
Prognostic Value of Cardiac Troponin and Risk Assessment in Pediatric Supraventricular Tachycardia

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
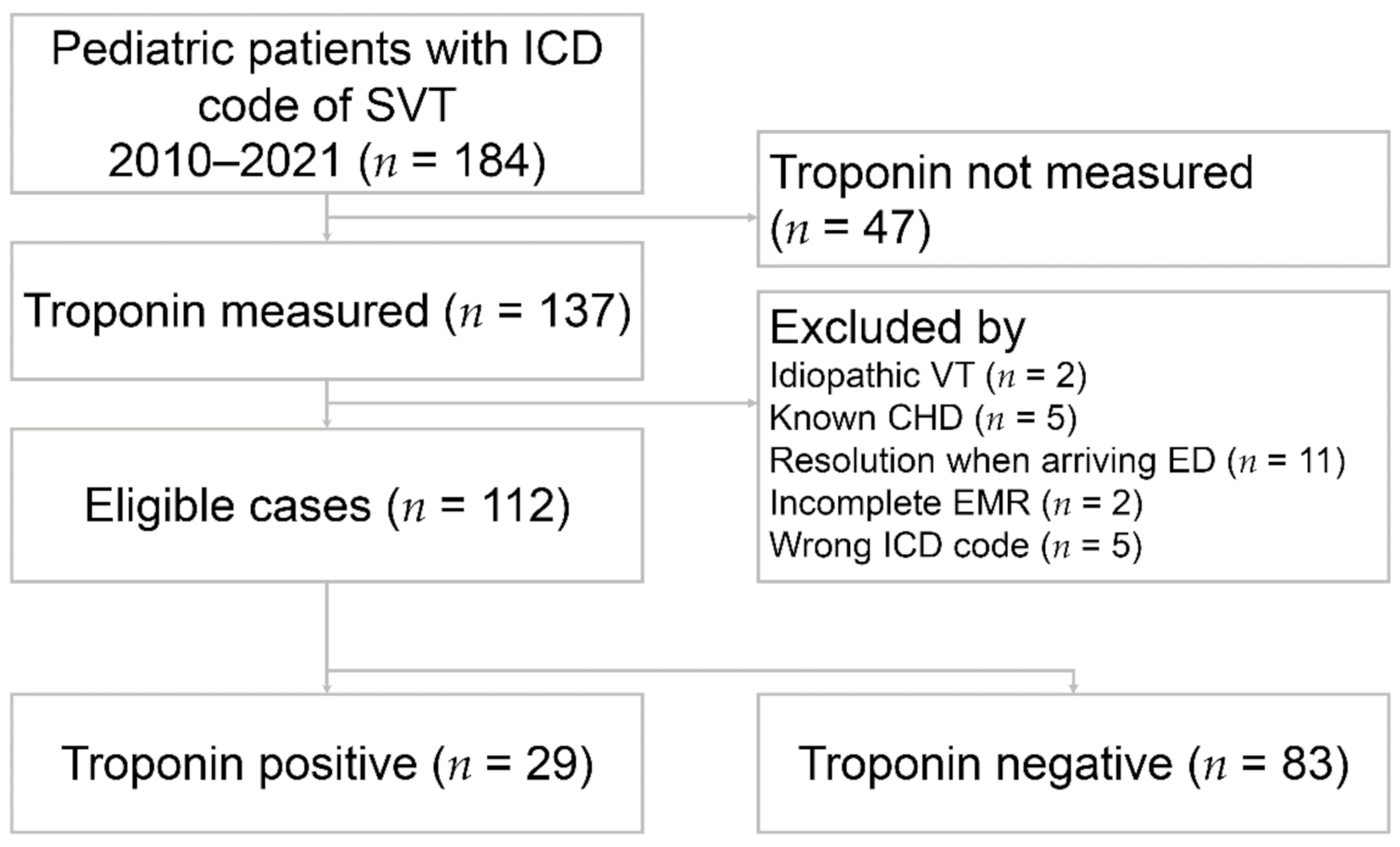
2.2. Patient Selection and Data Collection
2.3. Measurement of Cardiac Troponin I
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- L’Italien, K.; Conlon, S.; Kertesz, N.; Bezold, L.; Kamp, A. Usefulness of Echocardiography in Children with New-Onset Supraventricular Tachycardia. J. Am. Soc. Echocardiogr. 2018, 31, 1146–1150. [Google Scholar] [CrossRef]
- Quattrocelli, A.; Lang, J.; Davis, A.; Pflaumer, A. Age makes a difference: Symptoms in pediatric supraventricular tachycardia. J. Arrhythmia 2018, 34, 565–571. [Google Scholar] [CrossRef]
- Yetkin, E.; Ozturk, S.; Cuglan, B.; Turhan, H. Clinical presentation of paroxysmal supraventricular tachycardia: Evaluation of usual and unusual symptoms. Cardiovasc. Endocrinol. Metab. 2020, 9, 153–158. [Google Scholar] [CrossRef]
- Wood, K.A.; Drew, B.J.; Scheinman, M.M. Frequency of Disabling Symptoms in Supraventricular Tachycardia. Am. J. Cardiol. 1997, 79, 145–149. [Google Scholar] [CrossRef]
- Moore, J.P.; Arcilla, L.; Wang, S.; Lee, M.S.; Shannon, K.M. Characterization of Cardiac Troponin Elevation in the Setting of Pediatric Supraventricular Tachycardia. Pediatr. Cardiol. 2015, 37, 392–398. [Google Scholar] [CrossRef]
- Bagai, A.; Alexander, K.P.; Berger, J.; Senior, R.; Sajeev, C.; Pracon, R.; Mavromatis, K.; Lopez-Sendón, J.L.; Gosselin, G.; Diaz, A.; et al. Use of troponin assay 99th percentile as the decision level for myocardial infarction diagnosis. Am. Heart J. 2017, 190, 135–139. [Google Scholar] [CrossRef]
- Peacock, W.F.; De Marco, T.; Fonarow, G.; Diercks, D.B.; Wynne, J.; Apple, F.S.; Wu, A.H. Cardiac Troponin and Outcome in Acute Heart Failure. N. Engl. J. Med. 2008, 358, 2117–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korff, S.; Katus, H.A.; Giannitsis, E. Differential diagnosis of elevated troponins. Heart 2006, 92, 987–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousufuddin, M.; Abdalrhim, A.D.; Wang, Z.; Murad, M.H. Cardiac troponin in patients hospitalized with acute decompensated heart failure: A systematic review and meta-analysis. J. Hosp. Med. 2016, 11, 446–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghersin, I.; Zahran, M.; Azzam, Z.S.; Suleiman, M.; Bahouth, F. Prognostic value of cardiac troponin levels in patients presenting with supraventricular tachycardias. J. Electrocardiol. 