
A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome—A Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
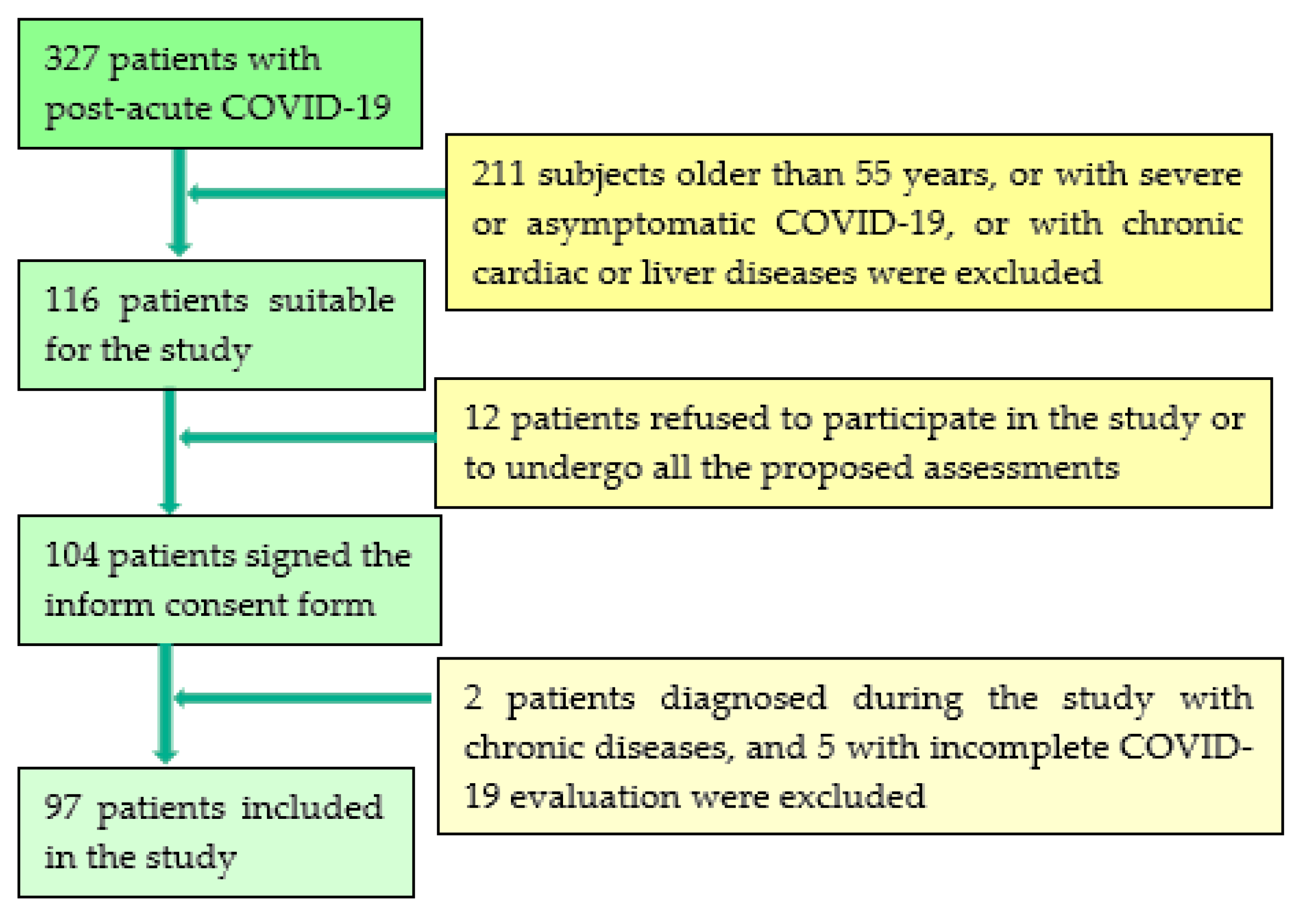
2.1. Study Population
2.2. Methods
- −
- ShearWave PLUS Elastography
- −
- Viscosity PLUS
- −
- Attenuation PLUS and Sound Speed PLUS
- −
- Transient Elastography and Controlled Attenuation Parameter
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html (accessed on 10 January 2021).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to Sars-Cov-2 (Covid-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef]
- Ungureanu, B.S.; Vladut, C.; Bende, F.; Sandru, V.; Tocia, C.; Turcu-Stiolica, R.-A.; Groza, A.; Balan, G.G.; Turcu-Stiolica, A. Impact of the COVID-19 Pandemic on Health-Related Quality of Life, Anxiety, and Training Among Young Gastroenterologists in Romania. Front. Psychol. 2020, 11, 579177. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M.; et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- Mantovani, A.; Beatrice, G.; Dalbeni, A. Coronavirus disease 2019 and prevalence of chronic liver disease: A meta-analysis. Liver Int. 2020, 40, 1316–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Wong, Y.J.; Tan, M.; Zheng, Q.; Li, J.W.; Kumar, R.; Fock, K.M.; Teo, E.K.; Ang, T.L. A systematic review and meta-analysis of the COVID-19 associated liver injury. Ann. Hepatol. 2020, 19, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.-Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the cardiovascular system: Acute and long-term implications. Eur. Hear. J. 2020, 41, 1798–1800. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Fonarow, G.C. Coronavirus Disease 2019 (COVID-19) and the Heart—Is Heart Failure the Next Chapter? JAMA Cardiol. 2020, 5, 1216. [Google Scholar] [CrossRef]
