
Rectus Abdominis Flap Replantation after 18 h Hypothermic Extracorporeal Perfusion—A Porcine Model

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Procedure
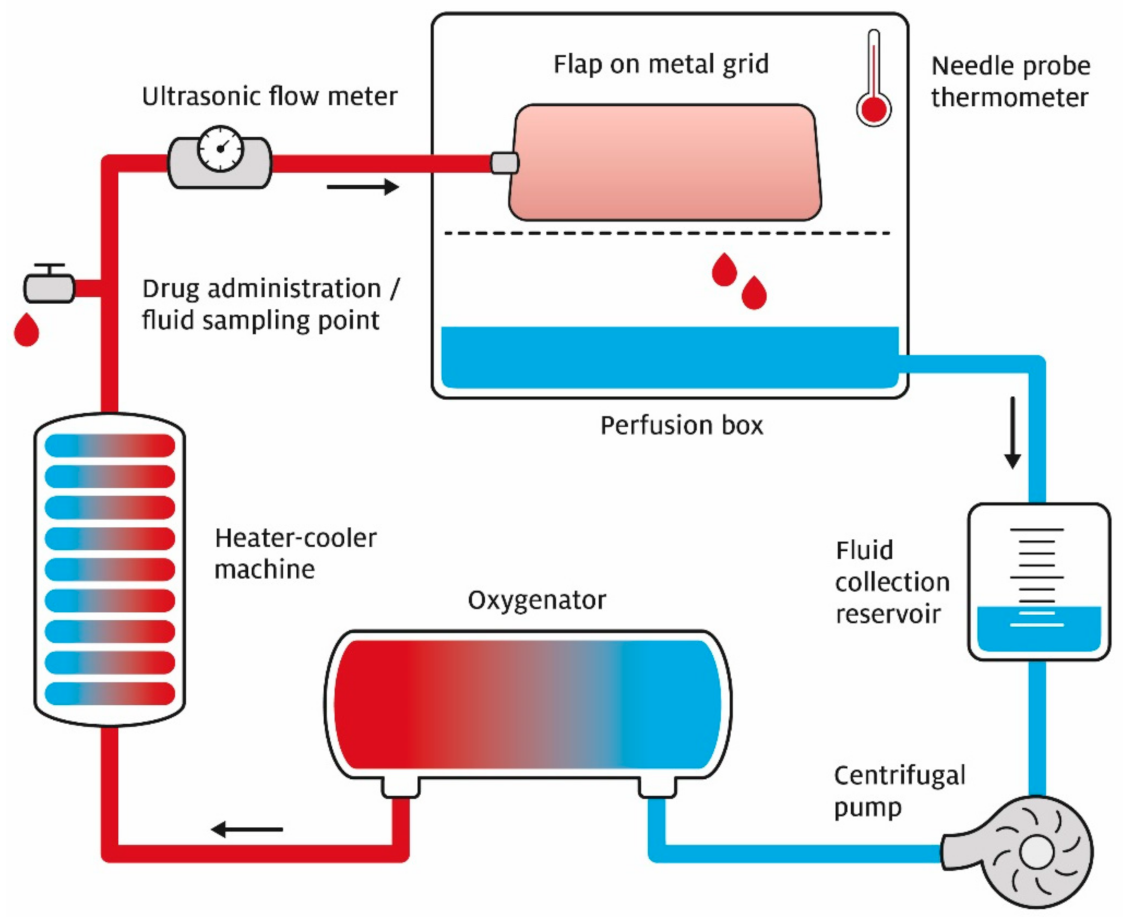
2.2. Perfusion System
2.3. Baseline Measurements
2.4. Measurements during Flap Preservation
2.5. Measurements after Flap Replantation
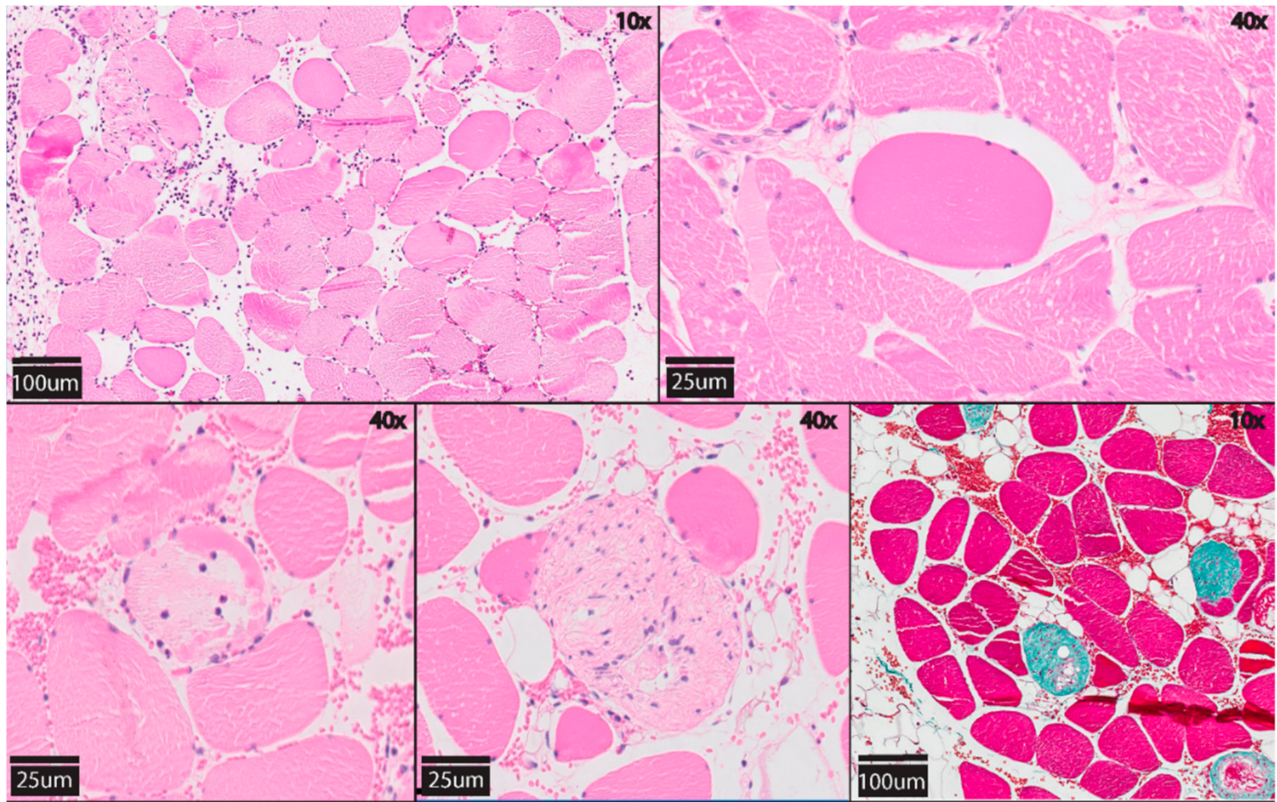
2.6. Histology
2.7. Statistical Analysis
3. Results
3.1. Measurements during Flap Preservation
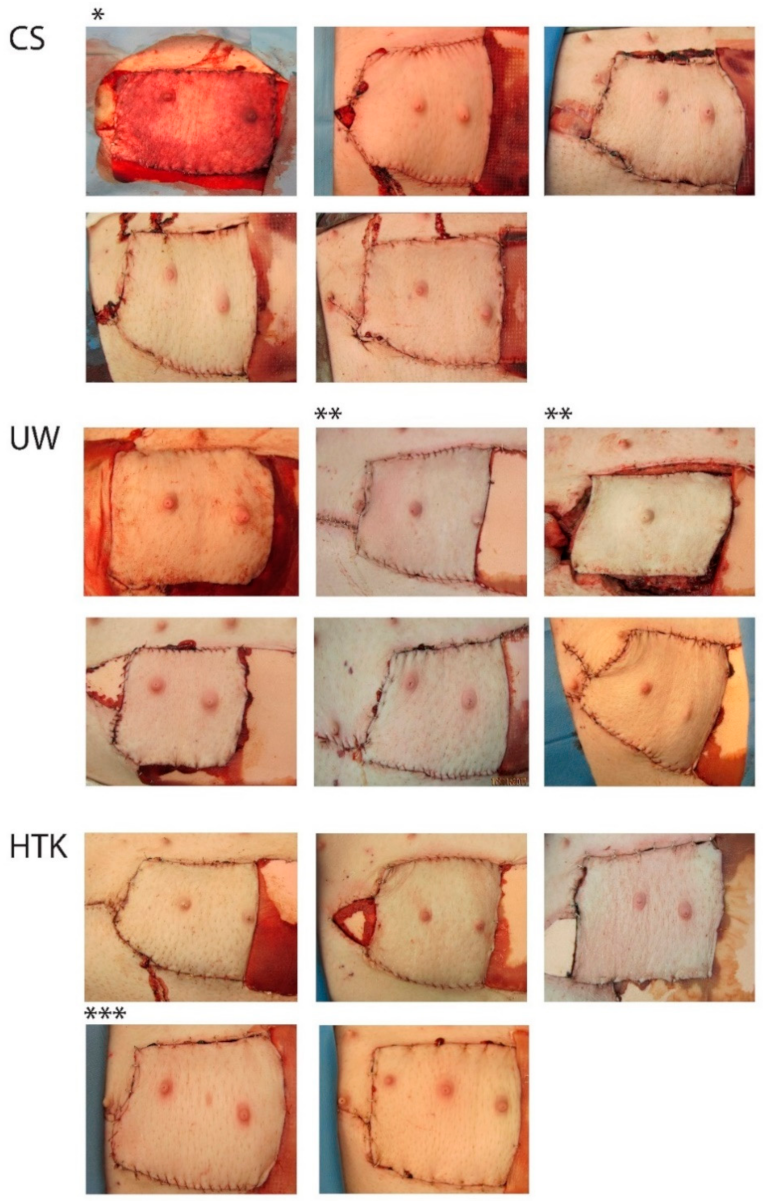
3.2. Measurements after Flap Replantation
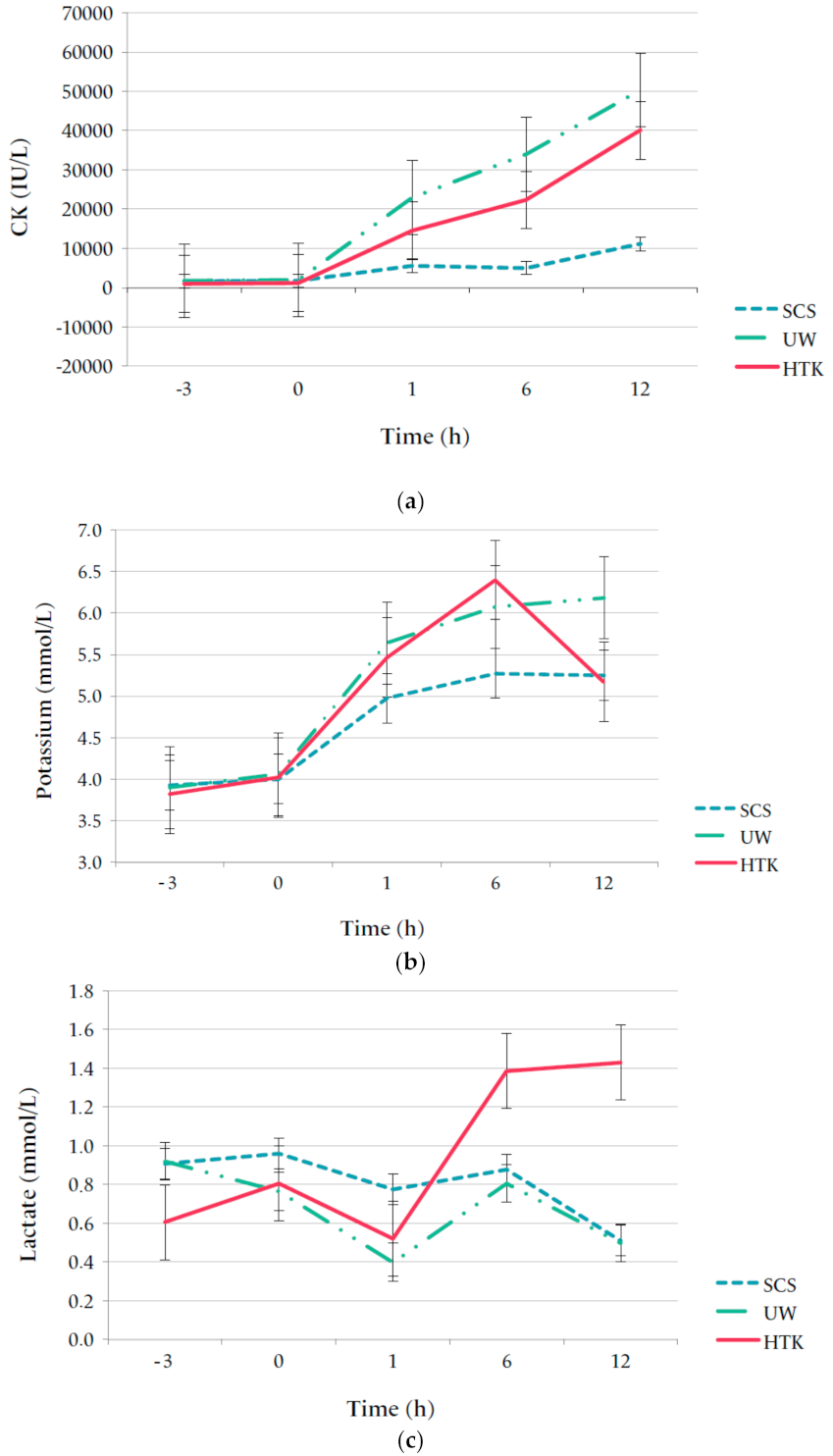
3.3. Laboratory Measurements
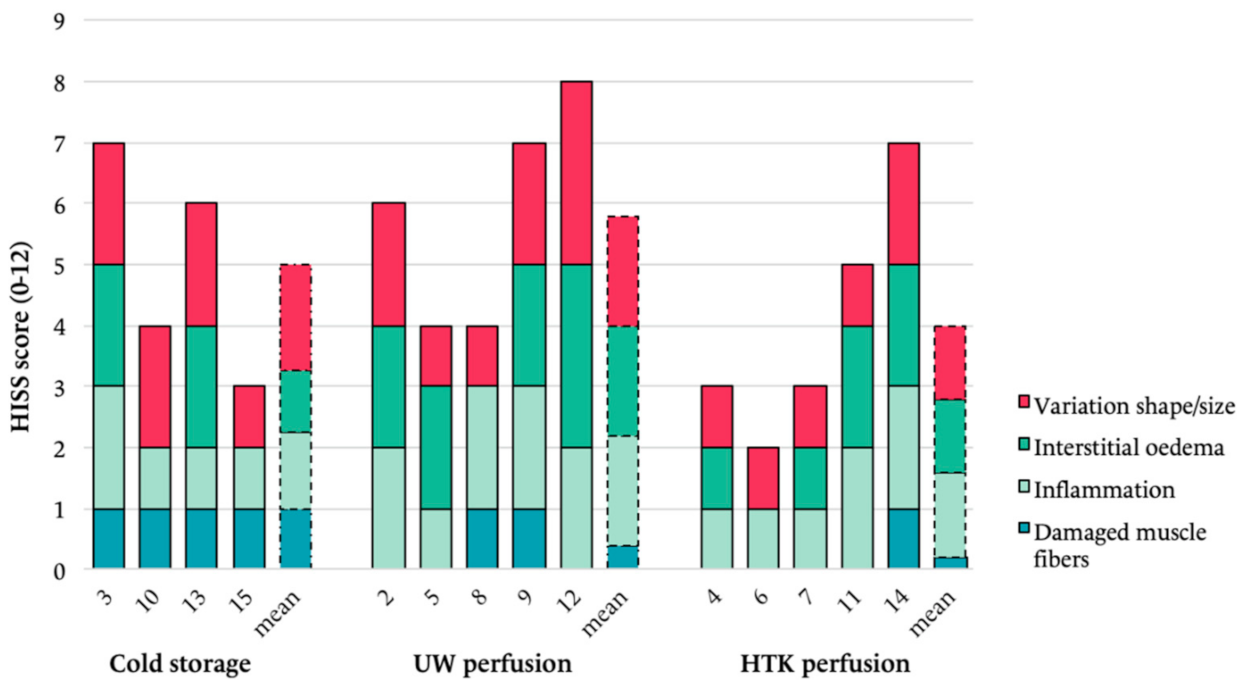
3.4. Histology
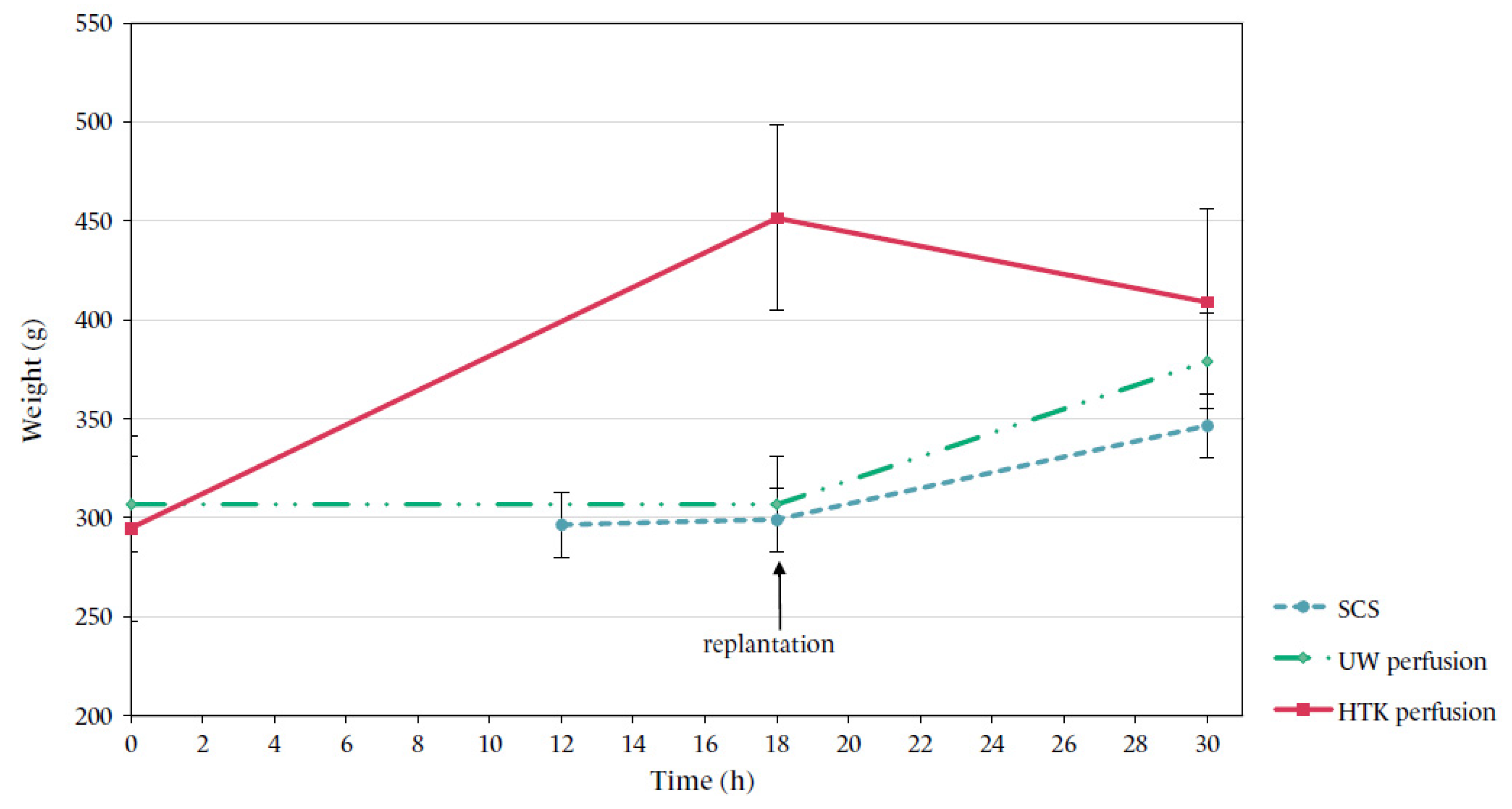
3.5. Flap Weight
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scully, R.E.; Hughes, C.W. The pathology of ischemia of skeletal muscle in man; a description of early changes in muscles of the extremities following damage to major peripheral arteries on the battlefield. Am. J. Pathol. 1956, 32, 805–829. [Google Scholar]
- Harman, J.W. A histologic study of skeletal muscle in acute ischemia. Am. J. Pathol. 1947, 23, 551–565. [Google Scholar]
- Datta, N.; Devaney, S.G.; Busuttil, R.W.; Azari, K.; Kupiec-Weglinski, J.W. Prolonged Cold Ischemia Time Results in Local and Remote Organ Dysfunction in a Murine Model of Vascularized Composite Transplantation. Arab. Archaeol. Epigr. 2017, 17, 2572–2579. [Google Scholar] [CrossRef] [Green Version]
