
The Ratio of C-Reactive Protein to Albumin Is an Independent Predictor of Malignant Intraductal Papillary Mucinous Neoplasms of the Pancreas

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumors of the Digestive System; IARC Press: Lyon, France, 2010. [Google Scholar]
- Tanaka, M.; Fernández-del Castillo, C.; Kamisawa, T.; Jang, J.Y.; Levy, P.; Ohtsuka, T.; Salvia, R.; Shimizu, Y.; Tada, M.; Wolfgang, C.L. Revisions of International Consensus Fukuoka Guidelines for the Management of IPMN of the Pancreas. Pancreatology 2017, 17, 738–753. [Google Scholar] [CrossRef] [PubMed]
- Kaimakliotis, P.; Riff, B.; Pourmand, K.; Chandrasekhara, V.; Furth, E.E.; Siegelman, E.S.; Drebin, J.; Vollmer, C.M.; Kochman, M.L.; Ginsberg, G.G.; et al. Sendai and Fukuoka Consensus Guidelines Identify Advanced Neoplasia in Patients with Suspected Mucinous Cystic Neoplasms of the Pancreas. Clin. Gastroenterol. Hepatol. 2015, 13, 1808–1815. [Google Scholar] [CrossRef]
- Kim, J.R.; Jang, J.-Y.; Kang, M.J.; Park, T.; Lee, S.Y.; Jung, W.; Chang, J.; Shin, Y.; Han, Y.; Kim, S.-W. Clinical Implication of Serum Carcinoembryonic Antigen and Carbohydrate Antigen 19-9 for the Prediction of Malignancy in Intraductal Papillary Mucinous Neoplasm of Pancreas. J. Hepato-Biliary-Pancreat. Sci. 2015, 22, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Kono, Y.; Murakami, Y.; Shishido, Y.; Kuroda, H.; Matsunaga, T.; Fukumoto, Y.; Osaki, T.; Ashida, K.; Fujiwara, Y. Prognostic Significance of the Preoperative Ratio of C-Reactive Protein to Albumin and Neutrophil–Lymphocyte Ratio in Gastric Cancer Patients. World J. Surg. 2018, 42, 1819–1825. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Agizamhan, S.; Zhao, X.; Jiang, B.; Qin, H.; Chen, M.; Guo, H. Preoperative C-Reactive Protein/Albumin Ratio Predicts Outcome of Surgical Papillary Renal Cell Carcinoma. Future Oncol. 2019, 15, 1459–1468. [Google Scholar] [CrossRef]
- Xiang, Z.; Hu, T.; Wang, Y.; Wang, H.; Xu, L.; Cui, N. Neutrophil–Lymphocyte Ratio (NLR) Was Associated with Prognosis and Immunomodulatory in Patients with Pancreatic Ductal Adenocarcinoma (PDAC). Biosci. Rep. 2020, 40, BSR20201190. [Google Scholar] [CrossRef]
