
Acupuncture Relieved Chemotherapy-Induced Peripheral Neuropathy in Patients with Breast Cancer: A Pilot Randomized Sham-Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
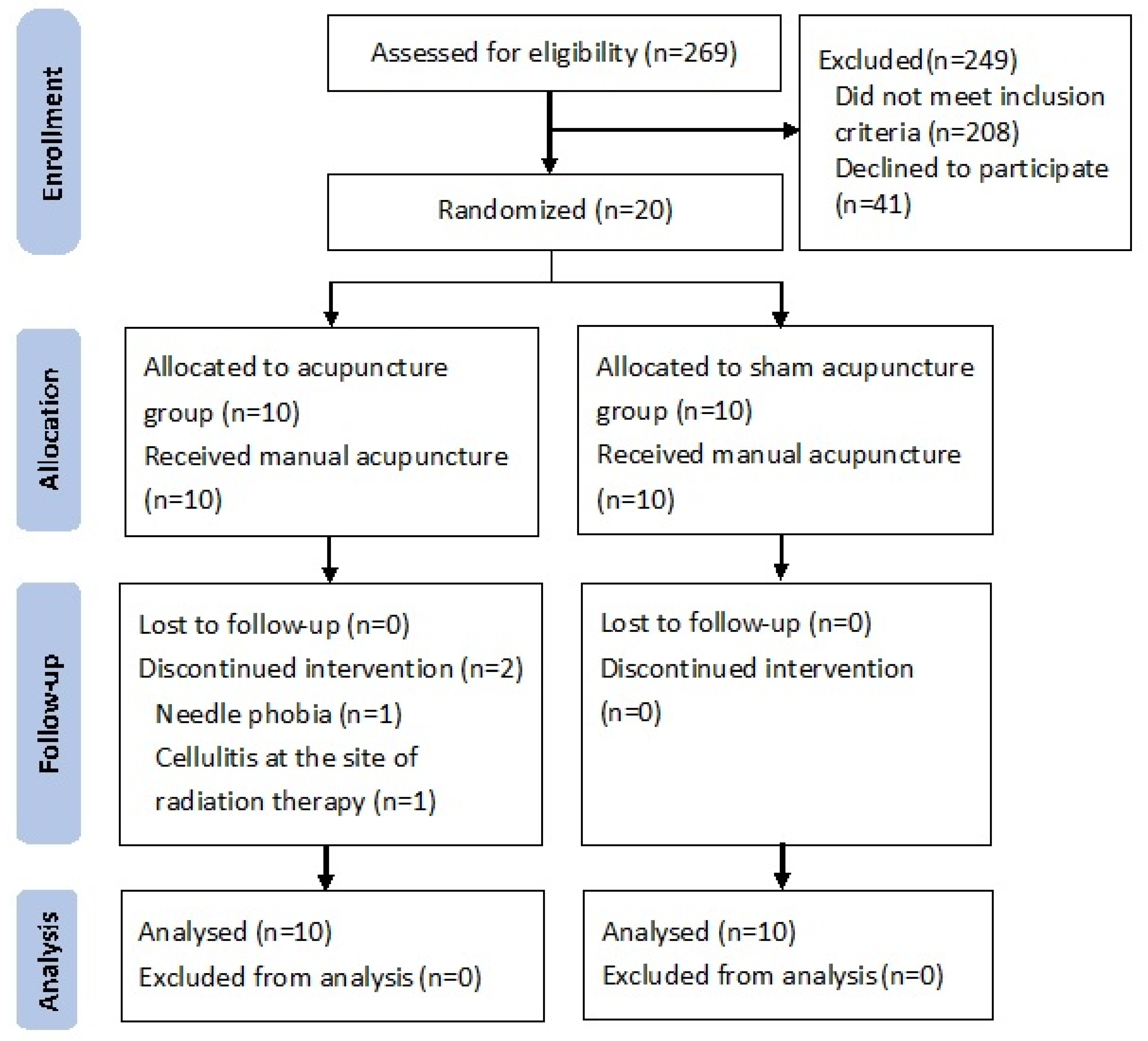
2.1. Trial Design
2.2. Patient Eligibility
2.3. Randomization and Intervention
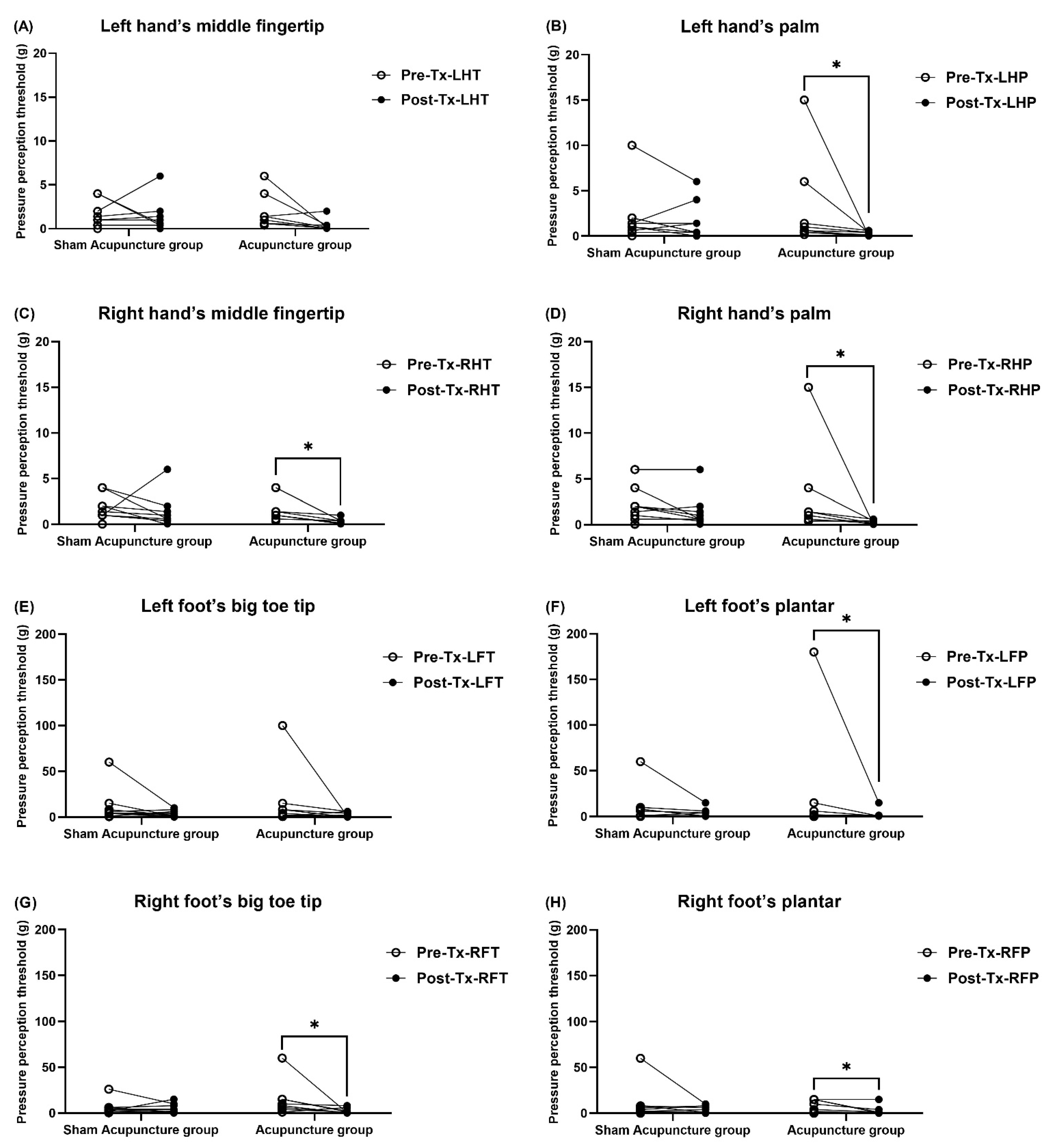
2.4. Quantitative Sensory Test (QST)
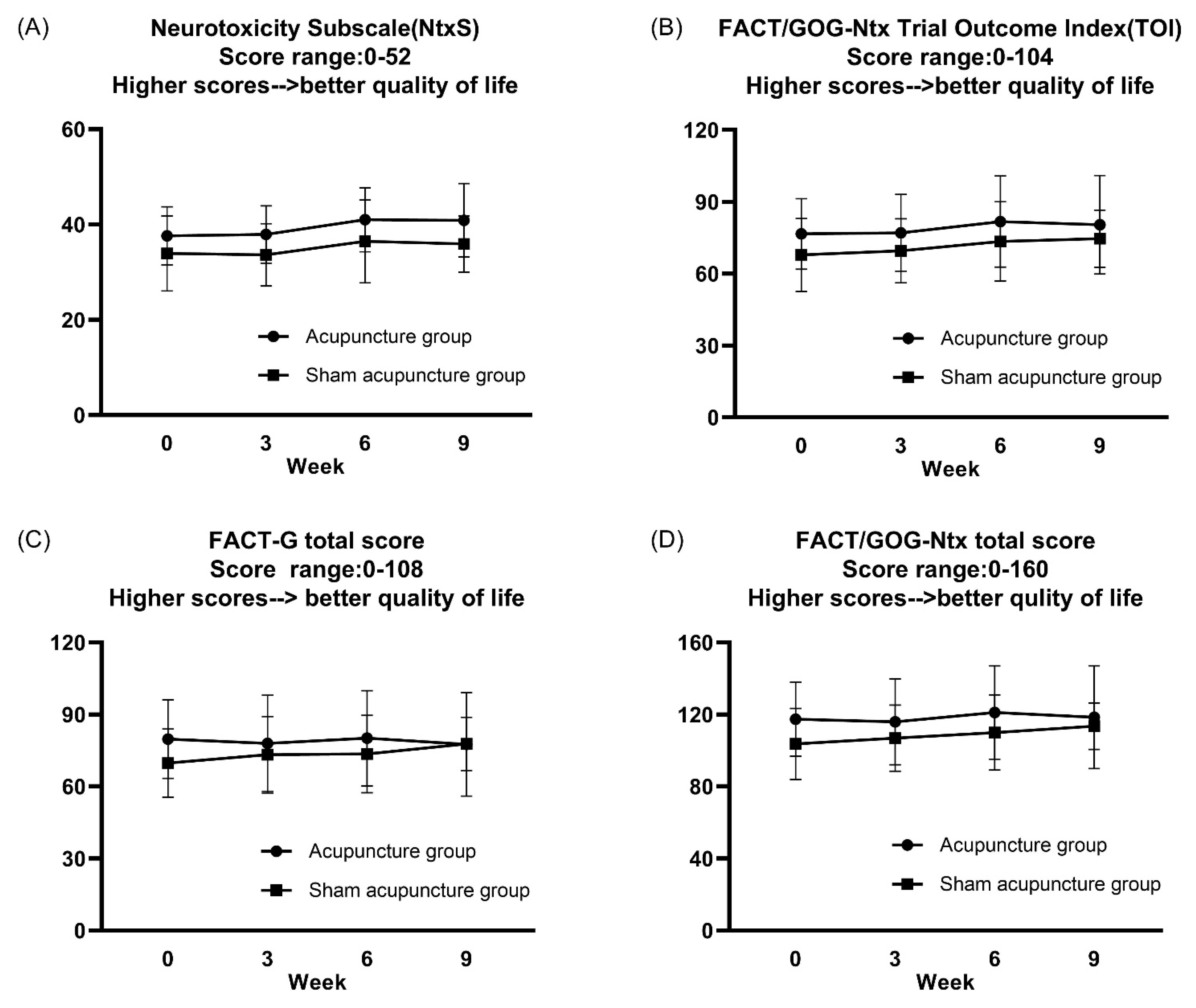
2.5. Patient-Reported Outcome Measures (PROMs)
2.6. Statistical Analysis
3. Results
3.1. Demographics
3.2. Primary Outcome
Effects of Acupuncture on Average Pain Severity
3.3. Secondary Outcomes
3.3.1. Effects of Acupuncture on Pain Interference
3.3.2. Effects of Acupuncture on Quantitative Sensory Test
3.3.3. Effects of Acupuncture on Chemotherapy-Induced Neurotoxicity
3.3.4. Effects of Acupuncture on WHOQOL-BREF
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banach, M.; Juranek, J.K.; Zygulska, A.L. Chemotherapy-induced neuropathies—A growing problem for patients and health care providers. Brain Behav. 2017, 7, e00558. [Google Scholar] [CrossRef]
- Postma, T.; Heimans, J. Grading of chemotherapy-induced peripheral neuropathy. Ann. Oncol. 2000, 11, 509–513. [Google Scholar] [CrossRef]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers: ASCO Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Sedhom, R.; Gupta, A. Chemotherapy-Induced Peripheral Neuropathy. JAMA Oncol. 2019, 5, 750. [Google Scholar] [CrossRef] [Green Version]
- Park, S.B.; Goldstein, D.; Krishnan, A.V.; Lin, C.S.; Friedlander, M.L.; Cassidy, J.; Koltzenburg, M.; Kiernan, M.C. Chemotherapy-induced peripheral neurotoxicity: A critical analysis. CA Cancer J. Clin. 2013, 63, 419–437. [Google Scholar] [CrossRef] [PubMed]
- Zhi, W.I.; Chen, P.; Kwon, A.; Chen, C.; Harte, S.E.; Piulson, L.; Li, S.; Patil, S.; Mao, J.J.; Bao, T. Chemotherapy-induced peripheral neuropathy (CIPN) in breast cancer survivors: A comparison of patient-reported outcomes and quantitative sensory testing. Breast Cancer Res. Treat. 2019, 178, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Rolke, R.; Baron, R.; Maier, C.; Tolle, T.R.; Treede, R.D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Botefur, I.C.; et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef]
