
Hyperuricemia Is an Early and Relatively Common Feature in Children with HNF1B Nephropathy but Its Utility as a Predictor of the Disease Is Limited

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Assessment and Definitions of Analyzed Parameters
2.3. Molecular Analysis of HNF1B Gene
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Patients
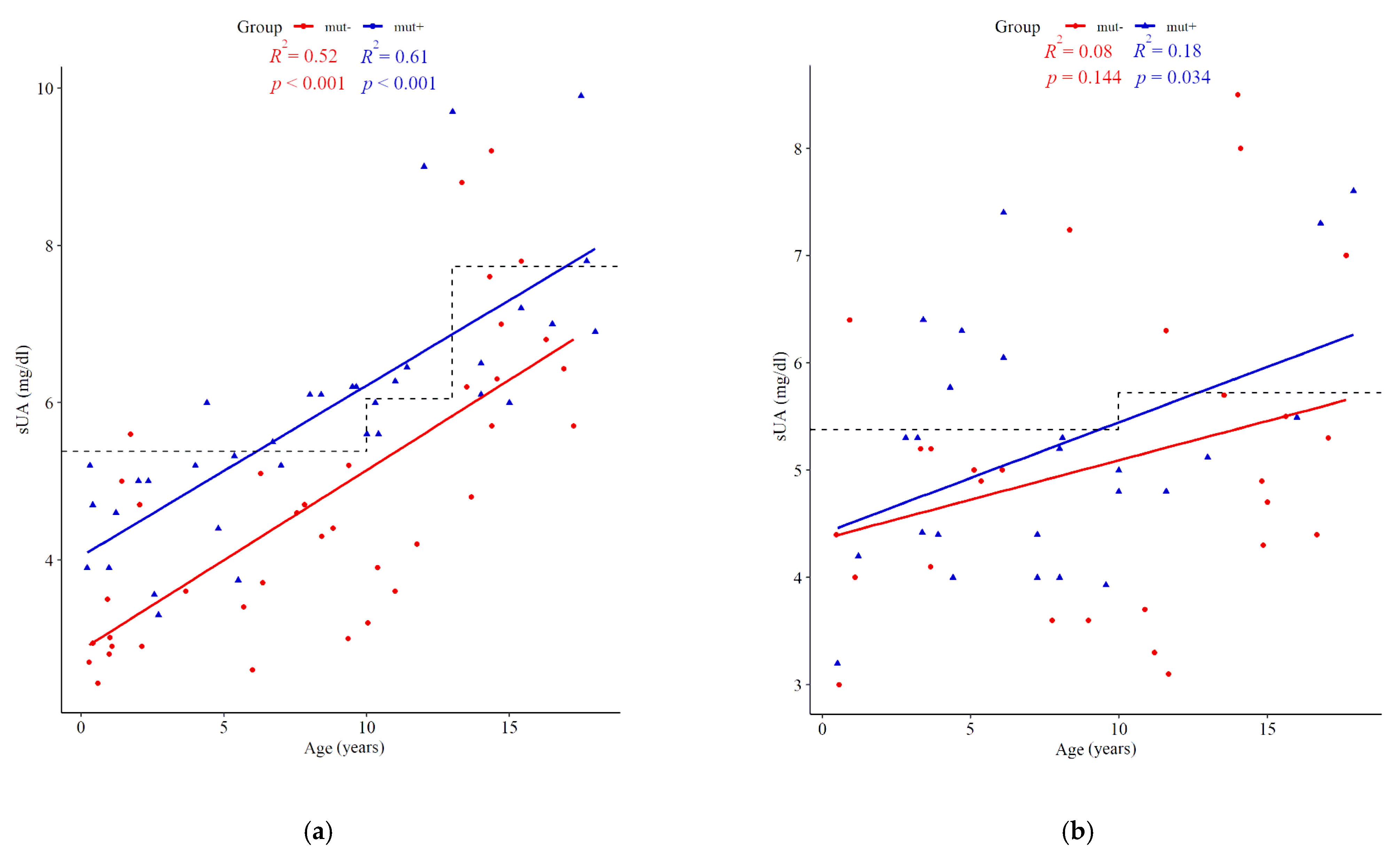
3.2. Serum Uric Acid Concentration
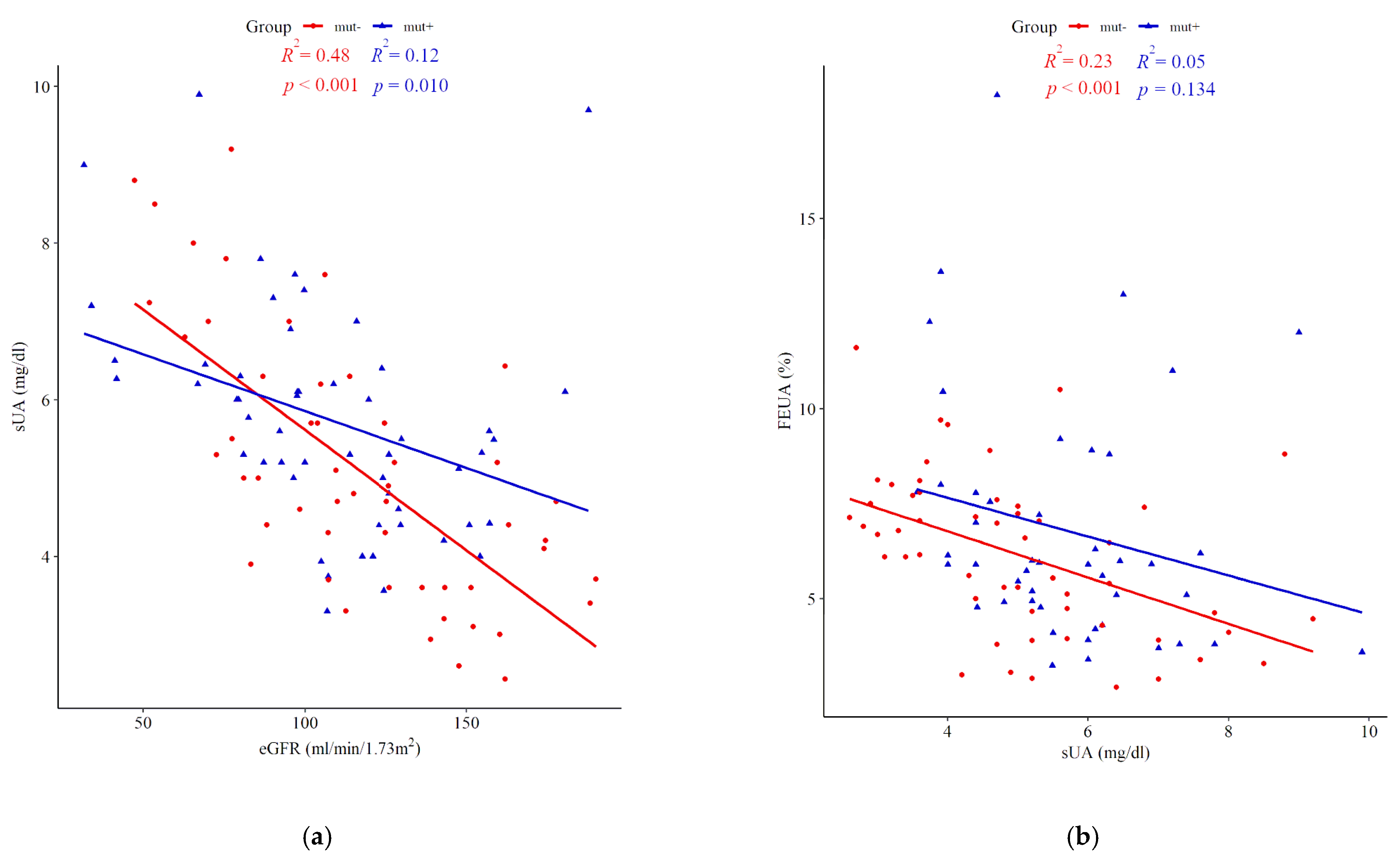
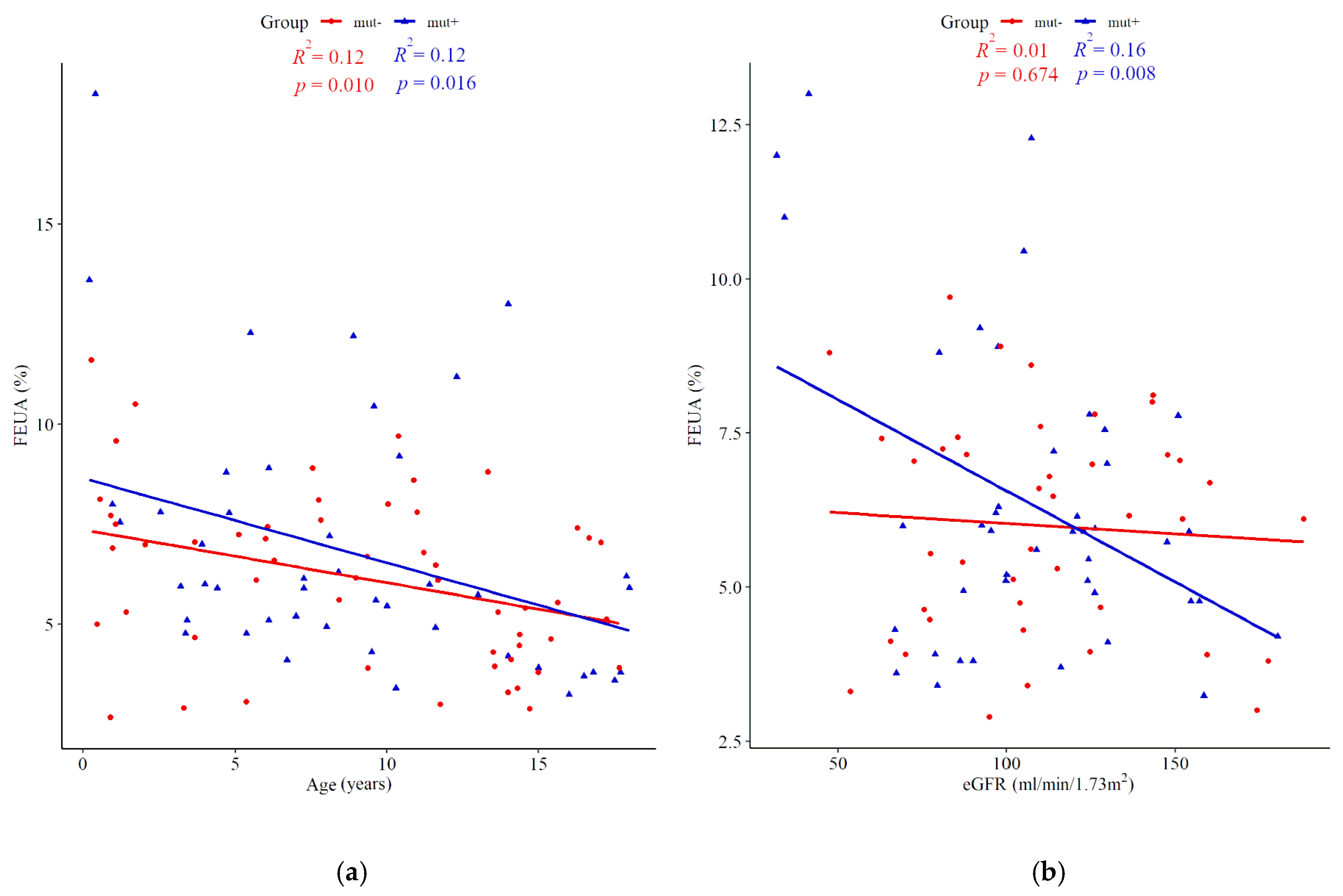
3.3. Fractional Excretion of Uric Acid
3.4. Determinants of Serum Uric Acid
3.5. Hyperuricemia as a Predictor of HNF1B Mutation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adalat, S.; Bockenhauer, D.; Ledermann, S.E.; Hennekam, R.C.; Woolf, A.S. Renal malformations associated with mutations of developmental genes: Messages from the clinic. Pediatr. Nephrol. 2010, 25, 2247–2255. [Google Scholar] [CrossRef]
- Bingham, C.; Hattersley, A.T. Renal cysts and diabetes syndrome resulting from mutations in hepatocyte nuclear factor-1beta. Nephrol. Dial. Transplant. 2004, 19, 2703–2708. [Google Scholar] [CrossRef] [PubMed]
- Ferrè, S.; Igarashi, P. New insights into the role of HNF-1β in kidney (patho)physiology. Pediatr. Nephrol. 2019, 34, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Bockenhauer, D.; Jaureguiberry, G. HNF1B-associated clinical phenotypes: The kidney and beyond. Pediatr. Nephrol. 2016, 31, 707–714. [Google Scholar] [CrossRef]
- Clissold, R.L.; Hamilton, A.J.; Hattersley, A.T.; Ellard, S.; Bingham, C. HNF1B-associated renal and extra-renal disease-an expanding clinical spectrum. Nat. Rev. Nephrol. 2015, 11, 102–112. [Google Scholar] [CrossRef]
