
Impact of Different Approaches to Kidney Transplant with and without Chronic Hemodialysis on Cardiac Function and Morphology: A Case–Control Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Echocardiography
2.3. Conventional and Tissue Doppler Imaging
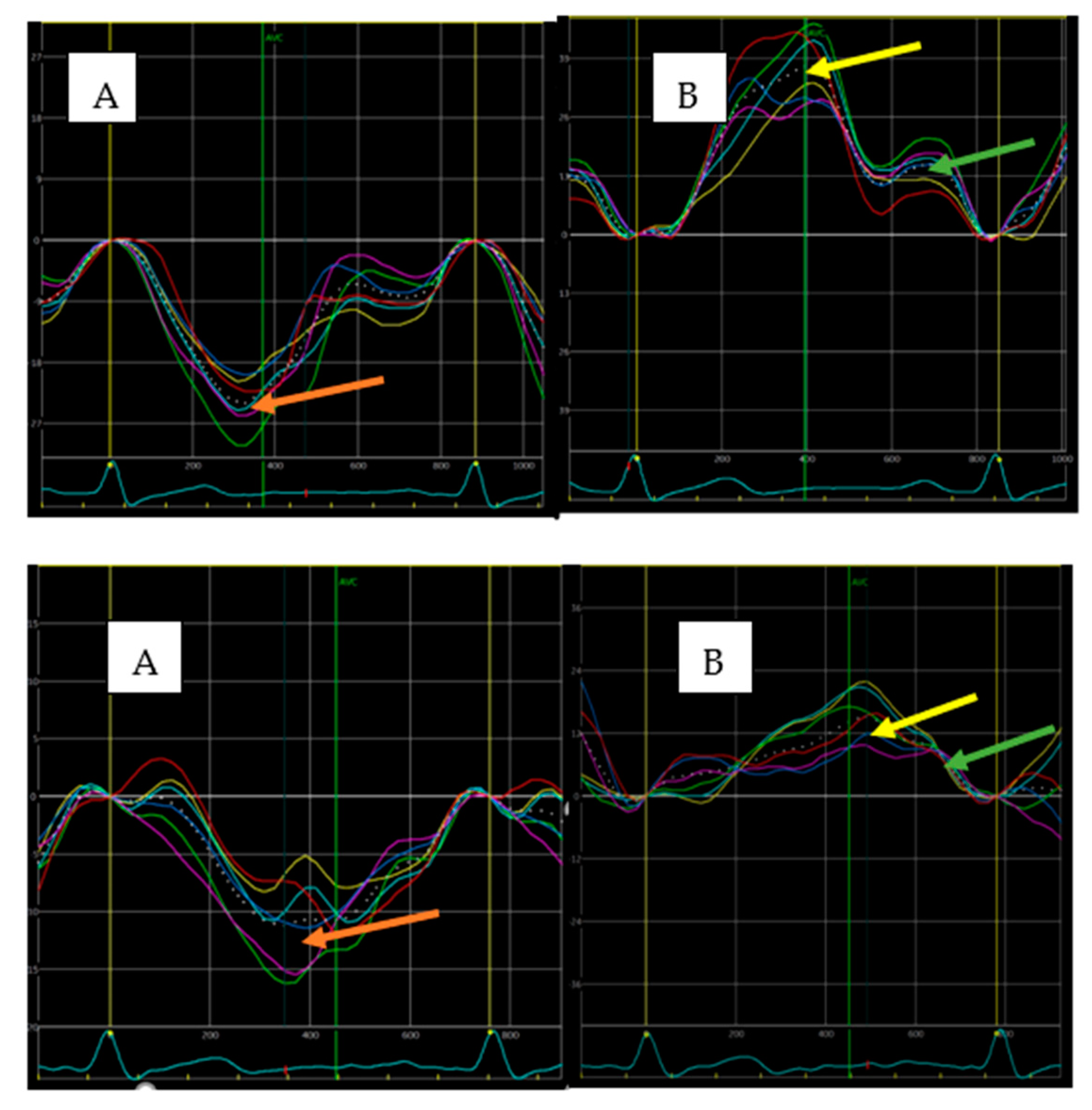
2.4. Speckle-Tracking Imaging
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Echocardiographic Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.; Chalmers, J.; Heerspink, H.J.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Chronic Kidney Disease Prognosis Consortium. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes: A meta-analysis of 1,024,977 individuals. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef] [Green Version]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Chronic Kidney Disease Prognosis Consortium. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: A meta-analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef] [Green Version]
- Kasiske, B.L.; Snyder, J.J.; Matas, A.J.; Ellison, M.D.; Gill, J.S.; Kausz, A.T. Preemptive kidney transplantation: The advantage and the advantaged. J. Am. Soc. Nephrol. 2002, 13, 1358–1364. [Google Scholar] [CrossRef] [Green Version]
- Goto, N.; Okada, M.; Yamamoto, T.; Tsujita, M.; Hiramitsu, T.; Narumi, S.; Katayama, A.; Kobayashi, T.; Uchida, K.; Watarai, Y. Association of dialysis duration with outcomes after transplantation in a Japanese cohort. Clin. J. Am. Soc. Nephrol. 2016, 11, 497–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meier-Kriesche, H.U.; Schold, J.D. The impact of pretransplant dialysis on outcomes in renal transplantation. Semin. Dial. 2005, 18, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Helanterä, I.; Salmela, K.; Kyllönen, L.; Koskinen, P.; Grönhagen-Riska, C.; Finne, P. Pretransplant dialysis duration and risk of death after kidney transplantation in the current era. Transplantation 2014, 98, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Amann, K.; Shoji, T. The heart and vascular system in dialysis. Lancet 2016, 388, 276–284. [Google Scholar] [CrossRef]
- Arcari, L.; Ciavarella, G.M.; Altieri, S.; Limite, L.R.; Russo, D.; Luciani, M.; De Biase, L.; Mené, P.; Volpe, M. Longitudinal changes of left and right cardiac structure and function in patients with end-stage renal disease on replacement therapy. Eur. J. Intern. Med. 2020, 78, 95–100. [Google Scholar] [CrossRef]
- Kramann, R.; Erpenbeck, J.; Schneider, R.K.; Röhl, A.B.; Hein, M.; Brandenburg, V.M.; van Diepen, M.; Dekker, F.; Marx, N.; Floege, J.; et al. Speckle tracking echocardiography detects uremic cardiomyopathy early and predicts cardiovascular mortality in ESRD. J. Am. Soc. Nephrol. 2014, 25, 2351–2365. