
High Prevalence of Late-Onset Fabry Cardiomyopathy in a Cohort of 499 Non-Selective Patients with Left Ventricular Hypertrophy: The Asian Fabry Cardiomyopathy High-Risk Screening Study (ASIAN-FAME)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
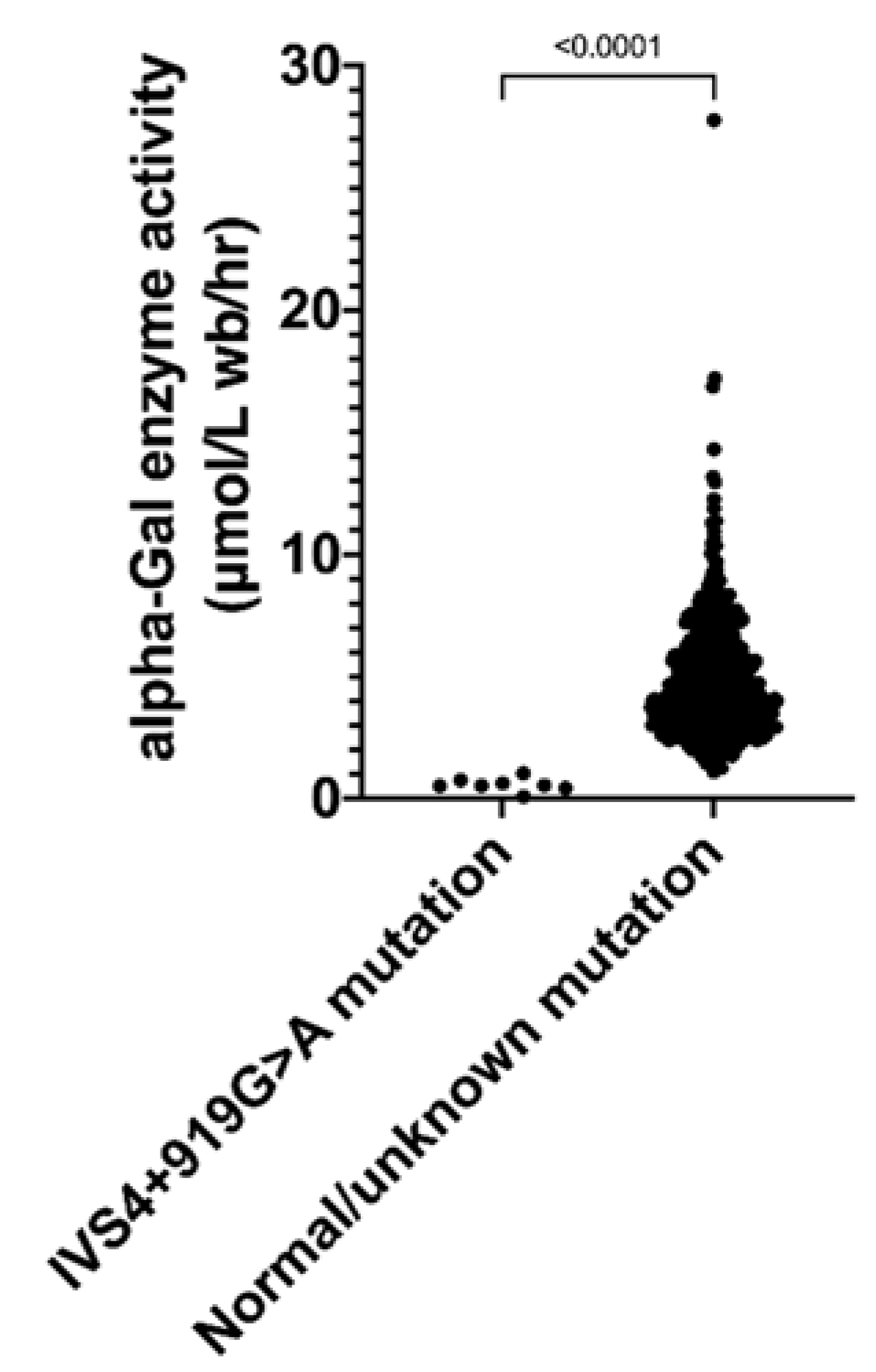
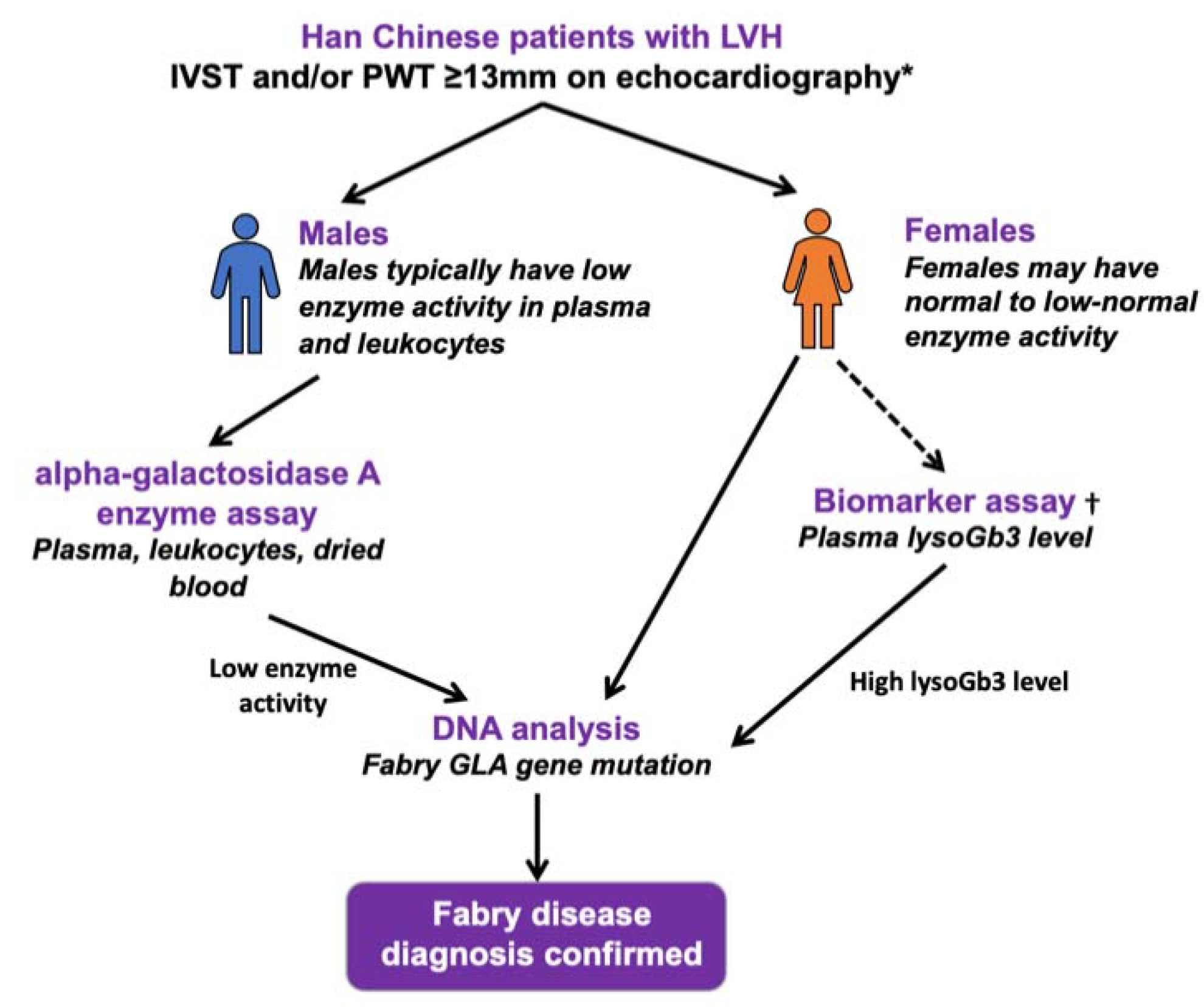
2.2. Alpha-Galactosidase A Activity Assay and Genetic Study of the GLA Gene
2.3. Demographic and Clinical Data Collection
2.4. Cardiac Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hagege, A.; Reant, P.; Habib, G.; Damy, T.; Barone-Rochette, G.; Soulat, G.; Donal, E.; Germain, D.P. Fabry disease in cardiology practice: Literature review and expert point of view. Arch. Cardiovasc. Dis. 2019, 112, 278–287. [Google Scholar] [CrossRef]
- Hwu, W.L.; Chien, Y.H.; Lee, N.C.; Chiang, S.C.; Dobrovolny, R.; Huang, A.C.; Yeh, H.Y.; Chao, M.C.; Lin, S.J.; Kitagawa, T.; et al. Newborn screening for Fabry disease in Taiwan reveals a high incidence of the later-onset GLA mutation c.936+919G>A (IVS4+919G>A). Hum. Mutat. 2009, 30, 1397–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chimenti, C.; Pieroni, M.; Morgante, E.; Antuzzi, D.; Russo, A.; Russo, M.A.; Maseri, A.; Frustaci, A. Prevalence of Fabry disease in female patients with late-onset hypertrophic cardiomyopathy. Circulation 2004, 110, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Monserrat, L.; Gimeno-Blanes, J.R.; Marin, F.; Hermida-Prieto, M.; Garcia-Honrubia, A.; Perez, I.; Fernandez, X.; de Nicolas, R.; de la Morena, G.; Paya, E.; et al. Prevalence of fabry disease in a cohort of 508 unrelated patients with hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2007, 50, 2399–2403. [Google Scholar] [CrossRef] [Green Version]
- Mehta, A.; Widmer UIn: Mehta, A.; Beck, M.; Sunder-Plassmann, G. (Eds.) Fabry Disease: Perspectives from 5 Years of FOS; Oxford PharmaGenesis: Oxford, UK, 2006. [Google Scholar]