- Alagappan, M.; Pollom, E.L.; von Eyben, R.; Kozak, M.M.; Aggarwal, S.; Poultsides, G.A.; Koong, A.C.; Chang, D.T. Albumin and Neutrophil-Lymphocyte Ratio (NLR) Predict Survival in Patients with Pancreatic Adenocarcinoma Treated With SBRT. Am. J. Clin. Oncol. 2018, 41, 242–247. [Google Scholar] [CrossRef]
- Shen, Y.; Wang, H.; Li, W.; Chen, J. Prognostic Significance of the CRP/Alb and Neutrophil to Lymphocyte Ratios in Hepatocellular Carcinoma Patients Undergoing TACE and RFA. J. Clin. Lab. Anal. 2019, 33, e22999. [Google Scholar] [CrossRef] [Green Version]
- Gemenetzis, G.; Bagante, F.; Griffin, J.F.; Rezaee, N.; Javed, A.A.; Manos, L.L.; Lennon, A.M.; Wood, L.D.; Hruban, R.H.; Zheng, L.; et al. Neutrophil-to-Lymphocyte Ratio Is a Predictive Marker for Invasive Malignancy in Intraductal Papillary Mucinous Neoplasms of the Pancreas. Ann. Surg. 2017, 266, 339–345. [Google Scholar] [CrossRef]
- Hata, T.; Mizuma, M.; Motoi, F.; Ishida, M.; Morikawa, T.; Nakagawa, K.; Hayashi, H.; Kanno, A.; Masamune, A.; Kamei, T.; et al. An Integrated Analysis of Host- and Tumor-Derived Markers for Predicting High-Grade Dysplasia and Associated Invasive Carcinoma of Intraductal Papillary Mucinous Neoplasms of the Pancreas. Surg. Today 2020, 50, 1039–1048. [Google Scholar] [CrossRef]
- Li, J.A.; Han, X.; Fang, Y.; Zhang, L.; Lou, W.H.; Xu, X.F.; Wu, W.C.; Kuang, T.T.; Wang, D.S.; Rong, Y.F. The value of preoperative CA19-9 combined with platelet-to-lymphocyte ratio in predicting invasive malignancy in intraductal papillary mucinous neoplasms. Zhonghua Wai Ke Za Zhi 2019, 57, 170–175. [Google Scholar] [PubMed]
- Basturk, O.; Hong, S.-M.; Wood, L.D.; Adsay, N.V.; Albores-Saavedra, J.; Biankin, A.V.; Brosens, L.A.A.; Fukushima, N.; Goggins, M.; Hruban, R.H.; et al. A Revised Classification System and Recommendations From the Baltimore Consensus Meeting for Neoplastic Precursor Lesions in the Pancreas. Am. J. Surg. Pathol. 2015, 39, 1730–1741. [Google Scholar] [CrossRef]