- Velasco, R.; Besora, S.; Argyriou, A.A.; Santos, C.; Sala, R.; Izquierdo, C.; Simo, M.; Gil-Gil, M.; Pardo, B.; Jimenez, L.; et al. Duloxetine against symptomatic chemotherapy-induced peripheral neurotoxicity in cancer survivors: A real world, open-label experience. Anti-Cancer Drugs 2021, 32, 88–94. [Google Scholar] [CrossRef]
- Birch, S.; Lee, M.S.; Alraek, T.; Kim, T.H. Evidence, safety and recommendations for when to use acupuncture for treating cancer related symptoms: A narrative review. Integr. Med. Res. 2019, 8, 160–166. [Google Scholar] [CrossRef]
- D’Alessandro, E.G.; Nebuloni Nagy, D.R.; de Brito, C.M.M.; Almeida, E.P.M.; Battistella, L.R.; Cecatto, R.B. Acupuncture for chemotherapy-induced peripheral neuropathy: A randomised controlled pilot study. BMJ Support. Palliat. Care 2019. [Google Scholar] [CrossRef] [PubMed]
- Molassiotis, A.; Suen, L.K.P.; Cheng, H.L.; Mok, T.S.K.; Lee, S.C.Y.; Wang, C.H.; Lee, P.; Leung, H.; Chan, V.; Lau, T.K.H.; et al. A Randomized Assessor-Blinded Wait-List-Controlled Trial to Assess the Effectiveness of Acupuncture in the Management of Chemotherapy-Induced Peripheral Neuropathy. Integr. Cancer Ther. 2019, 18, 1534735419836501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, W.; Giobbie-Hurder, A.; Freedman, R.A.; Shin, I.H.; Lin, N.U.; Partridge, A.H.; Rosenthal, D.S.; Ligibel, J.A. Acupuncture for Chemotherapy-Induced Peripheral Neuropathy in Breast Cancer Survivors: A Randomized Controlled Pilot Trial. Oncologist 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, T.; Patil, S.; Chen, C.; Zhi, I.W.; Li, Q.S.; Piulson, L.; Mao, J.J. Effect of Acupuncture vs Sham Procedure on Chemotherapy-Induced Peripheral Neuropathy Symptoms: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neligan, A.; O’Sullivan, S.S.; Mullins, G.M.; McCarthy, A.; Kowalski, R.G.; Kinsella, J.; McNamara, B. A review of nerve conduction studies in cases of suspected compression neuropathies of the upper limb. Eur. Neurol. 2010, 63, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Arifin, W. Random sampling and allocation using SPSS. Educ. Med. J. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Focks, C. Atlas of Acupuncture; Churchill Livingstone: Edinburgh, UK, 2008. [Google Scholar]
