
Characterization of the GHB Withdrawal Syndrome
by
 , , , , , and
, , , , , and
Casper J. H. Wolf
1,2,3,* ,
,
Harmen Beurmanjer
3,4,
Boukje A. G. Dijkstra
3,4,
Alexander C. Geerlings
1,
Marcia Spoelder
2,
Judith R. Homberg
2 and
and
Arnt F. A. Schellekens
1,3 1
Medical Center, Department of Psychiatry, Radboud University, 6525 GA Nijmegen, The Netherlands
2
Department of Cognitive Neuroscience, Donders Institute for Brain Cognition and Behaviour, Radboud University, 6525 EN, Nijmegen, The Netherlands
3
Nijmegen Institute for Scientist-Practitioners in Addiction (NISPA), 6525 HR Nijmegen, The Netherlands
4
Novadic-Kentron Addiction Care, 5261 LX Vught, The Netherlands
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2021, 10(11), 2333; https://doi.org/10.3390/jcm10112333
Submission received: 8 April 2021
/
Revised: 23 May 2021
/
Accepted: 25 May 2021
/
Published: 26 May 2021
(This article belongs to the Section Mental Health)
Abstract
:The gamma-hydroxybutyric acid (GHB) withdrawal syndrome can have a fulminant course, complicated by severe complications such as delirium or seizures. Detoxification by tapering with pharmaceutical GHB is a safe way to manage GHB withdrawal. However, a detailed description of the course of the GHB withdrawal syndrome is currently lacking. This study aimed to (1) describe the course of GHB withdrawal symptoms over time, (2) assess the association between vital signs and withdrawal symptoms, and (3) explore sex differences in GHB withdrawal. In this observational multicenter study, patients with GHB use disorder (n = 285) were tapered off with pharmaceutical GHB. The most reported subjective withdrawal symptoms (SWS) were related to cravings, fatigue, insomnia, sweating and feeling gloomy. The most prevalent objective withdrawal symptoms (OWS) were related to cravings, fatigue, tremors, sweating, and sudden cold/warm feelings. No association between vital signs and SWS/OWS was found. Sex differences were observed in the severity and prevalence of specific withdrawal symptoms. Our results suggest that the GHB withdrawal syndrome under pharmaceutical GHB tapering does not strongly differ from withdrawal syndromes of other sedative drugs. The lack of association between vital signs and other withdrawal symptoms, and the relative stability of vitals over time suggest that vitals are not suitable for withdrawal monitoring. The reported sex differences highlight the importance of a personalized approach in GHB detoxification.
1. Introduction
The repeated use of the recreational drug γ-hydroxybutyric acid (GHB) can lead to GHB use disorder (GUD) [1,2]. Similar to other substance use disorders (SUDs), GUD is characterized by a loss of control over GHB intake and physical dependence on GHB [3]. In 2019, the prevalence of GHB use in European countries varied from 0.1% in adults (16–64 year old) to 1.7% among young adults (16–34 year old) [2]. Although GUD has a relatively low prevalence compared to other SUDs, its societal and financial impact are disproportionally high. GHB use is involved in ~12% of drug-related emergency care cases in Europe, caused by accidental overdosing or severe withdrawal symptoms upon sudden abstinence [2,4].
Due to the rapid onset of action (Tmax = 25–40 min) and the short half-life (T½ = 30–60 min) of GHB, patients with GUD typically consume GHB every 2–3 h to prevent withdrawal symptoms [5,6]. Cessation of GHB use results in a severe withdrawal syndrome, characterized by an erratic and fulminant course. Reported symptoms of GHB withdrawal are tremors, agitation, anxiety, hallucinations, psychoses and delirium [6,7]. Abrupt GHB withdrawal without adequate treatment leads to delirium in over 50% of cases [7].
Treatment of GHB withdrawal during detoxification aims to reduce the severity of withdrawal symptoms. Two commonly used methods for GHB detoxification are benzodiazepine tapering and the more extensively studied pharmaceutical GHB tapering. Benzodiazepine administration increases GABAergic signaling through the GABAA receptor, and requires dose regimens of up to six times per day [8,9]. In contrast, pharmaceutical GHB activates both the GABAB and GHB receptor, and is administered to the patient every two to three hours [10].
Some studies suggest that pharmaceutical GHB tapering is a safer method for detoxification compared to benzodiazepines [6,8]. This might be related to the complex pharmacological profile of GHB. Studies have shown that low doses of GHB primarily affect the metabotropic GHB receptor, causing an increase in glutamatergic signaling and a decrease in GABAergic signaling [11,12]. In contrast, high doses of GHB also activate the GABAB receptor, decreasing glutamatergic signaling and increasing GABAergic signaling [13,14]. Benzodiazepines, acting at GABAA receptors, might therefore not sufficiently suppress GABAB-mediated GHB withdrawal, leading to an increased risk for adverse events during benzodiazepine detoxification, such as delirium [8].
Despite the existing evidence for the safety of pharmaceutical GHB tapering, several important issues regarding this approach remain to be elucidated [6,15]. For instance, little is known about the development of individual withdrawal symptoms over time during GHB detoxification. Additionally, some suggest to base the speed of tapering on the monitoring of vital signs, such as blood pressure and heart rate [16,17,18], whereas others propagate the monitoring of (subjective) withdrawal symptoms [15,19]. Understanding the development of individual withdrawal symptoms over time, and their relationship with vital signs, could facilitate the effective dosing and monitoring of the detoxification process.
The GUD population is characterized by a substantial proportion of women of about one third [6,20]. Women with SUDs are known to show higher rates of internalizing psychiatric symptoms, such as depression and anxiety, whereas men with SUDs show higher rates of externalizing symptoms, such as antisocial personality [21,22,23]. It has been shown that women with GUD experience stronger withdrawal compared to men with GUD [6]. However, detailed information on the exact nature of these sex differences is lacking.
The aim of the current study is to further our understanding of the GHB withdrawal syndrome, in order to improve medical treatment of this condition. We characterize the course of the GHB withdrawal syndrome during inpatient pharmaceutical GHB detoxification in a large database of clinical observations in patients with GUD. Specifically, we analyze: 1. the course of individual withdrawal symptoms over time, 2. the association between vital signs and subjective withdrawal symptoms, and 3. sex differences in the course of the GHB withdrawal syndrome.
2. Materials and Methods
2.1. Study Design
We used data from two large observational multicenter studies in patients with GUD. The main focus of these studies was to assess the safety of detoxification with pharmaceutical GHB, as published elsewhere [6,24]. Both studies had similar inclusion criteria, treatment paradigms, and outcome measures. The Medical Ethical Research Committee Twente and Central Committee on Research Involving Human Subjects approved the study protocols and considered that the study did not fall under the scope of the Medical Research Involving Human Subjects Act (WMO). The off-label use of pharmaceutical GHB for GHB detoxification was approved by the Dutch Health Care Inspection.