- Tanaka, M.; Chari, S.; Adsay, V.; Carlos Castillo, F.-D.; Falconi, M.; Shimizu, M.; Yamaguchi, K.; Yamao, K.; Matsuno, S. International Consensus Guidelines for Management of Intraductal Papillary Mucinous Neoplasms and Mucinous Cystic Neoplasms of the Pancreas. Pancreatology 2006, 6, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Laird, B.J.; Kaasa, S.; McMillan, D.C.; Fallon, M.T.; Hjermstad, M.J.; Fayers, P.; Klepstad, P. Prognostic Factors in Patients with Advanced Cancer: A Comparison of Clinicopathological Factors and the Development of an Inflammation-Based Prognostic System. Clin. Cancer Res. 2013, 19, 5456–5464. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Fernández-del Castillo, C.; Adsay, V.; Chari, S.; Falconi, M.; Jang, J.-Y.; Kimura, W.; Levy, P.; Pitman, M.B.; Schmidt, C.M.; et al. International Consensus Guidelines 2012 for the Management of IPMN and MCN of the Pancreas. Pancreatology 2012, 12, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Kwon, W.; Han, Y.; Byun, Y.; Kang, J.S.; Choi, Y.J.; Kim, H.; Jang, J.-Y. Predictive Features of Malignancy in Branch Duct Type Intraductal Papillary Mucinous Neoplasm of the Pancreas: A Meta-Analysis. Cancers 2020, 12, 2618. [Google Scholar] [CrossRef]
- Goh, B.K.P.; Tan, D.M.Y.; Chan, C.-Y.; Lee, S.-Y.; Lee, V.T.W.; Thng, C.-H.; Low, A.S.C.; Tai, D.W.M.; Cheow, P.-C.; Chow, P.K.H.; et al. Are Preoperative Blood Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios Useful in Predicting Malignancy in Surgically-Treated Mucin-Producing Pancreatic Cystic Neoplasms?: NLR and PLR in Pancreatic Cysts. J. Surg. Oncol. 2015, 112, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Arima, K.; Okabe, H.; Hashimoto, D.; Chikamoto, A.; Kuroki, H.; Taki, K.; Kaida, T.; Higashi, T.; Nitta, H.; Komohara, Y.; et al. The Neutrophil-to-Lymphocyte Ratio Predicts Malignant Potential in Intraductal Papillary Mucinous Neoplasms. J. Gastrointest. Surg. 2015, 19, 2171–2177. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Masamune, A.; Shimosegawa, T. Inflammation and Pancreatic Cancer: Disease Promoter and New Therapeutic Target. J. Gastroenterol. 2014, 49, 605–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadot, E.; Basturk, O.; Klimstra, D.S.; Gönen, M.; Lokshin, A.; Do, R.K.G.; D’Angelica, M.I.; DeMatteo, R.P.; Kingham, T.P.; Jarnagin, W.R.; et al. Tumor-Associated Neutrophils and Malignant Progression in Intraductal Papillary Mucinous Neoplasms: An Opportunity for Identification of High-Risk Disease. Ann. Surg. 2015, 262, 1102–1107. [Google Scholar] [CrossRef] [Green Version]