- Chang, W.H.; Niu, D.M.; Lu, C.Y.; Lin, S.Y.; Liu, T.C.; Chang, J.G. Modulation the alternative splicing of GLA (IVS4+919G>A) in Fabry disease. PLoS ONE 2017, 12, e0175929. [Google Scholar] [CrossRef]
- Kubo, T.; Ochi, Y.; Baba, Y.; Hirota, T.; Tanioka, K.; Yamasaki, N.; Yoshimitsu, M.; Higuchi, K.; Takenaka, T.; Nakajima, K.; et al. Prevalence and clinical features of Fabry disease in Japanese male patients with diagnosis of hypertrophic cardiomyopathy. J. Cardiol. 2017, 69, 302–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.Y.; Chong, K.W.; Hsu, J.H.; Yu, H.C.; Shih, C.C.; Huang, C.H.; Lin, S.J.; Chen, C.H.; Chiang, C.C.; Ho, H.J.; et al. High incidence of the cardiac variant of Fabry disease revealed by newborn screening in the Taiwan Chinese population. Circ. Cardiovasc. Genet. 2009, 2, 450–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, K.H.; Lu, Y.H.; Niu, C.W.; Chang, S.K.; Chen, Y.R.; Cheng, C.Y.; Hsu, T.R.; Yang, C.F.; Nakamura, K.; Niu, D.M. The Fabry disease-causing mutation, GLA IVS4+919G>A, originated in Mainland China more than 800 years ago. J. Hum. Genet. 2020, 65, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Havndrup, O.; Christiansen, M.; Stoevring, B.; Jensen, M.; Hoffman-Bang, J.; Andersen, P.S.; Hasholt, L.; Norremolle, A.; Feldt-Rasmussen, U.; Kober, L.; et al. Fabry disease mimicking hypertrophic cardiomyopathy: Genetic screening needed for establishing the diagnosis in women. Eur. J. Heart Fail. 2010, 12, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Palecek, T.; Honzikova, J.; Poupetova, H.; Vlaskova, H.; Kuchynka, P.; Golan, L.; Magage, S.; Linhart, A. Prevalence of Fabry disease in male patients with unexplained left ventricular hypertrophy in primary cardiology practice: Prospective Fabry cardiomyopathy screening study (FACSS). J. Inherit. Metab. Dis. 2014, 37, 455–460. [Google Scholar] [CrossRef]