2.2. Participants
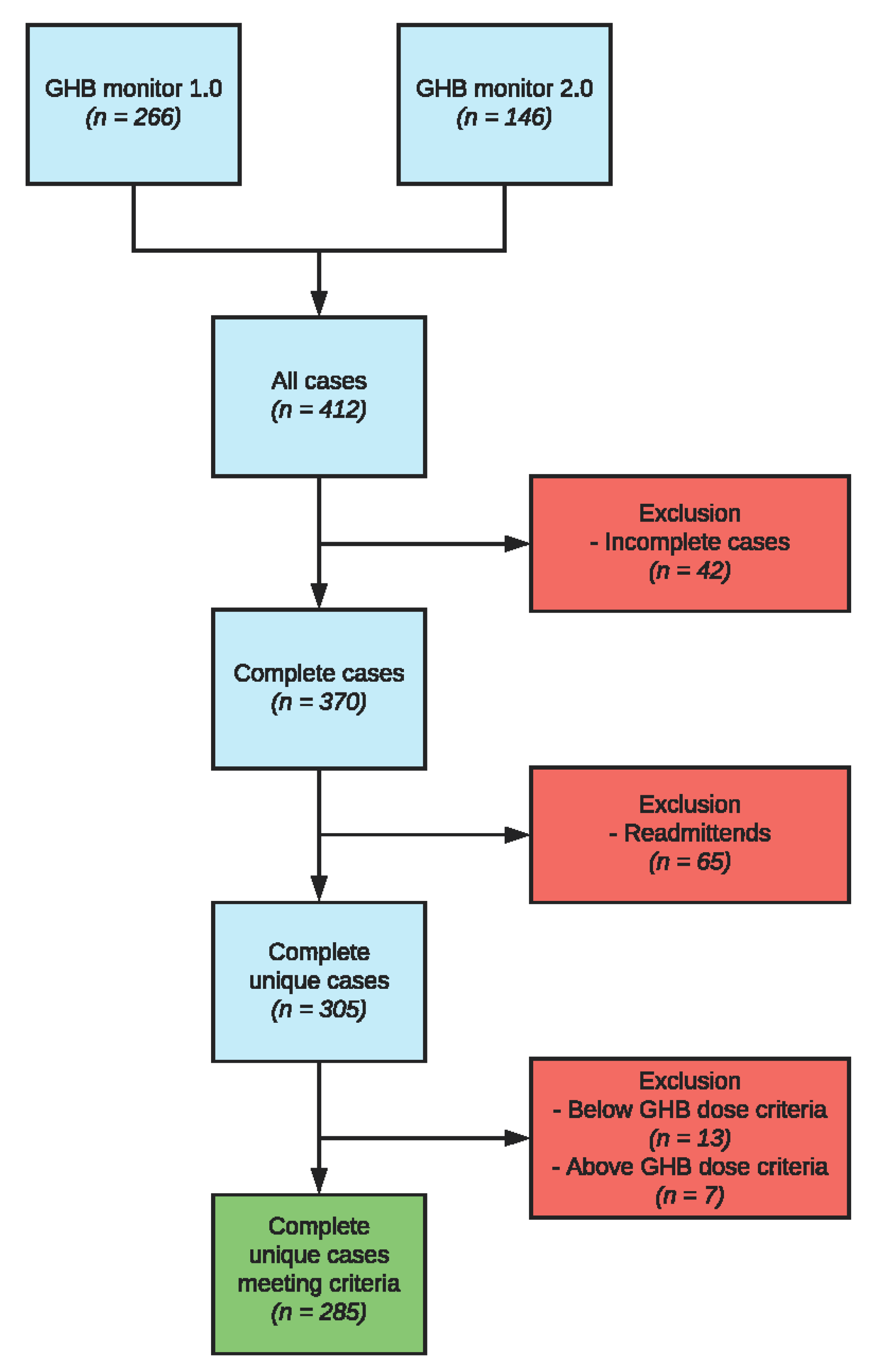
Inpatients being treated for GUD (n = 412) at one of the seven participating addiction treatment centers in the Netherlands (Novadic-Kentron, Tactus, IrisZorg, Victas, Verslavingszorg Noord-Nederland, Brijder and Mondriaan GGZ) were included between 2011 and 2015. Patients were between 18 and 60 years old. All patients were classified with GHB dependence according to the Diagnostic and Statistical Manual of Mental Disorders IV-TR [25] general criteria for psychoactive substance dependence. Patients were excluded from the study if they could not speak or read the Dutch language, if they suffered from a severe co-morbid psychiatric condition that required immediate attention (e.g., psychosis, manic episodes, or suicidal ideation), or in the case of pregnancy [6]. Patients were excluded from data analyses if they had less than three tapering days, or if their GHB dose before admission was below 30 milliliters (since these patients should have been treated ambulatory) or above 240 milliliters (since these patients showed an aberrant, non-representative GHB withdrawal syndrome under pharmaceutical GHB tapering). The threshold of >240 mL was determined by adding 2.5 SDs to the daily average consumption volume. If patients were included in both monitors, data of the first treatment episode were used. This resulted in a database of 285 complete, unique patients with GUD undergoing inpatient GHB detoxification (Figure 1).
2.3. Instruments
Demographics and other clinical data were obtained from chart reviews (admission data, discharge data and the discharge summary). Measurements in the Addictions for Triage and Evaluation (MATE) Section 1 was used to assess current substance use (past 30 days), lifetime substance use, and the classification of substance dependence according to DSM-IV [26]. In Dutch addiction treatment centers, the MATE is the standard clinical assessment tool, and has proven to have good psychometric quality [26]. The GHB questionnaire, specifically assessing the pattern of previous GHB use, was used in addition to the MATE [6]. The GHB questionnaire consists of 23 parameters, including total years of use, daily dose, volume per dose and time interval between doses. The questionnaire is commonly used in Dutch addiction treatment centers that treat patients with GUD.
2.3.1. Subjective Withdrawal Scale
The subjective withdrawal scale consists of 33 items representing individual withdrawal symptoms. Patients indicate to what degree they experience each symptom on a 5-point Likert scale (0 = not at all, 1 = a little, 2 = moderately, 3 = quite a bit, 4 = extremely). The subjective withdrawal scale is based on the format of the Subjective Opiate Withdrawal Scale [27], extended with subjective withdrawal symptoms of other psychoactive substances as described in the DSM-IV-TR [25]. Its Dutch translation has good psychometric properties in opioid-dependent inpatients [28].
2.3.2. Objective Withdrawal Scale
The objective withdrawal scale consists of 34 observable signs of withdrawal. It is composed of symptoms included in the Objective Opiate Withdrawal Scale [27] and objective withdrawal symptoms of other psychoactive substances as described in the DSM-IV-TR [25]. The objective withdrawal scale is filled in by health professionals (mostly nursing staff), where symptoms are classified as present (1) or absent (0). The objective and subjective withdrawal scale have been reported in several previous studies assessing GHB withdrawal [6,8], and are the standard GHB withdrawal assessment scales in addiction treatment centers in the Netherlands. As a result, clinical staff are experienced with applying these instruments in their daily routine. Furthermore, prior to the data collection of both samples, all nursing staff received instructions and training in how to handle the withdrawal scales.
2.3.3. Vitals
Vital signs (heart rate, systolic- and diastolic blood pressure) were measured by the nursing staff. Vitals were annotated under the objective withdrawal scale.
2.4. Procedure
Upon admission to the addiction treatment center, information on GHB use and GUD was acquired by trained study nurses through the above-mentioned questionnaires. The detoxification procedure consisted of three phases: titration, tapering, and recovery. During the titration phase, patients were treated with pharmaceutical GHB that was 70% of the reported self-administered illicit GHB dose (based on an average ‘street’ concentration of 650 mg/mL). The GHB dose was increased in the case of withdrawal and decreased in the case of sedation, until the pharmaceutical GHB dose was found on which patients were stable and experienced neither withdrawal nor sedation. This usually took between one and two days, after which, the tapering phase started. During the tapering phase, the GHB dose was lowered by 300 mg of the GHB per dose per day. The interval between doses was usually two to three hours. Symptoms were assessed 30 min prior to each GHB dose. The tapering phase lasted 11 days on average. The recovery phase started when the pharmaceutical GHB was tapered to 0, which lasted six days on average. For a more detailed description of the protocol, see Dijkstra et al. (2017) [6].
2.5. Data Analysis
Demographics were summarized using descriptive statistics and compared between men and women using one-way MANOVAs (GHB use characteristics (including age, age at first GHB use, mean years of GHB use, mean days of GHB use, mean daily GHB dose, mean interval between two GHB doses) and co-morbid substance use) and Pearson chi-square test (medication).
To describe the general course of GHB withdrawal, we examined the first 11 days of tapering, since the average tapering period lasted 10.3 days. Linear mixed model analysis was performed to assess the development of total SWS/OWS scores over time. Mean daily SWS/OWS scores were used as dependent variables.
We visualized symptom severity and prevalence using heat maps. The average relative symptom severity and prevalence were calculated by dividing the average symptom score on the respective scale by the maximum possible score on that scale. To examine the development of individual withdrawal symptoms over time, we performed descriptive statistics. Pearson correlation analysis was performed to assess the association of individual withdrawal symptoms between both scales. Bonferroni corrections were applied to correct for multiple comparisons.
Linear mixed model analysis was performed to assess the development of vital signs over time. The mean daily scores of the vital parameters were used as dependent variables. Pearson correlation analysis was performed to assess the association of vital signs with daily average SWS/OWS scores. Bonferroni corrections were applied to correct for multiple comparisons.
Finally, to explore sex differences in the course of withdrawal symptoms over time, we performed linear mixed model analysis. Daily average SWS and OWS scores were used as the dependent variables, and sex was used as an independent variable. Sex differences in the severity and prevalence of individual withdrawal symptoms were analyzed using one-way MANOVA, using average scores per patient per symptom across the entire tapering period.
ANOVAs, chi-square tests, correlations, heat map analyses and linear mixed model analyses were carried out with the Statistical Package for the Social Sciences (SPSS) (25.0) and with GraphPad Prism (9.0). Significance was set at p < 0.05.
3. Results
3.1. Demographics
Demographic characteristics of participants (n = 285) are presented in Table 1. Men and women differed in GHB-related characteristics (Table 1: one-way MANOVA, F(6,174) = 2.227, p < 0.05; Wilk’s λ = 0.929). Men included in the analysis were older and started using GHB at a later age compared to women (Table 1: age (F(1,179) = 8.978, p < 0.01); age at first GHB use (F(1,179) = 6.797, p < 0.01)). Men and women did not differ in rates of co-morbid substance use or in the prevalence of medication use.