- Inman, K.S. Complex Role for the Immune System in Initiation and Progression of Pancreatic Cancer. World J. Gastroenterol. 2014, 20, 11160. [Google Scholar] [CrossRef]
- Arima, K.; Okabe, H.; Hashimoto, D.; Chikamoto, A.; Tsuji, A.; Yamamura, K.; Kitano, Y.; Inoue, R.; Kaida, T.; Higashi, T.; et al. The Diagnostic Role of the Neutrophil-to-Lymphocyte Ratio in Predicting Pancreatic Ductal Adenocarcinoma in Patients with Pancreatic Diseases. Int. J. Clin. Oncol. 2016, 21, 940–945. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, C.A.; Pulvirenti, A.; Lawrence, S.A.; Seier, K.; Gonen, M.; Balachandran, V.P.; Kingham, T.P.; D’Angelica, M.I.; Drebin, J.A.; Jarnagin, W.R.; et al. Neutrophil-to-Lymphocyte Ratio as a Predictor of Invasive Carcinoma in Patients with Intraductal Papillary Mucinous Neoplasms of the Pancreas. Pancreas 2019, 48, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Ohno, R.; Kawamoto, R.; Kanamoto, M.; Watanabe, J.; Fujii, M.; Ohtani, H.; Harada, M.; Kumagi, T.; Kawasaki, H. Neutrophil to Lymphocyte Ratio Is a Predictive Factor of Malignant Potential for Intraductal Papillary Mucinous Neoplasms of the Pancreas. Biomark. Insights 2019, 14, 117727191985150. [Google Scholar] [CrossRef]
- Hata, T.; Mizuma, M.; Motoi, F.; Ishida, M.; Morikawa, T.; Takadate, T.; Nakagawa, K.; Hayashi, H.; Kanno, A.; Masamune, A.; et al. Diagnostic and Prognostic Impact of Neutrophil-to-Lymphocyte Ratio for Intraductal Papillary Mucinous Neoplasms of the Pancreas With High-Grade Dysplasia and Associated Invasive Carcinoma. Pancreas 2019, 48, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Goh, B.K.P.; Teo, J.-Y.; Allen, J.C.; Tan, D.M.Y.; Chan, C.-Y.; Lee, S.-Y.; Tai, D.W.M.; Thng, C.-H.; Cheow, P.-C.; Chow, P.K.H.; et al. Preoperative Platelet-to-Lymphocyte Ratio Improves the Performance of the International Consensus Guidelines in Predicting Malignant Pancreatic Cystic Neoplasms. Pancreatology 2016, 16, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, I.; Peacock, O.; Lloyd, G.; Larvin, M.; Hall, R.I. Preoperative Hematologic Markers as Independent Predictors of Prognosis in Resected Pancreatic Ductal Adenocarcinoma: Neutrophil-Lymphocyte versus Platelet-Lymphocyte Ratio. Am. J. Surg. 