- Yang, Y.; Wang, L.P.; Zhang, L.; Wang, L.C.; Wei, J.; Li, J.J.; Sun, Y.L. Factors contributing to de qi in acupuncture randomized clinical trials. Evid. Based Complement. Alternat. Med. 2013, 2013, 329392. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, H.; Tsukayama, H. Safety of acupuncture practice in Japan: Patient reactions, therapist negligence and error reduction strategies. Evid. Based Complement. Alternat. Med. 2008, 5, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Witt, C.M.; Pach, D.; Brinkhaus, B.; Wruck, K.; Tag, B.; Mank, S.; Willich, S.N. Safety of acupuncture: Results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementmed. 2009, 16, 91–97. [Google Scholar] [CrossRef]
- Lu, Z.; Moody, J.; Marx, B.L.; Hammerstrom, T. Treatment of Chemotherapy-Induced Peripheral Neuropathy in Integrative Oncology: A Survey of Acupuncture and Oriental Medicine Practitioners. J. Altern. Complement. Med. (N. Y.) 2017, 23, 964–970. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Satoh, A.; Yamada, T.; Aisu, N.; Matsuoka, T.; Koganemaru, T.; Kajitani, R.; Munechika, T.; Matsumoto, Y.; Nagano, H.; et al. The Relationship Between Evaluation Methods for Chemotherapy-Induced Peripheral Neuropathy. Sci. Rep. 2019, 9, 20361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamei, N.; Yamane, K.; Nakanishi, S.; Yamashita, Y.; Tamura, T.; Ohshita, K.; Watanabe, H.; Fujikawa, R.; Okubo, M.; Kohno, N. Effectiveness of Semmes-Weinstein monofilament examination for diabetic peripheral neuropathy screening. J. Diabetes Complicat. 2005, 19, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.P. Utilization of brief pain inventory as an assessment tool for pain in patients with cancer: A focused review. Indian J. Palliat Care 2011, 17, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Pang, H.; Cirrincione, C.; Fleishman, S.; Paskett, E.D.; Ahles, T.; Bressler, L.R.; Fadul, C.E.; Knox, C.; Le-Lindqwister, N.; et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: