
Analysis on Microbial Profiles & Components of Bile in Patients with Recurrent CBD Stones after Endoscopic CBD Stone Removal: A Preliminary Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Bile Sample Collection
2.2. Next-Generation Sequencing of Bacterial 16s rRNA Fragments in Bile Samples
2.3. Composition of Bile
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Richness of Microbiota in Bile
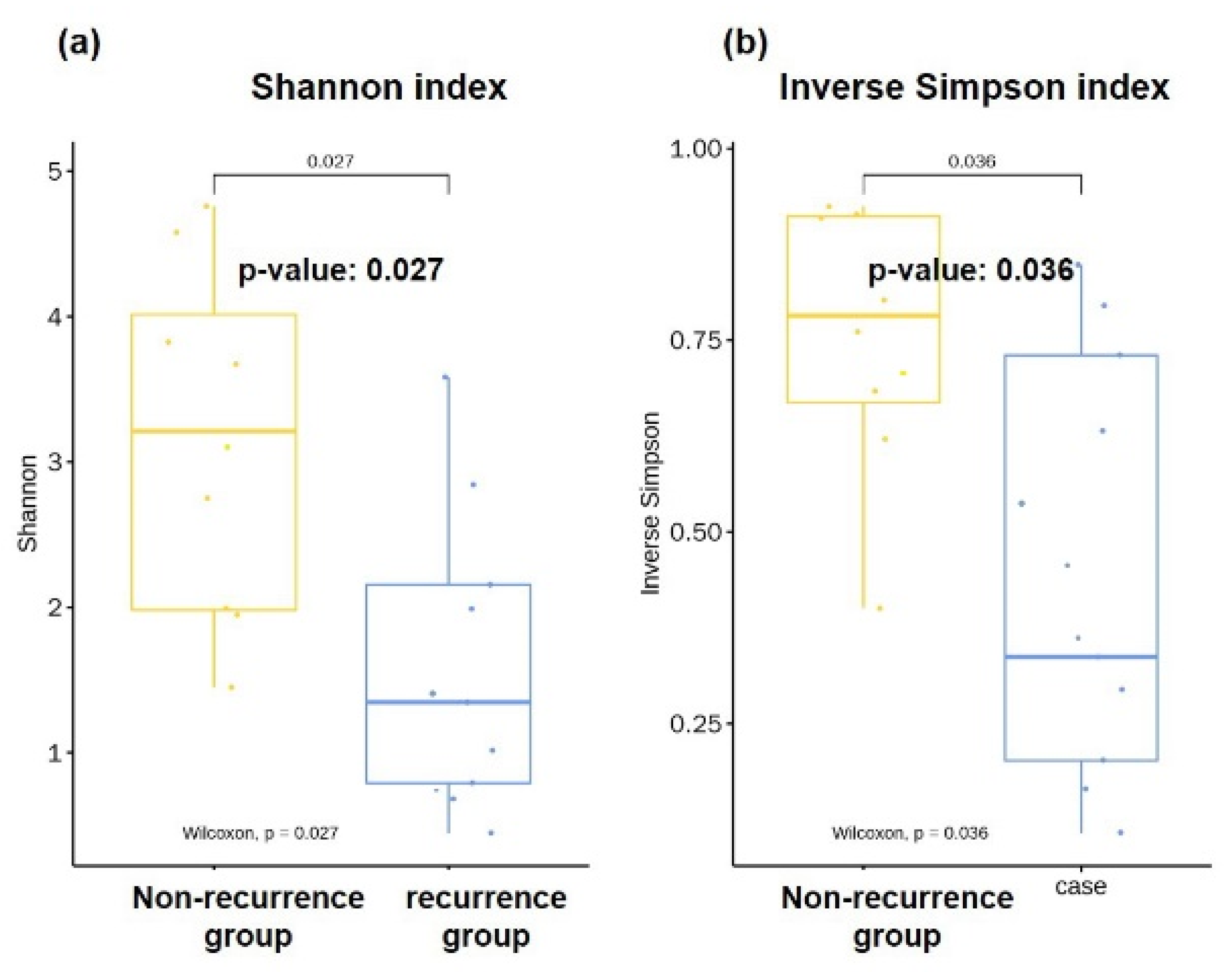
3.3. Diversities of Microbiota in Bile
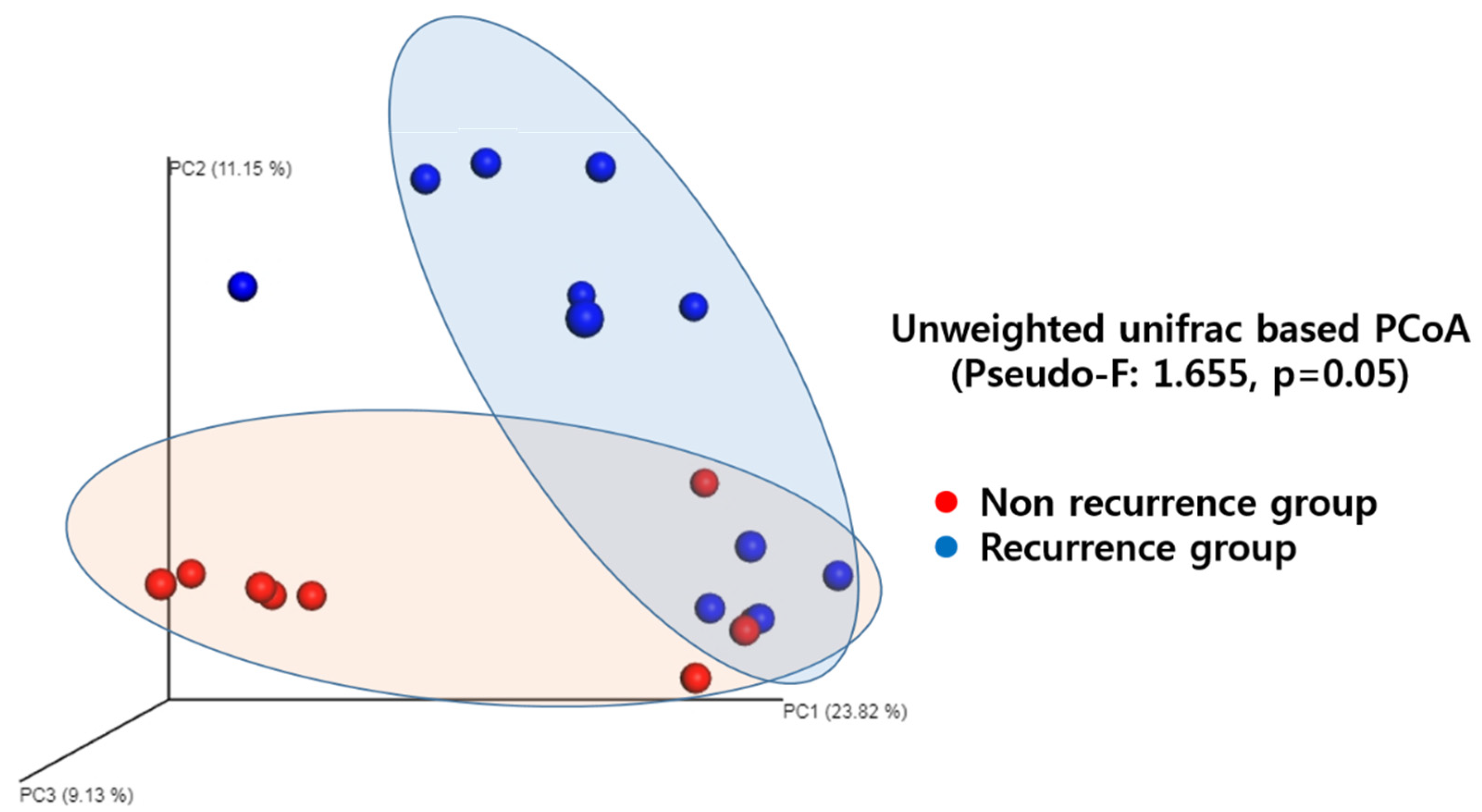
3.4. Microbial Community Similarity
3.5. Microbiome
3.6. Bile Composition
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lai, K.H.; Peng, N.J.; Lo, G.H.; Cheng, J.S.; Huang, R.L.; Lin, C.K.; Huang, J.S.; Chiang, H.T.; Ger, L.P. Prediction of recurrent choledocholithiasis by quantitative cholescintigraphy in patients after endoscopic sphincterotomy. Gut 1997, 41, 399–403. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, S.; Tanaka, M.; Matsumoto, S.; Yoshimoto, H.; Itoh, H. Endoscopic sphincterotomy: Long-term results in 408 patients with complete follow-up. Endoscopy 1988, 20, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Cheon, Y.K.; Lehman, G.A. Identification of risk factors for stone recurrence after endoscopic treatment of bile duct stones. Eur. J. Gastroenterol. Hepatol. 2006, 18, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Swidsinski, A.; Lee, S.P. The role of bacteria in gallstone pathogenesis. Front. Biosci. 2001, 6, E93–E103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, L.; Grifiss, J.M.; Jarvis, G.A.; Way, L.W. Biliary bacterial factors determine the path of gallstone formation. Am. J. Surg. 2006, 192, 598–603. [Google Scholar] [CrossRef]
- Maki, T. Pathogenesis of calcium bilirubinate gallstone: Role of E. coli, beta-glucuronidase and coagulation by inorganic ions, polyelectrolytes and agitation. Ann. Surg. 1966, 164, 90–100. [Google Scholar] [CrossRef]
- Kaufman, H.S.; Magnuson, T.H.; Lillemoe, K.D.; Frasca, P.; Pitt, H.A. The role of bacteria in gallbladder and common duct stone formation. Ann. Surg. 1989, 209, 584–591. [Google Scholar] [CrossRef]
- Theron, J.; Cloete, T.E. Molecular techniques for determining microbial diversity and community structure in natural environments. Crit. Rev. Microbiol. 2000, 26, 37–57. [Google Scholar] [CrossRef]