2010, 200, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, J.; Grimes, N.; Farid, S.; Morris-Stiff, G. Inflammatory Response Related Scoring Systems in Assessing the Prognosis of Patients with Pancreatic Ductal Adenocarcinoma: A Systematic Review. Hepatobiliary Pancreat. Dis. Int. 2014, 13, 474–481. [Google Scholar] [CrossRef]
- Stotz, M.; Gerger, A.; Eisner, F.; Szkandera, J.; Loibner, H.; Ress, A.L.; Kornprat, P.; A Zoughbi, W.; Seggewies, F.S.; Lackner, C.; et al. Increased Neutrophil-Lymphocyte Ratio Is a Poor Prognostic Factor in Patients with Primary Operable and Inoperable Pancreatic Cancer. Br. J. Cancer 2013, 109, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Shusterman, M.; Jou, E.; Kaubisch, A.; Chuy, J.W.; Rajdev, L.; Aparo, S.; Tang, J.; Ohri, N.; Negassa, A.; Goel, S. The Neutrophil-to-Lymphocyte Ratio Is a Prognostic Biomarker in An Ethnically Diverse Patient Population with Advanced Pancreatic Cancer. J. Gastrointest. Cancer 2020, 51, 868–876. [Google Scholar] [CrossRef]
- Asari, S.; Matsumoto, I.; Toyama, H.; Shinzeki, M.; Goto, T.; Ishida, J.; Ajiki, T.; Fukumoto, T.; Ku, Y. Preoperative Independent Prognostic Factors in Patients with Borderline Resectable Pancreatic Ductal Adenocarcinoma Following Curative Resection: The Neutrophil-Lymphocyte and Platelet-Lymphocyte Ratios. Surg. Today 2016, 46, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wei, Q.; Fan, J.; Cheng, S.; Ding, W.; Hua, Z. Prognostic Role of the Neutrophil-to-Lymphocyte Ratio in Pancreatic Cancer: A Meta-Analysis Containing 8252 Patients. Clin. Chim. Acta 2018, 479, 181–189. [Google Scholar] [CrossRef]
- Haruki, K.; Shiba, H.; Shirai, Y.; Horiuchi, T.; Iwase, R.; Fujiwara, Y.; Furukawa, K.; Misawa, T.; Yanaga, K. The C-Reactive Protein to Albumin Ratio Predicts Long-Term Outcomes in Patients with Pancreatic Cancer After Pancreatic Resection. World J. Surg. 2016, 40, 2254–2260. [Google Scholar] [CrossRef]