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glicklich, D.; Vohra, P. Cardiovascular risk assessment before and after kidney transplantation. Cardiol. Rev. 2014, 22, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Boenink, R.; Stel, V.S.; Waldum-Grevbo, B.E.; Collart, F.; Kerschbaum, J.; Heaf, J.G.; de Meester, J.; Finne, P.; García-Marcos, S.A.; Evans, M.; et al. Data from the ERA-EDTA Registry were examined for trends in excess mortality in European adults on kidney replacement therapy. Kidney Int. 2020, 98, 999–1008. [Google Scholar] [CrossRef]
- Irish, G.L.; Chadban, S.; McDonald, S.; Clayton, P.A. Quantifying lead time bias when estimating patient survival in preemptive living kidney donor transplantation. Am. J. Transplant. 2019, 19, 3367–3376. [Google Scholar] [CrossRef]
- Jay, C.L.; Dean, P.G.; Helmick, R.A.; Stegall, M.D. Reassessing preemptive kidney transplantation in the United States: Are we making progress? Transplantation 2016, 100, 1120.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaral, S.; Sayed, B.A.; Kutner, N.; Patzer, R.E. Preemptive kidney transplantation asassociated with survival benefits among pediatric patients with end-stage renal disease. Kidney Int. 2016, 90, 1100–1108. [Google Scholar] [CrossRef] [Green Version]
- Kosmala, W.; Marwick, T.H. Asymptomatic Left Ventricular Diastolic Dysfunction: Predicting Progression to Symptomatic Heart Failure. JACC Cardiovasc. Imaging 2020, 13, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Biering-Sørensen, T.; Biering-Sørensen, S.R.; Olsen, F.J.; Sengeløv, M.; Jørgensen, P.G.; Mogelvang, R.; Shah, A.M.; Jensen, J.S. Global Longitudinal Strain by Echocardiography Predicts Long-Term Risk of Cardiovascular Morbidity and Mortality in a Low-Risk General Population: The Copenhagen City Heart Study. Circ. Cardiovasc. Imaging 2017, 10, e005521. [Google Scholar] [CrossRef] [Green Version]
- Fujikura, K.; Peltzer, B.; Tiwari, N.; Shim, H.G.; Dinhofer, A.B.; Shitole, S.G.; Kizer, J.R.; Garcia, M.J. Reduced global longitudinal strain is associated with increased risk of cardiovascular events or death after kidney transplant. Int. J. Cardiol. 2018, 272, 323–328. [Google Scholar] [CrossRef]
- Farshid, A.; Pathak, R.; Shadbolt, B.; Arnolda, L.; Talaulikar, G. Diastolic function is a strong predictor of mortality in patients with chronic kidney disease. BMC Nephrol. 2013, 14, 280. [Google Scholar] [CrossRef] [Green Version]
- Panoulas, V.F.; Sulemane, S.; Konstantinou, K.; Bratsas, A.; Elliott, S.J.; Dawson, D.; Frankel, A.H.; Nihoyannopoulos, P. Early detection of subclinical left ventricular myocardial dysfunction in patients with chronic kidney disease. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 539.e48. [Google Scholar] [CrossRef] [Green Version]
- Malik, J.; Lachmanova, J.; Kudlicka, J.; Rocinova, K.; Valerianova, A.; Bartkova, M.; Tesar, V. Left Atrial Dysfunction in End-Stage Renal Disease Patients Treated by Hemodialysis. Nephron 2016, 133, 169–174. [Google Scholar] [CrossRef]