- Ulinski, T.; Lescure, S.; Beaufils, S.; Guigonis, V.; Decramer, S.; Morin, D.; Clauin, S.; Deschênes, G.; Bouissou, F.; Bensman, A.; et al. Renal phenotypes related to hepatocyte nuclear factor-1beta (TCF2) mutations in a pediatric cohort. J. Am. Soc. Nephrol. 2006, 17, 497–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decramer, S.; Parant, O.; Beaufils, S.; Clauin, S.; Guillou, C.; Kessler, S.; Aziza, J.; Bandin, F.; Schanstra, J.P.; Bellanné-Chantelot, C. Anomalies of the TCF2 gene are the main cause of fetal bilateral hyperechogenic kidneys. J. Am. Soc. Nephrol. 2007, 18, 923–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adalat, S.; Woolf, A.S.; Johnstone, K.A.; Wirsing, A.; Harries, L.W.; Long, D.A.; Hennekam, R.C.; Ledermann, S.E.; Rees, L.; van’t Hoff, W.; et al. HNF1B mutations associate with hypomagnesemia and renal magnesium wasting. J. Am. Soc. Nephrol. 2009, 20, 1123–1131. [Google Scholar] [CrossRef] [Green Version]
- Heidet, L.; Decramer, S.; Pawtowski, A.; Morinière, V.; Bandin, F.; Knebelmann, B.; Lebre, A.-S.; Faguer, S.; Guigonis, V.; Antignac, C.; et al. Spectrum of HNF1B mutations in a large cohort of patients who harbor renal diseases. Clin. J. Am. Soc. Nephrol. 2010, 5, 1079–1090. [Google Scholar] [CrossRef] [Green Version]
- Raaijmakers, A.; Corveleyn, A.; Devriendt, K.; van Tienoven, T.P.; Allegaert, K.; Van Dyck, M.; van den Heuvel, L.; Kuypers, D.; Claes, K.; Mekahli, D.; et al. Criteria for HNF1B analysis in patients with congenital abnormalities of kidney and urinary tract. Nephrol. Dial. Transplant. 2015, 30, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Madariaga, L.; García-Castaño, A.; Ariceta, G.; Martínez-Salazar, R.; Aguayo, A.; Castaño, L. Variable phenotype in HNF1B mutations: Extrarenal manifestations distinguish affected individuals from the population with congenital anomalies of the kidney and urinary tract. Clin. Kidney J. 2019, 12, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Okorn, C.; Goertz, A.; Vester, U.; Beck, B.B.; Bergmann, C.; Habbig, S.; König, J.; Konrad, M.; Müller, D.; Oh, J.; et al. HNF1B nephropathy has a slow-progressive phenotype in childhood-with the exception of very early onset cases: Results of the German Multicenter HNF1B Childhood Registry. Pediatr. Nephrol. 