- Blaisdell, F. The pathophysiology of skeletal muscle ischemia and the reperfusion syndrome: A review. Cardiovasc. Surg. 2002, 10, 620–630. [Google Scholar] [CrossRef]
- Eckert, P.; Schnackerz, K. Ischemic Tolerance of Human Skeletal Muscle. Ann. Plast. Surg. 1991, 26, 77–84. [Google Scholar] [CrossRef]
- Kalogeris, T.; Baines, C.P.; Krenz, M.; Korthuis, R.J. Cell Biology of Ischemia/Reperfusion Injury. Int. Rev. Cell Mol. Biol. 2012, 298, 229–317. [Google Scholar] [CrossRef] [Green Version]
- Sternbergh, W.C., 3rd; Adelman, B. The temporal relationship between endothelial cell dysfunction and skeletal muscle damage after ischemia and reperfusion. J. Vasc. Surg. 1992, 16, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Amin, K.R.; Ball, A.L.; Chhina, C.; Edge, R.J.; Stone, J.P.; Critchley, W.R.; Wong, J.K.; Fildes, J.E. Ex-vivo flush of the limb allograft reduces inflammatory burden prior to transplantation. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Dickey, R.M.; Hembd, A.S.; Fruge, S.; Haddock, N.; Papas, K.K.; Suszynski, T.M. Composite Tissue Preservation. Ann. Plast. Surg. 2020, 84, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Barnes, J.; Issa, F.; Vrakas, G.; Friend, P.; Giele, H. The abdominal wall transplant as a sentinel skin graft. Curr. Opin. Organ Transplant. 2016, 21, 536–540. [Google Scholar] [CrossRef]
- Amin, K.R.; Wong, J.K.; Fildes, J.E. Strategies to Reduce Ischemia Reperfusion Injury in Vascularized Composite Allotransplantation of the Limb. J. Hand Surg. 2017, 42, 1019–1024. [Google Scholar] [CrossRef]
