
Clinical Characteristics and Outcomes of Adults with Nephrotic Syndrome Due to Minimal Change Disease

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.2. Statistical Methods
3. Results
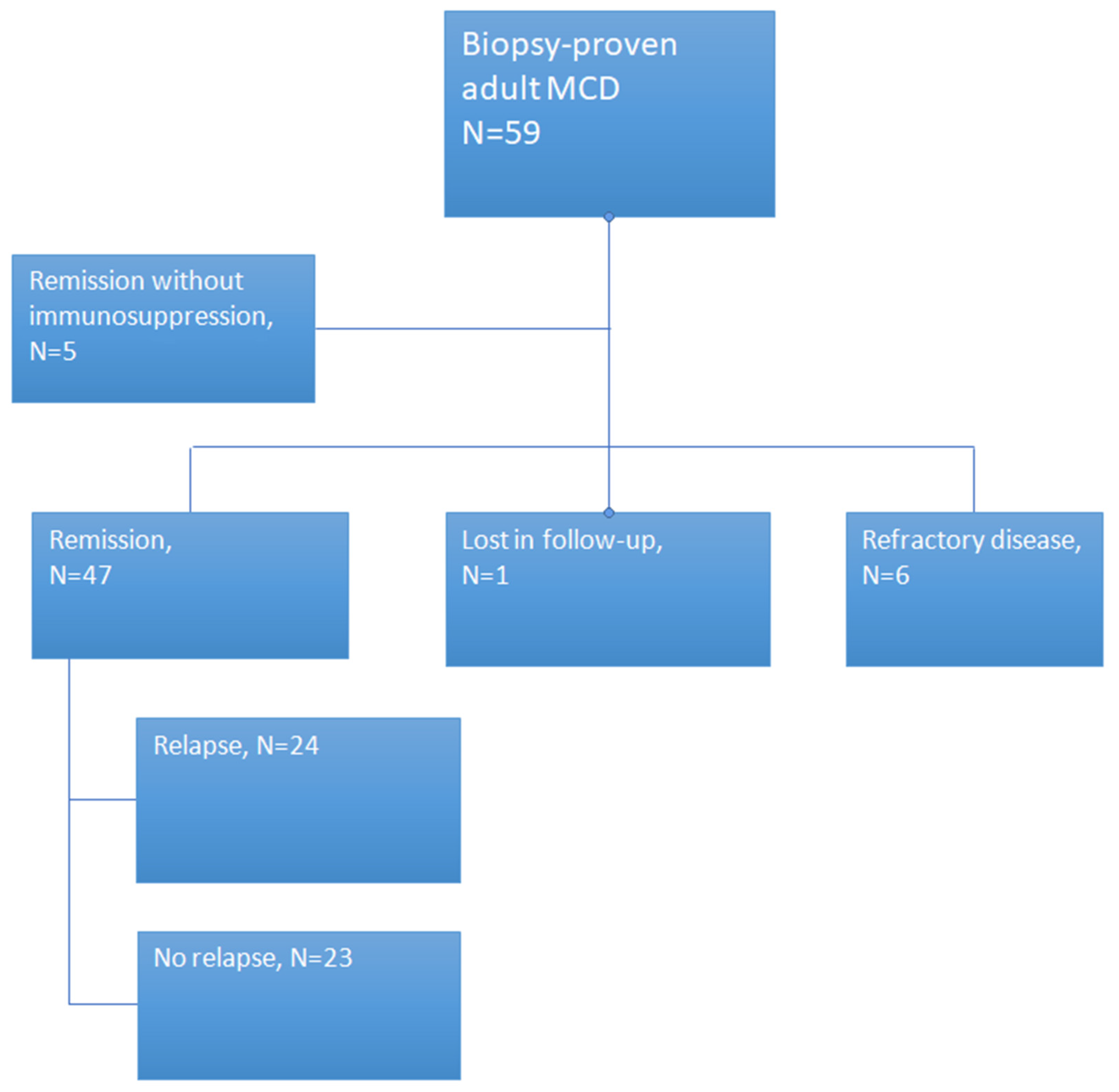
3.1. Description of Study Population
3.1.1. Relapsing Patients
3.1.2. Relapsers versus Non-Relapsers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nachman, P.H.; Jennette, J.C.; Falk, R.J. Primary glomerular disease. In The Kidney, 8th ed.; Brenner, B.M., Ed.; Elsevier: Philadelphia, PA, USA, 2008; pp. 987–1066. [Google Scholar]
- Haas, M.; Meehan, S.M.; Karrison, T.G.; Spargo, B.H. Changing etiologies of unexplained adult nephrotic syndrome: A comparison of renal biopsy findings from 1976–1979 and 1995–1997. Am. J. Kidney Dis. 1997, 30, 621–631. [Google Scholar] [CrossRef]
- Korbet, S.M.; Genchi, R.; Borok, R.; Schwartz, M.M. The racial prevalence of glomerular lesions in nephrotic adults. Am. J. Kidney Dis. 1996, 27, 647–651. [Google Scholar] [CrossRef]
- Cameron, J.S. Nephrotic syndrome in the elderly. Semin. Nephrol. 1996, 16, 319–329. [Google Scholar] [PubMed]
- Schnaper, H.W.; Robson, A.A.; Kopp, J.B. Nephrotic syndrome: Minimal change nephropathy, focal segmental glomerulosclerosis, and collapsing glomerulopathy. In Diseases of the Kidney and Urinary Tract, 8th ed.; Schrier, R.W., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; p. 1585. [Google Scholar]
- Zech, P.; Colon, S.; Pointet, P.; Deteix, P.; Labeeuw, M.; Leitienne, P. The nephrotic syndrome in adults aged over 60: Etiology, evolution and treatment of 76 cases. Clin. Nephrol. 1982, 17, 232–236. [Google Scholar] [PubMed]
- Keskar, V.; Jamale, T.E.; Kulkarni, M.J.; Jagadish, P.K.; Fernandes, G.; Hase, N. Minimal-change disease in adolescents and adults: Epidemiology and therapeutic response. Clin. Kidney J. 2013, 6, 469–472. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, T.; Simon, S.D.; Alon, U.S. High incidence of focal segmental glomerulosclerosis in nephrotic syndrome of childhood. Pediatr. Nephrol. 1999, 13, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Jennette, J.C.; Falk, R.J. Adult minimal change glomerulopathy with acute renal failure. Am. J. Kidney Dis. 1990, 16, 432–437. [Google Scholar] [CrossRef]
