
Diagnostic Performance of Selected Baseline Electrocardiographic Parameters for Prediction of Left Ventricular Remodeling in Patients with ST-Segment Elevation Myocardial Infarction


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Evaluation of Electrocardiograms
- heart rate,
- location of MI,
- number of leads with ST-segment elevation,
- sum of ST-segment elevation in all leads,
- maximum ST-segment elevation in a single lead,
- presence of reciprocal ST-segment depression ≥0.1 mV on admission to hospital,
- number of leads with pathological Q-waves (according to the 2007 universal definition of MI) [18],
- the degree of ischemia according to the Birnbaum–Sklarovsky classification [2] and
- QRS complex width.
2.3. Percutaneous Coronary Intervention
2.4. Concomitant Pharmacotherapy
2.5. Echocardiography
2.6. Statistical Analysis
3. Results
3.1. The Course of the Study
3.2. Clinical, Demographic, Angiographic and Biochemical Parameters
3.3. Echocardiographic Characteristics
3.4. Electrocardiographic Characteristics
3.5. Comparison of Demographic, Clinical, Angiographic and Biochemical Characteristics of Patients with LVR (LVR (+) Group) and without LVR (LVR (−) Group)
3.6. Electrocardiographic Characteristics of Patients with LVR
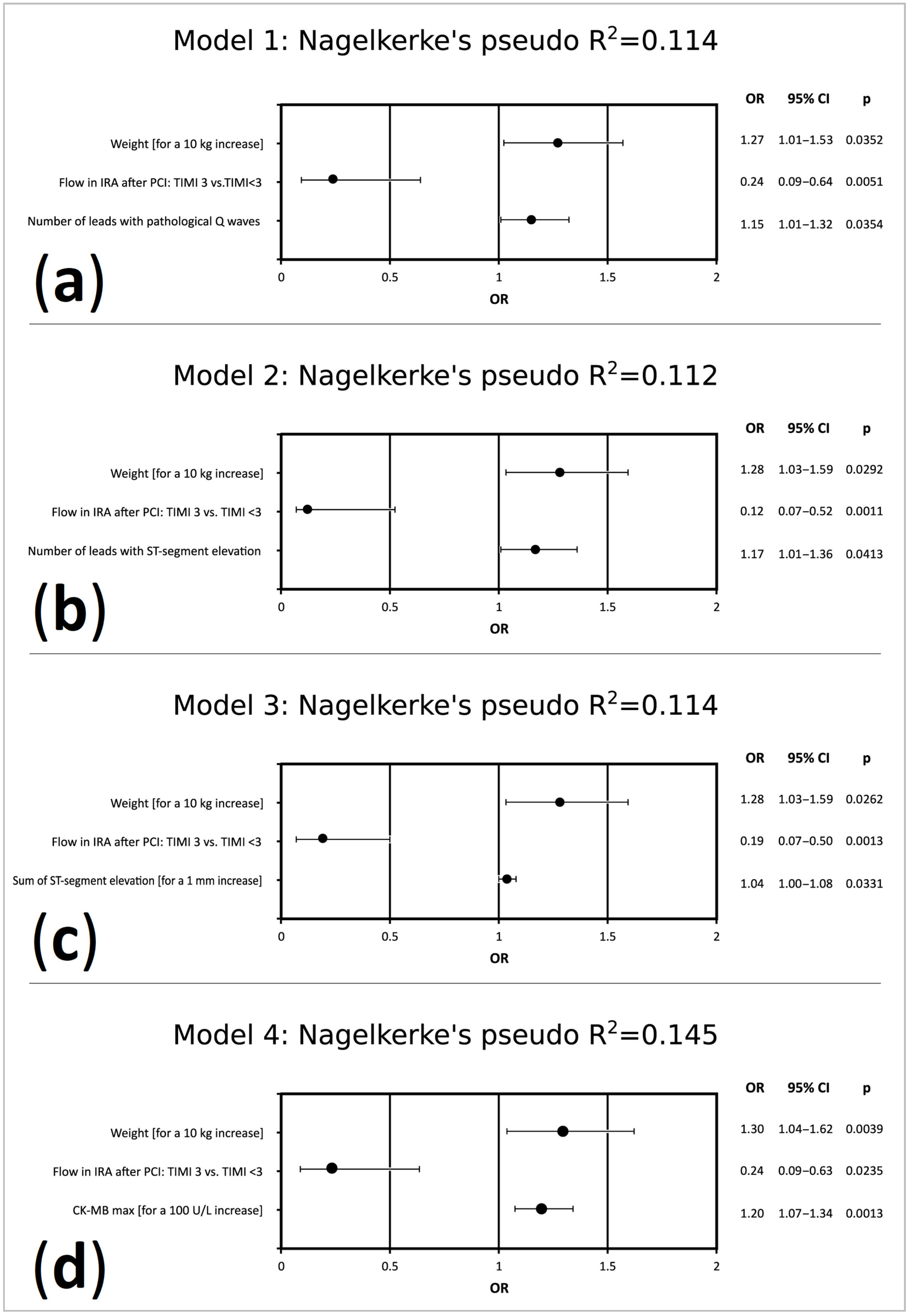
3.7. Predictors of LVR Occurrence 6 Months after Discharge from Hospital in Univariate and Multivariate Logistic Regression Models
3.8. Determinants of Increase in LVEDV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Macfarlane, P.W. The coming of age of electrocardiology. In Comprehensive Electrocardiology; Macfarlane, P.W., van Oosterom, A., Pahlm, O., Kligfield, P., Janse, M., Camm, J., Eds.; Springer: London, UK, 2011; pp. 3–48. [Google Scholar]
- Birnbaum, Y.; Drew, B.J. The electrocardiogram in ST elevation acute myocardial infarction: Correlation with coronary anatomy and prognosis. Postgrad Med. J. 2003, 79, 490–504. [Google Scholar] [CrossRef] [Green Version]
- Huey, B.L.; Gheorghiade, M.; Crampton, R.S.; Beller, G.A.; Kaiser, D.L.; Watson, D.D.; Nygaard, T.W.; Craddock, G.B.; Sayre, S.L.; Gibson, R.S. Acute non-Q wave myocardial infarction associated with early ST segment elevation: Evidence for spontaneouscoronaryreperfusion and implications for thrombolytictrials. J. Am. Coll. Cardiol. 1987, 9, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Kaul, P.; Fu, Y.; Westerhout, C.M.; Granger, C.B.; Armstrong, P.W. Relative prognostic value of baseline Q wave and time from symptom onset among men and women with ST-elevation myocardial infarction undergoing percutaneous coronary intervention. Am. J. Cardiol. 2012, 110, 1555–1560. [Google Scholar] [CrossRef]