- Latchana, N. Preservation solutions used during abdominal transplantation: Current status and outcomes. World J. Transplant. 2015, 5, 154–164. [Google Scholar] [CrossRef]
- Kruit, A.S.; Winters, H.; Van Luijk, J.; Schreinemachers, M.-C.J.; Ulrich, D.J. Current insights into extracorporeal perfusion of free tissue flaps and extremities: A systematic review and data synthesis. J. Surg. Res. 2018, 227, 7–16. [Google Scholar] [CrossRef]
- Krezdorn, N.; Macleod, F.; Tasigiorgos, S.; Turk, M.; Wo, L.; Kiwanuka, H.; Lopdrup, B.R.; Kollar, B.; Edelman, E.R.; Pomahac, B. Twenty-Four–Hour Ex Vivo Perfusion with Acellular Solution Enables Successful Replantation of Porcine Forelimbs. Plast. Reconstr. Surg. 2019, 144, 608e–618e. [Google Scholar] [CrossRef]
- Kruit, A.S.; Schreinemachers, M.-C.J.; Koers, E.J.; Zegers, H.J.; Hummelink, S.; Ulrich, D.J. Successful Long-term Extracorporeal Perfusion of Free Musculocutaneous Flaps in a Porcine Model. J. Surg. Res. 2019, 235, 113–123. [Google Scholar] [CrossRef]
- Kruit, A.S.; Smits, L.; Pouwels, A.; Schreinemachers, M.-C.J.; Hummelink, S.L.; Ulrich, D.J. Ex-vivo perfusion as a successful strategy for reduction of ischemia-reperfusion injury in prolonged muscle flap preservation—A gene expression study. Gene 2019, 701, 89–97. [Google Scholar] [CrossRef]
- Karangwa, S.A.; Dutkowski, P.; Fontes, P.; Friend, P.J.; Guarrera, J.V.; Markmann, J.F.; Mergental, H.; Minor, T.; Quintini, C.; Selzner, M.; et al. Machine Perfusion of Donor Livers for Transplantation: A Proposal for Standardized Nomenclature and Reporting Guidelines. Arab. Archaeol. Epigr. 2016, 16, 2932–2942. [Google Scholar] [CrossRef]
