR | ||||
| Wang et al., 2021 [67] | 11 | 5-aminolevulinic acid (5-ALA) | 10% cream | 7 | 3 | 1 |
| Jerjes et al., 2011 [36] | 38 | Meso-tetrahydroxyphenyl chlorin (mTHPC) | 0.15 mg/kg | 26 | ||
| Ikeda et al., 2013 [68] | 25 | Photofrin® | 2 mg/kg | 24 | 1 | 0 |
| Study | Number of Patients | Photosensitiser | Dose | Response (At the End of Follow-Up) * | ||
|---|---|---|---|---|---|---|
| CR | PR | NR | ||||
| Lambert et al., 2021 [9] | 26 | mTHPC | 0.15 mg/kg | 20 | 3 | 3 |
| Karakullukcu et al., 2011 [79] | 170 | mTHPC | 0.15 mg/kg | 119 | 36 | 15 |
| Jerjes et al., 2011 [42] | 21 | mTHPC | 0.15 mg/kg | 2 | 13 | 6 |
| Study | Number of Patients | Photosensitiser | Dose | Response (At the End of Follow-Up) * | ||
|---|---|---|---|---|---|---|
| CR | PR | NR | ||||
| Biel [44] | 115 | Photofrin ® | 2 mg/kg | 105 | 10 | 0 |
| Rigual et al. [83] | 6 | Photofrin ® | 2 mg/kg | 5 | 0 | 1 |
| Von Beckerath et al. [84] | 10 | Photofrin ® (n = 2), temoporfin (n = 7), both (n = 1) | Photofrin 2 mg/kg or 5 mg/kg Temoporfin 0.15 mg/kg | 7 | 3 | 0 |
| Shafirstein et al. [85] | 29 (30 lesions) | HPPH | 4 mg/m2 | 20 | 6 | 4 ** |
| Hosokawa et al. [6] | 10 | Photofrin ® | 2 mg/kg | 9 | 1 | 0 |
| Study and Year of Publication | Number of Patients | Photo-Sensitiser | Results |
|---|---|---|---|
| Jerjes et al., 2011 [37] | 43 | m-THPC | Radiological assessment (MRI) taken 5–6 weeks post-PDT showed 15 significant responses, 11 moderate responses, 12 minimal responses, 4 no change with stable disease, 1 progressive disease **. |
| Zhao et al., 2011 [90] * | 39 | Hemoporfin | 26 patients showed significant response; 8 showed response to PDT treatment *** |
| Gao et al., 2013 [89] * | 15 | Hemoporfin | 9 red-coloured CMs showed 11–24% blanching rate after a single session of PDL compared to 22–55% for PDT. 6 purple-coloured CMs showed 8–33% improvement after PDL compared to 30–45% for PDT. |
| Zhao et al., 2016 [92] * | 440 | Hemoporfin | 89.7% of the PDT group showed at least some improvement, compared to 24.5% of the placebo group. |
| Wu et al., 2018 [91] * | 100 | Hemoporfin | Primary efficacy assessment revealed that for the high-dose group, 30/40 patients (75%) showed at least some improvement, with 16/40 (40%) showing at least great improvement. This compares with 16 (40%) and 1 (2.5%) out of 40 for the low dose group, respectively. In the control group, 3/20 patients (15%) showed some improvement, with 17/20 (85%) showing no improvement. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramsay, D.; Stevenson, H.; Jerjes, W. From Basic Mechanisms to Clinical Research: Photodynamic Therapy Applications in Head and Neck Malignancies and Vascular Anomalies. J. Clin. Med. 2021, 10, 4404. https://doi.org/10.3390/jcm10194404
Ramsay D, Stevenson H, Jerjes W. From Basic Mechanisms to Clinical Research: Photodynamic Therapy Applications in Head and Neck Malignancies and Vascular Anomalies. Journal of Clinical Medicine. 2021; 10(19):4404. https://doi.org/10.3390/jcm10194404
Chicago/Turabian StyleRamsay, Daniele, Harvey Stevenson, and Waseem Jerjes. 2021. "From Basic Mechanisms to Clinical Research: Photodynamic Therapy Applications in Head and Neck Malignancies and Vascular Anomalies" Journal of Clinical Medicine 10, no. 19: 4404. https://doi.org/10.3390/jcm10194404