2020, 62, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Fernando, H.; Adams, N.; Mitra, B. Review article: The utility of troponin and other investigations in patients presenting to the emergency department with supraventricular tachycardia. Emerg. Med. Australas. 2019, 31, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Bukkapatnam, R.N.; Robinson, M.; Turnipseed, S.; Tancredi, D.; Amsterdam, E.; Srivatsa, U.N. Relationship of myocardial ischemia and injury to coronary artery disease in patients with supraventricular tachycardia. Am. J. Cardiol. 2010, 106, 374–377. [Google Scholar] [CrossRef]
- Bratincsák, A.; Kimata, C.; Limm-Chan, B.N.; Vincent, K.P.; Williams, M.R.; Perry, J.C. Electrocardiogram Standards for Children and Young Adults Using Z -Scores. Circ. Arrhythmia Electrophysiol. 2020, 13, 008253. [Google Scholar] [CrossRef] [PubMed]
- Murer, M.; Cuculi, F.; Toggweiler, S.; Weberndoerfer, V.; Young, M.; Kobza, R. Elevated high-sensitivity troponin does not indicate the presence of coronary artery disease in patients presenting with supraventricular tachycardia. Cardiol. J. 2017, 24, 642–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noorvash, D.; Ramos, R.; Hatch, L.; Muck, A.; Olson, A.S. Assessment of the Utility of Ordering a Troponin in Low- and Intermediate-Risk Patients Presenting to the Emergency Department with Supraventricular Tachycardia: A Retrospective Chart Review. J. Emerg. Med. 2018, 55, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sayadnik, M.; Shafiee, A.; Jenab, Y.; Jalali, A.; Sadeghian, S. Predictors of High-Sensitivity Cardiac Troponin T Elevation in Patients with Acute Paroxysmal Supra-ventricular Tachycardia and Ischemic Heart Disease. Tex. Heart Inst. J. 2017, 44, 306–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, R.; deSouza, I.S. Troponin Testing in Patients with Supraventricular Tachycardia—Are We Overtesting? A Teachable Moment. JAMA Intern. Med. 2021, 181, 842–843. [Google Scholar] [CrossRef]
- Maresca, B.; Manzione, A.; Moioli, A.; Salerno, G.; Cardelli, P.; Punzo, G.; Barberi, S.; Menè, P. Prognostic value of high-sensitive cardiac troponin I in asymptomatic chronic hemodialysis patients. J. Nephrol. 2019, 33, 129–136. [Google Scholar] [CrossRef]
- Chow, G.V.; Hirsch, G.A.; Spragg, D.D.; Cai, J.X.; Cheng, A.; Ziegelstein, R.C.; Marine, J.E. Prognostic Significance of Cardiac Troponin I Levels in Hospitalized Patients Presenting with Supraventricular Tachycardia. Medicine 2010, 89, 141–148. [Google Scholar] [CrossRef]