A randomized clinical trial. JAMA 2013, 309, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.S.; Mendoza, T.R.; Gao, S.Z.; Cleeland, C.S. The Chinese version of the Brief Pain Inventory (BPI-C): Its development and use in a study of cancer pain. Pain 1996, 67, 407–416. [Google Scholar] [CrossRef]
- Ger, L.P.; Ho, S.T.; Sun, W.Z.; Wang, M.S.; Cleeland, C.S. Validation of the Brief Pain Inventory in a Taiwanese population. J. Pain Symptom Manag. 1999, 18, 316–322. [Google Scholar] [CrossRef]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Linn, E.; Bonomi, A.; Silberman, M.; Yellen, S.B.; Winicour, P.; Brannon, J.; et al. The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1993, 11, 570–579. [Google Scholar] [CrossRef]
- Huang, H.Q.; Brady, M.F.; Cella, D.; Fleming, G. Validation and reduction of FACT/GOG-Ntx subscale for platinum/paclitaxel-induced neurologic symptoms: A gynecologic oncology group study. Int. J. Gynecol. Cancer 2007, 17, 387–393. [Google Scholar] [CrossRef]
- Calhoun, E.A.; Welshman, E.E.; Chang, C.H.; Lurain, J.R.; Fishman, D.A.; Hunt, T.L.; Cella, D. Psychometric evaluation of the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity (Fact/GOG-Ntx) questionnaire for patients receiving systemic chemotherapy. Int. J. Gynecol. Cancer 2003, 13, 741–748. [Google Scholar] [CrossRef]
- Kaiser, K.; Lyleroehr, M.; Shaunfield, S.; Lacson, L.; Corona, M.; Kircher, S.; Nittve, M.; Cella, D. Neuropathy experienced by colorectal cancer patients receiving oxaliplatin: A qualitative study to validate the Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity scale. World J. Gastrointest. Oncol. 2020, 12, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Hwang, J.S.; Wang, W.C.; Lai, W.W.; Su, W.C.; Wu, T.Y.; Yao, G.; Wang, J.D. Psychometric evaluation of the WHOQOL-BREF, Taiwan version, across five kinds of Taiwanese cancer survivors: Rasch analysis and confirmatory factor analysis. J. Formos Med. Assoc. 2019, 118, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Schober, P.; Vetter, T.R. Nonparametric Statistical Methods in Medical Research. Anesth. Analg. 