2019, 34, 1065–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagano, C.; Morisada, N.; Nozu, K.; Kamei, K.; Tanaka, R.; Kanda, S.; Shiona, S.; Araki, Y.; Ohara, S.; Matsumura, C.; et al. Clinical characteristics of HNF1B-related disorders in a Japanese population. Clin. Exp. Nephrol. 2019, 23, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Kim, J.H.; Han, K.H.; Ahn, Y.H.; Kang, H.G.; Ha, I.-S.; Cheong, H. Il Genotype and Phenotype Analyses in Pediatric Patients with HNF1B Mutations. J. Clin. Med. 2020, 9, 2320. [Google Scholar] [CrossRef] [PubMed]
- Bingham, C.; Ellard, S.; van’t Hoff, W.G.; Simmonds, H.A.; Marinaki, A.M.; Badman, M.K.; Winocour, P.H.; Stride, A.; Lockwood, C.R.; Nicholls, A.J.; et al. Atypical familial juvenile hyperuricemic nephropathy associated with a hepatocyte nuclear factor-1beta gene mutation. Kidney Int. 2003, 63, 1645–1651. [Google Scholar] [CrossRef] [Green Version]
- Baldree, L.A.; Stapleton, F.B. Uric acid metabolism in children. Pediatr. Clin. N. Am. 1990, 37, 391–418. [Google Scholar] [CrossRef]
- Ridefelt, P.; Hilsted, L.; Juul, A.; Hellberg, D.; Rustad, P. Pediatric reference intervals for general clinical chemistry components—Merging of studies from Denmark and Sweden. Scand. J. Clin. Lab. Investig. 2018, 78, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Kołbuc, M.; Leßmeier, L.; Salamon-Słowińska, D.; Małecka, I.; Pawlaczyk, K.; Walkowiak, J.; Wysocki, J.; Beck, B.B.; Zaniew, M. Hypomagnesemia is underestimated in children with HNF1B mutations. Pediatr. Nephrol. 2020, 35, 1877–1886. [Google Scholar] [CrossRef]