- Liu, Z.; Jin, K.; Guo, M.; Long, J.; Liu, L.; Liu, C.; Xu, J.; Ni, Q.; Luo, G.; Yu, X. Prognostic Value of the CRP/Alb Ratio, a Novel Inflammation-Based Score in Pancreatic Cancer. Ann. Surg. Oncol. 2017, 24, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Tanaka, K.; Fushiya, N.; Koike, K.; Nishino, H.; Matsushima, M. The C-Reactive Protein/Albumin Ratio, a Novel Inflammation-Based Prognostic Score, Predicts Outcomes in Patients with Hepatocellular Carcinoma. Ann. Surg. Oncol. 2015, 22, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An Inflammation-Based Prognostic Score (MGPS) Predicts Cancer Survival Independent of Tumour Site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, V.K.H.; Malik, H.Z.; Hamady, Z.Z.R.; Al-Mukhtar, A.; Gomez, D.; Prasad, K.R.; Toogood, G.J.; Lodge, J.P.A. C-Reactive Protein as a Predictor of Prognosis Following Curative Resection for Colorectal Liver Metastases. Br. J. Cancer 2007, 96, 222–225. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Wezeman, M.; Zhang, X.; Lin, P.; Wang, M.; Qian, J.; Wan, B.; Kwak, L.W.; Yu, L.; Yi, Q. Human C-Reactive Protein Binds Activating Fcgamma Receptors and Protects Myeloma Tumor Cells from Apoptosis. Cancer Cell 2007, 12, 252–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanda, M.; Fujii, T.; Kodera, Y.; Nagai, S.; Takeda, S.; Nakao, A. Nutritional Predictors of Postoperative Outcome in Pancreatic Cancer. Br. J. Surg. 2011, 98, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Okumura, S.; Kaido, T.; Hamaguchi, Y.; Fujimoto, Y.; Masui, T.; Mizumoto, M.; Hammad, A.; Mori, A.; Takaori, K.; Uemoto, S. Impact of Preoperative Quality as Well as Quantity of Skeletal Muscle on Survival after Resection of Pancreatic Cancer. Surgery 2015, 157, 1088–1098. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Whole Cohort (n = 83) |
|---|---|
| Sex, male n, % | 45 (54%) |
| Female n,% | 38 (46%) |
| Age, median (IQR range), y | 69 (62–76) |
| IPMN type, n (%) | |
| MD_IPMNs | 40 (48%) |
| BD_IPMNs | 10 (12%) |
| Combined type_IPMNs | 33 (40%) |
| Surgical procedure n (%) | |
| Pancreaticoduodenectomy | 50 (60%) |
| Distal pancreatectomy + splenectomy | 22 (27%) |
| Spleen-preserving distal pancreatectomy | 7 (9%) |
| Central pancreatectomy | 1 (1%) |
| Total pancreatectomy | 1 (1%) |
| Tumor enucleation | 2 (2%) |
| Histological grade, n (%) | |
| Low-grade dysplasia | 30 (36%) |
| Intermediate dysplasia | 7 (8%) |
| High-grade dysplasia | 7 (8%) |
| Invasive carcinoma | 39 (47%) |
| High-risk stigmata n (%) | |
