
Pre-Stroke Statin Therapy Improves In-Hospital Prognosis Following Acute Ischemic Stroke Associated with Well-Controlled Nonvalvular Atrial Fibrillation

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Comparison of Variables in Patients with AF-Related Stroke Who Were Taking Statins before Hospitalization versus Those Not Taking Statins before Hospitalization
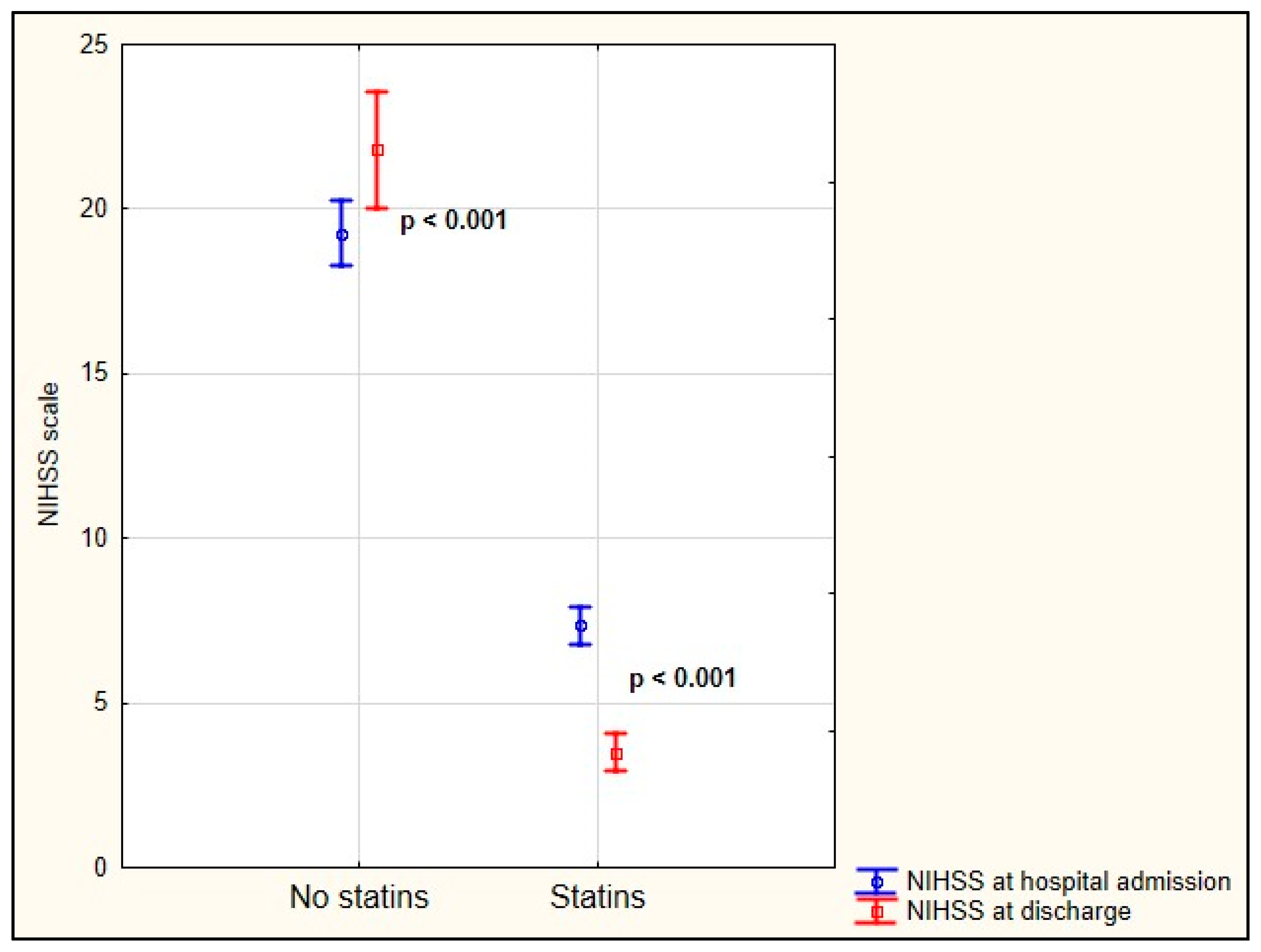
3.2. Prognosis in Patients with Acute AF-Related Stroke Who Were Taking Statins before Hospitalization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolowacz, S.E.; Samuel, M.; Brennan, V.K.; Jasso-Mosqueda, J.-G.; Van Gelder, I.C. The cost of illness of atrial fibrillation: A systematic review of the recent literature. Europace 2011, 13, 1375–1385. [Google Scholar] [CrossRef]
- Friberg, L.; Bergfeldt, L. Atrial fibrillation prevalence revisited. J. Intern. Med. 2013, 274, 461–468. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Krijthe, B.P.; Kunst, A.; Benjamin, E.; Lip, G.Y.; Franco, O.H.; Hofman, A.; Witteman, J.C.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef] [Green Version]
- EAFT (European Atrial Fibrillation Trial) Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet 1993, 342, 1255–1262. [Google Scholar] [CrossRef]
- Laupacis, A. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch. Intern. Med. 1994, 154, 1449–1457. [Google Scholar]
- Undas, A.; Pasierski, T.; Windyga, J.; Crowther, M. Practical aspects of new oral anticoagulant use in atrial fibrillation. Pol. Arch. Intern. Med. 2014, 124, 124–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.V.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef]
- Giugliano, R.; Ruff, C.T.; Braunwald, E.; Murphy, A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus Warfarin in Patients with Atrial Fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [Green Version]
- Heidbuchel, H.; Verhamme, P.; Alings, M.; Antz, M.; Hacke, W.; Oldgren, J.; Sinnaeve, P.; Camm, A.J.; Kirchhof, P. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Europace 2013, 15, 625–651. [Google Scholar] [CrossRef] [PubMed]
- Ciurus, T.; Sobczak, S.; Cichocka-Radwan, A.; Lelonek, M. New oral anticoagulants—A practical guide. Pol. J. Cardio-Thoracic Surg. 2015, 12, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Raval, A.N.; Cigarroa, J.E.; Chung, M.K.; Diaz-Sandoval, L.J.; Diercks, D.; Piccini, J.P.; Jung, H.S.; Washam, J.B.; Welch, B.G.; Zazulia, A.R.; et al. Management of Patients on Non–Vitamin K Antagonist Oral Anticoagulants in the Acute Care and Periprocedural Setting: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e604–e633. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Levy, D.; Vaziri, S.M.; D’Agostino, R.B.; Belanger, A.J.; Wolf, P.A. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA 1994, 271, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Psaty, B.M.; Manolio, T.A.; Kuller, L.H.; Kronmal, R.A.; Cushman, M.; Fried, L.P.; White, R.; Furberg, C.D.; Rautaharju, P.M. Incidence of and risk factors for atrial fibrillation in older adults. Circulation 1997, 96, 2455–2461. [Google Scholar] [CrossRef]