3.2. Development of Withdrawal Symptoms over Time during GHB Detoxification
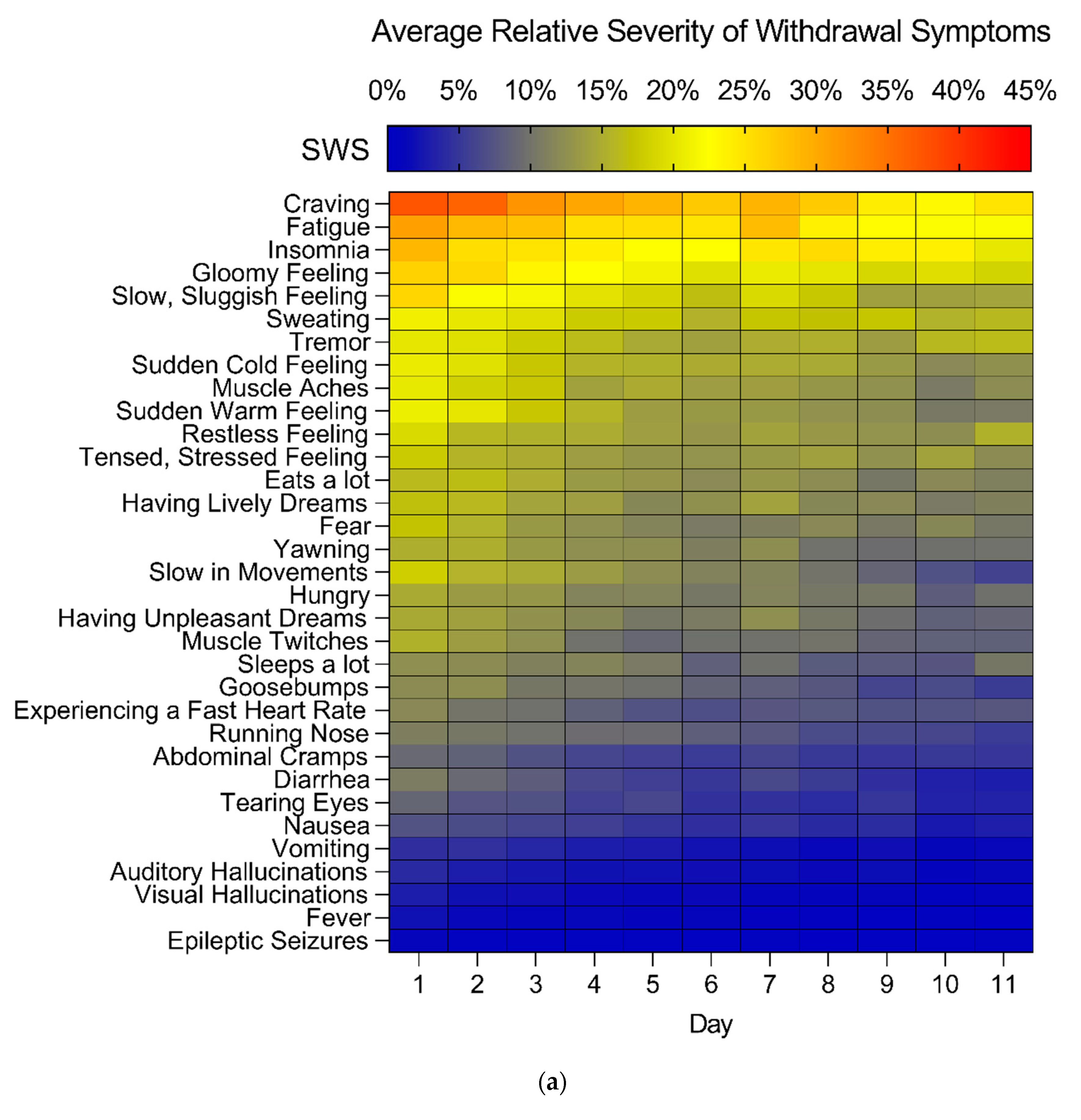
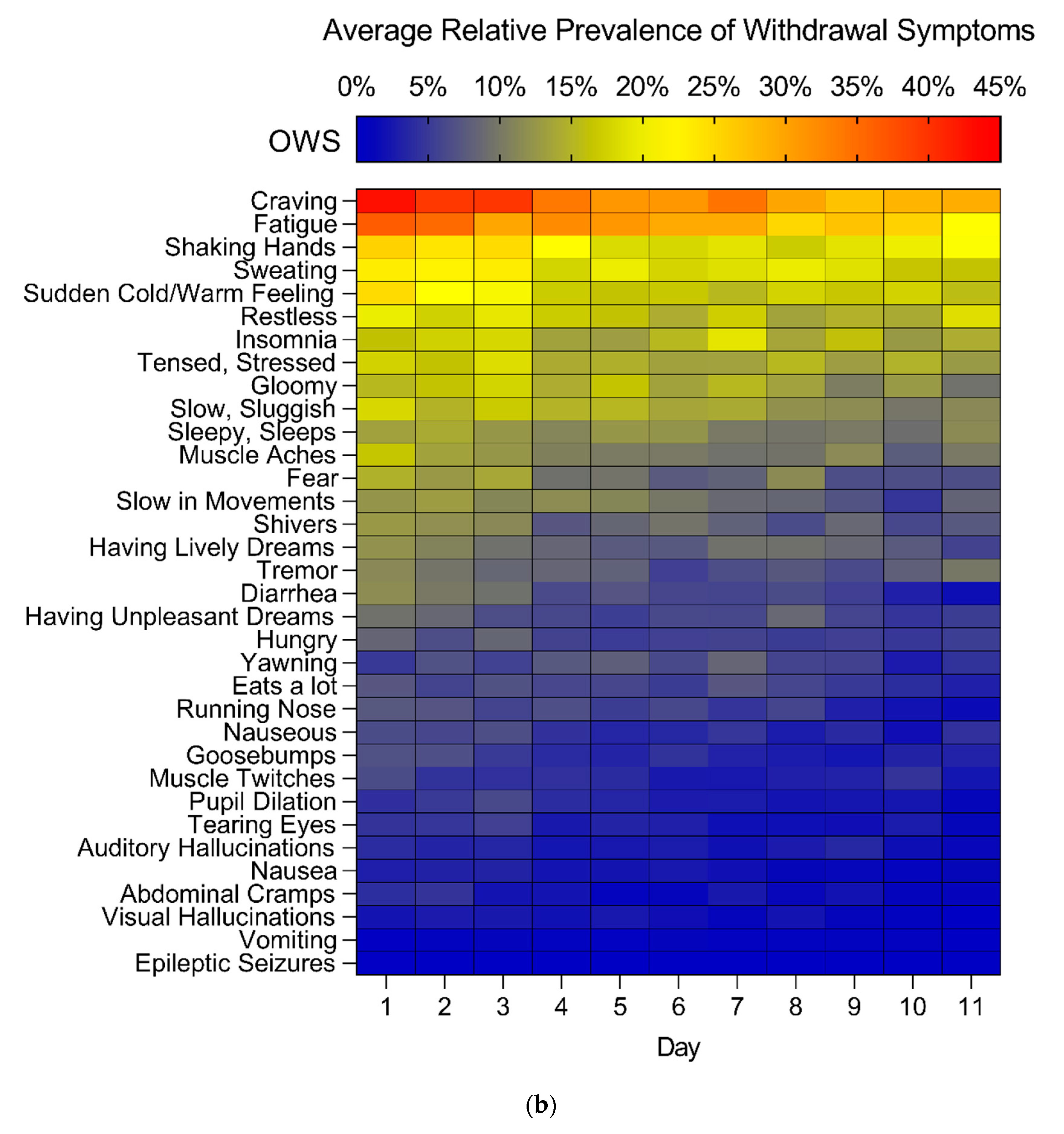
The total SWS and OWS scores gradually decreased across the tapering phase (linear mixed models, SWS: main effect of time, F(10,198) = 12.185, p < 0.0001; OWS, main effect of time, F(10,209) = 9.639, p < 0.0001). The most severely experienced SWS were “craving”, “fatigue”, “insomnia” and a “gloomy” and “slow, sluggish feeling” (Figure 2). The most often reported OWS by nurses were “craving” and “fatigue”, next to the symptoms “shaking hands”, “sweating” and a “sudden cold/warm feeling” (Figure 2).
The SWS “muscle aches”, “muscle twitches”, “tensed, stressed feeling”, “experiencing a fast heart rate” and “abdominal cramps” were most severe in the first part of detoxification (first three days). Over the first four days, a >70% decrease in severity was reported for these symptoms. In contrast, several SWS (“sweating”, “tremor”, “sleeps a lot”, and “restless feeling”) remained stable over time (<25% decrease in severity over 11 days). On average, there were no SWS that became more severe during the tapering phase.