- Lee, H.; Yoo, K.D.; Oh, Y.K.; Kim, D.K.; Oh, K.-H.; Joo, K.W.; Kim, Y.S.; Ahn, C.; Han, J.S.; Lim, C.S. Predictors of relapse in adult-onset nephrotic minimal change disease. Medicina 2016, 95, e3179. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Marshall, G.D. Role of CD28/B7 costimulation in the dexamethasone-induced suppression of IFN-γ. J. Interf. Cytokine Res. 2000, 20, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Waldman, M.; Crew, R.J.; Valeri, A.; Busch, J.; Stokes, M.; Markowitz, G.; D’Agati, V.; Appel, G. Adult minimal-change disease: Clinical characteristics, treatment, and outcomes. Clin. J. Am. Soc. Nephrol. 2007, 2, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Niaudet, P.; Meyrier, A. Minimal change disease: Clinical features and diagnosis. In Oxford Textbook of Clinical Nephrology, 4th ed.; Turner, N., Lameire, N., Goldsmith, D.J., Eds.; Oxford University Press: Oxford, UK, 2016; Volume 1, p. 501. [Google Scholar]
- Fenton, A.; Smith, S.W.; Hewins, P. Adult minimal-change disease: Observational data from a UK centre on patient characteristics, therapies, and outcomes. BMC Nephrol. 2018, 19, 207. [Google Scholar] [CrossRef]
- Dias, C.B.; Pinheiro, C.C.; Silva, V.D.S.; Hagemann, R.; Barros, R.T.; Woronik, V. Proteinuria predicts relapse in adolescent and adult minimal change disease. Clinics 2012, 67, 1271–1274. [Google Scholar] [CrossRef]
- Nakayama, M.; Katafuchi, R.; Yanase, T.; Ikeda, K.; Tanaka, H.; Fujimi, S. Steroid responsiveness and frequency of relapse in adult-onset minimal change nephrotic syndrome. Am. J. Kidney Dis. 2002, 39, 503–512. [Google Scholar] [CrossRef]
- Korbet, S.M.; Schwartz, M.M.; Lewis, E.J. Minimal-change glomerulopathy of adulthood. Am. J. Nephrol. 1988, 8, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Ruggenenti, P.; Ruggiero, B.; Cravedi, P.; Vivarelli, M.; Massella, L.; Marasà, M.; Chianca, A.; Rubis, N.; Ene-Iordache, B.; Rudnicki, M.; et al. Rituximab in steroid-dependent or frequently relapsing idiopathic nephrotic syndrome. J. Am. Soc. Nephrol. 2014, 25, 850–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trautmann, A.; Schnaidt, S.; Lipska-Ziętkiewicz, B.S.; Bodria, M.; Ozaltin, F.; Emma, F.; Anarat, A.; Melk, A.; Azocar, M.; Oh, J.; et al. Long-term outcome of steroid-resistant nephrotic syndrome in children. J. Am. Soc. Nephrol. 2017, 28, 3055–3065. [Google Scholar] [CrossRef] [Green Version]
- Ozeki, T.; Ando, M.; Yamaguchi, M.; Katsuno, T.; Kato, S.; Yasuda, Y.; Tsuboi, N.; Maruyama, S. Treatment patterns and steroid dose for adult minimal change disease relapses: A retrospective cohort study. PLoS ONE 2018, 13, e0199228. [Google Scholar] [CrossRef] [Green Version]
- Vivarelli, M.; Massella, L.; Ruggiero, B.; Emma, F. Minimal change disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 332–345. [Google Scholar] [CrossRef] [Green Version]
