
Development and Validation of a Bayesian Network for Supporting the Etiological Diagnosis of Uveitis

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
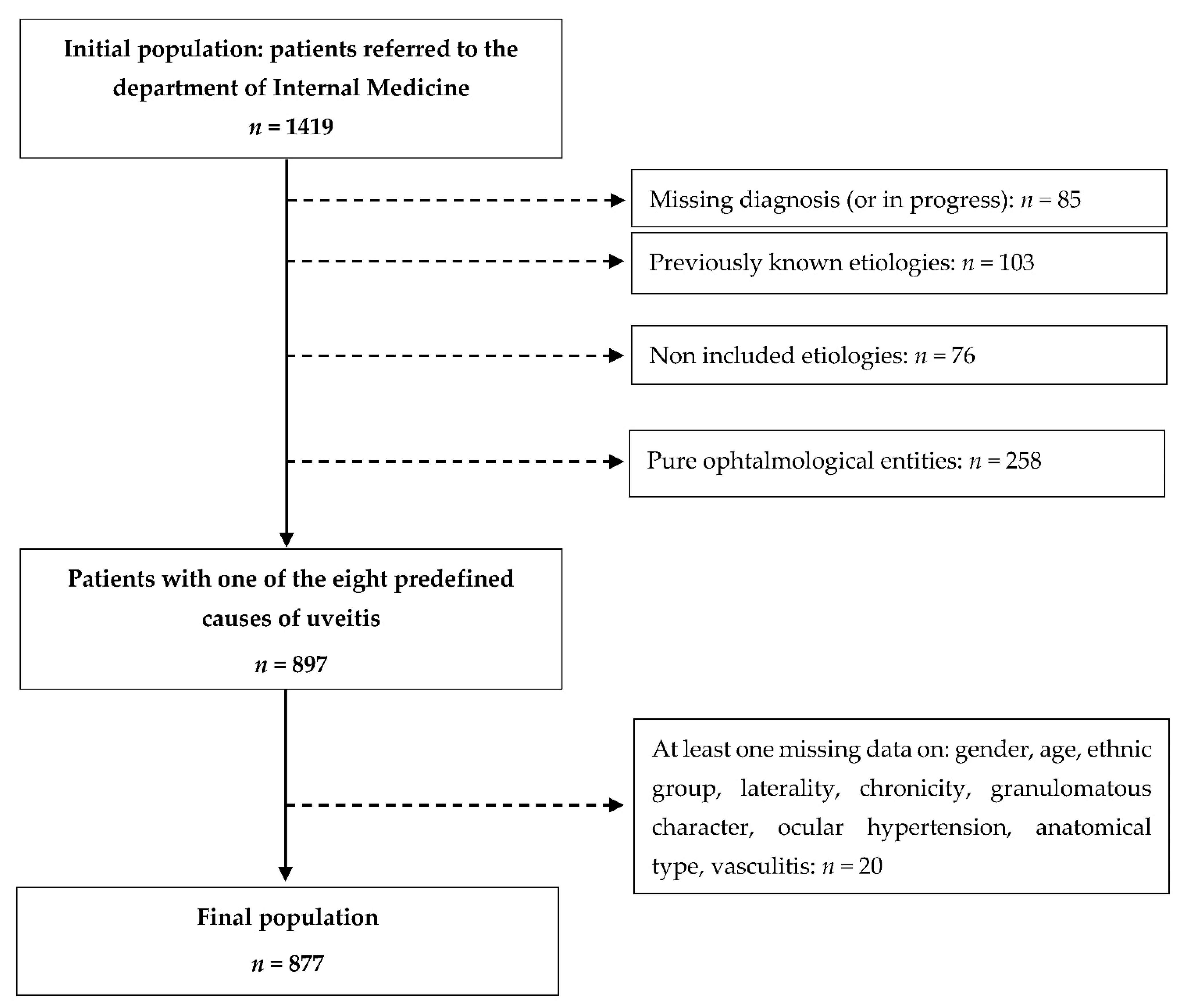
2.1. Datasets
2.2. Definitions
2.3. Study Factors
2.4. Selected Uveitis Causes
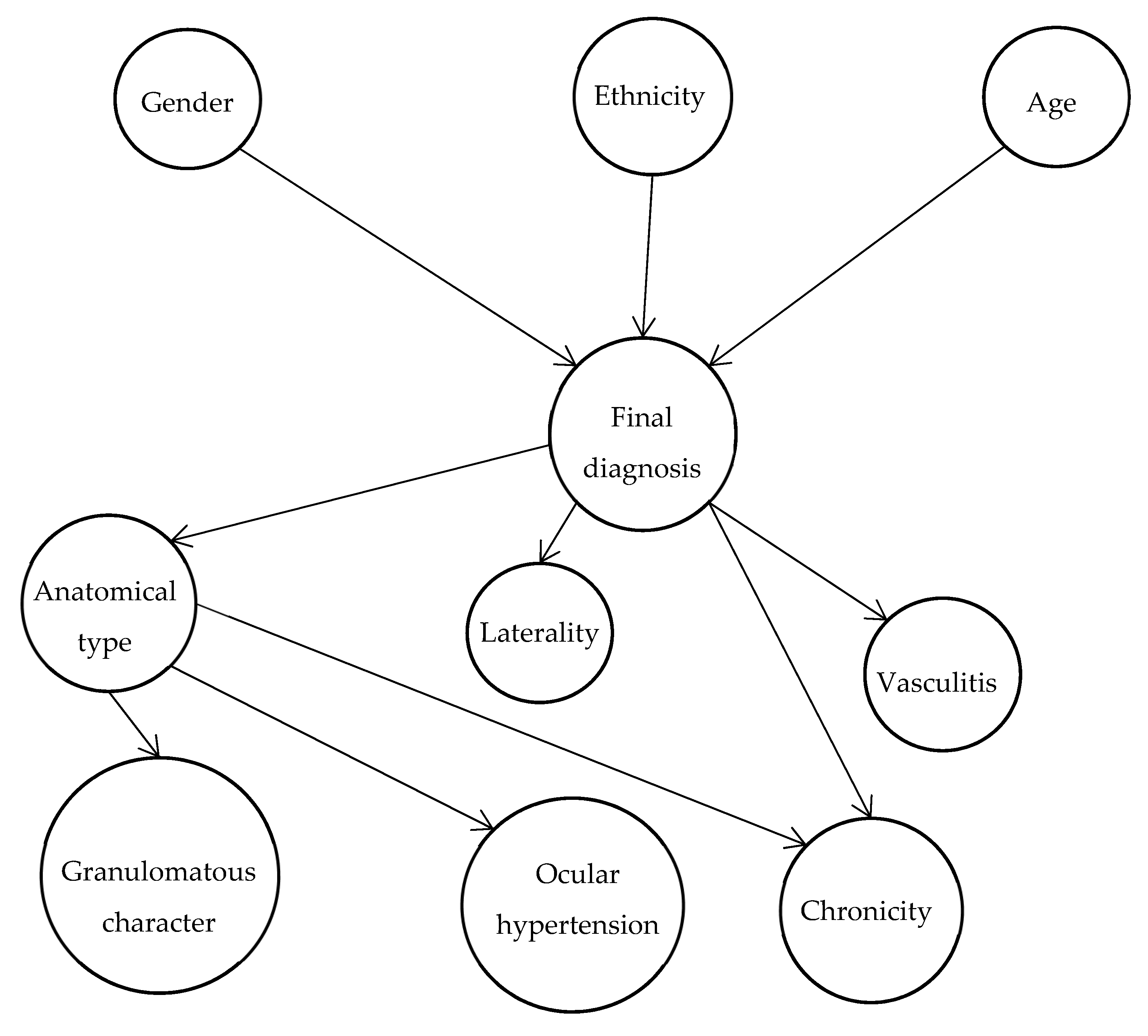
2.5. Bayesian Networks
2.6. Ethic Statement
3. Results
3.1. Description of the Study Populations
3.1.1. Training Dataset
3.1.2. Test Dataset
3.2. Precision, Sensitivity and Specificity Estimates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prete, M.; Dammacco, R.; Fatone, M.C.; Racanelli, V. Autoimmune uveitis: Clinical, pathogenetic, and therapeutic features. Clin. Exp. Med. 2016, 16, 125–136. [Google Scholar] [CrossRef]
- Gritz, D.C.; Wong, I.G. Incidence and prevalence of uveitis in Northern California; The Northern California epidemiology of uveitis study. Ophthalmology 2004, 111, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Rim, T.H.; Kim, S.S.; Ham, D.-I.; Yu, S.-Y.; Chung, E.J.; Lee, S.C. Korean uveitis society incidence and prevalence of uveitis in South Korea: A nationwide cohort study. Br. J. Ophthalmol. 2018, 102, 79–83. [Google Scholar] [CrossRef]
- Chen, S.-C.; Sheu, S.-J. Recent advances in managing and understanding uveitis. F1000Research 2017, 6, 280. [Google Scholar] [CrossRef] [Green Version]
- El Jammal, T.; Loria, O.; Jamilloux, Y.; Gerfaud-Valentin, M.; Kodjikian, L.; Sève, P. Uveitis as an open window to systemic inflammatory diseases. J. Clin. Med. 2021, 10, 281. [Google Scholar] [CrossRef]
- Sève, P.; Cacoub, P.; Bodaghi, B.; Trad, S.; Sellam, J.; Bellocq, D.; Bielefeld, P.; Sène, D.; Kaplanski, G.; Monnet, D.; et al. Uveitis: Diagnostic work-up. A literature review and recommendations from an expert committee. Autoimmun. Rev. 2017, 16, 1254–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keino, H.; Nakashima, C.; Watanabe, T.; Taki, W.; Hayakawa, R.; Sugitani, A.; Okada, A.A. Frequency and clinical features of intraocular inflammation in Tokyo. Clin. Experiment. Ophthalmol. 2009, 37, 595–601. [Google Scholar] [CrossRef]