- Motyka, R.; Kołbuc, M.; Wierzchołowski, W.; Beck, B.B.; Towpik, I.E.; Zaniew, M. Four Cases of Maturity Onset Diabetes of the Young (MODY) Type 5 Associated with Mutations in the Hepatocyte Nuclear Factor 1 Beta (HNF1B) Gene Presenting in a 13-Year-Old Boy and in Adult Men Aged 33, 34, and 35 Years in Poland. Am. J. Case Rep. 2020, 22, e928994. [Google Scholar] [CrossRef]
- Faguer, S.; Chassaing, N.; Bandin, F.; Prouheze, C.; Garnier, A.; Casemayou, A.; Huart, A.; Schanstra, J.P.; Calvas, P.; Decramer, S.; et al. The HNF1B score is a simple tool to select patients for HNF1B gene analysis. Kidney Int. 2014, 86, 1007–1015. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.J.; Brion, L.P.; Spitzer, A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr. Clin. N. Am. 1987, 34, 571–590. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Coresh, J.; Bolton, K.; Culleton, B.; Harvey, K.S.; Ikizler, T.A.; Johnson, C.A.; Kausz, A.; Kimmel, P.L.; Kusek, J.; et al. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Mayer-Davis, E.J.; Kahkoska, A.R.; Jefferies, C.; Dabelea, D.; Balde, N.; Gong, C.X.; Aschner, P.; Craig, M.E. ISPAD Clinical Practice Consensus Guidelines 2018: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr. Diabetes 2018, 19 (Suppl. 27), 7–19. [Google Scholar] [CrossRef] [PubMed]
- Grajda, A.; Kułaga, Z.; Gurzkowska, B.; Wojtyło, M.; Góźdź, M.; Litwin, M. Preschool children blood pressure percentiles by age and height. J. Hum. Hypertens. 2017, 31, 400–408. [Google Scholar] [CrossRef]
- Kułaga, Z.; Litwin, M.; Grajda, A.; Kułaga, K.; Gurzkowska, B.; Góźdź, M.; Pan, H. OLAF Study Group. Oscillometric blood pressure percentiles for Polish normal-weight school-aged children and adolescents. J. Hypertens. 2012, 30, 1942–1954. [Google Scholar] [CrossRef] [PubMed]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114 (Suppl. S2), 555–576. [Google Scholar] [CrossRef]
- Fathallah-Shaykh, S.A.; Cramer, M.T. Uric acid and the kidney. Pediatr. Nephrol. 2014, 29, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Mintz, D.H.; Canary, J.J.; Carreon, G.; Kyle, L.H. Hyperuricemia in hyperparathyroidism. N. Engl. J. Med. 1961, 265, 112–115. [Google Scholar] [CrossRef]