| Obstructive jaundice | 18 (22%) |
| Enhancing solid component | 47 (57%) |
| MPD ≥ 10 mm | 12 (14%) |
| Worrisome features n (%) | |
| Tumor ≥ 3 cm | 26 (31%) |
| Pancreatitis | 22 (27%) |
| Enhancing cyst wall | 23 (28%) |
| MPD 5–9 mm | 38 (46%) |
| Abrupt change in caliber of pancreatic duct with distal pancreatic atrophy | 39 (47%) |
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| Variables | Benign IPMNs (n = 37) | Malignant IPMNs (n = 46) | p Value | OR (95% CI) | p Value |
| Sex, male n (%) | 22 (59.46%) | 23 (50%) | 0.39 | NC | |
| Age, median (IQR) | 67.5 (62–73.5) | 71 (62–78) | 0.18 | NC | |
| Abdominal pain n (%) | 21 (56.76%) | 18 (39.13%) | 0.12 | NC | |
| Dyspepsia n (%) | 21 (56.76%) | 17 (36.96%) | 0.181 | NC | |
| Cephalic location n (%) | 27 (72.97%) | 27 (58.70%) | 0.175 | NC | |
| Compression syndrome n (%) | 13 (35.14%) | 7 (15.22%) | 0.093 | NC | |
| Tumor size cm, median (IQR) | 2 (1.8–3) | 2.8 (2–3.2) | 0.084 | NC | |
| MPD diameter mm, median (IQR) | 6 (3–8) | 7 (4–8) | 0.14 | NC | |
| Cyst diameter cm, median (IQR) | 3 (2–4) | 3 (2–4) | 0.69 | NC | |
| High-risk stigmata, n (%) | |||||
| Obstructive jaundice | 13 (35.14%) | 5 (10.87%) | 0.022 | 0.37 (0.08–0.158) | 0.18 |
| Enhancing mural nodule | 25 (67.57%) | 22 (47.83%) | 0.09 | NC | |
| MPD > 10 mm | 7 (18.92%) | 5 (10.87%) | 0.54 | NC | |
| Worrisome features, n (%) | |||||
| Cyst size > 3 cm | 12 (32.43%) | 14 (30.43%) | 0.97 | NC | |
| Pancreatitis | 13 (35.14%) | 9 (19.57%) | 0.27 | NC | |
| Enhancing cyst wall | 10 (27.03%) | 13 (28.26%) | 0.71 | NC | |
| MPD 5–10 mm | 17 (45.95%) | 21 (45.65%) | 0.96 | NC | |
| Abrupt change in caliber of pancreatic duct with distal pancreatic atrophy | 17 (45.95%) | 22 (47.83%) | 0.39 | NC | |
| CA19.9, median (IQR) | 4 (2–11) | 24 (4–253) | 0.42 | NC | |
| CEA, median (IQR) | 1 (0–3) | 2 (1–5) | 0.17 | NC | |
| mGps | NC | ||||
| 0 | 31 (83.78%) | 37 (80.43%) | 0.46 | ||
| 1 | 4 (10.81%) | 4 (8.70%) | 0.52 | ||
| 2 | 2 (5.41%) | 5 (10.87%) | 0.32 | ||
| NLR | NC | ||||
| <2.38 | 17 (45.95%) | 24 (52.17%) | 0.573 | ||
| >2.38 | 20 (54.05%) | 22 (47.83%) | |||
| PLR | NC | ||||
| <185.5 n % | 28 (75.68%) | 29 (63.04%) | 0.217 | ||
| ≥185.5 n % | 9 (24.32%) | 17 (36.96%) | |||
| CAR | |||||