- Elliott, P.; Baker, R.; Pasquale, F.; Quarta, G.; Ebrahim, H.; Mehta, A.B.; Hughes, D.A.; Group AS. Prevalence of Anderson-Fabry disease in patients with hypertrophic cardiomyopathy: The European Anderson-Fabry Disease survey. Heart 2011, 97, 1957–1960. [Google Scholar] [CrossRef]
- Zhang, X.K.; Elbin, C.S.; Chuang, W.L.; Cooper, S.K.; Marashio, C.A.; Beauregard, C.; Keutzer, J.M. Multiplex enzyme assay screening of dried blood spots for lysosomal storage disorders by using tandem mass spectrometry. Clin. Chem. 2008, 54, 1725–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.J.; Chien, Y.H.; Lai, T.S.; Shih, H.M.; Chen, Y.C.; Pan, C.F.; Chen, H.H.; Hwu, W.L.; Wu, C.J. Results of Fabry Disease Screening in Male Pre-End Stage Renal Disease Patients with Unknown Etiology Found Through the Platform of a Chronic Kidney Disease Education Program in a Northern Taiwan Medical Center. Kidney Blood Press. Res. 2018, 43, 1636–1645. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, T.R.; Hung, S.C.; Chang, F.P.; Yu, W.C.; Sung, S.H.; Hsu, C.L.; Dzhagalov, I.; Yang, C.F.; Chu, T.H.; Lee, H.J.; et al. Later Onset Fabry Disease, Cardiac Damage Progress in Silence: Experience With a Highly Prevalent Mutation. J. Am. Coll. Cardiol. 2016, 68, 2554–2563. [Google Scholar] [CrossRef]
- Lin, H.Y.; Liu, H.C.; Huang, Y.H.; Liao, H.C.; Hsu, T.R.; Shen, C.I.; Li, S.T.; Li, C.F.; Lee, L.H.; Lee, P.C.; et al. Effects of enzyme replacement therapy for cardiac-type Fabry patients with a Chinese hotspot late-onset Fabry mutation (IVS4+919G>A). BMJ Open 2013, 3, e003146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, D.-M.; Yu, W.-C.; Hsu, T.; Chang, F.-P.; Sung, S.-H.; Chu, T.-H. When is the best time to start enzyme replacement therapy in patients with cardiac-type Fabry disease? Experience from Taiwan, an area highly prevalent in this cardiac phenotype. Mol. Genet. Metab. 2015, 114, S87–S88. [Google Scholar] [CrossRef]