- Conen, D.; Tedrow, U.B.; Koplan, B.A.; Glynn, R.J.; Buring, J.E.; Albert, C.M. Response to Letter Regarding Article, “Influence of Systolic and Diastolic Blood Pressure on the Risk of Incident Atrial Fibrillation in Women”. Circulation 2010, 121, 2146–2152. [Google Scholar] [CrossRef]
- Huxley, R.R.; Lopez, F.L.; Folsom, A.R.; Agarwal, S.K.; Loehr, L.R.; Soliman, E.Z.; Maclehose, R.; Konety, S.; Alonso, A. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: The Atherosclerosis Risk in Communities (ARIC) study. Circulation 2011, 123, 1501–1508. [Google Scholar] [CrossRef] [Green Version]
- Nalliah, C.J.; Sanders, P.; Kottkamp, H.; Kalman, J.M. The role of obesity in atrial fibrillation. Eur. Heart J. 2016, 37, 1565–1572. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Nowacki, P.; Gołąb-Janowska, M. Atrial fibrillation risk factors in patients with ischemic stroke. Arch. Med. Sci. 2021, 17, 19–24. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collabora-tion with the European Association of Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–489. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Nowacki, P.; Gołąb-Janowska, M. Risk factors for ischemic stroke in patients with non-valvular atrial fibrillation and therapeutic international normalized ratio range. Arch. Med. Sci. 2019, 15, 1217–1222. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Staszewski, J.; Dębiec, A.; Nowakowska-Kotas, M.; Szylińska, A.; Rotter, I. Ischemic Stroke Risk Factors in Patients with Atrial Fibrillation Treated with New Oral Anticoagulants. J. Clin. Med. 2021, 10, 1223. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.K.; Laufs, U. Pleiotropic Effects of Statins. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 89–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavalipati, N.; Shah, J.; Ramakrishan, A.; Vasnawala, H. Pleiotropic effects of statins. Indian J. Endocrinol. Metab. 2015, 19, 554–562. [Google Scholar] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef] [Green Version]
- Tramacere, I.; Boncoraglio, G.B.; Banzi, R.; Del Giovane, C.; Kwag, K.H.; Squizzato, A.; Moja, L. Comparison of statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: A systematic review and network meta-analysis. BMC Med. 2019, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Ntaios, G.; Papavasileiou, V.; Makaritsis, K.; Milionis, H.; Manios, E.; Michel, P.; Lip, G.; Vemmos, K. Statin treatment is associated with improved prognosis in patients with AF-related stroke. Int. J. Cardiol. 2014, 177, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.; Seo, W.; Park, M.; Kim, J.; Chung, J.; Bang, O.Y.; Kim, G.; Song, T.; Kim, B.J.; Heo, S.H.; et al. Effect of Statin Therapy on Outcomes of Patients With Acute Ischemic Stroke and Atrial Fibrillation. J. Am. Heart Assoc. 2019, 8, e013941. [Google Scholar] [CrossRef]