- Kaltenborn, A.; Gwiasda, J.; Amelung, V.; Krauth, C.; Lehner, F.; Braun, F.; Klempnauer, J.; Reichert, B.; Schrem, H. Comparable outcome of liver transplantation with Histidine-Tryptophan-Ketoglutarate vs. University of Wisconsin preservation solution: A retrospective observational double-center trial. BMC Gastroenterol. 2014, 14, 169. [Google Scholar] [CrossRef] [Green Version]
- Van der Heijden, E.P.; Kroese, A.B.; Werker, P.M.; Grabietz, P.D.; de Jong, M.B.; Bär, P.R.; Kon, M. Function of rat skeletal muscles after storage at 10 degrees C in various preservation solutions. Clin Sci. 1998, 94, 271–278. [Google Scholar] [CrossRef]
- Fuller, B.J.; Lee, C.Y. Hypothermic perfusion preservation: The future of organ preservation revisited? Cryobiology 2007, 54, 129–145. [Google Scholar] [CrossRef]
- Ishikawa, S.; Ueda, K.; Neya, K.; Abe, K.; Kugawa, S.; Kawasaki, A.; Nishizawa, S.; Yamaoka, K. Effects of original crystalloid cardioplegia followed by additional blood cardioplegia: Treatments for prolonged cardiac arrest. Ann. Thorac. Cardiovasc. Surg. 2010, 16, 335–339. [Google Scholar]
- Munabi, N.C.; Olorunnipa, O.B.; Goltsman, D.; Rohde, C.H.; Ascherman, J.A. The ability of intra-operative perfusion mapping with laser-assisted indocyanine green angiography to predict mastectomy flap necrosis in breast reconstruction: A prospective trial. J. Plast. Reconstr. Aesthetic Surg. 2014, 67, 449–455. [Google Scholar] [CrossRef]