- Nolasco, F.; Cameron, J.S.; Heywood, E.; Hicks, J.; Ogg, C.; Williams, D.G. Adult-onset minimal change nephrotic syndrome: A long-term follow-up. Kidney Int. 1986, 29, 1215–1223. [Google Scholar] [CrossRef] [Green Version]
- Rüth, E.-M.; Kemper, M.J.; Leumann, E.P.; Laube, G.F.; Neuhaus, T.J. Children with steroid-sensitive nephrotic syndrome come of age: Long-term outcome. J. Pediatr. 2005, 147, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Fakhouri, F.; Bocquet, N.; Taupin, P.; Presne, C.; Gagnadoux, M.-F.; Landais, P.; Lesavre, P.; Chauveau, D.; Knebelmann, B.; Broyer, M.; et al. Steroid-sensitive nephrotic syndrome: From childhood to adulthood. Am. J. Kidney Dis. 2003, 41, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Avner, E.D.; Harmon, W.E.; Niaudet, P.; Yoshikawa, N.; Emma, F.; Goldstein, S.L. Idiopathic nephrotic syndrome in children: Clinical aspects. In Pediatric Nephrology, 7th ed.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 27–30. [Google Scholar]
- Emma, F.; Sesto, A.; Rizzoni, G. Long-term linear growth of children with severe steroid-responsive nephrotic syndrome. Pediatr. Nephrol. 2003, 18, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Mariani, L.H.; Bomback, A.S.; Canetta, P.A.; Flessner, M.F.; Helmuth, M.; Hladunewich, M.A.; Hogan, J.J.; Kiryluk, K.; Nachman, P.H.; Nast, C.C.; et al. CureGN study rationale, design, and methods: Establishing a large prospective observational study of glomerular disease. Am. J. Kidney Dis. 2019, 73, 218–229. [Google Scholar] [CrossRef] [PubMed]
- Munyentwali, H.; Bouachi, K.; Audard, V.; Remy, P.; Lang, P.; Mojaat, R.; Deschenes, G.; Ronco, P.M.; Plaisier, E.M.; Dahan, K.Y. Rituximab is an efficient and safe treatment in adults with steroid-dependent minimal change disease. Kidney Int. 2013, 83, 511–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoxha, E.; Stahl, R.A.; Harendza, S. Rituximab in adult patients with immunosuppressive-dependent minimal change disease. Clin. Nephrol. 2011, 76, 151–158. [Google Scholar] [CrossRef]
- Sinha, A.; Bagga, A. Rituximab therapy in nephrotic syndrome: Implications for patients’ management. Nat. Rev. Nephrol. 2013, 9, 154–169. [Google Scholar] [CrossRef]
- Iwabuchi, Y.; Takei, T.; Moriyama, T.; Itabashi, M.; Nitta, K. Long-term prognosis of adult patients with steroid-dependent minimal change nephrotic syndrome following rituximab treatment. Medicina 2014, 93, e300. [Google Scholar] [CrossRef] [Green Version]
- King, C.; Logan, S.; Smith, S.W.; Hewins, P. The efficacy of rituximab in adult frequently relapsing minimal change disease. Clin. Kidney J. 2016, 10, 16–19. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean (SD) or N (%) |