The OWS “sweating”, “sudden cold/warm feeling”, “muscle aches”, “tensed, stressed feeling”, “shivers”, “having unpleasant dreams”, “hungry”, and “goosebumps” were primarily present in the first part of detoxification (first 3 days). Over the first four days, a >70% decrease in prevalence was observed for these symptoms. The OWS “tremor”, “shaking hands”, “sleepy, sleeps”, “insomnia”, “restless” and “yawning” were consistently present over time (<25% decrease in presence over 11 days). The OWS “yawning”, “insomnia”, “gloomy” and “visual hallucinations” were on some days more prevalent compared to day 1. The majority of SWS and OWS that appeared on both scales showed a moderate to strong correlation with the corresponding symptom on the other scale (r = 0.226 to 0.826, p < 0.0015 after Bonferroni correction) (Table A1).
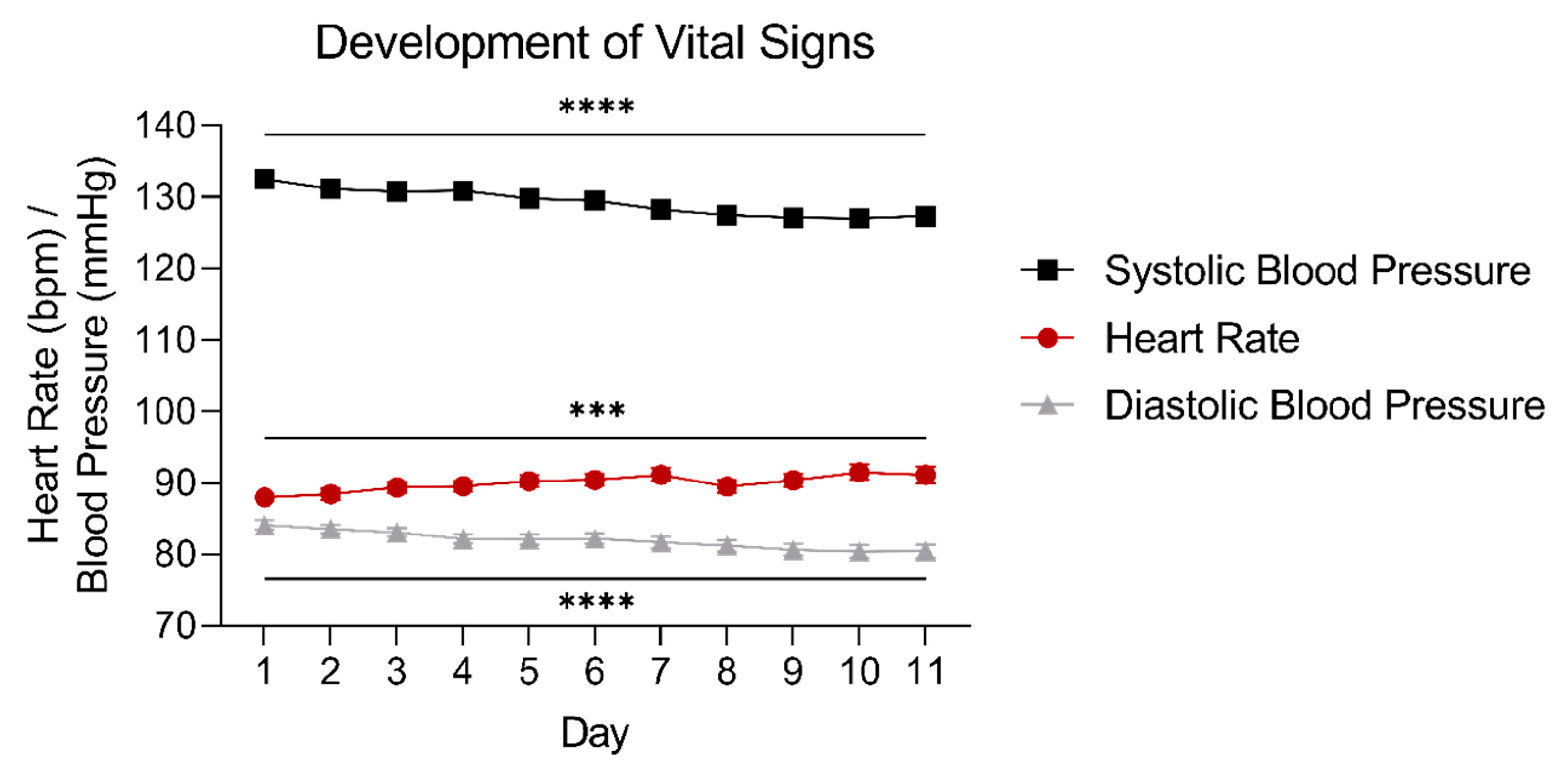
The average heart rate gradually increased over time during detoxification from 87.9 to 91.1 bpm (linear mixed models, heart rate: main effect of time: F(10,192) = 3.509, p < 0.001). The average systolic and diastolic blood pressure gradually decreased over time from 132.5 to 127.3 mmHg, and from 84.1 to 80.4 mmHg, respectively (linear mixed models, systolic blood pressure main effect of time: F(10,196) = 5.848, p < 0.0001; diastolic blood pressure main effect of time: F(10,183) = 10.095, p < 0.0001), as shown in Figure 3.
3.3. Association between Vital Signs and Subjective- and Objective Symptoms of GHB Withdrawal
3.4. Differences in GHB Withdrawal Syndrome between Men and Women
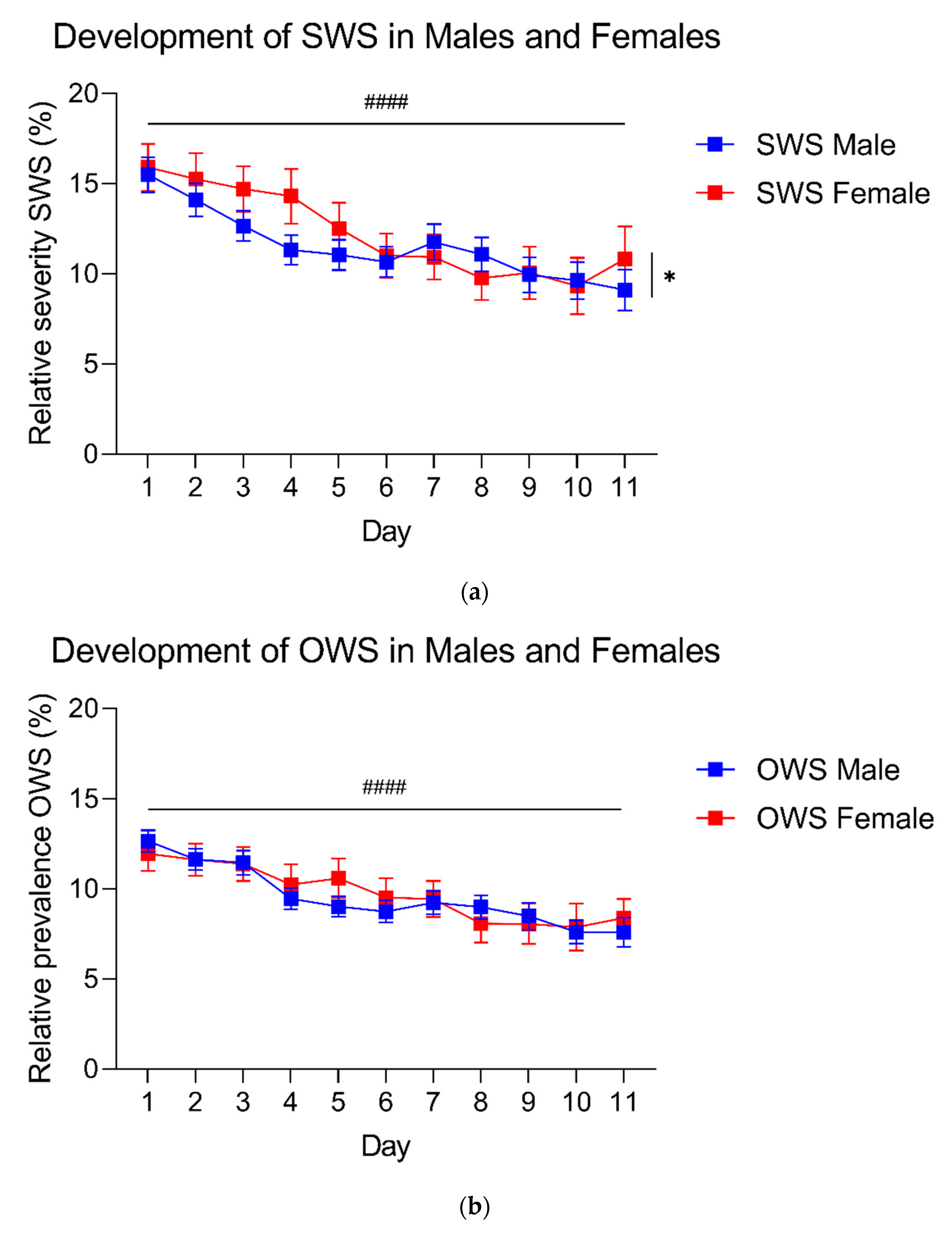
In contrast to what we expected, there was no difference in total SWS and OWS scores between men and women across the tapering phase (Figure 4: linear mixed models, no effect of sex), and both sexes showed a similar decrease in total OWS score over time (Figure 4: linear mixed models, OWS no significant interaction). Men and women showed a slightly different course of total SWS score over time (Figure 4: linear mixed models, SWS time x sex interaction, F(10,198) = 2.038, p < 0.05).