- Ingrid, L.; Von Euler, M.; Sunnerhagen, K.S. Association of prestroke medicine use and health outcomes after ischaemic stroke in Sweden: A registry-based cohort study. BMJ Open 2020, 10, e036159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, H.; Wakisaka, Y.; Matsuo, R.; Makihara, N.; Hata, J.; Kuroda, J.; Ago, T.; Kitayama, J.; Nakane, H.; Kamouchi, M.; et al. Influence of Statin Pretreatment on Initial Neurological Severity and Short-Term Functional Outcome in Acute Ischemic Stroke Patients: The Fukuoka Stroke Registry. Cerebrovasc. Dis. 2016, 42, 395–403. [Google Scholar] [CrossRef]
- Lyden, P. Using the National Institutes of Health Stroke Scale: A Cautionary Tale. Stroke 2017, 48, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, J.S.; O’Connell, H.; Li, S.; Ziegler, P.D. Thirty-Second Gold Standard Definition of Atrial Fibrillation and Its Relationship with Subsequent Arrhythmia Patterns: Analysis of a Large Prospective Device Database. Circ. Arrhythm. Electrophysiol. 2018, 11, e006274. [Google Scholar] [CrossRef]
- Mancia, G.; Laurent, S.; Agabiti-Rosei, E.; Ambrosioni, E.; Burnier, M.; Caulfield, M.J.; Cifkova, R.; Clement, D.; Coca, A.; Dominiczak, A.; et al. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2007, 25, 1105–1187. [Google Scholar] [CrossRef]
- Tahrani, A.A.; Bailey, C.J.; Del Prato, S.; Barnett, A.H. Management of type 2 diabetes: New and future developments in treatment. Lancet 2011, 378, 182–197. [Google Scholar] [CrossRef]
- Inzitari, D.; Eliasziw, M.; Gates, P.; Sharpe, B.L.; Chan, R.K.; Meldrum, H.E.; Barnett, H.J. The Causes and Risk of Stroke in Patients with Asymptomatic Internal-Carotid-Artery Stenosis. N. Engl. J. Med. 2000, 342, 1693–1701. [Google Scholar] [CrossRef]
- Halliday, A.; Harrison, M.; Hayter, E. Ten-Year Stroke Prevention after Successful Carotid Endarterectomy for Asymptomatic Stenosis (ACST-1): A Multicentre Randomised Trial. J. Vasc. Surg. 2011, 53, 246. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.-S.; Pak, H.-N.; Park, D.-H.; Yoo, J.; Kim, T.-H.; Uhm, J.-S.; Kim, Y.D.; Nam, H.S.; Joung, B.; Lee, M.-H.; et al. Non-cardioembolic risk factors in atrial fibrillation-associated ischemic stroke. PLoS ONE 2018, 13, e0201062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar]
- Biffi, A.; Devan, W.J.; Anderson, C.D.; Cortellini, L.; Furie, K.L.; Rosand, J.; Rost, N.S. Statin treatment and functional outcome after ischemic stroke: Case-control and meta-analysis. Stroke 2011, 42, 1314–1319. [Google Scholar] [CrossRef] [Green Version]