- Hensen, L.C.R.; Delgado, V.; van Wijngaarden, S.E.; Leung, M.; de Bie, M.K.; Buiten, M.S.; Schalij, M.J.; Van de Kerkhof, J.J.; Rabelink, T.J.; Rotmans, J.I.; et al. Echocardiographic associates of atrial fibrillation in end-stage renal disease. Nephrol. Dial. Transplant. 2017, 32, 1409–1414. [Google Scholar] [CrossRef] [Green Version]
- Mimura, I.; Nishi, H.; Mise, N.; Mori, M.; Sugimoto, T. Left ventricular geometry and cardiovascular mortality based on haemodialysis patient autopsy analyses. Nephrology 2010, 15, 549–554. [Google Scholar] [CrossRef]
- Kim, E.D.; Sozio, S.M.; Estrella, M.M.; Jaar, B.G.; Shafi, T.; Meoni, L.A.; Kao, W.H.; Lima, J.A.; Parekh, R.S. Cross-sectional association of volume, blood pressures, and aortic stiffness with left ventricular mass in incident hemodialysis patients: The Predictors of Arrhythmic and Cardiovascular Risk in End-Stage Renal Disease (PACE) study. BMC Nephrol. 2015, 16, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kainz, A.; Goliasch, G.; Wiesbauer, F.; Binder, T.; Maurer, G.; Nesser, H.J.; Mascherbauer, R.; Ebner, C.; Kramar, R.; Wilflingseder, J.; et al. Left atrial diameter and survival among renal allograft recipients. Clin. J. Am. Soc. Nephrol. 2013, 8, 2100–2105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavazzoni, M.; Badano, L.P.; Vizzardi, E.; Raddino, R.; Genovese, D.; Taramasso, M.; Sciatti, E.; Palermo, C.; Metra, M.; Muraru, D. Prognostic value of right ventricular free wall longitudinal strain in a large cohort of outpatients with left-side heart disease. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Arcari, L.; Engel, J.; Freiwald, T.; Zhou, H.; Zainal, H.; Gawor, M.; Buettner, S.; Geiger, H.; Hauser, I.; Nagel, E.; et al. Cardiac biomarkers in chronic kidney disease are independently associated with myocardial edema and diffuse fibrosis by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 71. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, V.; Courtellemont, C.; Cariou, E.; Fournier, P.; Lavie-Badie, Y.; Pascal, P.; Galinier, M.; Kamar, N.; Carrié, D.; Lairez, O. Cardiac impact of arteriovenous fistulas: What tools to assess? Heart Vessels 2020, 35, 1583–1593. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Preemptive KTx n = 21 | HD KTx n = 21 | p Value |
|---|---|---|---|
| age, years (SD) | 45.1(12.3) | 45.1 (12.1) | 0.99 |
| sex, male, n (%) | 14 (67) | 14(67) | 1.0 |
| BMI, kg/m2 (SD) | 23.9 (2.2) | 25.2 (3.5) | 0.19 |
| time after KTx, months (IQR) | 39 (16–60) | 41(24–85) | 0.72 |
| causes of kidney failure | |||
| glomerulonephritis, n (%) | 11 (52) | 9 (43) | 0.75 |
| interstitial nephropathy, n (%) | 0 (0) | 3 (14) | 0.23 |
| hypertensive nephropathy, n (%) | 1 (5) | 2 (9) | 0.99 |
| diabetic nephropathy, n (%) | 0 (0) | 1(5) | 0.99 |
| polycystic kidney disease, n (%) | 4 (19) | 4 (19) | 0.99 |