- Ben Yedder, N.; Roux, J.F.; Paredes, F.A. Troponin Elevation in Supraventricular Tachycardia: Primary Dependence on Heart Rate. Can. J. Cardiol. 2011, 27, 105–109. [Google Scholar] [CrossRef]
- Healey, J.S. Troponin Elevation in Patients with Supraventricular Tachycardia: What Does It Mean? Can. J. Cardiol. 2011, 27, 110–111. [Google Scholar] [CrossRef]
- Taskapan, M.C.; Taskapan, H.; Ulutas, O.; Orhan, M.; Sahin, I. Relationships between Brain Natriuretic Peptide, Troponin I and QT Dispersion in Asymptomatic Dialysis Patients. Ren. Fail. 2007, 29, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Higgins, J.A. Elevation of cardiac troponin I indicates more than myocardial ischemia. Clin. Invest. Med. 2003, 26, 133–147. [Google Scholar] [PubMed]
- Snyder, C.S.; Fenrich, A.L.; Friedman, R.A.; Rosenthal, G.; Kertesz, N.J. Usefulness of echocardiography in infants with supraventricular tachycardia. Am. J. Cardiol. 2003, 91, 1277–1279. [Google Scholar] [CrossRef]
- Chandra, M.S.; Kerber, R.E.; Brown, D.D.; Funk, D.C. Echocardiography in Wolff-Parkinson-White syndrome. Circulation 1976, 53, 943–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dallaire, F.; Bigras, J.-L.; Prsa, M.; Dahdah, N. Bias Related to Body Mass Index in Pediatric Echocardiographic Z Scores. Pediatr. Cardiol. 2014, 36, 667–676. [Google Scholar] [CrossRef]
- Ashok, A.; Cabalag, M.; Taylor, D.M. Usefulness of laboratory and radiological investigations in the management of supraventricular tachycardia. Emerg. Med. Australas. 2017, 29, 394–399. [Google Scholar] [CrossRef]
- Bonato, F.O.B.; Canziani, M.E.F. Ventricular arrhythmia in chronic kidney disease patients. Braz. J. Nephrol. 2017, 39, 186–195. [Google Scholar] [CrossRef]
- Mak, W.W.; Nurazni, R.A.R.; Badrulnizam, L.B.M. Severe hypothyroidism presenting with supraventricular tachycardia. Med. J. Malays. 2018, 73, 349–350. [Google Scholar]
- Abbasoğlu, A.; Ecevit, A.; Tuğcu, A.U.; Kınık, S.T.; Tarcan, A. Neonatal thyrotoxicosis with severe supraventricular tachycardia: Case report and review of the literature. J. Pediatr. Endocrinol. Metab. 2015, 28, 463–466. [Google Scholar] [CrossRef]
- Vanin, L.N.; Smetnev, A.S.; Sokolov, S.F.; Kotova, G.A.; Masenko, V.P. Study of thyroid function in patients with paroxysmal supraventricular tachycardia. Kardiologiia 1989, 29, 71–74. [Google Scholar] [PubMed]
- Riggs, T.W.; Byrd, J.A.; Weinhouse, E. Recurrence risk of supraventricular tachycardia in pediatric patients. Cardiology 1999, 91, 25–30. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | cTnI(+) (n = 29) | cTnI(–) (n = 83) | p Value |