- Eun, M.Y.; Jung, J.M.; Choi, K.H.; Seo, W.K. Statin Effects in Atrial Fibrillation-Related Stroke: A Systematic Review and Meta-Analysis. Front. Neurol. 2020, 11, 589684. [Google Scholar] [CrossRef]
- Endres, M. Statins and Stroke. Br. J. Pharmacol. 2005, 25, 1093–1110. [Google Scholar] [CrossRef] [Green Version]
- Tu, H.T.; Campbell, B.; Christensen, S.; Collins, M.; De Silva, D.A.; Butcher, K.S.; Parsons, M.W.; Desmond, P.M.; Barber, P.A.; Levi, C.R.; et al. Pathophysiological Determinants of Worse Stroke Outcome in Atrial Fibrillation. Cerebrovasc. Dis. 2010, 30, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Iguchi, Y.; Yamashita, S.; Shibazaki, K.; Kobayashi, K.; Inoue, T. Atrial fibrillation as an independent predictor for no early recanalization after IV-t-PA in acute ischemic stroke. J. Neurol. Sci. 2008, 267, 57–61. [Google Scholar] [CrossRef]
- Pecoraro, V.; Moja, L.; Dall’Olmo, L.; Cappellini, G.; Garattini, S. Most appropriate animal models to study the efficacy of statins: A systematic review. Eur. J. Clin. Investig. 2014, 44, 848–871. [Google Scholar] [CrossRef] [PubMed]
- Horwich, T.B.; Middlekauff, H.R. Potential Autonomic Nervous System Effects of Statins in Heart Failure. Heart Fail. Clin. 2008, 4, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacoy, G.; Akboga, M.K.; Yayla, C.; Akyel, A.; Turkoglu, S.; Ozdemir, M.; Yalcin, R. The effect of statin treatment on P-wave characteristics and atrial conduction time. Kardiol. Polska 2015, 73, 747-452. [Google Scholar] [CrossRef]
- Loppnow, H.; Zhang, L.; Buerke, M.; Lautenschlager, M.; Chen, L.; Frister, A.; Schlitt, A.; Luther, T.; Song, N.; Hofmann, B.; et al. Statins potently reduce the cytokine-mediated IL-6 release in SMC/MNC cocultures. J. Cell. Mol. Med. 2011, 15, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Dimmeler, S.; Aicher, A.; Vasa, M.; Mildner-Rihm, C.; Adler, K.; Tiemann, M.; Rutten, H.; Fichtlscherer, S.; Martin, H.; Zeiher, A.M. HMG-CoA reductase inhibitors (statins) increase endothelial progenitor cells via the PI 3-kinase/Akt pathway. J. Clin. Investig. 2001, 108, 391–397. [Google Scholar] [CrossRef]
- Suzuki, G.; Iyer, V.; Cimato, T.; Canty, J.J.M. Pravastatin Improves Function in Hibernating Myocardium by Mobilizing CD133 + and cKit + Bone Marrow Progenitor Cells and Promoting Myocytes to Reenter the Growth Phase of the Cardiac Cell Cycle. Circ. Res. 2009, 104, 255–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, K.E.; Turner, N.A. Statins and myocardial remodelling: Cell and molecular pathways. Expert Rev. Mol. Med. 2011, 13, e22. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables. | No Statins before Hospital Admission n = 191 | Statins before Hospital Admission n = 342 | p | |
|---|---|---|---|---|
| Age [years], mean ± SD; median | 81.86 ± 8.67; 83.0 | 75.76 ± 8.18; 77.0 | <0.001 | |