2020, 131, 1862–1863. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Lacchetti, C.; Dworkin, R.H.; Lavoie Smith, E.M.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Gavin, P.; Lavino, A.; Lustberg, M.B.; et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 1941–1967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.G.; Chen, C.H.; Huang, Y.C.; Chen, Y.H. How to design the control group in randomized controlled trials of acupuncture? Evid. Based Complement. Altern. Med. 2012, 2012, 875284. [Google Scholar] [CrossRef]
- Tracey, E.H.; Greene, A.J.; Doty, R.L. Optimizing reliability and sensitivity of Semmes-Weinstein monofilaments for establishing point tactile thresholds. Physiol. Behav. 2012, 105, 982–986. [Google Scholar] [CrossRef]
- Krumova, E.K.; Geber, C.; Westermann, A.; Maier, C. Neuropathic pain: Is quantitative sensory testing helpful? Curr. Diabetes Rep. 2012, 12, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.L.; Chou, L.W.; Hong, S.F.; Chang, F.C.; Tseng, S.W.; Huang, C.C.; Yang, C.H.; Yang, C.C.; Chiu, W.F. Laser acupuncture attenuates oxaliplatin-induced peripheral neuropathy in patients with gastrointestinal cancer: A pilot prospective cohort study. Acupunct. Med. 2016, 34, 398–405. [Google Scholar] [CrossRef]
- Wong, R.; Major, P.; Sagar, S. Phase 2 Study of Acupuncture-Like Transcutaneous Nerve Stimulation for Chemotherapy-Induced Peripheral Neuropathy. Integr. Cancer Ther. 2016, 15, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Chae, Y.; Um, S.I.; Yi, S.H.; Lee, H.; Chang, D.S.; Yin, C.S.; Park, H.J. Comparison of biomechanical properties between acupuncture and non-penetrating sham needle. Complement. Ther. Med. 2011, 19 (Suppl. 1), S8–S12. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, B.; Pan, Y.; Chen, B.; Guo, Y.; Guo, Y.; Pan, X. Progress of Clinical Study on Acupuncture Treatment of Chemotherapy-induced Peripheral Neuropathy in the Recent Decade. Shanghai J. Acupunct. Moxibustion 2016, 35, 1025–1029. [Google Scholar]
- Han, J.S. Acupuncture and endorphins. Neurosci. Lett. 2004, 361, 258–261. [Google Scholar] [CrossRef]