- Nakao, S.; Takenaka, T.; Maeda, M.; Kodama, C.; Tanaka, A.; Tahara, M.; Yoshida, A.; Kuriyama, M.; Hayashibe, H.; Sakuraba, H.; et al. An atypical variant of Fabry’s disease in men with left ventricular hypertrophy. N. Engl. J. Med. 1995, 333, 288–293. [Google Scholar] [CrossRef]
- Yousef, Z.; Elliott, P.M.; Cecchi, F.; Escoubet, B.; Linhart, A.; Monserrat, L.; Namdar, M.; Weidemann, F. Left ventricular hypertrophy in Fabry disease: A practical approach to diagnosis. Eur. Heart J. 2013, 34, 802–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachdev, B.; Takenaka, T.; Teraguchi, H.; Tei, C.; Lee, P.; McKenna, W.J.; Elliott, P.M. Prevalence of Anderson-Fabry disease in male patients with late onset hypertrophic cardiomyopathy. Circulation 2002, 105, 1407–1411. [Google Scholar] [CrossRef] [Green Version]
- Ommen, S.R.; Nishimura, R.A.; Edwards, W.D. Fabry disease: A mimic for obstructive hypertrophic cardiomyopathy? Heart 2003, 89, 929–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, H.; Larson, M.G.; Barr, S.C.; Vasan, R.S.; O’Donnell, C.J.; Hirschhorn, J.N.; Levy, D.; Corey, D.; Seidman, C.E.; Seidman, J.G.; et al. Single-gene mutations and increased left ventricular wall thickness in the community: The Framingham Heart Study. Circulation 2006, 113, 2697–2705. [Google Scholar] [CrossRef] [Green Version]
- Maron, M.S.; Xin, W.; Sims, K.B.; Butler, R.; Haas, T.S.; Rowin, E.J.; Desnick, R.J.; Maron, B.J. Identification of Fabry Disease in a Tertiary Referral Cohort of Patients with Hypertrophic Cardiomyopathy. Am. J. Med. 2018, 131, 200.e1–200.e8. [Google Scholar] [CrossRef] [PubMed]
- Cecchi, F.; Iascone, M.; Maurizi, N.; Pezzoli, L.; Binaco, I.; Biagini, E.; Fibbi, M.L.; Olivotto, I.; Pieruzzi, F.; Fruntelata, A.; et al. Intraoperative Diagnosis of Anderson-Fabry Disease in Patients With Obstructive Hypertrophic Cardiomyopathy Undergoing Surgical Myectomy. JAMA Cardiol. 2017, 2, 1147–1151. [Google Scholar] [CrossRef] [PubMed]