One-way MANOVA showed that men and women differed in the severity of individual SWS (F(33,233) = 2550, p < 0.001; Wilk’s λ = 0.735). Specifically, women scored higher on fear (F(1,265) = 4.531, p < 0.05), gloomy feeling (F(1,265) = 7.507, p < 0.01), yawning (F(1,265) = 6.132, p < 0.05), goosebumps (F(1,265) = 6.272, p < 0.05), sweating (F(1,265) = 7.583, p < 0.01), tearing eyes (F(1,265) = 6.863, p < 0.01), muscle aches (F(1,265) = 9.357, p < 0.01), nausea (F(1,265) = 4.700, p < 0.05), craving (F(1,265) = 7.519, p < 0.01), sudden cold feelings (F(1,265) = 13.248, p < 0.001), and sudden warm feelings (F(1,265) = 7.979, p < 0.01), whereas men were more often reported to eat a lot during detoxification compared to women (F(1,265) = 14.059, p < 0.001), see Figure 2).
One-way MANOVA showed that men and women differed in prevalence of individual OWS (F(34,234) = 2.004, p < 0.01; Wilk’s λ = 0.774). Women showed more shivering (F(1,267) = 16.046, p < 0.0001), sudden cold/warm feelings (F(1,267) = 5.664, p < 0.05, abdominal cramps (F(1,267) = 6.665, p < 0.05), nausea (F(1,267) = 10.103, p < 0.01) and vomiting (F(1,267) = 4.492, p < 0.05), while men showed more insomnia (F(1,267) = 5.024, p < 0.05) and eating a lot (F(1,267) = 7.382, p < 0.01). Additionally, men showed a higher blood pressure than women (Figure A1).
4. Discussion
This study set out to analyze the course of the GHB withdrawal syndrome in patients with GUD during inpatient detoxification with pharmaceutical GHB. The GHB withdrawal syndrome was primarily characterized by sleep-related symptoms, mood-related symptoms and several physiological symptoms, including sweating and tremors. The majority of symptoms steadily declined in severity over time, while some symptoms (e.g., tremors, sleeping a lot) were not strongly affected by GHB tapering. Vital signs did not correlate with other withdrawal symptoms. Women showed a different pattern of withdrawal symptoms compared to men.
The most prominent withdrawal symptoms that decreased over time include “craving”, “fatigue”, “insomnia”, “gloomy”, “slow, sluggish”, “sudden cold/warm feeling”, “muscle aches” and “tensed, stressed”, and might represent the core symptoms of GHB withdrawal. Other withdrawal symptoms that were frequently present during detoxification include “sweating”, “tremor” and “restlessness”. Withdrawal syndromes of other sedatives, such as alcohol and benzodiazepine withdrawal, show overlap with symptoms seen in this study, such as anxiety/fear, tremor, sweating, insomnia (alcohol/benzodiazepines), restlessness and muscle twitches (benzodiazepines) [29,30]. Other characteristic alcohol withdrawal symptoms such as hypertension, tachycardia, and fever were hardly seen in our sample [31,32]. Similarly, severe GHB withdrawal symptoms such as epileptic seizures, hallucinations and delirium, were rare in our sample, probably because GHB tapering dampened the overall severity of withdrawal symptoms. Future studies should address whether other withdrawal scales, for instance the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) tool, can also reliably be used to guide tapering [33]. Indeed, the CIWA-Ar has also been used to assess GHB withdrawal in two case reports [34,35].
Several symptoms present at the start of detoxification were not strongly affected by GHB tapering (“sweating”, “tremor”, “sleeps a lot”, ”sleepy”, “sleeps”, “restless feeling”, ”restless”, “yawning” and “shaking hands”). This may reflect a more long-term dysregulation of autonomic processes, for instance, due to a chronically disrupted sleep pattern. Several of these symptoms were also still present upon discharge of GHB detoxification treatment, including “craving” and “insomnia”. The presence of several symptoms following detoxification, including sleep-related disturbances, might also contribute to the high relapse rates seen with GUD, which is also observed with other SUDs such as alcohol, cocaine and opioid use disorder [36]. Aftercare following detoxification should therefore aim at reducing these symptoms that persist after detoxification, such as sleep-related issues and cravings.
Contrary to other substance withdrawal syndromes, we did not find an association between vital signs and objective or subjective GHB withdrawal symptoms [37,38]. In several other substance withdrawal syndromes, vitals are associated with withdrawal symptom severity and are therefore used as an indicator for overall withdrawal severity. For instance, in alcohol, vital signs are used to determine titration and tapering regimes during detoxification [3,38,39,40]. Our findings suggest that changes in vital signs during GHB detoxification may not be suitable for the monitoring of GHB withdrawal severity.
Additionally, both the increase in heart rate (from 87.9 to 91.1 bpm on average) and the decreases in systolic and diastolic blood pressure (from 132.5/84.1 to 127.3/80.4 mmHg on average) we observed here were rather small and of little clinical relevance, despite being statistically significant. Yet, with sudden GHB withdrawal, tachycardia and hypertension are often observed [7]. Our results indicate that GHB tapering might have prevented a derailment of vital signs, implicating that a change in withdrawal symptoms may precede a derailment of vital signs during GHB detoxification, as also suggested by Beurmanjer et al. (2020) [8].
Men and women showed different types of withdrawal symptoms. Specifically, women scored higher on average on a large variety of (mainly subjective) individual withdrawal symptoms. This is also observed with other SUDs such as opioids, cannabis and nicotine [41,42,43]. The differences in GHB withdrawal symptoms between males and females may be partially related to differences in co-occurring psychiatric conditions. Dijkstra et al. (2017) showed that patients with GUD with higher baseline levels of depression, anxiety and stress experienced higher levels of subjective withdrawal [6]. In addition, co-morbid mood and anxiety disorders are more common in women with SUDs compared to men with SUDs [21,22,23], possibly explaining the increased severity of several individual withdrawal symptoms in women during GHB detoxification compared to men. In contrast to the findings of Dijkstra et al. (2017), we did not find a difference in total SWS severity between men and women across the tapering phase [6]. This may be explained by the fact that Dijkstra et al. (2017) included the titration-, tapering- and recovery days, whereas we only focused on the tapering phase. The limited suppression of (co-morbid) symptoms during titration and recovery days might account for the observed differences. The reported differences between men and women suggest that women might benefit from more gradual tapering strategies compared to men.
In the assessment of GHB withdrawal severity, both objective and subjective symptoms were measured. There is a large overlap between the objective and subjective withdrawal scales regarding the type of symptoms assessed. It can be questioned whether both scales are required to obtain a complete picture of withdrawal severity. The current data show that subjective withdrawal severity generally parallels clinical observations by nursing staff, as also seen with, e.g., opioid withdrawal [28]. However, the subjective withdrawal scale seems more sensitive to a change in withdrawal severity, probably as a result of the 5-point Likert scale design compared to the dichotomous objective withdrawal scale. It might thus be sufficient to focus on self-reported withdrawal severity to monitor GHB detoxification.
The current findings should be viewed in light of several study limitations. A relatively high proportion of patients in our study showed co-morbid substance use (Table 1), possibly contributing to the observed withdrawal symptoms. However, the observed prevalence of co-morbid substance use is representative for the population of patients with GUD [44]. On the one hand, the high rates of co-morbid substance use hamper firm conclusions about the specific effects of GHB withdrawal. On the other hand, clinical reality is that people with GUD often have co-morbid SUDs, thus making our observations clinically relevant [44].