- Müller, S.; Constantinescu, M.A.; Kiermeir, D.M.; Gajanayake, T.; Bongoni, A.K.; Vollbach, F.H.; Meoli, M.; Plock, J.; Jenni, H.; Banic, A.; et al. Ischemia/reperfusion injury of porcine limbs after extracorporeal perfusion. J. Surg. Res. 2013, 181, 170–182. [Google Scholar] [CrossRef]
- Cooper, C.A.; Moraes, L.E.; Murray, J.D.; Owens, S.D. Hematologic and biochemical reference intervals for specific pathogen free 6-week-old Hampshire-Yorkshire crossbred pigs. J. Anim. Sci. Biotechnol. 2014, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Kueckelhaus, M.; Dermietzel, A.; Alhefzi, M.; Aycart, M.A.; Fischer, S.; Krezdorn, N.; Wo, L.; Maarouf, O.H.; Riella, L.V.; Abdi, R.; et al. Acellular Hypothermic Extracorporeal Perfusion Extends Allowable Ischemia Time in a Porcine Whole Limb Replantation Model. Plast. Reconstr. Surg. 2017, 139, 922e–932e. [Google Scholar] [CrossRef] [PubMed]
- Venance, S.L. Approach to the Patient With HyperCKemia. Contin. Lifelong Learn. Neurol. 2016, 22, 1803–1814. [Google Scholar] [CrossRef]
- Fahradyan, V.; Said, S.A.; Ordenana, C.; Pozza, E.D.; Frautschi, R.; Duraes, E.F.R.; Madajka-Niemeyer, M.; Papay, F.A.; Rampazzo, A.; Gharb, B.B. Extended ex vivo normothermic perfusion for preservation of vascularized composite allografts. Artif. Organs 2020, 44, 846–855. [Google Scholar] [CrossRef]