- Zhang, C.; Shi, L.; Wang, F.-S. Liver injury in COVID-19: Management and challenges. Lancet Gastroenterol. Hepatol. 2020, 5, 428–430. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: What do we know about “long covid”? BMJ 2020, 370, m2815. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, C.; Collins, L.F.; Malani, P. Long-term Health Consequences of COVID-19. JAMA 2020, 324, 1723. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiol. 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.; Marino, P.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrettou, A.-R.; Parissis, J.; Ikonomidis, I. The Dual Role of Echocardiography in the Diagnosis of Acute Cardiac Complications and Treatment Monitoring for Coronavirus Disease 2019 (COVID-19). Front. Cardiovasc. Med. 2020, 7. [Google Scholar] [CrossRef]
- Baycan, O.F.; Barman, H.A.; Atici, A.; Tatlisu, A.; Bolen, F.; Ergen, P.; Icten, S.; Gungor, B.; Caliskan, M. Evaluation of biventricular function in patients with COVID-19 using speckle tracking echocardiography. Int. J. Cardiovasc. Imaging 2021, 37, 135–144. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med.-Eur. J. Ultrasound 2017, 38, e16–e47. [Google Scholar] [CrossRef] [Green Version]
- Sasso, M.; Miette, V.; Sandrin, L.; Beaugrand, M. The controlled attenuation parameter (CAP): A novel tool for the non-invasive evaluation of steatosis using Fibroscan®. Clin. Res. Hepatol. Gastroenterol. 2012, 36, 13–20. [Google Scholar] [CrossRef]
- Petroff, D.; Blank, V.; Newsome, P.N.; Shalimar; Voican, C.S.; Thiele, M.; de Lédinghen, V.; Baumeler, S.; Chan, W.K.; Perlemuter, G.; et al. Assessment of hepatic steatosis by controlled attenuation parameter using the M and XL probes: An individual patient data meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 185–198. [Google Scholar] [CrossRef]
- Geddes, L. Why Strange and Debilitating Coronavirus Symptoms Can Last for Months. Available online: https://www.newscientist.com/article/mg24632881-400-why-strange-and-debilitating-coronavirus-symptoms-can-last-for-months/ (accessed on 5 March 2021).