- Christensson, T. Serum urate in subjects with hypercalcaemic hyperparathyroidism. Clin. Chim. Acta 1977, 80, 529–533. [Google Scholar] [CrossRef]
- Hui, J.Y.; Choi, J.W.J.; Mount, D.B.; Zhu, Y.; Zhang, Y.; Choi, H.K. The independent association between parathyroid hormone levels and hyperuricemia: A national population study. Arthritis Res. Ther. 2012, 14, R56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hisatome, I.; Ishimura, M.; Sasaki, N.; Yamakawa, M.; Kosaka, H.; Tanaka, Y.; Kouchi, T.; Mitani, Y.; Yoshida, A.; Kotake, H. Renal handling of urate in two patients with hyperuricemia and primary hyperparathyroidism. Intern. Med. 1992, 31, 807–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, M. Hyperuricemia in Children and Adolescents: Present Knowledge and Future Directions. J. Nutr. Metab. 2019, 2019, 3480718. [Google Scholar] [CrossRef]
- Stiburkova, B.; Bleyer, A.J. Changes in serum urate and urate excretion with age. Adv. Chronic Kidney Dis. 2012, 19, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Ferrè, S.; Bongers, E.M.H.F.; Sonneveld, R.; Cornelissen, E.A.M.; van der Vlag, J.; van Boekel, G.A.J.; Wetzels, J.F.M.; Hoenderop, J.G.J.; Bindels, R.J.M.; Nijenhuis, T. Early development of hyperparathyroidism due to loss of PTH transcriptional repression in patients with HNF1β mutations? J. Clin. Endocrinol. Metab. 2013, 98, 4089–4096. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | mut+ at Diagnosis | mut- | p Value |
|---|---|---|---|
| Age (years) | 7.84 (6.10–9.58) | 8.74 (7.34–10.14) | 0.436 |
| Gender (M/F) | 24/16 (60.5–39.5) | 38/27 (58.5–41.5) | 0.876 |
| Height-SDS | 0.04 (−0.53–0.61) | 0.10 (−0.24–0.45) | 0.857 |
| Short stature | 4 (11.1) | 2 (3.8) | 0.355 a |
| BMI-SDS | 0.49 (−0.03–1.00) | 0.34 (0.03–0.66) | 0.324 |
| Overweight | 13 (36.1) | 13 (24.5) | 0.238 |