|---|---|
| Age at start of symptoms | 47 (17.25) |
| Proteinuria duration before biopsy (weeks) | 8.8 (22.5) |
| Age at diagnosis (biopsy) | 47 (17.25) |
| Gender (males) | 35 (59.3) |
| Menopause (yes) | 10 (41.6) |
| Race (Caucasians) | 55 (98.2) |
| History of Smoking status | 14 (23.7) |
| Current | 8 (57.1) |
| Ex-smoker | 2 (14.3) |
| Never | 4 (28.6) |
| BMI | 26.9 (4.7) |
| Serum creatinine at biopsy, (mg/dL) | 0.8 (2.5) |
| Serum total protein, (g/dL) | 4.8 (1.1) |
| Serum albumin, (g/dL) | 2.5 (0.8) |
| Serum cholesterol, (mg/dL) | 360.5 (118.15) |
| Triglycerides, (mg/dL) | 177.5 (87.5) |
| Estimated GFR mL/min/1.73 m2 | 87 (29.5) |
| 24 h proteinuria biopsy (g) | 6.8 (3.7) |
| Urine analysis protein at biopsy | |
| + | 0 |
| ++ | 9 (15.2) |
| +++ | 27 (45.7) |
| >3+ | 22 (37.2) |
| Urine analysis hematuria at biopsy | 58 |
| + | 24 (40) |
| ++ | 8 (13.5) |
| +++ | 3 (5) |
| >3+ | 0 |
| Edema at biopsy | |
| + | 11 (18.6) |
| ++ | 16 (27.1) |
| +++ | 9 (15.2) |
| >3+ | 12 (20.3) |
| History of Diabetes mellitus | 2 (3.3) |
| History of hypertension | 23(38.9) |
| History of Lung disease | 3(5) |
| Single kidney | 1(1.6) |
| Malignancy | 3 (5) |
| Treatment for MCD | |
| ACE Inhibitor, | 26 (55.9) |
| AT-II (yes) | 6 (10) |
| Diuretics | 29 (49.15) |
| Other anti-hypertensives | 20 (33.8) |
| Glucocorticoids alone | 42 (77.7) |
| Cyclosporine plus glucocorticoids | 5 (9.2) |
| Cyclophosphamide plus glucocorticoids | 6 (11.1) |
| Rituximab plus glucocorticoids | 1(1.8) |
| Patients with Remission (complete or partial) | 52/59 (88.1) |
| Patients with Relapse | 24/52 (46.1) |
| Relapse (episodes per patient) | 2.4 (2.1) |
| Acute kidney injury | 6 (10) |
| Acute dialysis requirement | 4 (6) |
| Estimated GFR (end follow up), mL/min/1.72 m2 | 82 (29.1) |
| Patients with End stage kidney disease | 1(1.7) |
| Death (any cause) | 3 (5) |
| Characteristic | No Relapse N = 23 | Relapse N = 24 (All fup) | p-Value |
|---|---|---|---|
| Age at start of symptoms (years) | 51.65 (±17.3) | 41.08 (±15.2) | 0.03 |
| Age at diagnosis (years) | 51.73 (±17.3) | 41.20 (±15.4) | 0.03 |
| Gender (males) | 10 (0.4) | 14 (0.6) | 0.38 |
| Menopause (yes) | 3 (0.4) | 6 (0.6) | 0.34 |
| Race (Caucasians) | 19 (0.95) | 24 (1) | 0.45 |
| Smoker | 7 (0.3) | 5 (0.5) | 0.99 |
| Current | 4 (0.2) | 3 (0.3) | |
| Ex-smoker | 1(0.04) | 0 | |
| Never | 2 (0.08) | 2 (0.2) | |
| Body mass index | 31 (±3.9) | 23.1 (±3.5) | |
| History of diabetes mellitus | 1(0.4) | 1(0.04) | 1 |