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; Van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, S.; Xu, M.; Yu, P.; Zheng, S.; Duan, Z.; Liu, J.; Chen, Y.; Li, J. Risk Factors Related to Hepatic Injury in Patients with Corona Virus Disease 2019. medRxiv 2020. [Google Scholar] [CrossRef]
- Sharma, A.; Jaiswal, P.; Kerakhan, Y.; Saravanan, L.; Murtaza, Z.; Zergham, A.; Honganur, N.-S.; Akbar, A.; Deol, A.; Francis, B.; et al. Liver disease and outcomes among COVID-19 hospitalized patients—A systematic review and meta-analysis. Ann. Hepatol. 2021, 21, 100273. [Google Scholar] [CrossRef]
- Su, T.-H.; Kao, J.-H. The clinical manifestations and management of COVID-19-related liver injury. J. Formos. Med. Assoc. 2020, 119, 1016–1018. [Google Scholar] [CrossRef] [PubMed]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, A.G.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ distribution of severe acute respiratory syndrome(SARS) associated coronavirus(SARS-CoV) in SARS patients: Implications for pathogenesis and virus transmission pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Liu, J.; Lu, M.; Yang, D.; Zheng, X. Liver injury during highly pathogenic human coronavirus infections. Liver Int. 2020, 40, 998–1004. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Abe, M.; Yoshimasu, Y.; Kasai, Y.; Sakamaki, K.; Hara, T.; Itoi, T. The Role of Multiparametric US of the Liver for the Evaluation of Nonalcoholic Steatohepatitis. Radiology 2020, 296, 532–540. [Google Scholar] [CrossRef]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Furuichi, Y.; Itoi, T. Viscoelasticity Measurement in Rat Livers Using Shear-Wave US Elastography. Ultrasound Med. Biol. 2018, 44, 2018–2024. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, J.Y.; Bae, J.S.; Yi, N.-J.; Lee, K.-W.; Suh, K.-S.; Kim, H.; Lee, K.B.; Han, J.K. Shear-Wave Dispersion Slope from US Shear-Wave Elastography: Detection of Allograft Damage after Liver Transplantation. Radiology 2019, 293, 327–333. [Google Scholar] [CrossRef]