- Duraes, E.F.R.; Madajka, M.; Frautschi, R.; Soliman, B.; Cakmakoglu, C.; Barnett, A.; Tadisina, K.; Liu, Q.; Grady, P.; Quintini, C.; et al. Developing a protocol for normothermic ex-situ limb perfusion. Microsurgery 2017, 38, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Araki, J.; Sakai, H.; Takeuchi, D.; Kagaya, Y.; Tashiro, K.; Naito, M.; Mihara, M.; Narushima, M.; Iida, T.; Koshima, I. Normothermic Preservation of the Rat Hind Limb With Artificial Oxygen-carrying Hemoglobin Vesicles. Transplantation 2015, 99, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Kueckelhaus, M.; Fischer, S.; Sisk, G.; Kiwanuka, H.; Bueno, E.M.; Dermietzel, A.; Alhefzi, M.; Aycart, M.; Diehm, Y.; Pomahac, B. A Mobile Extracorporeal Extremity Salvage System for Replantation and Transplantation. Ann. Plast. Surg. 2016, 76, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Taeger, C.D.; Friedrich, O.; Drechsler, C.; Weigand, A.; Hobe, F.; Geppert, C.I.; Münch, F.; Birkholz, T.; Buchholz, R.; Horch, R.E.; et al. Hydroxyethyl starch solution for extracorporeal tissue perfusion. Clin. Hemorheol. Microcirc. 2016, 64, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Jaeschke, H. Preservation injury: Mechanisms, prevention and consequences. J. Hepatol. 1996, 25, 774–780. [Google Scholar] [CrossRef]
- Homer-Vanniasinkam, S.; Rowlands, T.; Hardy, S.; Gough, M. Skeletal Muscle Ischaemia-reperfusion Injury: Further Characterisation of a Rodent Model. Eur. J. Vasc. Endovasc. Surg. 2001, 22, 523–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, P.; Chang, D.W.; Miller, M.J.; Reece, G.; Robb, G.L. Analysis of 49 cases of flap compromise in 1310 free flaps for head and neck reconstruction. Head Neck 2009, 31, 45–51. [Google Scholar] [CrossRef]