- Adalsteinsdottir, B.; Teekakirikul, P.; Maron, B.J.; Burke, M.A.; Gudbjartsson, D.F.; Holm, H.; Stefansson, K.; DePalma, S.R.; Mazaika, E.; McDonough, B.; et al. Nationwide study on hypertrophic cardiomyopathy in Iceland: Evidence of a MYBPC3 founder mutation. Circulation 2014, 130, 1158–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadasivan, C.; Chow, J.T.Y.; Sheng, B.; Chan, D.K.H.; Fan, Y.; Choi, P.C.L.; Wong, J.K.T.; Tong, M.M.B.; Chan, T.N.; Fung, E.; et al. Screening for Fabry Disease in patients with unexplained left ventricular hypertrophy. PLoS ONE 2020, 15, e0239675. [Google Scholar] [CrossRef]
- Baptista, A.; Magalhaes, P.; Leao, S.; Carvalho, S.; Mateus, P.; Moreira, I. Screening for Fabry disease in left ventricular hypertrophy: Documentation of a novel mutation. Arq. Bras. Cardiol. 2015, 105, 139–144. [Google Scholar] [CrossRef]
- Seo, J.; Kim, M.; Hong, G.R.; Kim, D.S.; Son, J.W.; Cho, I.J.; Shim, C.Y.; Chang, H.J.; Ha, J.W.; Chung, N. Fabry disease in patients with hypertrophic cardiomyopathy: A practical approach to diagnosis. J. Hum. Genet. 2016, 61, 775–780. [Google Scholar] [CrossRef]
- Terryn, W.; Deschoenmakere, G.; De Keyser, J.; Meersseman, W.; Van Biesen, W.; Wuyts, B.; Hemelsoet, D.; Pascale, H.; De Backer, J.; De Paepe, A.; et al. Prevalence of Fabry disease in a predominantly hypertensive population with left ventricular hypertrophy. Int. J. Cardiol. 2013, 167, 2555–2560. [Google Scholar] [CrossRef] [PubMed]
- Tan, G.L. An Introduction to the Culture and History of the Teochews in Singapore; World Scientific: Singapore, 2018. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall | FD | Non-FD | p |
|---|---|---|---|---|
| (n = 499) | (n = 8) | (n = 491) | ||
| Demographic | ||||
| Age, years | 66.4 ± 12.7 | 63.0 ± 7.0 | 66.5 ± 12.8 | 0.211 |