- Zhao, Z.Q. Neural mechanism underlying acupuncture analgesia. Prog. Neurobiol. 2008, 85, 355–375. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Kain, Z.N.; White, P. Acupuncture analgesia: I. The scientific basis. Anesth. Analg. 2008, 106, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Kang, S.Y.; Choi, J.G.; Kang, D.W.; Kim, S.J.; Lee, S.D.; Park, J.B.; Ryu, Y.H.; Kim, H.W. Analgesic effect of electroacupuncture on paclitaxel-induced neuropathic pain via spinal opioidergic and adrenergic mechanisms in mice. Am. J. Chin. Med. 2015, 43, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Sagar, S. Acupuncture treatment for chemotherapy-induced peripheral neuropathy—A case series. Acupunct. Med. 2006, 24, 87–91. [Google Scholar] [CrossRef]
- Chen, Y.S.; Yao, C.H.; Chen, T.H.; Lin, J.G.; Hsieh, C.L.; Lin, C.C.; Lao, C.J.; Tsai, C.C. Effect of acupuncture stimulation on peripheral nerve regeneration using silicone rubber chambers. Am. J. Chin. Med. 2001, 29, 377–385. [Google Scholar] [CrossRef]
- Ho, C.Y.; Yao, C.H.; Chen, W.C.; Shen, W.C.; Bau, D.T. Electroacupuncture and Acupuncture Promote the Rat’s Transected Median Nerve Regeneration. Evid. Based Complement. Altern. Med. 2013, 2013, 514610. [Google Scholar] [CrossRef] [Green Version]
- Dubrovsky, G.; Ha, D.; Thomas, A.L.; Zhu, M.; Hubacher, J.; Itoh, T.; Dunn, J.C.Y. Electroacupuncture to Increase Neuronal Stem Cell Growth. Med. Acupunct. 2020, 32, 16–23. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Sociodemographic Data | Acupuncture Group (N = 10) | Sham Acupuncture Group (N = 10) | Total (N = 20) | p-Value |
|---|---|---|---|---|
| Age (years) | 47.10 (11.07) | 52.10 (11.18) | 49.60 (11.13) | 0.33 § |
| Sex (Female/Male) | 10/0 | 10/0 | 20/0 | -- ‡ |
| BMI | 24.96 (5.99) | 23.34 (2.79) | 24.15 (4.62) | 0.45 § |
| Past history † | ||||
| DM | 0 (0) | 0 (0) | 0 (0) | -- ‡ |
| HTN | 1 (10) | 1 (10) | 2 (10) | 1.00 ‡ |
| Others | 0 (0) | 2 (20) | 2 (10) | 0.47 ‡ |
| None | 7 (70) | 5 (50) | 12 (60) | 0.65 ‡ |
| Family history † | ||||
| Breast cancer | 1 (10) | 1 (10) | 2 (10) | 1.00 ‡ |
| Other cancer | 5 (50) | 6 (60) | 11 (55) | 1.00 ‡ |