- Zoccali, G.; Molina, A.; Farhadi, J. Is long-term post-operative monitoring of microsurgical flaps still necessary? J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 996–1000. [Google Scholar] [CrossRef]
- Bigdeli, A.K.; Gazyakan, E.; Schmidt, V.J.; Bauer, C.; Germann, G.; Radu, C.A.; Kneser, U.; Hirche, C. Long-Term Outcome after Successful Lower Extremity Free Flap Salvage. J. Reconstr. Microsurg. 2018, 35, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Slater, N.J.; Zegers, H.J.; Küsters, B.; Beune, T.; van Swieten, H.A.; Ulrich, D.J. Ex-vivo oxygenated perfusion of free flaps during ischemia time: A feasibility study in a porcine model and preliminary results. J. Surg. Res. 2016, 205, 292–295. [Google Scholar] [CrossRef]
- Chen, K.-T.; Mardini, S.; Chuang, D.C.-C.; Lin, C.-H.; Cheng, M.-H.; Lin, Y.-T.; Huang, W.-C.; Tsao, C.-K.; Wei, F.-C. Timing of Presentation of the First Signs of Vascular Compromise Dictates the Salvage Outcome of Free Flap Transfers. Plast. Reconstr. Surg. 2007, 120, 187–195. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | UW-mp | HTK |
|---|---|---|
| Osmolality (mOsm/L) | 320 | 310 |
| Potassium (mmol/L) | 25 | 9 |
| Sodium (mmol/L) | 80 | 15 |
| Calcium (mmol/L) | 0.5 | 0.015 |
| Scavangers | Glutathione, allopurinol | Tryptophan, mannitol |
| Buffers | Phosphate | Histidine |
| Energy delivery | Adenosine, phosphate | Ketoglutarate |
| Impermeants | HES, gluconate, raffinose | Mannitol |