- Deffieux, T.; Gennisson, J.-L.; Bousquet, L.; Corouge, M.; Cosconea, S.; Amroun, D.; Tripon, S.; Terris, B.; Mallet, V.; Sogni, P.; et al. Investigating liver stiffness and viscosity for fibrosis, steatosis and activity staging using shear wave elastography. J. Hepatol. 2015, 62, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Sanchez, W.; Callstrom, M.R.; Gorman, B.; Lewis, J.T.; Sanderson, S.O.; Greenleaf, J.F.; Xie, H.; Shi, Y.; Pashley, M.; et al. Assessment of Liver Viscoelasticity by Using Shear Waves Induced by Ultrasound Radiation Force. Radiology 2013, 266, 964–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertanto, D.M.; Sutanto, H.; Wungu, C.D.K. Immunomodulation as a Potent COVID-19 Pharmacotherapy: Past, Present and Future. Preprints 2021. [Google Scholar] [CrossRef]
- Popa, A.; Șirli, R.; Popescu, A.; Bâldea, V.; Lupușoru, R.; Bende, F.; Cotrău, R.; Sporea, I. Ultrasound-Based Quantification of Fibrosis and Steatosis with a New Software Considering Transient Elastography as Reference in Patients with Chronic Liver Diseases. Ultrasound Med. Biol. 2021, S0301562921001034. [Google Scholar] [CrossRef]
- Popa, A.; Bende, F.; Șirli, R.; Popescu, A.; Bâldea, V.; Lupușoru, R.; Cotrău, R.; Fofiu, R.; Foncea, C.; Sporea, I. Quantification of Liver Fibrosis, Steatosis, and Viscosity Using Multiparametric Ultrasound in Patients with Non-Alcoholic Liver Disease: A “Real-Life” Cohort Study. Diagnostics 2021, 11, 783. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics, Laboratory Data | COVID-19 Patients with Pulmonary Injury (2–40%) n = 53 | COVID-19 Patients without Pulmonary Injury n = 44 | p-Value |