- Amann, R.I.; Ludwig, W.; Schleifer, K.H. Phylogenetic Identification and in-Situ Detection of Individual Microbial-Cells without Cultivation. Microbiol. Rev. 1995, 59, 143–169. [Google Scholar] [CrossRef]
- Wu, T.; Zhang, Z.; Liu, B.; Hou, D.; Liang, Y.; Zhang, J.; Shi, P. Gut microbiota dysbiosis and bacterial community assembly associated with cholesterol gallstones in large-scale study. BMC Genom. 2013, 14, 669. [Google Scholar] [CrossRef] [Green Version]
- Lagier, J.C.; Armougom, F.; Million, M.; Hugon, P.; Pagnier, I.; Robert, C.; Bittar, F.; Fournous, G.; Gimenez, G.; Maraninchi, M.J.C.M.; et al. Microbial culturomics: Paradigm shift in the human gut microbiome study. Clin. Microbiol. Infect. 2012, 18, 1185–1193. [Google Scholar] [CrossRef] [Green Version]
- Keizman, D.; Shalom, M.I.; Konikoff, F.M. An angulated common bile duct predisposes to recurrent symptomatic bile duct stones after endoscopic stone extraction. Surg. Endosc. 2006, 20, 1594–1599. [Google Scholar] [CrossRef]
- Trotman, B.W.; Soloway, R.D. Pigment gallstone disease: Summary of the National Institutes of Health--international workshop. Hepatology 1982, 2, 879–884. [Google Scholar] [CrossRef]
- Rooks, M.G.; Garrett, W.S. Gut microbiota, metabolites and host immunity. Nat. Rev. Immunol. 2016, 16, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, J.R.; Adams, D.H.; Fava, F.; Hermes, G.D.; Hirschfield, G.M.; Hold, G.; Quraishi, M.N.; Kinross, J.; Smidt, H.; Tuohy, K.M.; et al. The gut microbiota and host health: A new clinical frontier. Gut 2016, 65, 330–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carding, S.; Verbeke, K.; Vipond, D.T.; Corfe, B.M.; Owen, L.J. Dysbiosis of the gut microbiota in disease. Microb. Ecol. Health Dis. 2015, 26, 26191. [Google Scholar] [CrossRef] [PubMed]
- Lupp, C.; Robertson, M.L.; Wickham, M.E.; Sekirov, I.; Champion, O.L.; Gaynor, E.C.; Finlay, B.B. Host-mediated inflammation disrupts the intestinal microbiota and promotes the overgrowth of Enterobacteriaceae. Cell Host Microbe 2007, 2, 204. [Google Scholar] [CrossRef] [Green Version]
- Lion, C.; Escande, F.; Burdin, J.C. Capnocytophaga canimorsus infections in human: Review of the literature and cases report. Eur. J. Epidemiol. 1996, 12, 521–533. [Google Scholar] [CrossRef]