- Jones, N.P. The Manchester uveitis clinic: The first 3000 patients—Epidemiology and casemix. Ocul. Immunol. Inflamm. 2015, 23, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Barisani-Asenbauer, T.; Maca, S.M.; Mejdoubi, L.; Emminger, W.; Machold, K.; Auer, H. Uveitis—A rare disease often associated with systemic diseases and infections—A systematic review of 2619 patients. Orphanet J. Rare Dis. 2012, 7, 57. [Google Scholar] [CrossRef] [Green Version]
- Oruc, S.; Kaplan, A.D.; Galen, M.; Kaplan, H.J. Uveitis referral pattern in a Midwest university eye center. Ocul. Immunol. Inflamm. 2003, 11, 287–298. [Google Scholar] [CrossRef]
- Suzuki, T.; Kaburaki, T.; Tanaka, R.; Shirahama, S.; Komae, K.; Nakahara, H.; Takamoto, M.; Kawashima, H.; Aihara, M. Incidence and Changing Patterns of Uveitis in Central Tokyo. Int. Ophthalmol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, P.-J.; Jamilloux, Y.; Ecochard, R.; Richard-Colmant, G.; Gerfaud-Valentin, M.; Guillaud, M.; Denis, P.; Kodjikian, L.; Sève, P. Uveitis: Autoimmunity… and beyond. Autoimmun. Rev. 2019, 18, 102351. [Google Scholar] [CrossRef]
- Jabs, D.A.; McCluskey, P.; Oden, N.; Palestine, A.G.; Peterson, J.S.; Saleem, S.M.; Thorne, J.E.; Trusko, B.E. Development of classification criteria for the uveitides. Am. J. Ophthalmol. 2021, 228, 96–105. [Google Scholar] [CrossRef]
- Haroon, M.; O’Rourke, M.; Ramasamy, P.; Murphy, C.C.; FitzGerald, O. A novel evidence-based detection of undiagnosed spondyloarthritis in patients presenting with acute anterior uveitis: The DUET (Dublin Uveitis Evaluation Tool). Ann. Rheum. Dis. 2015, 74, 1990–1995. [Google Scholar] [CrossRef]
- O’Rourke, M.; Haroon, M.; Alfarasy, S.; Ramasamy, P.; FitzGerald, O.; Murphy, C.C. The effect of anterior uveitis and previously undiagnosed spondyloarthritis: Results from the DUET cohort. J. Rheumatol. 2017, 44, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Rathinam, S.R.; Babu, M. Algorithmic approach in the diagnosis of uveitis. Indian J. Ophthalmol. 2013, 61, 255–262. [Google Scholar] [CrossRef]
- Herbort, C.P.; Rao, N.A.; Mochizuki, M.; members of Scientific Committee of First International Workshop on Ocular Sarcoidosis International Criteria for the Diagnosis of Ocular Sarcoidosis. Results of the first International Workshop on Ocular Sarcoidosis (IWOS). Ocul. Immunol. Inflamm. 2009, 17, 160–169. [Google Scholar] [CrossRef]