- Siha, H.; Das, D.; Fu, Y.; Zheng, Y.; Westerhout, C.M.; Storey, R.F.; James, S.; Wallentin, L.; Armstrong, P.W. Baseline Q waves as a prognostic modulator in patients with ST segment elevation: Insights from the PLATO trial. CMAJ 2012, 184, 1135–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minicucci, M.F.; Azevedo, P.S.; Polegato, B.F.; Paiva, S.A.; Zornoff, L.A. Heart failure after myocardial infarction: Clinical implications and treatment. Clin. Cardiol. 2011, 34, 410–414. [Google Scholar] [CrossRef]
- Sutton, M.G.; Sharpe, N. Left ventricular remodeling after myocardial infarction: Pathophysiology and therapy. Circulation 2000, 101, 2981–2988. [Google Scholar] [CrossRef] [PubMed]
- Dargie, H. Heart failure post-myocardial infarction: A review of the issues. Heart 2005, 91 (Suppl. 2), ii3–ii6. [Google Scholar] [CrossRef]
- Struthers, A. Pathophysiology of heart failure following myocardial infarction. Heart 2005, 91 (Suppl. 2), ii14–ii16. [Google Scholar] [CrossRef] [Green Version]
- Cohn, J.N.; Ferrari, R.; Sharpe, N.; Behalf of an International Forum on Cardiac Remodeling. Cardiac remodeling—Concepts and clinical implications: A consensus paper from an international forum on cardiac remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef] [Green Version]
- Bolognese, L.; Neskovic, A.N.; Parodi, G.; Cerisano, G.; Buonamici, P.; Santoro, G.M.; Antoniucci, D. Left ventricular remodeling after primary coronary angioplasty: Patterns of left ventricular dilation and long-term prognostic implications. Circulation 2002, 106, 2351–2357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutton, M.; Pfeffer, M.A.; Plappert, T.; Rouleau, J.L.; Moyé, L.A.; Dagenais, G.R.; Lamas, G.A.; Klein, M.; Sussex, B.; Goldman, S. Quantitative two-dimensional echocardiographic measurements are major predictors of adverse cardiovascular events after acute myocardial infarction. The protective effects of captopril. Circulation 1994, 89, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funaro, S.; La Torre, G.; Madonna, M.; Galiuto, L.; Scarà, A.; Labbadia, A.; Canali, E.; Mattatelli, A.; Fedele, F.; Alessandrini, F.; et al. Incidence, determinants, and prognostic value of reverse left ventricular remodeling after primary percutaneous coronary intervention: Results of the Acute Myocardial Infarction Contrast Imaging (AMICI) multicenter study. Eur. Heart J. 2009, 30, 566–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murkofsky, R.L.; Dangas, G.; Diamond, J.A.; Mehta, D.; Schaffer, A.; Ambrose, J.A. A prolonged QRS duration on surface electrocardiogram is a specific indicator of left ventricular dysfunction. J. Am. Coll. Cardiol. 1998, 32, 476–482. [Google Scholar] [CrossRef] [Green Version]