| other, n (%) | 6 (28) | 2 (9) | 0.24 |
| arterio-venous fistula, n (%) | 3 (14) | 14 (67) | 0.002 |
| living donor transplantation, n (%) | 9 (43) | 3 (14) | 0.09 |
| diabetes mellitus, n (%) | 1 (5) | 5 (23) | 0.19 |
| hypertension, n (%) | 16 (76) | 17 (81) | 0.71 |
| hemoglobin, g% (SD) | 13.7 (2.6) | 13.9 (2.2) | 0.79 |
| serum creatinine, mg% (SD) | 1.54 (0.72) | 1.71 (0.86) | 0.49 |
| eGFR, mL/min/1.73 m2 (SD) | 54.0 (15.7) | 51.4 (20.5) | 0.64 |
| systolic blood pressure, mmHg (SD) | 134.3 (15.6) | 138.1 (18.4) | 0.47 |
| diastolic blood pressure, mmHg (SD) | 84.9(10.6) | 84.8 (9.3) | 0.98 |
| immunosuppressive treatment, n (%) | |||
| tacrolimus, mycophenolate mofetil, steroids | 15 (71) | 16 (76) | 0.99 |
| cyclosporine, mycophenolate mofetil | 2 (10) | 2 (10) | 0.99 |
| tacrolimus, mycophenolate mofetil | 2 (10) | 3 (14) | 0.99 |
| tacrolimus, steroids | 1 (5) | 0 (0) | 0.99 |
| Azatopiryne | 0 (0) | 1 (5) | 0.99 |
| hypotensive treatment, n (%) | |||
| beta-blockers | 11 (52) | 15 (71) | 0.34 |
| ACEIs/ARBs | 2 (10) | 5 (24) | 0.41 |
| calcium blockers | 8 (38) | 10 (48) | 0.76 |
| alfa-1 blockers | 2 (10) | 6 (29) | 0.24 |
| Parameter | Preemptive KTx n = 21 | HD KTx n = 21 | p Value |
|---|---|---|---|
| LV end-diastolic dimension, mm (SD) | 47.1 (4.7) | 49.3 (3.9) | 0.09 |
| Relative wall thickness (SD) | 0.43 (0.04) | 0.42 (0.05) | 0.88 |
| LVMI, g/m2 (SD) | 94.4 (18.8) | 109.8 (18.8) | 0.01 |
| Left ventricular hypertrophy, n (%) | 4 (19) | 12 (57) | 0.03 |
| LAVI, mL/m2 (SD) | 29.4 (4.5) | 34.5 (5.3) | 0.002 |
| LAVI >34 mL/m2, n (%) | 0 (0) | 11 (52) | <0.001 |
| PALS, % (SD) | 34.1 (4.7) | 25.1 (6.9) | <0.001 |
| PACS, % (SD) | 15.9 (1.5) | 10.5 (3.8) | <0.001 |
| LV ejection fraction, % (SD) | 60.9 (2.3) | 62.6 (3.9) | 0.10 |
| E/A (SD) | 1.07 (0.28) | 0.98 (0.28) | 0.31 |
| Deceleration time of E wave, ms (SD) | 17.2 (37.1) | 178.4 (47.2) | 0.67 |
| e’ septal, cm/s (SD) | 8.0 (1.9) | 6.5 (1.7) | 0.01 |
| e’ lateral, cm/s (SD) | 11.8 (2.3) | 8.7 (2.7) | <0.001 |
| E/e’ (SD) | 6.9 (1.0) | 9.1 (1.4) | <0.001 |
| GLS, % (SD) | 20.0 (2.3) | 17.1 (3.0) | 0.001 |
| basal RV dimension, mm (SD) | 32.0 (3.3) | 34.1 (3.1) | 0.21 |
| TAPSE, mm (SD) | 21.5 (2.3) | 21.4(1.8) | 0.82 |
| RVGLS% (SD) | 24.5 (4.8) | 20.7 (5.9) | 0.03 |
| Age | Male Sex | BMI | HT | DM | eGFR | HD | AVF | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R | p | R | p | R | p | R | p | R | p | R | p | R | p | R | p | |
| LVMI | 0.33 | 0.03 | −0.35 | 0.02 | 0.42 | 0.005 | 0.42 | 0.005 | 0.14 | 0.36 | −0.31 | 0.049 | 0.37 | 0.02 | 0.29 | 0.06 |
| E/e` | 0.08 | 0.61 | 0.28 | 0.07 | 0.12 | 0.48 | 0.17 | 0.27 | 0.05 | 0.76 | −0.39 | 0.01 | 0.69 | <0.001 | 0.32 | 0.04 |
| GLS | 0.31 | 0.048 | 0.45 | 0.003 | −0.33 | 0.03 | −0.10 | 0.53 | −0.29 | 0.07 | 0.09 | 0.51 | −0.46 | 0.001 | −0.28 | 0.07 |