- Tugal-Tutkun, I.; Onal, S.; Stanford, M.; Akman, M.; Twisk, J.W.R.; Boers, M.; Oray, M.; Özdal, P.Ç.; Kadayifcilar, S.; Amer, R.; et al. An algorithm for the diagnosis of Behçet disease uveitis in adults. Ocul. Immunol. Inflamm. 2020. [Google Scholar] [CrossRef]
- De Parisot, A.; Kodjikian, L.; Errera, M.-H.; Sedira, N.; Heron, E.; Pérard, L.; Cornut, P.-L.; Schneider, C.; Rivière, S.; Ollé, P.; et al. Randomized controlled trial evaluating a standardized strategy for uveitis etiologic diagnosis (ULISSE). Am. J. Ophthalmol. 2017, 178, 176–185. [Google Scholar] [CrossRef]
- Fanlo, P.; Espinosa, G.; Adan, A.; Fonollosa, A.; Segura, A.; Grupo de Trabajo de Enfermedades Autoinmunes Sistémicas de la Sociedad Española de Medicina Interna (GEAS-SEMI) y Sociedad Española de Inflamación Ocular (SEIOC); Members of the Systemic Autoimmune Diseases Workgroup of the Spanish Society of Internal Medicine (GEAS-SEMI) and the Spanish Society of Inflammation Ocular (SEIOC). Multidisciplinary Care and Units for Uveitis in the Internal Medicine Departments in Spain: Survey of the systemic autoimmune diseases group. Rev. Clin. Esp. 2021, 221, 221–225. [Google Scholar] [CrossRef]
- Niessen, A.G.; Bollemeijer, J.G.; de Keizer, R.J.; de Meijer, P.H. Diagnosis of systemic causes of uveitis; a matter of ophthalmologist and internist. Ned. Tijdschr. Geneeskd. 1994, 138, 770–775. [Google Scholar]
- De Parisot, A.; Jamilloux, Y.; Kodjikian, L.; Errera, M.-H.; Sedira, N.; Heron, E.; Pérard, L.; Cornut, P.-L.; Schneider, C.; Rivière, S.; et al. Evaluating the cost-consequence of a standardized strategy for the etiological diagnosis of uveitis (ULISSE Study). PLoS ONE 2020, 15, e0228918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seixas, F.L.; Zadrozny, B.; Laks, J.; Conci, A.; Muchaluat Saade, D.C. A Bayesian network decision model for supporting the diagnosis of dementia, Alzheimer’s disease and mild cognitive impairment. Comput. Biol. Med. 2014, 51, 140–158. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, P.W.; Anderson, N.; Bartels, P.H.; Thompson, D. Expert system support using Bayesian belief networks in the diagnosis of fine needle aspiration biopsy specimens of the breast. J. Clin. Pathol. 1994, 47, 329–336. [Google Scholar] [CrossRef] [Green Version]