- Hofmann, A.F. The continuing importance of bile acids in liver and intestinal disease. Arch. Intern. Med. 1999, 159, 2647–2658. [Google Scholar] [CrossRef]
- Akiyoshi, T.; Nakayama, F. Bile acid composition in brown pigment stones. Dig Dis Sci. 1990, 35, 27–32. [Google Scholar] [CrossRef]
- Onochi, S.; Masu, A.; Takahashi, W.; Suzuki, N. Study on bile acid and lipid of gallbladder bile and gallstone in cases with calcium bilirubinate stones. Nihon Shokakibyo Gakkai Zasshi Jpn. J. Gastro-Enterol. 1984, 81, 2552–2560. [Google Scholar]
- Lorenzo-Zuniga, V.; Bartoli, R.; Planas, R.; Hofmann, A.F.; Vinado, B.; Hagey, L.R.; Hernandez, J.M.; Mane, J.; Alvarez, M.A.; Ausina, V.; et al. Oral bile acids reduce bacterial overgrowth, bacterial translocation, and endotoxemia in cirrhotic rats. Hepatology 2003, 37, 551–557. [Google Scholar] [CrossRef]
- Wahlstrom, A.; Sayin, S.I.; Marschall, H.U.; Backhed, F. Intestinal Crosstalk between Bile Acids and Microbiota and Its Impact on Host Metabolism. Cell Metab. 2016, 24, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridlon, J.M.; Kang, D.J.; Hylemon, P.B.; Bajaj, J.S. Bile acids and the gut microbiome. Curr. Opin. Gastroenterol. 2014, 30, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogerwerf, W.A.; Soloway, R.D. Gallstones. Curr. Opin. Gastroenterol. 1999, 15, 442–447. [Google Scholar] [CrossRef]
- Vitetta, L.; Best, S.P.; Sali, A. Single and multiple cholesterol gallstones and the influence of bacteria. Med. Hypotheses 2000, 55, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Pérez, O.; Cruz-Ramón, V.; Chinchilla-López, P.; Méndez-Sánchez, N. The Role of the Gut Microbiota in Bile Acid Metabolism. Ann. Hepatol. 2017, 16, s15–s20. [Google Scholar] [CrossRef]
- Sayin, S.I.; Wahlstrom, A.; Felin, J.; Jantti, S.; Marschall, H.U.; Bamberg, K.; Angelin, B.; Hyotylainen, T.; Oresic, M.; Backhed, F. Gut microbiota regulates bile acid metabolism by reducing the levels of tauro-beta-muricholic acid, a naturally occurring FXR antagonist. Cell Metab. 2013, 17, 225–235. [Google Scholar] [CrossRef] [Green Version]
- Islam, K.S.; Fukiya, S.; Hagio, M.; Fujii, N.; Ishizuka, S.; Ooka, T.; Ogura, Y.; Hayashi, T.; Yokota, A.J.G. Bile acid is a host factor that regulates the composition of the cecal microbiota in rats. Gastroenterology 2011, 141, 1773–1781. [Google Scholar] [CrossRef]