| Other diseases | 3 (30) | 2 (20) | 5 (25) | 1.00 ‡ |
| None | 3 (30) | 1 (10) | 4 (20) | 0.58 ‡ |
| Occupation | 1.00 ‡ | |||
| Employed | 5 (50) | 4 (50) | 9 (45) | |
| Unemployed | 5 (50) | 6 (60) | 11 (20) | |
| Breast cancer stages | 0.52 ‡ | |||
| I | 1 (10) | 3 (30) | 4 (20) | |
| II | 3 (30) | 4 (40) | 7 (35) | |
| III | 6 (60) | 3 (30) | 9 (45) | |
| Type of Chemotherapy † | ||||
| Docetaxel | 10 (100) | 10 (100) | 20 (100) | -- ‡ |
| Carboplatin | 1 (10) | 2 (20) | 3 (15) | 1.00 ‡ |
| Other taxanes | 0 (0) | 0 (0) | 0 (0) | -- ‡ |
| Other platinum | 0 (0) | 0 (0) | 0 (0) | -- ‡ |
| Cumulative doses (mg) | ||||
| Docetaxel | 635.80 (119.82) | 622.80 (78.18) | 629.30 (98.70) | 0.78 § |
| Carboplatin | 474 (1498.92) | 864 (1835.47) | 669.00 (1643.20) | 0.74 ¶ |
| ECOG | 1.00 ‡ | |||
| 0 | 10 (100) | 9 (90) | 19 (95) | |
| 1 | 0 (0) | 1 (10) | 1 (5) | |
| NCI-CTCAE | 1.00 ‡ | |||
| 1 | 8 (80) | 9 (90) | 17 (85) | |
| 2 | 2 (20) | 1 (10) | 3 (15) | |
| Interval from the end of chemotherapy to acupuncture treatment (days) | 277.90 (464.01) | 115.90 (101.98) | 196.90 (337.37) | 0.64 § |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-C.; Ho, T.-J.; Ho, H.-Y.; Chen, P.-Y.; Tu, C.-H.; Huang, Y.-C.; Lee, Y.-C.; Sun, M.-F.; Chen, Y.-H. Acupuncture Relieved Chemotherapy-Induced Peripheral Neuropathy in Patients with Breast Cancer: A Pilot Randomized Sham-Controlled Trial. J. Clin. Med. 2021, 10, 3694. https://doi.org/10.3390/jcm10163694
Huang C-C, Ho T-J, Ho H-Y, Chen P-Y, Tu C-H, Huang Y-C, Lee Y-C, Sun M-F, Chen Y-H. Acupuncture Relieved Chemotherapy-Induced Peripheral Neuropathy in Patients with Breast Cancer: A Pilot Randomized Sham-Controlled Trial. Journal of Clinical Medicine. 2021; 10(16):3694. https://doi.org/10.3390/jcm10163694
Chicago/Turabian StyleHuang, Chien-Chen, Tsung-Jung Ho, Hsin-Yueh Ho, Pei-Yu Chen, Cheng-Hao Tu, Yu-Chuen Huang, Yu-Chen Lee, Mao-Feng Sun, and Yi-Hung Chen. 2021. "Acupuncture Relieved Chemotherapy-Induced Peripheral Neuropathy in Patients with Breast Cancer: A Pilot Randomized Sham-Controlled Trial" Journal of Clinical Medicine 10, no. 16: 3694. https://doi.org/10.3390/jcm10163694