| eGFR (mL/min/1.73 m2) | 104.09 (90.40–117.78) | 115 (104.32–126.03) | 0.210 |
| CKD | --- | ||
| 1 | 21 (63.6) | 36 (70.6) | 0.505 |
| 2 | 9 (27.3) | 12 (23.5) | 0.699 |
| 3 | 3 (9.1) | 3 (5.9) | 0.577 |
| 4 | --- | --- | --- |
| 5 | --- | --- | --- |
| sMg (mmol/L) | 0.72 (0.69–0.76) | 0.86 (0.84–0.88) | <0.001 |
| Hypomagnesemia | 26 (65.0) | 3 (4.8) | <0.001 |
| sUA (mg/dL) | 5.74 (5.22–6.27) | 4.87 (4.47–5.28) | 0.006 |
| Hyperuricemia | 17 (42.5) | 10 (15.40) | 0.002 |
| sK (mmol/L) | 4.43 (4.26–4.60) | 4.64 (4.51–4.78) | 0.041 |
| Hypokalemia | 0 (0.0) | 0 (0.0) | --- |
| PTH (pg/mL) | 67.78 (45.50–90.06) | 33.46 (27.09–39.82) | 0.001 |
| Hyperparathyroidism | 10 (38.5) | 1 (3.0) | 0.001 |
| FEMg (%) | 6.89 (5.54–8.24) | 3.97 (3.35–4.60) | <0.001 |
| FEUA (%) | 6.88 (5.27–8.50) | 6.16 (5.59–6.74) | 0.888 |
| FECa (%) | 0.65 (0.29–1.01) | 0.51 (0.35–0.66) | 0.754 |
| FEK (%) | 7.48 (4.61–10.36) | 5.68 (4.72–6.65) | 0.149 |
| Positive family history b | 21 (51.2) | 27 (58.7) | 0.484 |
| IFG/DM | 10/2 (30.0) | 4/1 (7.70) | 0.003 |
| Pancreatic anomalies | 9 (20.9) | 0 (0) | <0.001 a |
| Liver involvement | 6 (14.3) | 1 (1.5) | 0.028 a |
| Genital tract anomaly | 2 (4.7) | 4 (6.2) | 0.305 a |
| Developmental/speech delay | 3 (7.0) | 1 (1.5) | 0.143 |
| Hypertension | 11 (27.5) c | 10 (15.4) d | 0.529 |
| HNF1B+ | HNF1B- | p Value | |
|---|---|---|---|
| Renal hyperechogenicity | 27 (73.0) | 10 (27.0) | <0.001 |
| Renal cysts | 26 (43.4) | 34 (56.7) | 0.359 |
| Multicystic dysplastic kidney | 17 (60.7) | 11 (39.3) | 0.008 |
| Renal hypoplasia/hypodysplasia | 8 (57.1) | 6 (42.9) | 0.147 |
| Urinary tract malformations | 11 (91.7) a | 1 (8.3) b | <0.001 |
| Solitary kidney | 5 (27.8) | 13 (72.2) | 0.267 |
| Parameter | Age Group | HNF1B+ | HNF1B- | p Value |
|---|---|---|---|---|
| BMI-SDS | 0–9 | 0.31 (−0.19–0.81; n = 37) | 0.32 (−0.26–0.90; n = 21) | 0.992 |