|---|---|---|---|
| Age (years) | 46.01 ± 7.66 | 41.31 ± 10.49 | 0.01 |
| Gender: | |||
| Females | 30/53 (56.6%) | 30/44 (68.2%) | 0.33 |
| Males | 23/53 (43.4%) | 14/44 (31.8%) | 0.33 |
| BMI (kg/m2) | 30.66 ± 6.54 | 26.53 ± 5.41 | 0.001 |
| Results of the Initial COVID-19 Assessment | |||
| TCT pulmonary injury | 13.71% (2–40) | 0% | 0.03 |
| Initial CRP (mg/L) | 26.12 ± 15.73 | 18.63 ± 9.53 | 0.006 |
| ALT (IU/L) | 55.35 ± 41.24 | 34.95 ± 18.39 | 0.007 |
| AST(IU/L) | 44.64 ± 30.99 | 32.47 ± 11.36 | 0.015 |
| O2 saturation (%) | 96.28 ± 1.34 | 97.68 ± 3.62 | 0.07 |
| Weeks since COVID | 7 (3–10) | 8 (4–11) | 0.01 |
| Nr. of symptoms | 4 (2–6) | 2 (1–5) | ˂0.0001 |
| Parameters | COVID-19 Patients with Pulmonary Injury (2–30%), n = 53 | COVID-19 Patients without Pulmonary Injury, n = 44 | p-Value |
|---|---|---|---|
| Echocardiographic Parameters | |||
| LVMI (˂95/115 g/m2) | 97.05 ± 27.96 | 85.47 ± 20.45 | 0.024 |
| LAVI (˂34 mL/m2) | 18.51 ± 6.63 | 16.9 ± 7.05 | 0.250 |
| E/A (˃1) | 1.18 ± 0.74 | 1.06 ± 0.20 | 0.299 |
| E/e’ (˂14) | 13.0 ±2.77 | 12.83 ± 2.33 | 0.876 |
| TRV (˂2.8 m/s) | 2.89 ± 0.30 | 2.37 ± 0.38 | <0.0001 |
| sPAP (˂ 35 mmHg) | 38.97 ± 6.97 | 28.23 ± 7.31 | <0.0001 |
| TAPSE (˃17 mm) | 19.33 ± 3.75 | 20.59 ± 2.95 | 0.073 |
| FAC (˃35%) | 34.75 ± 1.98 | 36.54 ± 1.39 | <0.0001 |
| MAPSE (˃10 mm) | 15.14 ± 2.89 | 15.78 ± 2.31 | 0.238 |
| LVEF (˃50%) | 60.0 ± 10.48 | 59.39 ± 7.18 | 0.744 |
| Liver Elastography Evaluation | |||
| LS by TE (kPa) | 5.08 ± 1.40 | 4.39 ± 1.41 | 0.017 |
| LS by 2D-SWE SSI PLUS (kPa) | 5.23 ± 1.00 | 4.79 ± 0.79 | 0.028 |
| Vi PLUS (PaS) | 1.74 ± 0.28 | 1.64 ± 0.25 | 0.0009 |
| CAP (db/m) | 291.64 ± 71.10 | 266.06 ± 60.77 | 0.062 |
| SSp PLUS (m/s) | 1530.3 ± 24.91 | 1542.88 ± 27.66 | 0.031 |