- González-López, J.J.; García-Aparicio, Á.M.; Sánchez-Ponce, D.; Muñoz-Sanz, N.; Fernandez-Ledo, N.; Beneyto, P.; Westcott, M.C. Development and validation of a Bayesian network for the differential diagnosis of anterior uveitis. Eye 2016, 30, 865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabs, D.A.; Nussenblatt, R.B.; Rosenbaum, J.T. Standardization of Uveitis Nomenclature (SUN) working group standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [CrossRef]
- Gupta, A.; Sharma, A.; Bansal, R.; Sharma, K. Classification of intraocular tuberculosis. Ocul. Immunol. Inflamm. 2015, 23, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; van der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The assessment of spondyloarthritis international society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general. Ann. Rheum. Dis. 2011, 70, 25–31. [Google Scholar] [CrossRef]
- Weichsler, B.; Davatchi, F.; Lehner, T.; O’duffy, J.D.; Rigby, A.S. Criteria for diagnosis of Behçet’s disease. International study group for Behçet’s disease. Lancet Lond. Engl. 1990, 335, 1078–1080. [Google Scholar]
- Read, R.W.; Holland, G.N.; Rao, N.A.; Tabbara, K.F.; Ohno, S.; Arellanes-Garcia, L.; Pivetti-Pezzi, P.; Tessler, H.H.; Usui, M. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: Report of an international committee on nomenclature. Am. J. Ophthalmol. 2001, 131, 647–652. [Google Scholar] [CrossRef]
- Levinson, R.D.; Brezin, A.; Rothova, A.; Accorinti, M.; Holland, G.N. Research criteria for the diagnosis of Birdshot Chorioretinopathy: Results of an international consensus conference. Am. J. Ophthalmol. 2006, 141, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Costabel, U.; Hunninghake, G.W. ATS/ERS/WASOG statement on sarcoidosis. Sarcoidosis statement committee. American thoracic society. European respiratory society. World association for sarcoidosis and other granulomatous disorders. Eur. Respir. J. 1999, 14, 735–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abad, S.; Meyssonier, V.; Allali, J.; Gouya, H.; Giraudet, A.L.; Monnet, D.; Parc, C.; Tenenbaum, F.; Alberini, J.L.; Grabar, S.; et al. Association of peripheral multifocal choroiditis with sarcoidosis: A study of thirty-seven patients. Arthritis Rheum. 2004, 51, 974–982. [Google Scholar] [CrossRef]