| 10–18 | 0.41 (−0.03–0.86; n = 31) | 0.36 (−0.03–0.74; n = 32) | 0.846 | |
| eGFR (mL/min/1.73 m2) | 1–9 | 112.28 (103.80–120.76; n = 33) | 128.89 (109.05–148.72; n = 17) | 0.119 |
| 10–18 | 95.01 (80.59–109.43; n = 32) | 107.89 (94.96–120.81; n = 32) | 0.180 | |
| sUA (mg/dL) | 0–9 | 4.93 (4.59–5.26; n = 35) | 4.14 (3.73–4.54; n = 33) | 0.003 |
| 10–18 | 6.50 (5.89–7.11; n = 25) | 5.63 (5.00–6.26; n = 32) | 0.052 | |
| Hyperuricemia (%) | 0–9 | 37.5% (n = 24) | 8.6% (n = 35) | 0.017 |
| 10–18 | 50% (n = 16) | 23.3% (n = 30) | 0.066 | |
| FEUA (%) | 0–9 | 7.33 (6.01–8.65; n = 25) | 6.82 (5.92–7.72; n = 25) | 0.511 |
| 10–18 | 6.16 (4.77–7.55; n = 21) | 5.60 (4.87–6.32; n = 29) | 0.425 |
| Parameter | B | SE | Beta | t | F | R2 |
|---|---|---|---|---|---|---|
| (Constant) | 9.95 | 0.85 | --- | 11.72 *** | 41.47 *** | 0.85 |
| eGFR | −0.03 | 0.01 | −0.60 | −6.31 *** | ||
| PTH | 0.02 | 0.00 | 0.44 | 4.75 *** | ||
| FEUA | −0.31 | 0.07 | −0.36 | −4.24 *** |
| Study Group | Hyperuricemia | Renal Function in Hyperuricemic Patients (Number of Cases) | Reference Values for Hyperuricemia | |||
|---|---|---|---|---|---|---|
| HNF1B+ | HNF1B- | |||||
| Children | Adults | Children | Adults | |||
| Ulinski et al. (2006) [6] | 7/23 a (30%) | - | - | not specified | not given | |
| Decramer et al. (2007) [7] | 11/18 (61%) | - | - | CKD I (3), CKD II (2), CKD III (5), CKD 5 (1) | not given | |
| Adalat et al. (2009) [8] | 10/14 (71%) | - | 7/15 (47%) | - | CKD ≤ III only for both HNF1B+ and HNF1B- | age-dependent reference limits |
| Heidet et al. (2010) [9] | 12/75 (16%) b | - | CKD I (3), CKD II (1), CKD III (1), CKD V (1), no data on remaining 6 cases | not given | ||
| Raaijmakers et.al (2014) [10] | 4/20 (20%) | 41/185 (22.2%) | CKD I–III (in all HNF1B+ cohort), no data on renal function in HNF1B- | >5.7 mg/dL in females, >7 mg/dL in males, irrespective of age | ||