|---|---|---|---|
| Age (yr) | 8.6 ± 5.4 | 10.3 ± 4.7 | 0.099 |
| Male | 13 (44.8%) | 37 (44.6%) | 1.000 |
| Previous SVT | 10 (34.5%) | 30 (36.1%) | 1.000 |
| Vital signs | |||
| Peak heart rate (beats/min) | 219.0 ± 42.0 | 200.8 ± 28.5 | 0.037 |
| Peak heart rate (z score) | 6.5 ± 1.6 | 6.3 ± 1.5 | 0.537 |
| Systolic blood pressure (mmHg) | 101.5 ± 18.9 | 108.9 ± 18.5 | 0.084 |
| Diastolic blood pressure (mmHg) | 64.1 ± 12.0 | 70.8 ± 14.0 | 0.027 |
| Hypotension | 6 (21.4%) | 7 (9.2%) | 0.106 |
| Fever † | 2 (6.9%) | 11 (13.3%) | 0.509 |
| Symptoms | |||
| Palpitation | 23 (79.3%) | 69 (83.1%) | 0.779 |
| Chest pain | 7 (24.1%) | 18 (21.7%) | 0.799 |
| Dyspnea | 8 (27.6%) | 6 (7.2%) | 0.008 |
| Dizziness | 2 (6.9%) | 8 (9.6%) | 1.000 |
| Syncope | 0 (0%) | 2 (2.4%) | 1.000 |
| Respiratory | 7 (24.1%) | 12 (14.5%) | 0.257 |
| Gastrointestinal | 7 (24.1%) | 4 (4.8%) | 0.006 |
| SVT duration since ED (min) | 60.5 ± 80.0 | 46.8 ± 78.7 | 0.424 |
| Length of stay (hr) | 48.3 ± 111.5 | 28.4 ± 47.0 | 0.190 |
| Treatment | |||
| Without medication § | 3 (10.3%) | 11 (13.4%) | 1.000 |
| Adenosine use | 25 (86.2%) | 72 (86.7%) | 1.000 |
| Verapamil use | 1 (3.4%) | 4 (4.8%) | 1.000 |
| Amiodarone use | 5 (17.2%) | 10 (12.0%) | 0.530 |
| Radiofrequency ablation ‡ | 16 (34.0%) | 1 (10.0%) | 0.247 |
| ED Disposition | |||
| Ordinary medical ward | 6 (20.7%) | 21 (25.3%) | 0.802 |
| Intensive care unit | 12 (41.4%) | 14 (16.9%) | 0.007 |
| Discharge | 11 (37.9%) | 48 (57.8%) | 0.084 |
| Variable | cTnI(+) (n = 29) | cTnI(–) (n = 83) | p Value |
|---|---|---|---|
| Laboratory exam | |||
| White cell count (103/uL) (n = 107) | 12.45 ± 5.41 ‡ | 10.05 ± 3.57 | 0.01 |
| Hemoglobin (g/dL) (n = 107) | 13.48 ± 1.41 | 13.56 ± 1.34 | 0.775 |
| Platelet (103/uL) (n = 107) | 316.1 ± 89.1 | 285.9 ± 68.0 | 0.06 |
| Blood urea nitrogen (mg/dL) (n = 41) | 12.8 ± 2.8 | 13.2 ± 10.5 | 0.908 |
| Creatinine (mg/dL) (n = 74) | 0.56 ± 0.20 | 0.69 ± 1.17 | 0.622 |
| Sodium (mEq/L) (n = 94) | 139.6 ± 2.2 | 139.4 ± 2.2 | 0.733 |
| Potassium (mEq/L) (n = 93) | 4.12 ± 0.56 | 3.95 ± 0.40 | 0.109 |
| Calcium (mg/dL) (n = 70) | 9.47 ± 0.40 | 9.38 ± 0.52 | 0.488 |
| Magnesium (mEq/L) (n = 39) | 1.85 ± 0.18 | 1.80 ± 0.20 | 0.499 |
| AST (U/L) (n = 70) | 32.50 ± 16.07 | 38.18 ± 46.41 | 0.596 |
| ALT (U/L) (n = 62) | 31.26 ± 48.14 | 0.441 | |
| Initial cTnI (ng/mL) (n = 112) | 0.172 ± 0.163 ‡ | 0.015 ± 0.010 | <0.001 |
| Peak cTnI (n = 112) | 0.256 ± 0.299 ‡ | 0.017 ± 0.008 | <0.001 |