| Men, n (%) | 336 (67.3) | 8 (100) | 328 (66.8) | 0.058 |
| Ethnicity subgroup, n (%) | 0.0172 | |||
| Canton | 284 (56.9) | 2 (25.0) | 282 (57.4) | |
| Teochew | 85 (17.0) | 5 (62.5) | 80 (16.3) | |
| Fujian | 11 (2.2) | 0 (0.0) | 11 (2.2) | |
| Shanghai | 5 (1.0) | 0 (0.0) | 5 (1.0) | |
| Others | 27 (5.4) | 1 (12.5) | 26 (5.3) | |
| Unknown | 8 (17.4) | 0 (0.0) | 87 (17.7) | |
| Diabetes, n (%) | 328 (65.7) | 1 (12.5) | 170 (34.6) | 0.274 |
| Hypertension, n (%) | 376 (75.4) | 4 (50.0) | 372 (75.8) | 0.107 |
| Aortic valve disease, n (%) | 48 (9.6) | 1 (12.5) | 47 (9.6) | 0.557 |
| Mitral valve disease, n (%) | 64 (12.8) | 2 (25.0) | 62 (12.6) | 0.274 |
| Heart failure,%) | 63 (12.6) | 4 (50.0) | 59 (12.0) | 0.011 |
| Arial fibrillation, n (%) | 112 (22.4) | 4 (50.0) | 108 (22.0) | 0.080 |
| Short PR interval (<120 ms), n (%) | 8 (1.6) | 0 (0.0) | 8 (1.6) | 1.000 |
| IVST, mm | 15 ± 2 | 18 ± 6 | 15 ± 2 | 0.118 |
| PWT, mm | 12 ± 3 | 13 ± 3 | 12 ± 3 | 0.255 |
| LVEDD, mm | 43 ± 7 | 49 ± 10 | 43 ± 7 | 0.177 |
| LVESD, mm | 30 ± 7 | 34 ± 9 | 29 ± 7 | 0.966 |
| LVM, g | 222 ± 73 | 355 ± 202 | 220 ± 67 | 0.100 |
| LVMI, g/m2 | 129 ± 38 | 181 ± 94 | 128 ± 36 | 0.159 |
| LVEDV, mL | 93 ± 41 | 126 ± 34 | 92 ± 41 | 0.028 |
| LVESV, mL | 42 ± 21 | 62 ± 30 | 41 ± 27 | 0.098 |
| LVEF, % | 57 ± 10 | 53 ± 14 | 57 ± 10 | 0.371 |
| LAV, ml | 66 ± 39 | 78 ± 32 | 66 ± 40 | 0.326 |
| RWT | 0.57 ± 0.19 | 0.57 ± 0.19 | 0.57 ± 0.19 | 0.956 |
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Age of diagnosis of FD, years | 74 | 59 | 53 | 69 | 59 | 69 | 59 | 63 |
| Gender | Male | Male | Male | Male | Male | Male | Male | Male |
| Ethnicity subgroup | Teochew | Canton | Wenzhou | Canton | Teochew | Teochew | Teochew | Teochew |
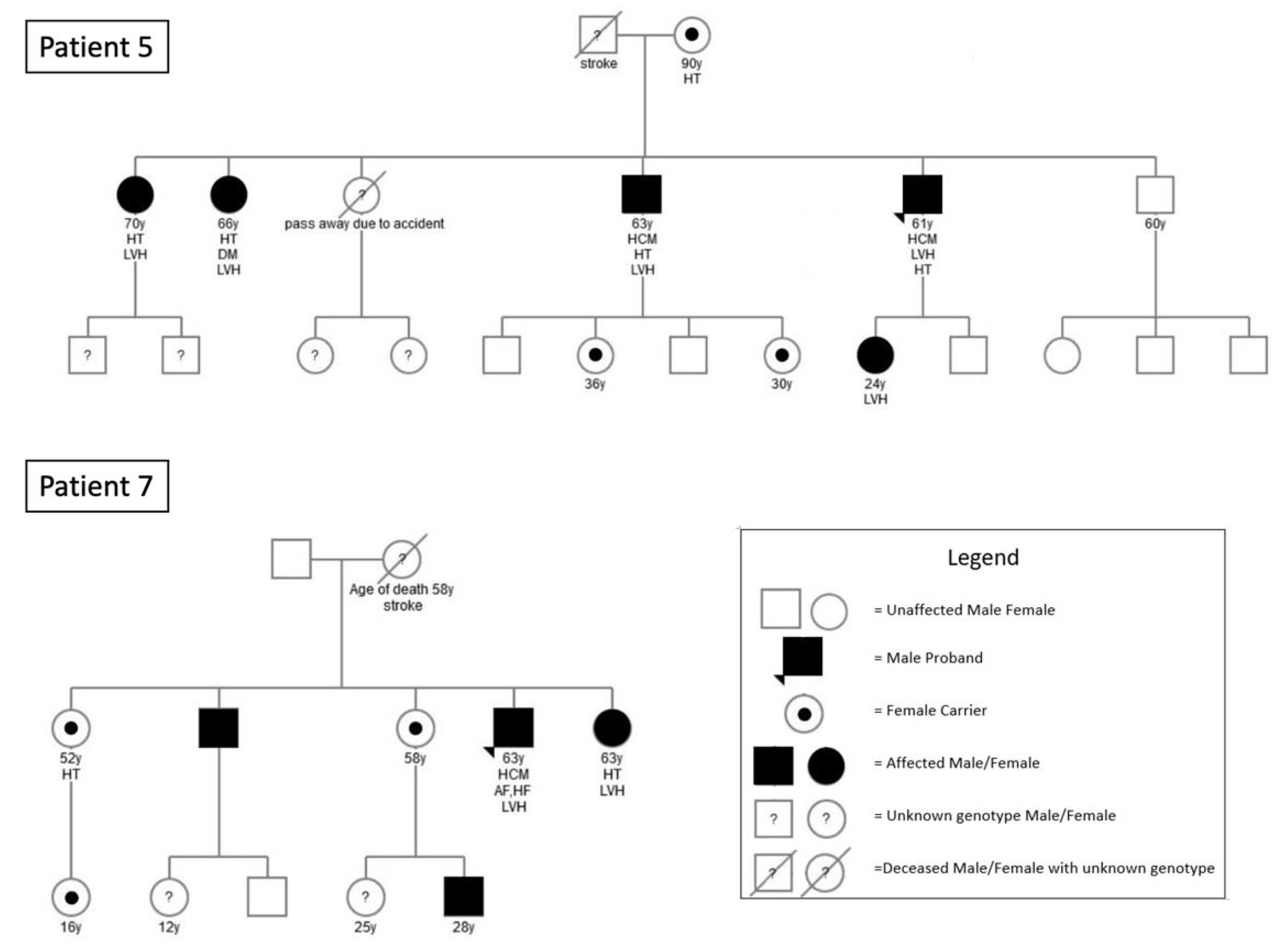