- Manes, C.; Pfeffer, M.A.; Rutherford, J.D.; Greaves, S.; Rouleau, J.L.; Arnold, J.M.; Menapace, F.; Solomon, S.D. Value of the electrocardiogram in predicting left ventricular enlargement and dysfunction after myocardial infarction. Am. J. Med. 2003, 114, 99–105. [Google Scholar] [CrossRef]
- Van de Werf, F.; Bax, J.; Betriu, A.; Blomstrom-Lundqvist, C.; Crea, F.; Falk, V.; Filippatos, G.; Fox, K.; Huber, K.; Kastrati, A.; et al. Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation. Eur. Heart J. 2008, 29, 2909–2945. [Google Scholar] [CrossRef]
- Van de Werf, F.; Ardissino, D.; Betriu, A.; Cokkinos, D.V.; Falk, E.; Fox, K.A.; Julian, D.; Lengyel, M.; Neumann, F.J.; Ruzyllo, W.; et al. Management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur. Heart J. 2003, 24, 28–66. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, K.; Alpert, J.S.; White, H.D.; on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Eur. Heart J. 2007, 28, 2525–2538. [Google Scholar] [PubMed]
- Schiller, N.; Shah, P.; Crawford, M.; DeMaria, A.; Devereux, R.; Feigenbaum, H.; Gutgesell, H.; Reichek, N.; Sahn, D.; Schnittger, I.; et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. J. Am. Soc. Echocardiogr. 1989, 2, 358–367. [Google Scholar] [CrossRef]
- Lang, R.; Bierig, M.; Devereux, B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar] [CrossRef]
- Armstrong, P.W.; Fu, Y.; Westerhout, C.M.; Hudson, M.P.; Mahaffey, K.W.; White, H.D.; Todaro, T.G.; Adams, P.X.; Aylward, P.E.; Granger, C.B. Baseline Q-wave surpasses time from symptom onset as a prognostic marker in ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention. J. Am. Coll. Cardiol. 2009, 53, 1503–1509. [Google Scholar] [CrossRef] [Green Version]
- Husser, O.; Bodí, V.; Sanchis, J.; Núnez, J.; Mainar, L.; Rumiz, E.; López-Lereu, M.P.; Monmeneu, J.; Chaustre, F.; Trapero, I.; et al. The sum of ST-segment elevation is the best predictor of microvascular obstruction in patients treated successfully by primary percutaneous coronary intervention. Cardiovascular magnetic resonance study. Rev. Esp. Cardiol. 2010, 63, 1145–1154. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Study Population (n = 249) | Patients with LVR at 6 Months (n = 68) | Patients without LVR at 6 Months (n = 181) | p-Value * |
|---|---|---|---|---|
| Age (years) | 57.0 (51.0-64.0) | 55.5 (50.0-62.0) | 58.0 (52.0-64.0) | 0.166 |
| Gender (male/female) | 186 (74.7%)/63 (25.3%) | 52 (76.5%)/16 (23.5%) | 134 (74.0%)/47 (26.0%) | 0.693 |