- Ben-Gal, I. Bayesian networks. In Encyclopedia of Statistics in Quality and Reliability; American Cancer Society: Atlanta, GA, USA, 2008; ISBN 978-0-470-06157-2. [Google Scholar]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004; ISBN 978-0-471-65574-9. [Google Scholar]
- Scutari, M. Learning Bayesian networks with the Bnlearn R package. arXiv 2010, arXiv:0908.3817. [Google Scholar]
- Højsgaard, S. Bayesian networks in R with the GRain package. J. Stat. Softw. 2012, 46, 1–26. [Google Scholar]
- Gegundez-Fernandez, J.A.; Fernandez-Vigo, J.I.; Diaz-Valle, D.; Mendez-Fernandez, R.; Cuiña-Sardiña, R.; Santos-Bueso, E.; Benitez-Del-Castillo, J.M. Uvemaster: A mobile app-based decision support system for the differential diagnosis of uveitis. Invest. Ophthalmol. Vis. Sci. 2017, 58, 3931–3939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Pérez, B.; de la Torre-Díez, I.; López-Coronado, M.; Sainz-de-Abajo, B.; Robles, M.; García-Gómez, J.M. Mobile clinical decision support systems and applications: A literature and commercial review. J. Med. Syst. 2014, 38, 4. [Google Scholar] [CrossRef] [PubMed]
- De la Torre-Díez, I.; Martínez-Pérez, B.; López-Coronado, M.; Díaz, J.R.; López, M.M. Decision support systems and applications in ophthalmology: Literature and commercial review focused on mobile apps. J. Med. Syst. 2015, 39, 174. [Google Scholar] [CrossRef]
- Richard Colmant, G.; Kodjikian, L.; De Parisot De Bernecourt, A.; Guillaud, M.; Gerfaud-Valentin, M.; Denis, P.; Broussolle, C.; Jamilloux, Y.; Sève, P. Uveitis of unknown etiology: Clinical and outcome features. A retrospective analysis of 355 patients. Ocul. Immunol. Inflamm. 2019, 27, 1251–1258. [Google Scholar] [CrossRef]
- Choi, R.Y.; Rivera-Grana, E.; Rosenbaum, J.T. Reclassifying idiopathic uveitis: Lessons from a tertiary uveitis center. Am. J. Ophthalmol. 2019, 198, 193–199. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Training Dataset 877 (100%) | Test Dataset 154 (100%) | ||
|---|---|---|---|
| Age at diagnosis (years) | <40 | 315 (35.9%) | 74 (48.1%) |