| Initial presentation | Poorly controlled hypertension since age 65; incidental murmur with severe aortic regurgitation at age 71 | Exertional dyspnea and chest pain at age 49; hypertension; acute pulmonary edema with severe mitral regurgitation associated with chordal rupture at age 59, requiring mitral valve surgery | Dizziness with lacunar infarct/ischemic changes on MRI brain at age 46; diabetes; Exertional dyspnea at age 53 | Hypertension and diabetes at age 51; syncope with third degree AVB requiring pacemaker at age 57; onset of AF and heart failure at age 67; NSVT requiring upgrade of pacemaker to ICD at age 69; echo showed septal hypertrophy IVDT = 16mm with posterior wall akinesia | Chest pain, non-ST MINOCA at age 53; hypertension; obstructive sleep apnea; labelled HCM | Heart failure with reduced ejection fraction and AF at age 65; treated as dilated cardiomyopathy possibly caused by alcoholism | Ischemic heart disease requiring percutaneous coronary intervention at age 48; obstructive sleep apnea; AF onset at age 59 requiring catheter ablation | age 61; chest pain and exertional dyspnea at age 62; labelled HCM |
| ECG findings | LVH with strain RBBB | LVH with strain | RBBB | AF, 3° AVB | LVH with strain | AF, LVH | AF, LVH | RBBB, LPFB, 2:1 AVB |
| IVST, mm | 19 | 29 | 14 | 14 | 17 | 13 | 24 | 15 |
| PWT, mm | 13 | 17 | 12 | 13 | 19 | 10 | 10 | 13 |
| LVEDD, mm | 52 | 60 | 36 | 65 | 39 | 50 | 41 | 46 |
| LVESD, mm | 33 | 43 | 23 | 50 | 29 | 38 | 26 | 32 |
| LVM, g | 378 | 812 | 160 | 420 | 302 | 218 | 294 | 257 |
| LVMI, g/m2 | 222 | 369 | 84 | 247 | 144 | 104 | 147 | 124 |
| LVEF, % | 60 | 40 | 73 | 31 | 45 | 49 | 65 | 59 |
| GLA activity, μmol/L wb/h | 0.55 | 0.43 | 0.09 | 0.54 | 0.76 | 0.64 | 0.52 | 1.04 |
| IDUA/GLA ratio | 27 | 11 | 18 | 27 | 10 | 10 | 10 | 10 |
| Creatinine, µmol/L | 204 | 116 | 89 | 118 | 87 | 74 | 98 | 83 |
| eGFR, mL/min/1.73 m² | 26 | 58 | 84 | 53 | 83 | 88 | 72 | 86 |