| Weight (kg) | 78.0 (70.0-88.0) | 80.0 (71.0-91.5) | 78.0 (70.0-87.0) | 0.092 |
| Height (cm) | 170.0 (165.0-176.0) | 172.5 (166.0-176.5) | 170.0 (164.0-176.0) | 0.085 |
| Time from symptom onset to PCI (min) | 220.0 (150.0-331.5) | 228.0 (140.0-345.0) | 220.0 (156.0-324.5) | 0.908 |
| Risk factors for coronary artery disease | ||||
| BMI (kg/m2) | 26.8 (24.2-29.4) | 26.9 (24.7-30.0) | 26.3 (24.2-29.1) | 0.252 |
| Hypertension | 103 (41.4%) | 31 (45.6%) | 72 (39.8%) | 0.407 |
| Diabetes mellitus | 50 (20.1%) | 16 (23.5%) | 34 (18.8%) | 0.405 |
| Previously known hyperlipidemia | 58 (23.3%) | 14 (20.6%) | 44 (24.3%) | 0.536 |
| Current or ex-smoker | 164 (65.9%) | 44 (64.7%) | 120 (66.3%) | 0.813 |
| Positive family history of IHD | 61 (24.5%) | 61 (24.5%) | 42 (23.2%) | 0.439 |
| Angiographic characteristics | ||||
| IRA: LAD/non-LAD | 121 (48.6%)/128 (51.5%) | 40 (58.8%)/28 (41.2%) | 81 (44.8%)/100 (55.2%) | 0.048 |
| TIMI 0 flow in IRA before PCI | 144 (57.8%) | 45 (66.2%) | 99 (54.7%) | 0.102 |
| TIMI 3 flow in IRA after PCI | 229 (92.0%) | 56 (82.4%) | 173 (95.6%) | 0.0006 |
| Multivessel coronary artery disease | 143 (57.4%) | 41 (60.3%) | 102 (56.4%) | 0.5753 |
| Stent implantation | 245 (98.4%) | 66 (97.1%) | 179 (98.9%) | 0.305 |
| GP IIb/IIIa inhibitor usage | 66 (26.5%) | 28 (41.2%) | 38 (21.2%) | 0.0016 |
| Biochemical characteristics | ||||
| Creatinine on admission (mg/dL) | 0.90 (0.81-1.06) | 0.93 (0.88-1.05) | 0.90 (0.80-1.06) | 0.618 |
| eGFR calculated using the CKD-EPI formula (mL/min/1.73 m2) | 84.4 (74.1-94.5) | 84.4 (74.6-94.6) | 84.7 (73.4-94.5) | 0.869 |
| Glucose on admission (mg/dL) | 138.5 (122.0-169.0) | 140.0 (122.0-170.0) | 136 (120.0-169.0) | 0.376 |
| cTnImax (ng/mL) | 41.2 (11.8-50.0) | 50.0 (20.7-50.0) | 35.7 (10.5-50.0) | 0.012 |
| CK-MBmax (U/L) | 242.0 (116.5-414.0) | 375.5 (162.0-612.0) | 207.0 (97.5-375.0) | 0.0002 |
| Total cholesterol (mg/dL) | 223.0 (195.0-251.0) | 221.5 (196.0-244.0) | 224.0 (195.0-253.0) | 0.582 |
| LDL-C (mg/dL) | 145.0 (125.0-173.0) | 146.5 (123.5-166.0) | 144.5(126.0-176.0) | 0.771 |
| HDL-C (mg/dL) | 52.0 (46.0-59.0) | 53.0 (48.0-61.0) | 51.0(45.0-58.0) | 0.205 |
| Triglycerides (mg/dL) | 82.0 (59.0-128.0) | 85.0 (57.0-130.5) | 82.0(60.0-124.0) | 0.729 |
| BNP on admission (pg/mL) | 53.9 (27.9-106.5) | 51.5 (26.8-102.2) | 55.3(28.6-114.6) | 0.854 |
| BNP at discharge (pg/mL) | 139.8 (74.7-284.2) | 159.5 (82.5-396.4) | 125.9 (70.1-239.4) | 0.021 |
| Medications prescribed at hospital discharge | ||||
| Acetylsalicylic acid | 249 (100.0%) | 68 (100.0%) | 181 (100.0%) | N/A |
| Clopidogrel | 249 (100.0%) | 68 (100.0%) | 181 (100.0%) | N/A |