The withdrawal scales used in this study were originally based on opioid withdrawal scales [27], and complemented with other symptoms based on the DSM-IV [25]. Although a total of 38 individual withdrawal signs and symptoms were assessed, it is still possible that withdrawal symptoms that are unique for GHB withdrawal were not assessed with the current withdrawal scales. Throughout detoxification, patients repeatedly mentioned that they had an itchy feeling. This symptom may be considered to be included in the GHB withdrawal scale.
During GHB detoxification, pharmacological treatment for co-morbid psychiatric disorders, such as benzodiazepines, selective serotonin reuptake inhibitors (SSRIs) or anti-psychotics, continued. We speculate this may have dampened the severity of GHB withdrawal, possibly causing our results to be an underestimation of the severity of GHB withdrawal compared to when only pharmaceutical GHB is provided, as also suggested in previous reports [9,45]. The effects of other medications on the course of the GHB withdrawal syndrome requires further study.
It is also important to note that the current findings do not generalize to other methods for GHB detoxification, such as benzodiazepine tapering (different receptor systems), or acute unassisted GHB detoxification (cold turkey). Severe withdrawal symptoms, such as epileptic seizures and psychotic symptoms that were hardly observed here, might be more common in such cases [7,8].
5. Conclusions
The GHB withdrawal syndrome during pharmaceutical GHB tapering is characterized by a variety of symptoms that fade over time, and which are also commonly observed during alcohol and benzodiazepine withdrawal. The observed lack of association between vitals and subjective or objective withdrawal symptoms, and the limited variation of vitals over time, question their relevance as an indicator for GHB withdrawal severity during detoxification. Finally, women experience qualitatively different GHB withdrawal symptoms during GHB detoxification compared to men. Our research suggests that the subjective withdrawal scale may serve as a basis to personalize tapering speed in order to minimize withdrawal severity, and account for sex differences in the GHB withdrawal syndrome.
Author Contributions
Conceptualization, B.A.G.D. and A.F.A.S.; data curation, C.J.H.W., H.B. and A.C.G.; formal analysis, C.J.H.W. and H.B.; funding acquisition, H.B., B.A.G.D. and A.F.A.S.; investigation, H.B. and B.A.G.D.; methodology, H.B. and B.A.G.D.; project administration, J.R.H. and A.F.A.S.; resources, B.A.G.D., J.R.H. and A.F.A.S.; supervision, J.R.H. and A.F.A.S.; visualization, C.J.H.W.; writing—original draft, C.J.H.W.; writing—review and editing, H.B., B.A.G.D., A.C.G., M.S., J.R.H. and A.F.A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Netherlands Ministry of Health, Welfare and Sports (VWS), grant number 316997, within the framework of the national program of the Dutch Association of Mental Health and Addiction Care: ‘Scoring results’.
Institutional Review Board Statement
Ethical review and approval were waived for this study, since the Medical Ethical Research Committee Twente and Central Committee on Research Involving Human Subjects considered that the study did not fall under the scope of the Medical Research Involving Human Subjects Act (WMO).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank the participating addiction treatment centers, as well as all of the individuals who assisted in this study. In particular, we thank the study nurses and patients for their effort and willingness.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Appendix A
Figure A1.
Development of vital signs over time in males and females during the first 11 days of GHB tapering. Data presented as mean ± SEM. Error bars are not shown if they are shorter than the size of the symbol. # = main effect of sex, p < 0.05; ### = main effect of time, p < 0.001; #### = main effect of time/sex, p < 0.0001; * = time × sex interaction, p < 0.05.
Figure A1.
Development of vital signs over time in males and females during the first 11 days of GHB tapering. Data presented as mean ± SEM. Error bars are not shown if they are shorter than the size of the symbol. # = main effect of sex, p < 0.05; ### = main effect of time, p < 0.001; #### = main effect of time/sex, p < 0.0001; * = time × sex interaction, p < 0.05.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
Correlation between similar withdrawal symptoms measured with both the subjective- and objective withdrawal scale.
Table A1.
Correlation between similar withdrawal symptoms measured with both the subjective- and objective withdrawal scale.
| SWS | OWS | Pearson’s r |
|---|---|---|
| Craving | Craving | 0.602 *** |
| Fatigue | Fatigue | 0.488 *** |
| Insomnia | Insomnia | 0.479 *** |
| Gloomy feeling | Gloomy | 0.532 *** |
| Slow, sluggish feeling | Slow, sluggish | 0.403 *** |
| Sweating | Sweating | 0.534 *** |
| Tremor | Tremor/shaking hands | 0.313 ***/0.409 *** |
| Sudden cold feeling | Sudden cold/warm feeling | 0.533 *** |
| Muscle aches | Muscle aches | 0.629 *** |
| Sudden warm feeling | Sudden cold/warm feeling | 0.528 *** |
| Restless feeling | Restless | 0.443 *** |
| Tensed, stressed feeling | Tensed, stressed | 0.511 *** |
| Having lively dreams | Having lively dreams | 0.679 *** |
| Eats a lot | Eats a lot | 0.512 *** |
| Fear | Fear | 0.660 *** |
| Yawning | Yawning | 0.318 *** |
| Slow in movements | Slow in movements | 0.403 *** |
| Having unpleasant dreams | Having unpleasant dreams | 0.687 *** |
| Hungry | Hungry | 0.470 *** |
| Muscle twitches | Muscle twitches | 0.516 *** |
| Sleeps a lot | Sleepy/sleeps | 0.399 *** |
| Goosebumps | Goosebumps | 0.370 *** |
| Experience a fast heart rate | Heart rate (vital sign) | 0.370 *** |
| Running nose | Running nose | 0.461 *** |
| Abdominal cramps | Abdominal cramps | 0.564 *** |
| Diarrhea | Diarrhea | 0.800 *** |
| Tearing eyes | Tearing eyes | 0.162 NS |
| Nausea | Nausea/Nauseous | 0.479 ***/0.657 *** |
| Vomiting | Vomiting | 0.226 ** |
| Auditory hallucinations | Auditory hallucinations | 0.826 *** |
| Visual hallucinations | Visual hallucinations | 0.725 *** |
| Epileptic seizures | Epileptic seizures | −0.017 NS |
| Fever | ||
| Shivers | ||
| Pupil dilation |
Correlation is significant if p < 0.0015 (Bonferroni correction, 2-tailed). ** = p < 0.001; *** = p < 0.0001; NS = non-significant.
Table A2.
Daily average subjective withdrawal symptoms correlated with vitals.
| Heart Rate | Systolic Blood Pressure | Diastolic Blood Pressure | N | |
|---|---|---|---|---|
| Tapering day 1 | 0.164 | −0.035 | 0.003 | 242 |
| Tapering day 2 | 0.137 | −0.078 | 0.038 | 234 |
| Tapering day 3 | 0.159 | −0.170 | −0.023 | 239 |
| Tapering day 4 | 0.103 | −0.137 | 0.011 | 219 |
| Tapering day 5 | 0.173 | −0.089 | −0.013 | 213 |
| Tapering day 6 | 0.159 | −0.094 | 0.016 | 203 |
| Tapering day 7 | 0.127 | −0.093 | 0.002 | 169 |
| Tapering day 8 | 0.190 | −0.006 | 0.051 | 152 |
| Tapering day 9 | 0.193 | −0.107 | 0.100 | 138 |
| Tapering day 10 | 0.071 | −0.053 | 0.007 | 116 |
| Tapering day 11 | 0.167 | −0.036 | 0.171 | 98 |
Shown values are Pearson r.
Table A3.
Daily average objective withdrawal symptoms correlated with vitals.
| Heart Rate | Systolic Blood Pressure | Diastolic Blood Pressure | N | |
|---|---|---|---|---|
| Tapering day 1 | 0.141 | −0.021 | 0.046 | 263 |
| Tapering day 2 | 0.133 | −0.079 | 0.030 | 254 |
| Tapering day 3 | 0.123 | −0.005 | 0.086 | 255 |
| Tapering day 4 | 0.050 | −0.101 | 0.039 | 241 |
| Tapering day 5 | 0.155 | −0.081 | 0.033 | 233 |
| Tapering day 6 | 0.055 | −0.078 | 0.018 | 219 |
| Tapering day 7 | 0.065 | −0.091 | 0.037 | 185 |
| Tapering day 8 | 0.114 | 0.047 | 0.134 | 168 |
| Tapering day 9 | 0.172 | −0.063 | 0.036 | 150 |
| Tapering day 10 | −0.040 | −0.021 | 0.078 | 128 |
| Tapering day 11 | 0.063 | −0.043 | 0.157 | 108 |
Shown values are Pearson r.