| 40–50 | 146 (16.6%) | 24 (15.6%) | |
| 50–60 | 134 (15.3%) | 19 (12.3%) | |
| >60 | 282 (32.2%) | 37 (24.0%) | |
| Sex | Female | 534 (60.9%) | 78 (50.6%) |
| Male | 343 (39.1%) | 76 (49.4%) | |
| Ethnic group | Caucasian | 676 (77.1%) | 127 (82.5%) |
| Sub-Saharan African | 12 (1.4%) | 5 (3.2%) | |
| North African | 157 (17.9%) | 22 (14.3%) | |
| South American | 11 (1.3%) | 0 | |
| Other | 7 (0.8%) | 0 | |
| Asian | 14 (1.6%) | 0 | |
| Anatomic type | Anterior uveitis | 311 (35.5%) | 103 (66.9%) |
| Combined uveitis | 104 (11.9%) | 6 (3.9%) | |
| Panuveitis | 267 (30.4%) | 19 (12.3%) | |
| Posterior uveitis | 111 (12.7%) | 14 (9.1%) | |
| Intermediate uveitis | 84 (9.6%) | 12 (7.8%) | |
| Chronicity | Acute | 292 (33.3%) | 144 (93.5%) |
| Chronic | 585 (66.7%) | 10 (6.5%) | |
| Laterality | Bilateral | 515 (58.7%) | 40 (26.0%) |
| Unilateral | 362 (41.3%) | 114 (74.0%) | |
| Not available | 3 (0.3%) | 0 | |
| Granulomatous character | No | 614 (70.0%) | 120 (77.9%) |
| Yes | 263 (30.0%) | 34 (22.1%) | |
| Not available | 8 (0.9%) | 0 | |
| Vasculitis | No | 793 (88.4%) | 132 (85.2%) |
| Yes | 104 (11.6%) | 23 (14.8%) | |
| Ocular hypertension | No | 804 (91.7%) | 137 (89.0%) |
| Yes | 73 (8.3%) | 17 (11.0%) | |
| Not available | 9 (1.0%) | 0 | |
| Etiology | Idiopathic uveitis | 431 (49.1%) | 103 (66.9%) |
| Sarcoidosis | 191 (21.8%) | 8 (5.2%) | |
| Spondyloarthritis & HLA-B27-related | 119 (13.6%) | 30 (19.5%) | |
| Tuberculosis | 59 (6.7%) | 1 (0.6%) | |
| Behcet’s disease | 30 (3.4%) | 3 (1.9%) | |
| Multiple sclerosis | 22 (2.5%) | 2 (1.3%) | |
| Lymphoma | 15 (1.7%) | 2 (1.3%) | |
| Other inflammatory diseases | 10 (1.1%) | 5 (3.2%) |
| Etiology | Most Probable Diagnosis | Two Most Probable Diagnoses | ||
|---|---|---|---|---|
| Sensitivity (95% CI) | Specificity (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | |
| Idiopathic | 0.70 (0.63; 0.76) | 0.55 (0.45; 0.65) | 0.96 (0.95; 0.96) | 0.03 (0.03; 0.03) |
| Sarcoidosis | 0.33 (0.26; 0.41) | 0.90 (0.89; 0.91) | 0.69 (0.62; 0.76) | 0.52 (0.42; 0.62) |
| Spondyloarthritis & HLA-B27-related | 0.76 (0.71; 0.81) | 0.93 (0.93; 0.94) | 0.92 (0.91; 0.93) | 0.85 (0.83; 0.87) |
| Tuberculosis | 0 (0; 0) | 0.97 (0.97; 0.97) | 0.23 (0.19; 0.28) | 0.92 (0.92; 0.93) |