| Proteinuria | Urine TP/Cr: 6.62 mg/mg Cr | Urine TP/Cr: 0.05 mg/mg Cr | Urine TP/Cr: 0.04 mg/mg Cr | Spot urine albumin: <0.3 mg/L | Urine TP/Cr: 0.05 mg/mg Cr | 24 h urine protein: 0.13 g/24 h | Urine TP/Cr: 0.04 mg/mg Cr | 24 h urine protein: <0.04 g/24 h |
| GLA gene mutation | IVS4 + 919G > A | IVS4 + 919G > A | IVS4 + 919G > A | IVS4 + 919G > A | IVS4 + 919G > A | IVS4 + 919G > A | IVS4 + 919G > A | IVS4 + 919G > A |
| ERT | Decided not for ERT due to clinically advanced kidney disease; patient refused renal and endomyocardial biopsy | Started | Started | Decided not for ERT due to clinically advanced cardiac disease | Started | Started | Started | Planned to start |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, Y.; Chan, T.-N.; Chow, J.T.Y.; Kam, K.K.H.; Chi, W.-K.; Chan, J.Y.S.; Fung, E.; Tong, M.M.P.; Wong, J.K.T.; Choi, P.C.L.; et al. High Prevalence of Late-Onset Fabry Cardiomyopathy in a Cohort of 499 Non-Selective Patients with Left Ventricular Hypertrophy: The Asian Fabry Cardiomyopathy High-Risk Screening Study (ASIAN-FAME). J. Clin. Med. 2021, 10, 2160. https://doi.org/10.3390/jcm10102160
Fan Y, Chan T-N, Chow JTY, Kam KKH, Chi W-K, Chan JYS, Fung E, Tong MMP, Wong JKT, Choi PCL, et al. High Prevalence of Late-Onset Fabry Cardiomyopathy in a Cohort of 499 Non-Selective Patients with Left Ventricular Hypertrophy: The Asian Fabry Cardiomyopathy High-Risk Screening Study (ASIAN-FAME). Journal of Clinical Medicine. 2021; 10(10):2160. https://doi.org/10.3390/jcm10102160
Chicago/Turabian StyleFan, Yiting, Tsz-Ngai Chan, Josie T. Y. Chow, Kevin K. H. Kam, Wai-Kin Chi, Joseph Y. S. Chan, Erik Fung, Mabel M. P. Tong, Jeffery K. T. Wong, Paul C. L. Choi, and et al. 2021. "High Prevalence of Late-Onset Fabry Cardiomyopathy in a Cohort of 499 Non-Selective Patients with Left Ventricular Hypertrophy: The Asian Fabry Cardiomyopathy High-Risk Screening Study (ASIAN-FAME)" Journal of Clinical Medicine 10, no. 10: 2160. https://doi.org/10.3390/jcm10102160