| History of hypertension | 9 (0.4) | 7(0.3) | 0.54 |
| History of lung disease | 2 (0.9) | 0 | 0.23 |
| Single kidney | 0 | 1(0.4) | 1 |
| History of malignancy | 2(0.9) | 0 | 0.23 |
| Characteristic | No Relapse N = 23 | Relapse N = 24 | p-Value |
|---|---|---|---|
| Duration of proteinuria prior to biopsy (weeks) | 6.3 (±10.85) | 11.5 (±33.3) | 0.05 |
| Serum creatinine at biopsy (mg/dL) | 1.8 (±3.9) | 0.9 (±0.4) | 0.31 |
| Serum total protein (g/dL) | 4.9 (±0.85) | 4.65 (±0.9) | 0.27 |
| Serum albumin (g/dL) | 2.5 (±0.7) | 2.45 (±0.7) | 0.82 |
| Serum cholesterol (mg/dL) | 349.3 (±101.9) | 382.5 (±99.9) | 0.30 |
| Triglycerides (mg/dL) | 169.1 (±90.5) | 220.05 (±91.4) | 0.08 |
| Estimated GFR (mL/min/1.73 m2) | 78.4 (±31.9) | 91.2 (±28.7) | 0.16 |
| 24 h proteinuria biopsy (g) | 7961(±4095) | 7326 (±2704) | 0.53 |
| Urine analysis protein at biopsy | 0.79 | ||
| + | 0 | 0 | |
| ++ | 3 (0.1) | 2 (0.1) | |
| +++ | 1(0.5) | 10 (0.4) | |
| >3+ | 9 (0.4) | 11(0.5) | |
| Urine analysis hematuria at biopsy | 0.58 | ||
| + | 9 (0.4) | 8 (0.3) | |
| ++ | 2 (0.04) | 4 (0.2) | |
| +++ | 2 (0.04) | 1(0.04) | |
| >3+ | 0 | 0 | |
| Edema at biopsy | 0.11 | ||
| + | 7 (0.3) | 3 (0.1) | |
| ++ | 5 (0.2) | 8 (0.4) | |
| +++ | 6 (0.3) | 2 (0.1) | |
| >3 | 3 (0.1) | 7 (0.3) |
| Characteristic N (%) or Mean (SD) | No Relapse N = 23 | Relapse N = 24 | p-Value |
|---|---|---|---|
| ACE-Inhibitor | 6 (0.3) | 10(0.4) | 0.35 |
| AT-II | 3 (0.1) | 2(0.08) | 0.66 |
| Diuretics | 3 (0.1) | 8(0.33) | 0.16 |
| Other anti-hypertensives | 9 (0.4) | 3(0.125) | 0.04 |
| Initial immunosuppressive therapy: Number of patients treated with: Glucocorticoids alone Cyclosporine plus glucocorticoids Cyclophosphamide plus glucocorticoids Rituximab plus glucocorticoids | 23 17 (73.9) 2 (8.7) 3 (13.0) 1 (0.4) | 24 21 (88) 1 (4) 2 (8) 0 | 0.23 0.24 0.99 1 |
| Patients with Remission | 23 (1) | 24(1) | 0.48 |
| Time to 1st Remission (days) | 73.05 (±31.5) | 72.8 (±58.1) | 0.99 |
| 24 h proteinuria at 1st remission (mg/day) | 1711(±1037) | 668 (±266) | 0.25 |
| Serum creatinine at 1st remission (mg/dL) | 0.9 (±0.3) | 0.9 (±0.3) | 0.91 |
| Estimated GFR at 1st remission-(mL/min/1.73 m2) | 84.5 (±25.4) | 92.4 (±25.1) | 0.32 |
| Serum albumin at 1st remission (g/dL) | 3.7 (±0.9) | 3.6 (±0.7) | 1 |
| Serum cholesterol at 1st remission (mg/dL) | 216.57 (±46.7) | 310.6 (±134.5) | 0.01 |
| 24 h proteinuria at end follow up, (mg) | 289.22 (±271.1) | 3631 (±1109.2) | 0.38 |
| Estimated GFR at end follow up, (mL/min/1.73 m2) | 85.1 (±27.8) | 92.6 (±23.9) | 0.38 |