| Att PLUS (dB/cm/mHz) | 0.47 ± 0.11 | 0.45 ± 0.10 | 0.385 |
| First 8 Weeks n = 60 | Weeks 9–11 n = 37 | p-Value | |
|---|---|---|---|
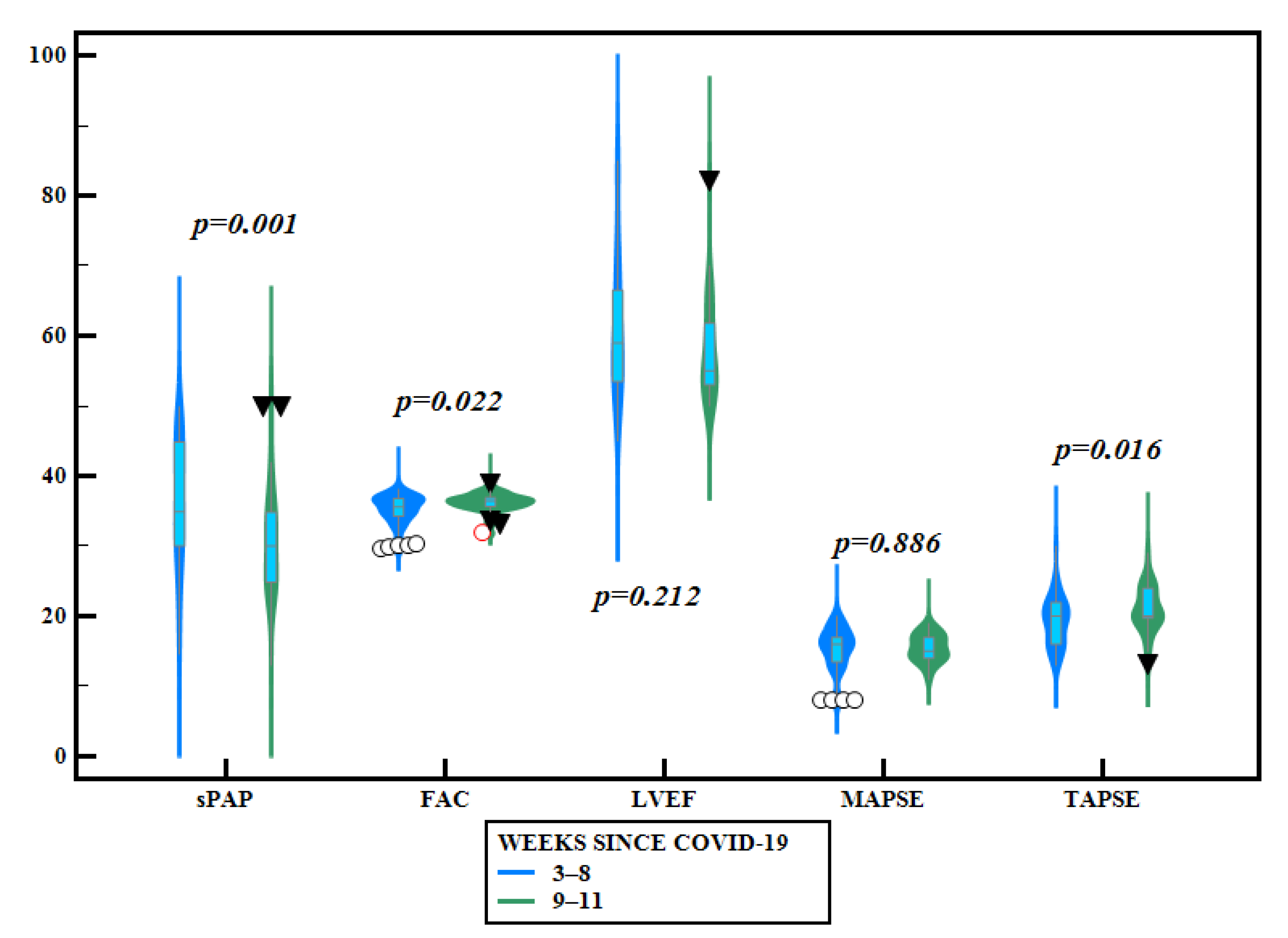
| Echocardiographic Parameters | |||
| E/A | 1.16 ± 0.70 | 1.07 ± 0.19 | p = 0.447 |
| E/e’ | 12.99 ± 2.75 | 12.82 ± 2.28 | p = 0.753 |
| TRV | 2.75 ± 0.42 | 2.50 ± 0.38 | p = 0.004 |
| sPAP | 36.72 ± 9.08 | 30.63 ± 7.71 | p = 0.001 |
| TAPSE | 19.25 ± 3.45 | 20.97 ± 3.21 | p = 0.016 |
| FAC | 35.15 ± 2.16 | 36.22 ± 1.33 | p = 0.022 |
| MAPSE | 15.40 ± 3.03 | 15.48 ± 1.92 | p = 0.886 |
| LVEF | 60.85 ± 10.05 | 57.90 ± 7.04 | p = 0.212 |
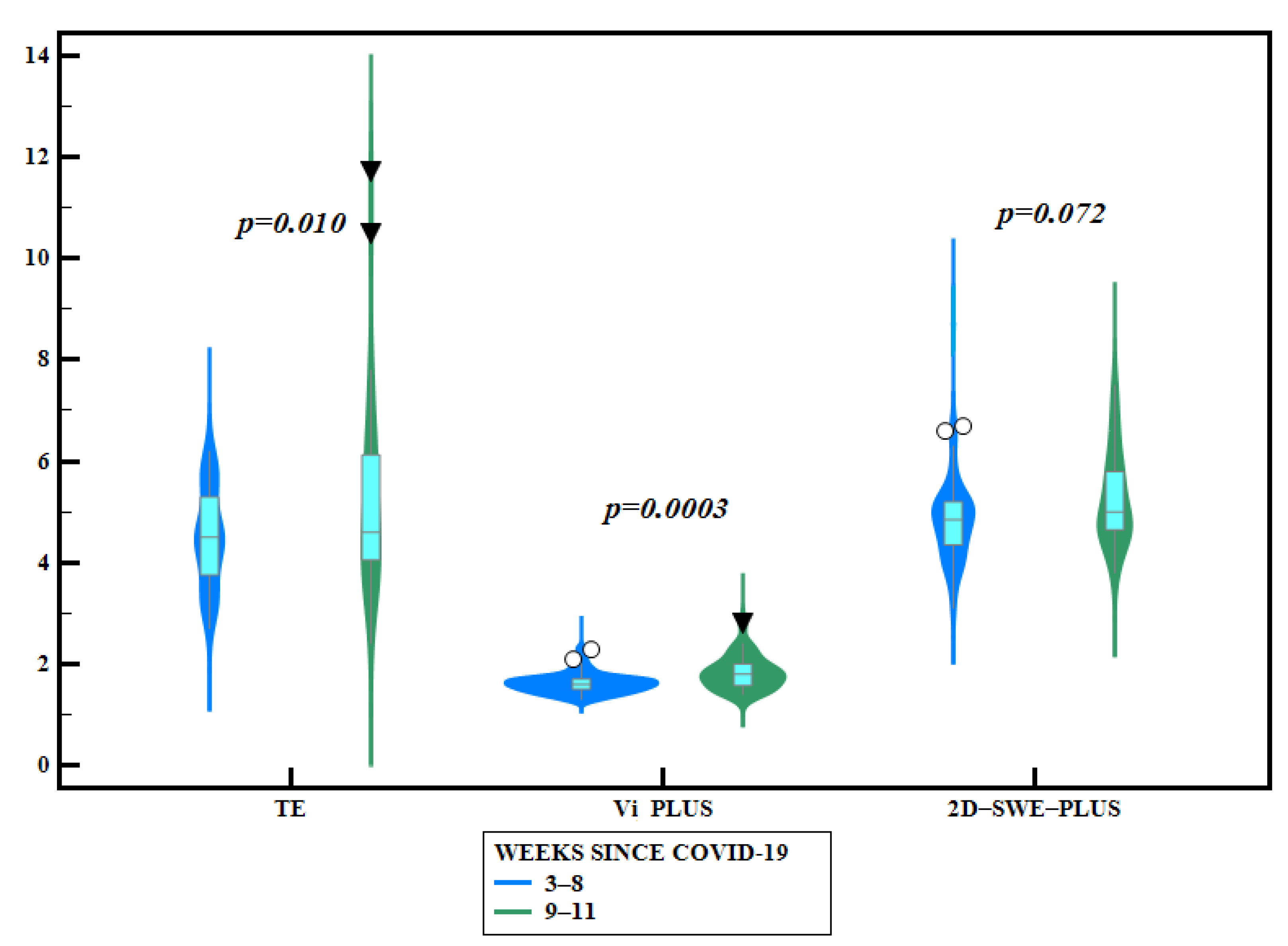
| Liver Elastography Evaluation | |||
| LS by TE (kPa) | 4.48 ±0.95 | 5.24 ± 1.92 | p = 0.010 |
| LS by 2D-SWE SSI PLUS | 4.87 ± 0.91 (n = 52) | 5.24 ± 0.9 (n = 32) | p = 0.072 |
| Vi PLUS (PaS) | 1.61 ± 0.19 (n = 52) | 1.82 ± 0.32 (n = 32) | p = 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bende, F.; Tudoran, C.; Sporea, I.; Fofiu, R.; Bâldea, V.; Cotrău, R.; Popescu, A.; Sirli, R.; Ungureanu, B.S.; Tudoran, M. A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome—A Pilot Study. J. Clin. Med. 2021, 10, 2507. https://doi.org/10.3390/jcm10112507
Bende F, Tudoran C, Sporea I, Fofiu R, Bâldea V, Cotrău R, Popescu A, Sirli R, Ungureanu BS, Tudoran M. A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome—A Pilot Study. Journal of Clinical Medicine. 2021; 10(11):2507. https://doi.org/10.3390/jcm10112507
Chicago/Turabian StyleBende, Felix, Cristina Tudoran, Ioan Sporea, Renata Fofiu, Victor Bâldea, Radu Cotrău, Alina Popescu, Roxana Sirli, Bogdan Silviu Ungureanu, and Mariana Tudoran. 2021. "A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome—A Pilot Study" Journal of Clinical Medicine 10, no. 11: 2507. https://doi.org/10.3390/jcm10112507