| LAVI | 0.53 | 0.02 | −0.23 | 0.14 | 0.02 | 0.87 | 0.18 | 0.25 | 0.14 | 0.38 | −0.21 | 0.17 | 0.47 | 0.002 | 0.42 | 0.005 |
| PALS | −0.10 | 0.53 | 0.06 | 0.69 | −0.29 | 0.06 | −0.23 | 0.15 | −0.31 | 0.04 | 0.16 | 0.31 | −0.64 | <0.001 | −0.20 | 0.20 |
| PACS | 0.21 | 0.18 | −0.16 | 0.31 | −0.13 | 0.41 | −0.19 | 0.22 | −0.16 | 0.30 | 0.19 | 0.20 | −0.67 | <0.001 | −0.34 | 0.02 |
| RVGLS | −0.11 | 0.51 | 0.24 | 0.14 | −0.35 | 0.03 | −0.14 | 0.39 | −0.01 | 0.93 | −0.11 | 0.51 | −0.33 | 0.04 | 0.16 | 0.34 |
| Model for LVMI | Model for LAVI | Model for E/e’ | Model for GLS | Model for PALS | Model for PACS | Model for RVGLS | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R2 = 0.61 | R2 = 0.67 | R2 = 0.60 | R2 = 0.51 | R2 = 0.41 | R2 = 0.50 | R2 = 0.22 | |||||||||||||||
| β | SE | p | β | SE | p | β | SE | p | β | SE | p | β | SE | p | β | SE | p | β | SE | p | |
| age | 0.32 | 0.10 | 0.002 | −0.58 | 0.09 | <0.001 | - | - | - | 0.28 | 0.11 | 0.02 | - | - | - | −0.32 | 0.12 | 0.01 | - | - | - |
| female sex | −0.83 | 0.10 | <0.001 | −0.51 | 0.10 | <0.001 | 0.28 | 0.10 | 0.02 | 0.46 | 0.11 | <0.001 | - | - | - | −0.20 | 0.12 | 0.09 | - | - | - |
| BMI | 0.14 | 0.11 | 0.21 | −0.31 | 0.10 | 0.006 | - | - | - | - | - | - | −0.19 | 0.13 | 0.14 | - | - | - | −0.30 | 0.16 | 0.06 |
| HT | 0.25 | 0.10 | 0.02 | - | - | - | 0.20 | 0.10 | 0.051 | - | - | - | −0.13 | 0.13 | 0.32 | −0.28 | 0.11 | 0.02 | - | - | - |
| DM | - | - | - | −0.14 | 0.10 | 0.16 | −0.16 | 0.11 | 0.13 | −0.21 | 0.12 | 0.08 | −0.19 | 0.13 | 0.14 | - | - | - | - | - | - |
| eGFR | −0.28 | 0.11 | 0.003 | −0.25 | 0.09 | 0.01 | −0.25 | 0.11 | 0.02 | 0.23 | 0.11 | 0.06 | 0.12 | 0.12 | 0.32 | −0.12 | 0.12 | 0.29 | −0.15 | −0.15 | 0.32 |
| HD | 0.32 | 0.10 | 0.003 | 0.55 | 0.10 | <0.001 | 0.68 | 0.10 | <0.001 | −0.41 | 0.12 | <0.001 | −0.50 | 0.13 | <0.001 | −0.60 | 0.11 | <0.001 | −0.29 | 0.16 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Obremska, M.; Kamińska, D.; Krawczyk, M.; Krajewska, M.; Kosmala, W. Impact of Different Approaches to Kidney Transplant with and without Chronic Hemodialysis on Cardiac Function and Morphology: A Case–Control Study. J. Clin. Med. 2021, 10, 3913. https://doi.org/10.3390/jcm10173913
Obremska M, Kamińska D, Krawczyk M, Krajewska M, Kosmala W. Impact of Different Approaches to Kidney Transplant with and without Chronic Hemodialysis on Cardiac Function and Morphology: A Case–Control Study. Journal of Clinical Medicine. 2021; 10(17):3913. https://doi.org/10.3390/jcm10173913
Chicago/Turabian StyleObremska, Marta, Dorota Kamińska, Magdalena Krawczyk, Magdalena Krajewska, and Wojciech Kosmala. 2021. "Impact of Different Approaches to Kidney Transplant with and without Chronic Hemodialysis on Cardiac Function and Morphology: A Case–Control Study" Journal of Clinical Medicine 10, no. 17: 3913. https://doi.org/10.3390/jcm10173913