- Jia, X.; Lu, S.; Zeng, Z.; Liu, Q.; Dong, Z.; Chen, Y.; Zhu, Z.; Hong, Z.; Zhang, T.; Du, G.; et al. Characterization of Gut Microbiota, Bile Acid Metabolism, and Cytokines in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 71, 893–906. [Google Scholar] [CrossRef]
- Hancke, E.; Nusche, A.; Marklein, G. Bacteria in the gallbladder wall and gallstones--indications for cholecystectomy. Langenbecks Arch. Chir. 1986, 368, 249–254. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Recurrence Group (N = 11) | Non-Recurrence Group (N = 9) | p-Value | |
|---|---|---|---|
| Age, median years (min-max) | 62 (32–78) | 63 (29–83) | 0.12 |
| Gender, male (%) | 6 (66.6) | 5 (62.5) | 0.45 |
| BMI, median kg/m2(min-max) | 22.6 (17.6–29.0) | 22.5 (16.2–29.4) | 0.45 |
| CBD diameter (mm, mean ± SD) | 17.7 ± 2.5 | 17.8 ± 2.2 | 0.89 |
| Angulation of bile duct (≤145°) (N, %) | 1 (11.1) | 0 | 0.85 |
| PAD (N, %) | 0.20 | ||
| I | 2 | 1 | |
| II | 5 | 4 | |
| III | 2 | 3 |
| Phylum | Recurrence Group | Non-Recurrence Group | p-Value | ||
|---|---|---|---|---|---|
| Mean Proportion | SEM | Mean Proportion | SEM | ||
| Euryarchaeota | <0.001 | <0.001 | 0.001 | 0.001 | 0.345 |
| Actinobacteria | 0.024 | 0.005 | 0.009 | 0.003 | 0.048 |
| Bacteroidetes | 0.074 | 0.045 | 0.188 | 0.066 | 0.042 |
| Chloroflexi | <0.001 | <0.001 | 0.002 | 0.003 | 0.345 |
| Cyanobacteria | 0.001 | 0.002 | <0.001 | <0.001 | 0.084 |
| Deinococcus | <0.001 | <0.001 | 0.001 | 0.001 | 0.346 |
| Firmicutes | 0.384 | 0.105 | 0.178 | 0.027 | 0.038 |
| Fusobacteria | 0.009 | 0.006 | 0.021 | 0.017 | 0.311 |
| Gemmatimonadetes | <0.001 | <0.001 | 0.001 | 0.001 | 0.345 |
| Proteobacteria | 0.504 | 0.121 | 0.568 | 0.094 | 0.814 |
| Spirochaetes | <0.001 | <0.001 | 0.001 | 0.001 | 0.345 |
| Synergistetes | <0.001 | <0.001 | 0.008 | 0.008 | 0.409 |
| Tenericutes | <0.001 | <0.001 | <0.001 | <0.001 | 0.999 |
| Unassigned | 0.001 | <0.001 | 0.017 | 0.013 | 0.411 |
| Genus | Recurrence Group | Non-Recurrence Group | p-Value | ||
|---|---|---|---|---|---|
| Mean Proportion | SEM | Mean Proportion | SEM | ||
| Neisseria | 0.001 | 0.001 | 0.162 | 0.021 | 0.008 |
| Capnocytophaga | 0.001 | 0.001 | 0.137 | 0.004 | 0.025 |