| TSH (uIU/mL) (n = 23) | 2.37 ± 1.41 | 2.31 ± 1.52 | 0.926 |
| Free thyroxine (ng/dL) (n = 20) | 1.26 ± 0.17 | 1.57 ± 1.15 | 0.436 |
| BNP (pg/mL) (n = 19) | 173.4 ± 185.3 ‡ | 163.3 ± 232.9 ‡ | 0.927 |
| C-Reactive Protein (mg/L) (n = 24) | 5.07 ± 9.23 ‡ | 1.13 ± 1.64 | 0.105 |
| Variable | cTnI(+) (n = 29) | cTnI(–) (n = 83) | p Value |
|---|---|---|---|
| SVT mechanism | |||
| AVRT § | 4 (13.8%) | 3 (3.6%) | 0.073 |
| AVNRT | 2 (6.9%) | 14 (16.9%) | 0.232 |
| AT | 0 (0%) | 2 (2.4%) | 1.000 |
| WPW | 8 (27.6%) | 12 (14.5%) | 0.157 |
| Not classified by EP study | 15 (51.7%) | 52 (62.7%) | 0.38 |
| Echocardiography † | (n = 27) | (n = 68) | |
| Normal | 25 (92.6%) | 59 (86.8%) | 0.723 |
| Incidental ‡ | 0 (0%) | 4 (5.9%) | 0.575 |
| Abnormal | 2 (7.4%) | 5 (7.4%) | 1.000 |
| LVEF(%) | 71.83 ± 5.18 | 70.66 ± 8.91 | 0.605 |
| LA diameter (mm) | 20.56 ± 6.26 | 23.20 ± 4.78 | 0.093 |
| LVEDD (mm) | 34.28 ± 10.77 | 38.22 ± 8.95 | 0.160 |
| LVESD (mm) | 20.67 ± 5.96 | 22.36 ± 5.55 | 0.307 |
| Aortic root diameter (mm) | 20.17 ± 5.85 | 21.11 ± 4.31 | 0.506 |
| Variable | cTnI(+) (n = 29) | cTnI(–) (n = 83) | p Value |
|---|---|---|---|
| MACE | 0 (0%) | 1 (0.01%) | 1.000 |
| 30-day SVT recurrence | 6 (20.7%) | 6 (7.2%) | 0.075 |
| Univariate | Multivariable | |||
|---|---|---|---|---|
| OR (95%CI) | p Value | OR (95%CI) | p Value | |
| Age | 0.86 (0.75, 0.98) | 0.022 | 0.87 (0.75, 1.001) | 0.051 |
| Male | 1.27 (0.38, 4.22) | 0.693 | ||
| Peak heart rate (z score) | 0.99 (0.66, 1.49) | 0.965 | ||
| Hypotension | 5.33 (1.31, 21.8) | 0.020 | 4.98 (1.02, 24.22) | 0.047 * |
| cTnI(+) | 3.35 (0.99, 11.4) | 0.053 | 2.52 (0.62, 10.19) | 0.195 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-C.; Chen, S.-Y.; Chaou, C.-H.; Wang, C.-K.; Yeh, H.-T.; Ng, C.-J. Prognostic Value of Cardiac Troponin and Risk Assessment in Pediatric Supraventricular Tachycardia. J. Clin. Med. 2021, 10, 3638. https://doi.org/10.3390/jcm10163638
Yen C-C, Chen S-Y, Chaou C-H, Wang C-K, Yeh H-T, Ng C-J. Prognostic Value of Cardiac Troponin and Risk Assessment in Pediatric Supraventricular Tachycardia. Journal of Clinical Medicine. 2021; 10(16):3638. https://doi.org/10.3390/jcm10163638
Chicago/Turabian StyleYen, Chieh-Ching, Shou-Yen Chen, Chung-Hsien Chaou, Chih-Kai Wang, Hsin-Tzu Yeh, and Chip-Jin Ng. 2021. "Prognostic Value of Cardiac Troponin and Risk Assessment in Pediatric Supraventricular Tachycardia" Journal of Clinical Medicine 10, no. 16: 3638. https://doi.org/10.3390/jcm10163638