| Madariaga et al. (2018) [11] | 6/17 (27%) | 0/4 | 12/36 (33%) | - | CKD I (1), CKD II (1), CKD III (2), CKD V (2) in HNF1B+, no data on renal function in HNF1B- | not given |
| Okorn et al. (2019) [12] | 19/52 (37%) | - | - | CKD I (10), CKD II (5),CKD IV (2), CKD V (2) | age-dependent reference limits | |
| Nagano et al. (2019) [13] | 2/18 (11%) | 4/13 (31%) | - | CKD III (5), CKD IV (1) | sUA > 7 mg/dL, irrespective of age and sex | |
| Lim et al. (2020) [14] | 8/11 (73%) | 3/3 (100%) | - | CKD I (2), CKD II (4), CKD III (4), CKD V (1) | sUA > 7 mg/dL, irrespective of age and sex | |
| Our study (2021) | 17/40 (42.5%) | - | 10/65 (15.4%) | - | CKD I (7), CKD II (8), CKD III (2) | age- and sex-appropriate norms |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kołbuc, M.; Bieniaś, B.; Habbig, S.; Kołek, M.F.; Szczepańska, M.; Kiliś-Pstrusińska, K.; Wasilewska, A.; Adamczyk, P.; Motyka, R.; Tkaczyk, M.; et al. Hyperuricemia Is an Early and Relatively Common Feature in Children with HNF1B Nephropathy but Its Utility as a Predictor of the Disease Is Limited. J. Clin. Med. 2021, 10, 3265. https://doi.org/10.3390/jcm10153265
Kołbuc M, Bieniaś B, Habbig S, Kołek MF, Szczepańska M, Kiliś-Pstrusińska K, Wasilewska A, Adamczyk P, Motyka R, Tkaczyk M, et al. Hyperuricemia Is an Early and Relatively Common Feature in Children with HNF1B Nephropathy but Its Utility as a Predictor of the Disease Is Limited. Journal of Clinical Medicine. 2021; 10(15):3265. https://doi.org/10.3390/jcm10153265
Chicago/Turabian StyleKołbuc, Marcin, Beata Bieniaś, Sandra Habbig, Mateusz F. Kołek, Maria Szczepańska, Katarzyna Kiliś-Pstrusińska, Anna Wasilewska, Piotr Adamczyk, Rafał Motyka, Marcin Tkaczyk, and et al. 2021. "Hyperuricemia Is an Early and Relatively Common Feature in Children with HNF1B Nephropathy but Its Utility as a Predictor of the Disease Is Limited" Journal of Clinical Medicine 10, no. 15: 3265. https://doi.org/10.3390/jcm10153265