| Gemella | <0.001 | <0.001 | 0.075 | 0.003 | 0.041 |
| Rothia | <0.001 | <0.001 | 0.003 | 0.001 | 0.052 |
| Haemophilus | 0.041 | 0.011 | 0.046 | 0.033 | 0.075 |
| Streptococcus | 0.132 | 0.102 | 0.029 | 0.009 | 0.091 |
| Klebsiella | 0.134 | 0.049 | 0.049 | 0.026 | 0.162 |
| Enterococcus | 0.033 | 0.006 | 0.006 | 0.003 | 0.191 |
| Clostridium | 0.044 | 0.029 | 0.059 | 0.029 | 0.201 |
| Pseudomonas | 0.081 | 0.023 | 0.073 | 0.048 | 0.746 |
| Staphylococcus | 0.003 | 0.002 | 0.002 | 0.001 | 0.807 |
| Acinetobacter | 0.002 | 0.001 | 0.001 | 0.001 | 0.957 |
| Lactobacillus | 0.034 | 0.034 | 0.001 | 0.001 | 0.999 |
| Citrobacter | 0.163 | 0.126 | 0.014 | 0.009 | 0.999 |
| Escherichia | 0.320 | 0.123 | 0.282 | 0.107 | 0.999 |
| Aeromonas | 0.001 | 0.001 | 0.007 | 0.006 | 0.473 |
| Fusobacterium | 0.009 | 0.007 | 0.028 | 0.018 | 0.245 |
| Unassigned | 0.001 | <0.001 | 0.017 | 0.013 | 0.411 |
| Recurrence Group (N = 11) | Non-Recurrence Group (N = 9) | p-Value | |
|---|---|---|---|
| pH | 7.8 ± 0.2 | 7.95 ± 0.4 | 0.85 |
| Total nucleated cell count | 12 ± 5 | 22 ± 10.4 | 0.07 |
| Total bilirubin (mg/dL) | 37.5 ± 63.5 | 27.7 ± 80.7 | 0.85 |
| Cholesterol (mg/dL) | 28.1 ± 50.7 | 34.2 ± 62.1 | 0.32 |
| Bile acid (mmol/L) | 147.1 ± 64.2 | 254.5 ± 82.0 | <0.01 |
| Phospholipid (mg/dL) | 324 ± 272 | 454 ± 350 | 0.25 |
| Ca2+ (mg/dL) | 7.7 ± 4.4 | 5.5 ± 2.2 | 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choe, J.W.; Lee, J.M.; Hyun, J.J.; Lee, H.S. Analysis on Microbial Profiles & Components of Bile in Patients with Recurrent CBD Stones after Endoscopic CBD Stone Removal: A Preliminary Study. J. Clin. Med. 2021, 10, 3303. https://doi.org/10.3390/jcm10153303
Choe JW, Lee JM, Hyun JJ, Lee HS. Analysis on Microbial Profiles & Components of Bile in Patients with Recurrent CBD Stones after Endoscopic CBD Stone Removal: A Preliminary Study. Journal of Clinical Medicine. 2021; 10(15):3303. https://doi.org/10.3390/jcm10153303
Chicago/Turabian StyleChoe, Jung Wan, Jae Min Lee, Jong Jin Hyun, and Hong Sik Lee. 2021. "Analysis on Microbial Profiles & Components of Bile in Patients with Recurrent CBD Stones after Endoscopic CBD Stone Removal: A Preliminary Study" Journal of Clinical Medicine 10, no. 15: 3303. https://doi.org/10.3390/jcm10153303