| Statin | 249 (100.0%) | 68 (100.0%) | 181 (100.0%) | N/A |
| Beta blocker | 247 (99.2%) | 67 (98.5%) | 180 (98.9%) | 0.6772 |
| ACEI or ARB | 249 (100.0%) | 68 (100.0%) | 181 (100.0%) | N/A |
| Aldosterone antagonist | 25 (10.0%) | 8 (11.8%) | 17 (9.4%) | 0.5702 |
| Diuretic | 24 (9.6%) | 9 (13.2%) | 15 (8.3%) | 0.3484 |
| Variable | At Discharge (n = 249) | At 6 Months after Discharge (n = 249) | p-Value |
|---|---|---|---|
| LA (mm) | 40.0 (37.0-43.0) | 40.0 (38.0-44.0) | 0.000006 |
| LVEDd (mm) | 49.0 (45.0-53.0) | 50.0 (46.0-54.0) | <0.000001 |
| LVESd (mm) | 34.0 (30.0-37.0) | 34.0 (31.0-37.0) | 0.038 |
| LVEDV (mL) | 99.4 (84.0-121.0) | 110.0 (94.0-134.0) | <0.000001 |
| LVESV (mL) | 55.0 (45.0-69.0) | 57.0 (48.0-76.0) | <0.000001 |
| LVEF (%) | 44.0 (39.0-48.4) | 46.0 (42.0-51.5) | <0.000001 |
| LVSD (LVEF ≤ 40%) | 84.0 (33.7%) | 52.0 (20.9%) | <0.00001 |
| WMSI (points) | 1.56 (1.38-1.75) | 1.44 (1.31-1.69) | <0.000001 |
| Variable | Overall Study Population (n = 249) | Patients with LVR at 6 Months (n = 68) | Patients without LVR at 6 Months (n = 181) | p-Value * |
|---|---|---|---|---|
| Heart rate (BPM) | 75.0 (62.0-88.0) | 79.0 (64.5-89.0) | 74.0 (62.0-86.0) | 0.197 |
| Anterior location of STEMI | 116 (47.0%) | 38 (55.9%) | 78 (43.1%) | 0.071 |
| Number of leads with ST-segment elevation (n) | 4.0 (3.0-6.0) | 5.0 (3.0-6.0) | 4.0 (3.0-6.0) | 0.019 |
| Sum of ST-segment elevation (mm) | 8.5 (4.0-14.0) | 9.5 (6.3-16.0) | 8.0 (4.0-13.5) | 0.014 |
| Maximal ST-segment elevation (mm) | 3.0 (2.0-4.0) | 3.0 (2.0-5.0) | 3.0 (1.8-4.0) | 0.089 |
| Number of leads with pathological Q waves (n) | 2.0 (1.0-4.0) | 3.0 (1.5-5.0) | 2.0 (1.0-3.0) | 0.004 |
| Presence of reciprocal ST-segment depression ≥1mm | 193 (77.5%) | 50 (73.5%) | 143 (79.0%) | 0.356 |
| QRS duration (ms) | 95.0 (85.0-100.0) | 93.0 (85.0-100.0) | 96.5 (87.5-102.0) | 0.170 |
| Grade of ischemia according to Birnbaum and Sclarovsky | grade 2: 198(79.5%); grade 3: 51(20.5%) | grade 2: 53 (77.9%); grade 3: 15 (22.1%) | grade 2: 145 (80.1%); grade 3: 36 (19.9%) | 0.705 |
| Variable | Beta Coefficient | Beta Coefficient Standard Error | Direction Component Beta | Direction Component Beta Standard Error | p-Value |
|---|---|---|---|---|---|
| Model 1. Characteristics: R = 0.428; R2 = 0.183; corrected R2 = 0.173; p < 0.0001 | |||||
| Intercept | 19.40 | 4.47 | <0.0001 | ||
| IRA: LAD/non-LAD | 0.18 | 0.06 | 6.73 | 2.30 | 0.0037 |
| Flow in IRA after PCI: TIMI 3 vs. TIMI < 3 | −0.23 | 0.06 | −15.91 | 4.09 | 0.0001 |
| Number of leads with pathological Q waves | 0.22 | 0.06 | 1.83 | 0.54 | 0.0007 |