| Gender | male | 55 (28.80%) | 119 (34.80%) | 0.157 |
| female | 136 (71.20%) | 223 (65.20%) | ||
| Hypertension | no | 27 (14.14%) | 2 (0.58%) | <0.001 |
| yes | 164 (85.86%) | 340 (99.42%) | ||
| Coronary heart disease | no | 70 (36.65%) | 125 (36.55%) | 0.982 |
| yes | 121 (63.35%) | 217 (63.45%) | ||
| Peripheral arterial disease | no | 165 (86.39%) | 291 (85.09%) | 0.682 |
| yes | 26 (13.61%) | 51 (14.91%) | ||
| Diabetes mellitus | no | 106 (55.50%) | 188 (54.97%) | 0.907 |
| yes | 85 (44.50%) | 154 (45.03%) | ||
| Smoking | no | 126 (65.97%) | 165 (48.25%) | <0.001 |
| yes | 65 (34.03%) | 177 (51.75%) | ||
| Dyslipidemia | no | 138 (73.02%) | 0 (0.00%) | <0.001 |
| yes | 51 (26.98%) | 342 (100.00%) | ||
| Stenosis/occlusion | no | 167 (87.43%) | 302 (88.30%) | 0.767 |
| yes | 24 (12.57%) | 40 (11.70%) | ||
| NIHSS at hospital admission, mean ± SD; median | 19.27 ± 6.71; 20.0 | 7.36 ± 5.29; 6.0 | <0.001 | |
| NIHSS at discharge, mean ± SD; median | 21.81 ± 12.01; 23.0 | 3.51 ± 5.29; 2.0 | <0.001 | |
| Delta NIHSS, mean ± SD; median | 3.25 ± 8.52; 4.0 | −3.73 ± 3.77; −3.0 | <0.001 | |
| Death | no | 95 (49.74%) | 332 (97.08%) | <0.001 |
| yes | 96 (50.26%) | 10 (2.92%) | ||
| Variables | No Adjusted | Adjusted * | ||||||
|---|---|---|---|---|---|---|---|---|
| p | OR | CI OR—95% | CI + OR 95% | p | OR | CI OR—95% | CI + OR 95% | |
| Death | <0.001 | 0.030 | 0.015 | 0.059 | <0.001 | 0.022 | 0.008 | 0.060 |
| NIHSS on admission to hospital | <0.001 | 0.766 | 0.734 | 0.799 | <0.001 | 0.790 | 0.742 | 0.843 |
| NIHSS at discharge | <0.001 | 0.818 | 0.791 | 0.846 | <0.001 | 0.840 | 0.804 | 0.877 |
| Delta NIHSS | <0.001 | 0.824 | 0.791 | 0.858 | <0.001 | 0.775 | 0.718 | 0.836 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wańkowicz, P.; Staszewski, J.; Dębiec, A.; Nowakowska-Kotas, M.; Szylińska, A.; Turoń-Skrzypińska, A.; Rotter, I. Pre-Stroke Statin Therapy Improves In-Hospital Prognosis Following Acute Ischemic Stroke Associated with Well-Controlled Nonvalvular Atrial Fibrillation. J. Clin. Med. 2021, 10, 3036. https://doi.org/10.3390/jcm10143036
Wańkowicz P, Staszewski J, Dębiec A, Nowakowska-Kotas M, Szylińska A, Turoń-Skrzypińska A, Rotter I. Pre-Stroke Statin Therapy Improves In-Hospital Prognosis Following Acute Ischemic Stroke Associated with Well-Controlled Nonvalvular Atrial Fibrillation. Journal of Clinical Medicine. 2021; 10(14):3036. https://doi.org/10.3390/jcm10143036
Chicago/Turabian StyleWańkowicz, Paweł, Jacek Staszewski, Aleksander Dębiec, Marta Nowakowska-Kotas, Aleksandra Szylińska, Agnieszka Turoń-Skrzypińska, and Iwona Rotter. 2021. "Pre-Stroke Statin Therapy Improves In-Hospital Prognosis Following Acute Ischemic Stroke Associated with Well-Controlled Nonvalvular Atrial Fibrillation" Journal of Clinical Medicine 10, no. 14: 3036. https://doi.org/10.3390/jcm10143036