References
- Arunogiri, S.; Moayeri, F.; Crossin, R.; Killian, J.J.; Smith, K.; Scott, D.; Lubman, D.I. Trends in gamma-hydroxybutyrate-related harms based on ambulance attendances from 2012 to 2018 in Victoria, Australia. Addiction 2020, 115, 473–479. [Google Scholar] [CrossRef]
- EMCDDA. European Drug Report 2019: Trends and Developments; European Monitoring Centre for Drugs and Drug Addiction: Luxembourg, 2019. [Google Scholar]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Dines, A.M.; Wood, D.M.; Yates, C.; Heyerdahl, F.; Hovda, K.E.; Giraudon, I.; Sedefov, R.; Dargan, P.I.; Group, E.-D.R. Acute recreational drug and new psychoactive substance toxicity in Europe: 12 months data collection from the European Drug Emergencies Network (Euro-DEN). Clin. Toxicol. 2015, 53, 893–900. [Google Scholar] [CrossRef]
- Busardo, F.; Jones, A. GHB pharmacology and toxicology: Acute intoxication, concentrations in blood and urine in forensic cases and treatment of the withdrawal syndrome. Curr. Neuropharmacol. 2015, 13, 47–70. [Google Scholar] [CrossRef] [Green Version]
- Dijkstra, B.A.; Kamal, R.; van Noorden, M.S.; de Haan, H.; Loonen, A.J.; De Jong, C.A. Detoxification with titration and tapering in gamma-hydroxybutyrate (GHB) dependent patients: The Dutch GHB monitor project. Drug Alcohol Depend. 2017, 170, 164–173. [Google Scholar] [CrossRef]
- McDonough, M.; Kennedy, N.; Glasper, A.; Bearn, J. Clinical features and management of gamma-hydroxybutyrate (GHB) withdrawal: A review. Drug Alcohol Depend. 2004, 75, 3–9. [Google Scholar] [CrossRef]
- Beurmanjer, H.; Luykx, J.; De Wilde, B.; van Rompaey, K.; Buwalda, V.; De Jong, C.; Dijkstra, B.; Schellekens, A. Tapering with Pharmaceutical GHB or Benzodiazepines for Detoxification in GHB-Dependent Patients: A Matched-Subject Observational Study of Treatment-as-Usual in Belgium and The Netherlands. CNS Drugs 2020, 34, 651–659. [Google Scholar] [CrossRef]
- Kamal, R.M.; van Noorden, M.S.; Wannet, W.; Beurmanjer, H.; Dijkstra, B.A.; Schellekens, A. Pharmacological treatment in γ-hydroxybutyrate (GHB) and γ-Butyrolactone (GBL) dependence: Detoxification and relapse prevention. CNS Drugs 2017, 31, 51–64. [Google Scholar] [CrossRef] [Green Version]
- Kamal, R.M.; van Noorden, M.S.; Franzek, E.; Dijkstra, B.A.; Loonen, A.J.; De Jong, C.A. The neurobiological mechanisms of gamma-hydroxybutyrate dependence and withdrawal and their clinical relevance: A review. Neuropsychobiology 2016, 73, 65–80. [Google Scholar] [CrossRef]
- Gobaille, S.; Hechler, V.; Andriamampandry, C.; Kemmel, V.; Maitre, M. γ-Hydroxybutyrate modulates synthesis and extracellular concentration of γ-aminobutyric acid in discrete rat brain regions in vivo. J. Pharmacol. Exp. Ther. 1999, 290, 303–309. [Google Scholar]
- Hu, R.; Banerjee, P.; Snead Iii, O. Regulation of γ-aminobutyric acid (GABA) release in cerebral cortex in the γ-hydroxybutyric acid (GHB) model of absence seizures in rat. Neuropharmacology 2000, 39, 427–439. [Google Scholar] [CrossRef]
- Carai, M.A.; Colombo, G.; Brunetti, G.; Melis, S.; Serra, S.; Vacca, G.; Mastinu, S.; Pistuddi, A.M.; Solinas, C.; Cignarella, G. Role of GABAB receptors in the sedative/hypnotic effect of γ-hydroxybutyric acid. Eur. J. Pharmacol. 2001, 428, 315–321. [Google Scholar] [CrossRef]
- Liechti, M.E.; Quednow, B.B.; Liakoni, E.; Dornbierer, D.; von Rotz, R.; Gachet, M.S.; Gertsch, J.; Seifritz, E.; Bosch, O.G. Pharmacokinetics and pharmacodynamics of γ-hydroxybutyrate in healthy subjects. Br. J. Clin. Pharmacol. 2016, 81, 980–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, C.A.; Kamal, R.; Dijkstra, B.A.; de Haan, H.A. Gamma-hydroxybutyrate detoxification by titration and tapering. Eur. Addict. Res. 2012, 18, 40–45. [Google Scholar] [CrossRef]
- Hack, J.B.; Hoffman, R.; Nelson, L.S. Resistant alcohol withdrawal: Does an unexpectedly large sedative requirement identify these patients early? J. Med. Toxicol. 2006, 2, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Ling, W.; Hillhouse, M.; Domier, C.; Doraimani, G.; Hunter, J.; Thomas, C.; Jenkins, J.; Hasson, A.; Annon, J.; Saxon, A. Buprenorphine tapering schedule and illicit opioid use. Addiction 2009, 104, 256–265. [Google Scholar] [CrossRef]
- Sivilotti, M.L.; Burns, M.J.; Aaron, C.K.; Greenberg, M.J. Pentobarbital for severe gamma-butyrolactone withdrawal. Ann. Emerg. Med. 2001, 38, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, A.; Chandra, M.; Deshpande, S.N. A comparative study of fixed tapering dose regimen versus symptom-triggered regimen of lorazepam for alcohol detoxification. Alcohol Alcohol. 2014, 49, 287–291. [Google Scholar] [CrossRef] [Green Version]
- Vasilenko, S.A.; Evans-Polce, R.J.; Lanza, S.T. Age trends in rates of substance use disorders across ages 18–90: Differences by gender and race/ethnicity. Drug Alcohol Depend. 2017, 180, 260–264. [Google Scholar] [CrossRef]
- McHugh, R.K.; Votaw, V.R.; Sugarman, D.E.; Greenfield, S.F. Sex and gender differences in substance use disorders. Clin. Psychol. Rev. 2018, 66, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; De Girolamo, G.; Haro, J.M.; Jin, R. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef]
- Zilberman, M.L.; Tavares, H.; Blume, S.B.; El-Guebaly, N. Substance use disorders: Sex differences and psychiatric comorbidities. Can. J. Psychiatry 2003, 48, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Beurmanjer, H.; Kamal, R.M.; de Jong, C.A.; Dijkstra, B.A.; Schellekens, A.F. Baclofen to prevent relapse in gamma-hydroxybutyrate (GHB)-dependent patients: A multicentre, open-label, non-randomized, controlled trial. CNS Drugs 2018, 32, 437–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar]
- Schippers, G.M.; Broekman, T.G.; Buchholz, A.; Koeter, M.W.; Van Den Brink, W. Measurements in the Addictions for Triage and Evaluation (MATE): An instrument based on the World Health Organization family of international classifications. Addiction 2010, 105, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Handelsman, L.; Cochrane, K.J.; Aronson, M.J.; Ness, R.; Rubinstein, K.J.; Kanof, P.D. Two new rating scales for opiate withdrawal. Am. J. Drug Alcohol Abus. 1987, 13, 293–308. [Google Scholar] [CrossRef]
- Dijkstra, B.A.; Krabbe, P.F.; Riezebos, T.G.; van der Staak, C.P.; De Jong, C.A. Psychometric evaluation of the Dutch version of the Subjective Opiate Withdrawal Scale (SOWS). Eur. Addict. Res. 2007, 13, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Ashton, H. The diagnosis and management of benzodiazepine dependence. Curr. Opin. Psychiatry 2005, 18, 249–255. [Google Scholar] [CrossRef]
- Perry, E.C. Inpatient management of acute alcohol withdrawal syndrome. CNS Drugs 2014, 28, 401–410. [Google Scholar] [CrossRef]
- Mirijello, A.; D’Angelo, C.; Ferrulli, A.; Vassallo, G.; Antonelli, M.; Caputo, F.; Leggio, L.; Gasbarrini, A.; Addolorato, G. Identification and management of alcohol withdrawal syndrome. Drugs 2015, 75, 353–365. [Google Scholar] [CrossRef] [Green Version]
- Quaglio, G.; Pattaro, C.; Gerra, G.; Mathewson, S.; Verbanck, P.; Des Jarlais, D.C.; Lugoboni, F. High dose benzodiazepine dependence: Description of 29 patients treated with flumazenil infusion and stabilised with clonazepam. Psychiatry Res. 2012, 198, 457–462. [Google Scholar] [CrossRef]
- Sullivan, J.T.; Sykora, K.; Schneiderman, J.; Naranjo, C.A.; Sellers, E.M. Assessment of alcohol withdrawal: The revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br. J. Addict. 1989, 84, 1353–1357. [Google Scholar] [CrossRef]
- Liao, P.-C.; Chang, H.-M.; Chen, L.-Y. Clinical management of gamma-hydroxybutyrate (GHB) withdrawal delirium with CIWA-Ar protocol. J. Formos. Med. Assoc. 2018, 117, 1124–1127. [Google Scholar] [CrossRef]