| Model 2. Characteristics: R = 0.404; R2 = 0.163; corrected R2 = 0.153; p < 0.00001 | |||||
| Intercept | −33.42 | 24.45 | 0.1729 | ||
| Height (cm) | 0.13 | 0.06 | 0.32 | 0.14 | 0.0284 |
| Flow in IRA after PCI: TIMI 3 vs. TIMI < 3 | −0.29 | 0.06 | −19.91 | 4.05 | <0.0001 |
| Number of leads with ST-segment elevation | 0.24 | 0.06 | 2.34 | 0.59 | 0.0001 |
| Model 3. Characteristics: R = 0.417; R2 = 0.174; corrected R2 = 0.160; p < 0.00001 | |||||
| Intercept | −26.80 | 24.37 | 0.2725 | ||
| Height (cm) | 0.12 | 0.06 | 0.30 | 0.14 | 0.0366 |
| IRA: LAD/non-LAD | 0.17 | 0.07 | 6.42 | 2.46 | 0.0097 |
| Flow in IRA after PCI: TIMI 3 vs. TIMI < 3 | −0.28 | 0.06 | −19.30 | 4.05 | <0.0001 |
| Sum of ST-segment elevation (for a 1 mm increase) | 0.13 | 0.06 | 0.32 | 0.16 | 0.0422 |
| Model 4. Characteristics: R = 0.484; R2 = 0.235; corrected R2 = 0.220; p < 0.00001 | |||||
| Intercept | −39.04 | 25.90 | 0.1332 | ||
| Height (cm) | 0.14 | 0.06 | 0.34 | 0.15 | 0.0260 |
| Flow in IRA after PCI: TIMI 3 vs. TIMI < 3 | −0.29 | 0.06 | −19.98 | 4.32 | <0.0001 |
| Number of leads with ST-segment elevation | 0.18 | 0.06 | 1.77 | 0.65 | 0.0065 |
| Number of leads with pathological Q waves | 0.20 | 0.07 | 1.74 | 0.58 | 0.0029 |
| Model 5. Characteristics: R = 0.471; R2 = 0.222; corrected R2 = 0.209; p < 0.00001 | |||||
| Intercept | −36.42 | 23.81 | 0.1275 | ||
| Height (cm) | 0.13 | 0.06 | 0.33 | 0.14 | 0.0194 |
| Flow in IRA after PCI: TIMI 3 vs. TIMI < 3 | −0.24 | 0.06 | −16.53 | 3.97 | <0.0001 |
| IRA: LAD/non-LAD | 0.16 | 0.06 | 5.97 | 2.23 | 0.0079 |
| CK-MBmax (for a 100 U/L increase) | 0.27 | 0.06 | 1.94 | 0.43 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasprzak, M.; Fabiszak, T.; Koziński, M.; Kubica, J. Diagnostic Performance of Selected Baseline Electrocardiographic Parameters for Prediction of Left Ventricular Remodeling in Patients with ST-Segment Elevation Myocardial Infarction. J. Clin. Med. 2021, 10, 2405. https://doi.org/10.3390/jcm10112405
Kasprzak M, Fabiszak T, Koziński M, Kubica J. Diagnostic Performance of Selected Baseline Electrocardiographic Parameters for Prediction of Left Ventricular Remodeling in Patients with ST-Segment Elevation Myocardial Infarction. Journal of Clinical Medicine. 2021; 10(11):2405. https://doi.org/10.3390/jcm10112405
Chicago/Turabian StyleKasprzak, Michał, Tomasz Fabiszak, Marek Koziński, and Jacek Kubica. 2021. "Diagnostic Performance of Selected Baseline Electrocardiographic Parameters for Prediction of Left Ventricular Remodeling in Patients with ST-Segment Elevation Myocardial Infarction" Journal of Clinical Medicine 10, no. 11: 2405. https://doi.org/10.3390/jcm10112405