| Behcet’s disease | 0.67 (0.59; 0.74) | 0.95 (0.95; 0.95) | 0.67 (0.59; 0.74) | 0.94 (0.93; 0.94) |
| Multiple sclerosis | 0.20 (0.17; 0.24) | 0.99 (0.99; 0.99) | 0.40 (0.31; 0.49) | 0.97 (0.97; 0.97) |
| Lymphoma | 0 (0; 0) | 1 (1; 1) | 0.67 (0.59; 0.74) | 0.97 (0.97; 0.97) |
| Other inflammatory etiologies | 0 (0; 0) | 0.99 (0.99; 0.99) | 0 (0; 0) | 0.99 (0.99; 0.99) |
| Etiology | Most Probable Diagnosis | Two Most Probable Diagnoses | ||
|---|---|---|---|---|
| Sensitivity (95% CI) | Specificity (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | |
| Idiopathic | 0.52 (0.42; 0.62) | 0.65 (0.57; 0.73) | 0.99 (0.99; 0.99) | 0.04 (0.04; 0.04) |
| Sarcoidosis | 0.38 (0.29; 0.46) | 0.98 (0.98; 0.98) | 0.50 (0.4; 0.6) | 0.72 (0.66; 0.78) |
| Spondyloarthritis & HLA-B27-related | 0.63 (0.55; 0.72) | 0.54 (0.44; 0.64) | 0.83 (0.81; 0.86) | 0.33 (0.25; 0.40) |
| Tuberculosis | 0 (0; 0) | 1 (1; 1) | 0 (0; 0) | 0.97 (0.97; 0.98) |
| Behcet’s disease | 0 (0; 0) | 1 (1; 1) | 0 (0; 0) | 1 (1; 1) |
| Multiple sclerosis | 0 (0; 0) | 1 (1; 1) | 0 (0; 0) | 1 (1; 1) |
| Lymphoma | 0 (0; 0) | 1 (1; 1) | 0 (0; 0) | 1 (1; 1) |
| Other inflammatory etiologies | 0 (0; 0) | 1 (1; 1) | 0 (0; 0) | 1 (1; 1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamilloux, Y.; Romain-Scelle, N.; Rabilloud, M.; Morel, C.; Kodjikian, L.; Maucort-Boulch, D.; Bielefeld, P.; Sève, P. Development and Validation of a Bayesian Network for Supporting the Etiological Diagnosis of Uveitis. J. Clin. Med. 2021, 10, 3398. https://doi.org/10.3390/jcm10153398
Jamilloux Y, Romain-Scelle N, Rabilloud M, Morel C, Kodjikian L, Maucort-Boulch D, Bielefeld P, Sève P. Development and Validation of a Bayesian Network for Supporting the Etiological Diagnosis of Uveitis. Journal of Clinical Medicine. 2021; 10(15):3398. https://doi.org/10.3390/jcm10153398
Chicago/Turabian StyleJamilloux, Yvan, Nicolas Romain-Scelle, Muriel Rabilloud, Coralie Morel, Laurent Kodjikian, Delphine Maucort-Boulch, Philip Bielefeld, and Pascal Sève. 2021. "Development and Validation of a Bayesian Network for Supporting the Etiological Diagnosis of Uveitis" Journal of Clinical Medicine 10, no. 15: 3398. https://doi.org/10.3390/jcm10153398