| Morphological Changes | Categories |
|---|---|
| Interstitial oedema |
|
| Inflammation |
|
| Variation in shape and size of myocytes |
|
| Damaged muscle fibres * |
|
| I. Cold Storage | II. UW-mp Perfusion | III. HTK Perfusion | p-Value | |
|---|---|---|---|---|
| Pig weight (kg) | 72 ± 8 | 67 ± 4 | 71 ± 6 | 0.946 |
| Flush duration (min) | 18 ± 6 | 22 ± 8 | 18 ± 7 | 0.738 |
| Replantation time (min) | 73 ± 18 | 59 ± 25 | 58 ± 25 | 0.201 |
| Total off-pedicle time (h) | 5 ± 0.3 | 19 ± 0.8 | 19 ± 0.5 | 0.009 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kruit, A.S.; van Midden, D.; Schreinemachers, M.-C.; Koers, E.; Zegers, H.; Kusters, B.; Hummelink, S.; Ulrich, D.J.O. Rectus Abdominis Flap Replantation after 18 h Hypothermic Extracorporeal Perfusion—A Porcine Model. J. Clin. Med. 2021, 10, 3858. https://doi.org/10.3390/jcm10173858
Kruit AS, van Midden D, Schreinemachers M-C, Koers E, Zegers H, Kusters B, Hummelink S, Ulrich DJO. Rectus Abdominis Flap Replantation after 18 h Hypothermic Extracorporeal Perfusion—A Porcine Model. Journal of Clinical Medicine. 2021; 10(17):3858. https://doi.org/10.3390/jcm10173858
Chicago/Turabian StyleKruit, Anne Sophie, Dominique van Midden, Marie-Claire Schreinemachers, Erik Koers, Her Zegers, Benno Kusters, Stefan Hummelink, and Dietmar J. O. Ulrich. 2021. "Rectus Abdominis Flap Replantation after 18 h Hypothermic Extracorporeal Perfusion—A Porcine Model" Journal of Clinical Medicine 10, no. 17: 3858. https://doi.org/10.3390/jcm10173858