- Habibian, S.; Ahamad, K.; McLean, M.; Socias, M.E. Successful management of gamma-hydroxybutyrate (GHB) withdrawal using baclofen as a standalone therapy: A case report. J. Addict. Med. 2019, 13, 415. [Google Scholar] [CrossRef]
- Garcia, A.N.; Salloum, I.M. Polysomnographic sleep disturbances in nicotine, caffeine, alcohol, cocaine, opioid, and cannabis use: A focused review. Am. J. Addict. 2015, 24, 590–598. [Google Scholar] [CrossRef]
- Arroyo-Novoa, C.M.; Figueroa-Ramos, M.I.; Balas, M.; Rodríguez, P.; Puntillo, K.A. Opioid and benzodiazepine withdrawal syndromes in trauma ICU patients: A prospective exploratory study. Crit. Care Explor. 2020, 2, e0089. [Google Scholar] [CrossRef] [PubMed]
- Kattimani, S.; Bharadwaj, B. Clinical management of alcohol withdrawal: A systematic review. Ind. Psychiatry J. 2013, 22, 100–108. [Google Scholar]
- Maldonado, J.R.; Sher, Y.; Ashouri, J.F.; Hills-Evans, K.; Swendsen, H.; Lolak, S.; Miller, A.C. The “Prediction of Alcohol Withdrawal Severity Scale” (PAWSS): Systematic literature review and pilot study of a new scale for the prediction of complicated alcohol withdrawal syndrome. Alcohol 2014, 48, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Schuckit, M.A. Recognition and management of withdrawal delirium (delirium tremens). N. Engl. J. Med. 2014, 371, 2109–2113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Back, S.E.; Payne, R.L.; Wahlquist, A.H.; Carter, R.E.; Stroud, Z.; Haynes, L.; Hillhouse, M.; Brady, K.T.; Ling, W. Comparative profiles of men and women with opioid dependence: Results from a national multisite effectiveness trial. Am. J. Drug Alcohol Abus. 2011, 37, 313–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrmann, E.S.; Weerts, E.M.; Vandrey, R. Sex differences in cannabis withdrawal symptoms among treatment-seeking cannabis users. Exp. Clin. Psychopharmacol. 2015, 23, 415. [Google Scholar] [CrossRef]
- Leventhal, A.M.; Waters, A.J.; Boyd, S.; Moolchan, E.T.; Lerman, C.; Pickworth, W.B. Gender differences in acute tobacco withdrawal: Effects on subjective, cognitive, and physiological measures. Exp. Clin. Psychopharmacol. 2007, 15, 21. [Google Scholar] [CrossRef] [Green Version]
- Kamal, R.M.; Dijkstra, B.A.; Loonen, A.J.; De Jong, C.A. The effect of co-occurring substance use on gamma-hydroxybutyric acid withdrawal syndrome. J. Addict. Med. 2016, 10, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Cappetta, M.; Murnion, B.P. Inpatient management of gamma-hydroxybutyrate withdrawal. Australas. Psychiatry 2019, 27, 284–287. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of participants included in the study.

Figure 2.
Average relative severity and prevalence of subjective- and objective withdrawal symptoms. (a) Heat map of all 33 SWS over time for the first 11 detoxification days. Symptoms are ranked based on the average severity of the symptom over all days for males and females combined. (b) Heat map of all 34 OWS over time for the first 11 detoxification days. Symptoms are ranked based on the average presence of the symptom over all days for males and females combined.
Figure 2.
Average relative severity and prevalence of subjective- and objective withdrawal symptoms. (a) Heat map of all 33 SWS over time for the first 11 detoxification days. Symptoms are ranked based on the average severity of the symptom over all days for males and females combined. (b) Heat map of all 34 OWS over time for the first 11 detoxification days. Symptoms are ranked based on the average presence of the symptom over all days for males and females combined.


Figure 3.
Development of vital signs over time during the first 11 days of GHB tapering. Data are presented as the average of all patients measured on the respective days ± SEM (n = 108–263). Error bars may lie under the symbol of the graph. *** = main effect of time p < 0.001; **** = main effect of time p < 0.0001.
Figure 3.
Development of vital signs over time during the first 11 days of GHB tapering. Data are presented as the average of all patients measured on the respective days ± SEM (n = 108–263). Error bars may lie under the symbol of the graph. *** = main effect of time p < 0.001; **** = main effect of time p < 0.0001.

Figure 4.
Development of subjective- and objective withdrawal symptoms over time in males and females. (a) Development of subjective withdrawal symptoms (SWS) during GHB detoxification, divided by sex. SWS are presented as the average severity of all 33 measured SWS during the day (males n = 74–184, females n = 31–76). (b) Development of objective withdrawal symptoms (OWS) during GHB detoxification, divided by sex. OWS are presented as the average presence of all 34 measured objective withdrawal symptoms during the day (males n = 77–191, females n = 31–72). Data are presented as mean ± SEM. #### = main effect of time p < 0.0001; * = time x sex interaction p < 0.05.
Figure 4.
Development of subjective- and objective withdrawal symptoms over time in males and females. (a) Development of subjective withdrawal symptoms (SWS) during GHB detoxification, divided by sex. SWS are presented as the average severity of all 33 measured SWS during the day (males n = 74–184, females n = 31–76). (b) Development of objective withdrawal symptoms (OWS) during GHB detoxification, divided by sex. OWS are presented as the average presence of all 34 measured objective withdrawal symptoms during the day (males n = 77–191, females n = 31–72). Data are presented as mean ± SEM. #### = main effect of time p < 0.0001; * = time x sex interaction p < 0.05.

Table 1.
Patients with GUD characteristics of unique patients (n = 285).
| Characteristics | Male (n = 206) | Female (n = 79) | |
|---|---|---|---|
| Sex | 72.3% | 27.7% | |
| Mean age in years (SD) ** | 29.34 (6.44) | 26.63 (6.67) | |
| Mean age at first GHB use (SD) ** | 25.05 (6.67) | 21.96 (6.62) | |
| Mean years of GHB use (SD) | 4.18 (2.62) | 3.83 (2.96) | |
| Mean days of GHB use in last 30 days (SD) | 29.69 (1.74) | 29.91 (0.71) | |
| Mean daily GHB dose before admission in mL (SD) | 92.01 (48.75) | 76.44 (43.05) | |
| Mean interval between two GHB doses in hours (SD) | 2.30 (5.88) | 1.85 (0.64) | |
| Mean number of days of co-morbid substance use in last 30 days (SD) | Alcohol | 4.95 (8.87) | 2.96 (5.77) |
| Nicotine | 20.97 (13.55) | 23.04 (12.64) | |
| Cannabis | 6.68 (11.56) | 5.73 (10.60) | |
| Stimulants | 5.46 (10.23) | 5.35 (10.07) | |
| Cocaine | 2.11 (5.97) | 1.64 (0.95) | |
| Sedatives | 8.16 (12.88) | 8.87 (12.92) | |
| Medication | Anti-psychotics | 15.53% | 12.66% |
| Beta blockers | 3.88% | 2.53% | |
| Benzodiazepines | 40.78% | 41.77% | |
| Sleep medication | 17.48% | 15.19% | |
| Other | 24.27% | 29.11% |
** = p < 0.01.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wolf, C.J.H.; Beurmanjer, H.; Dijkstra, B.A.G.; Geerlings, A.C.; Spoelder, M.; Homberg, J.R.; Schellekens, A.F.A. Characterization of the GHB Withdrawal Syndrome. J. Clin. Med. 2021, 10, 2333. https://doi.org/10.3390/jcm10112333
AMA Style
Wolf CJH, Beurmanjer H, Dijkstra BAG, Geerlings AC, Spoelder M, Homberg JR, Schellekens AFA. Characterization of the GHB Withdrawal Syndrome. Journal of Clinical Medicine. 2021; 10(11):2333. https://doi.org/10.3390/jcm10112333
Chicago/Turabian StyleWolf, Casper J. H., Harmen Beurmanjer, Boukje A. G. Dijkstra, Alexander C. Geerlings, Marcia Spoelder, Judith R. Homberg, and Arnt F. A. Schellekens. 2021. "Characterization of the GHB Withdrawal Syndrome" Journal of Clinical Medicine 10, no. 11: 2333. https://doi.org/10.3390/jcm10112333
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.