| Therapy for 1stRelapse Number of patients treated with: Glucocorticoids alone Cyclosporine plus glucocorticoids Cyclophosphamide plus glucocorticoids | NA | 16 (0.7) 3 (0.1) 4 (0.2) | |
| Therapy for 2ndRelapse Number of patients treated with: Glucocorticoids alone Cyclosporine plus glucocorticoids Cyclophosphamide plus glucocorticoids | NA | 7 (0.5) 3 (0.2) 5 (0.3) | |
| Therapy of 3rdrelapse Number of patients treated with: Glucocorticoids alone Cyclosporine plus glucocorticoids Cyclophosphamide plus glucocorticoids | NA | 3 (0.4) 2 (0.25) 3 (0.4) | |
| Patients with Acute Kidney Injury | 4 (0.17) | 0 | 0.04 |
| Acute dialysis requirement | 3 (0.1) | 0 | 0.1 |
| Patients with End Stage Kidney Disease | 0 | 0 | 1 |
| Death (any cause) | 1(0.04) | 1(0.04) | 1 |
| Variable | Unadjusted OR (95% CI) | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|
| Age at onset (years) | 0.95 (0.91–0.98) | 0.91 (0.83–0.99) | 0.035 |
| Gender (males) | 0.91 (0.29–2.82) | 3.24 (0.47–22.21) | 0.113 |
| eGFR (mL/min/1.73 m2) | 1.01 (0.99–1.03) | 0.97 (0.93–1.02) | 0.342 |
| 24-hrproteinuria (g) | 0.90 (0.75–1.05) | 0.77 (0.55–1.08) | 0.065 |
| Time to remission (months) | 0.95 (0.82–1.09) | 0.79 (0.59–1.06) | 0.237 |
| History of hypertension | 0.77 (0.23–2.50) | 2.28 (0.39–13.38) | 0.341 |
| Initial immunosuppressive therapy | |||
| Cyclophosphamide + glucocorticoids | 0.73 (0.11–4.70) | 4.34 (0.29–64.83) | 0.297 |
| Cyclosporine + glucocorticoids | 0.72 (0.05–9.74) | 1.40 (0.07–27.60) | 0.606 |
| ACE inhibitors | 1.32 (0.41–4.28) | 6.87 (0.76–61.79) | 0.185 |
| ATII inhibitors | 0.88 (0.17–4.36) | 21.16 (0.88–507.81) | 0.155 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lionaki, S.; Mantios, E.; Tsoumbou, I.; Marinaki, S.; Makris, G.; Liapis, G.; Vergandis, C.; Boletis, I. Clinical Characteristics and Outcomes of Adults with Nephrotic Syndrome Due to Minimal Change Disease. J. Clin. Med. 2021, 10, 3632. https://doi.org/10.3390/jcm10163632
Lionaki S, Mantios E, Tsoumbou I, Marinaki S, Makris G, Liapis G, Vergandis C, Boletis I. Clinical Characteristics and Outcomes of Adults with Nephrotic Syndrome Due to Minimal Change Disease. Journal of Clinical Medicine. 2021; 10(16):3632. https://doi.org/10.3390/jcm10163632
Chicago/Turabian StyleLionaki, Sophia, Evangelos Mantios, Ioanna Tsoumbou, Smaragdi Marinaki, George Makris, George Liapis, Chrysovalantis Vergandis, and Ioannis Boletis. 2021. "Clinical Characteristics and Outcomes of Adults with Nephrotic Syndrome Due to Minimal Change Disease" Journal of Clinical Medicine 10, no. 16: 3632. https://doi.org/10.3390/jcm10163632