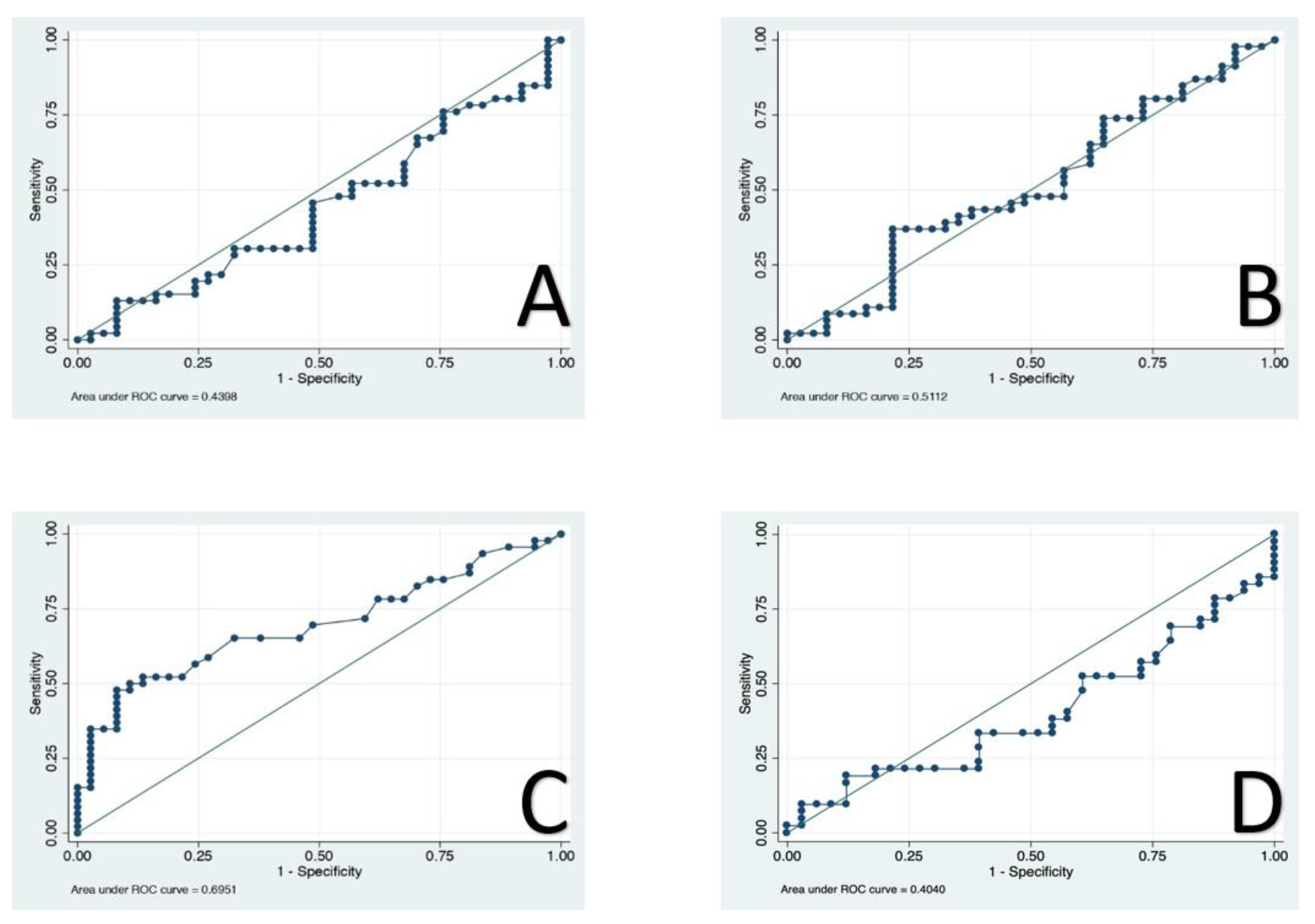
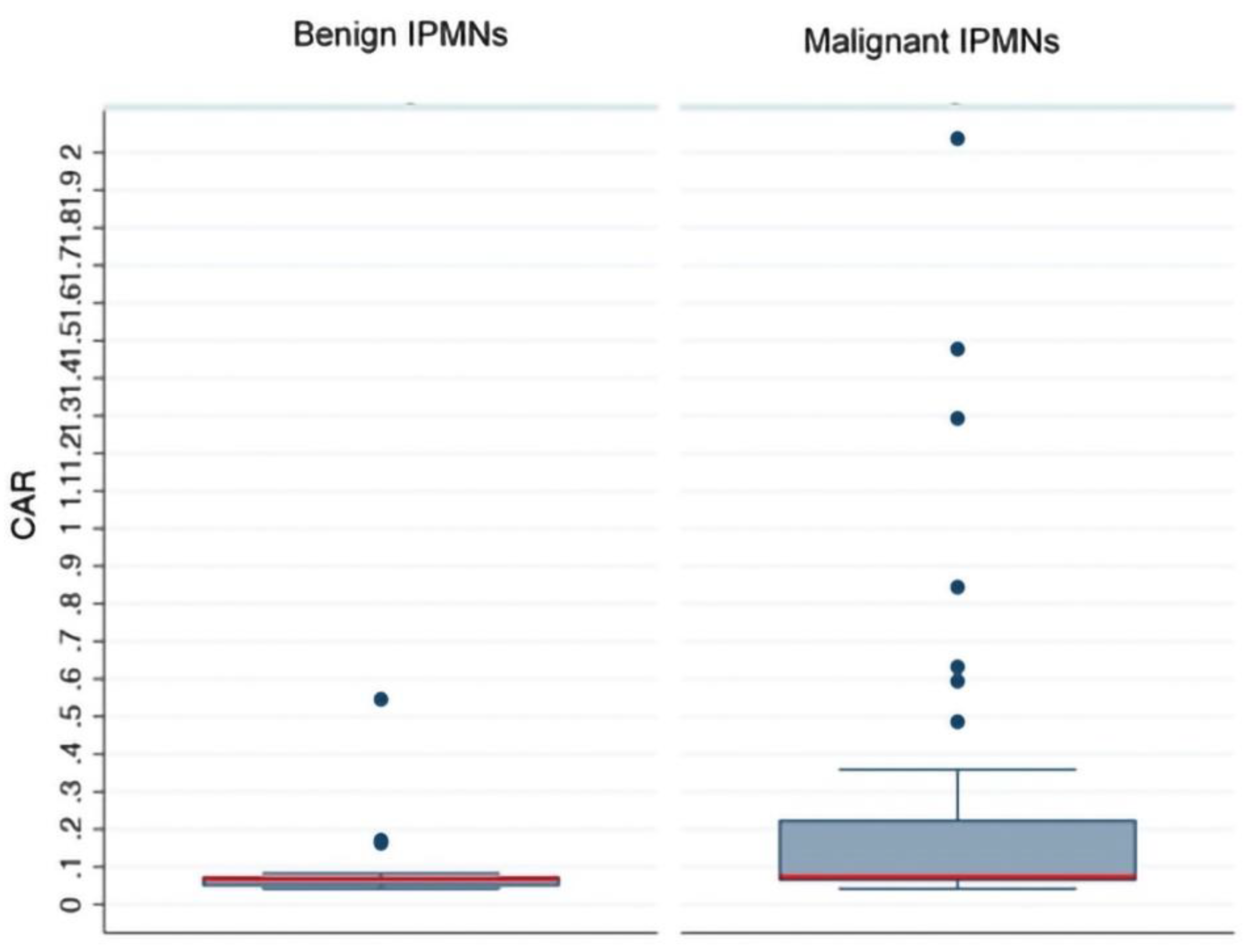
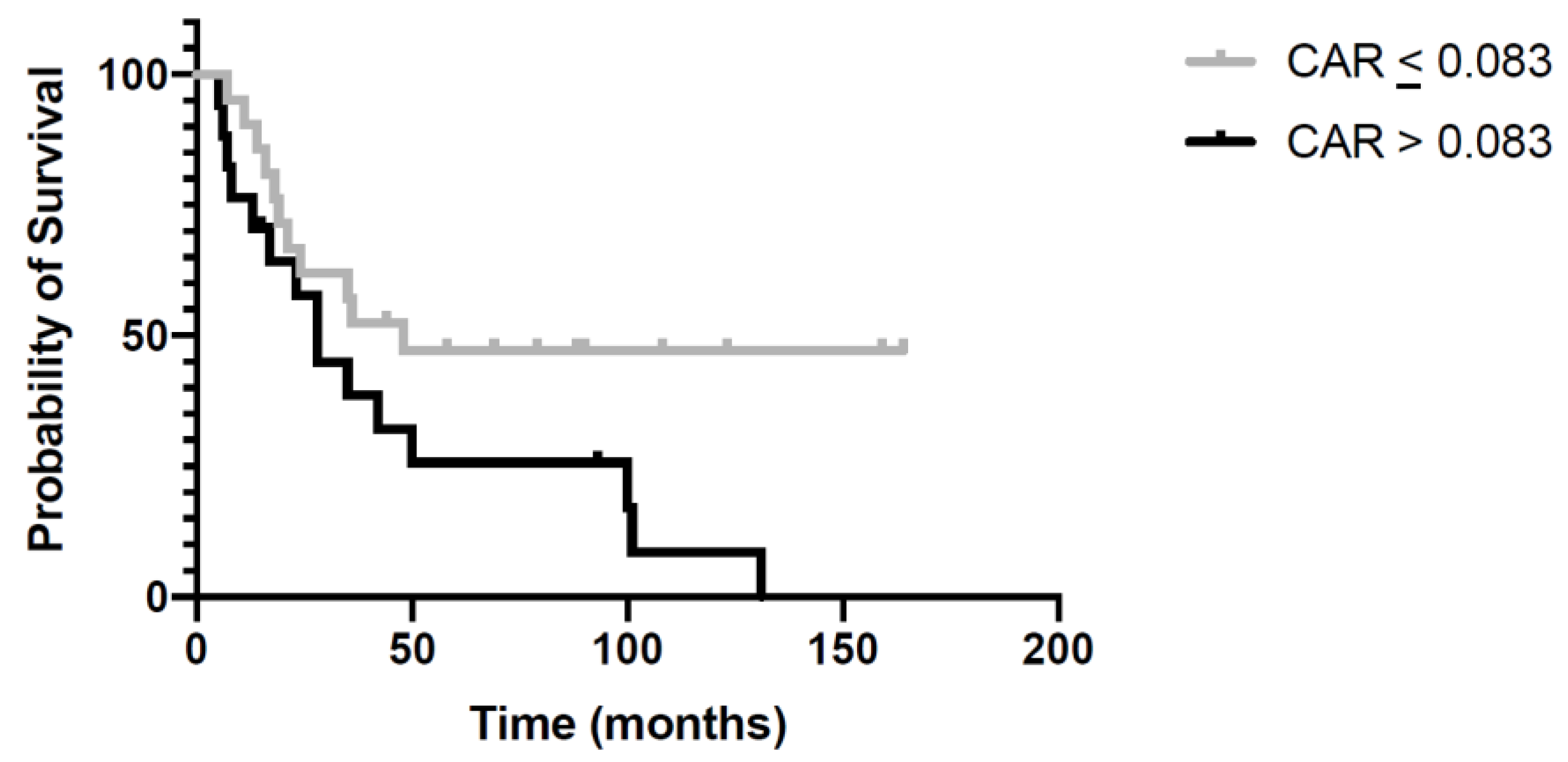
| <0.083 n % | 31 (83.78%) | 22 (47.83%) | 0.001 | 7.9 (2.01–31.83) | 0.003 |
| ≥0.083 n % | 6 (16.22%) | 24 (52.17%) | |||
| PNI | NC | ||||
| <42.05 n % | 14 (37.84%) | 26 (56.52%) | 0.15 | ||
| >42.05 n % | 23 (62.16%) | 20 (43.48%) | 0.07 | ||
| Variables | CAR ≤ 0.083 (n 53) | CAR ≥ 0.083 (n 30) | p Value |
|---|---|---|---|
| Sex, male n, % | 28 (52.83%) | 17 (56.67) | 0.46 |
| Age, median (IQR) | 69.5 (63–76.5) | 68 (61–75) | 0.42 |
| Abdominal pain n, % | 27 (50.94%) | 12 (41.38%) | 0.28 |
| Dyspepsia n, % | 28 (52.83%) | 10 (35.71%) | 0.11 |
| Cephalic location n, % | 36 (67.92%) | 18 (60%) | 0.31 |
| Compression syndrome n, % | 13 (25%) | 7 (25.93%) | 0.57 |
| Tumour size cm, median (IQR) | 3 (2–3.75) | 2.5 (1.8–3.3) | 0.06 |
| MPD diameter mm, median (IQR) | 6 (4–9) | 5.5 (3.5–7.5) | 0.12 |
| Cyst diameter cm, median (IQR) | 3 (2–4) | 2.6 (2–3.8) | 0.26 |
| High risk stigmata, n (%) | |||
| Obstructive jaundice | 12 (22.64%) | 6 (20%) | 0.5 |
| Enhancing mural nodule | 31 (62%) | 16 (53.33%) | 0.3 |
| MPD >10 mm | 10 (20.41%) | 2 (7.14%) | 0.11 |
| Worrisome features n (%) | |||
| Cyst size >3 cm | 20 (38.46%) | 6 (20.69%) | 0.08 |
| Pancreatitis | 15 (29.41%) | 7 (23.33%) | 0.37 |
| Enhancing cyst wall | 16 (31.37%) | 7 (25%) | 0.37 |
| MPD 5–10 mm | 22 (44.9%) | 16 (57.14%) | 0.21 |
| Abrupt change in calibre of pancreatic duct with distal pancreatic atrophy | 24 (48.98%) | 15 (53.57%) | 0.44 |
| CA19.9, median (IQR) | 8.5 (2–39) | 17.5 (3–107) | 0.24 |
| CEA, median (IQR) | 1 (0.4–3) | 2 (1–4.5) | 0.27 |
| Inflammatory biomarkers | |||
| Neutrophils, median (IQR) | 3.7 (2.9–4.7) | 3.55 (2.9–5.3) | 0.73 |
| Lymphocytes, median (IQR) | 1.5 (1.26–2.1) | 1.5 (1.2–1.9) | 0.62 |
| Platelets, median (IQR) | 223 (189–271) | 241 (192–296) | 0.48 |
| CRP, median (IQR) | 3 (2.9–5) | 3 (2–4) | 0.77 |
| Albumin, median (IQR) | 4.2 (4–4.4) | 4.2 (4.1–4.4) | 0.93 |
| PNI ≥ 42.05, n% | 4 (7.55%) | 4 (13.33%) | 0.31 |
| NLR ≥ 2.38, n% | 26 (49.86%) | 16 (53.33%) | 0.44 |
| PLR ≥ 185.5 n % | 13 (24.53%) | 13 (43.33%) | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serafini, S.; Friziero, A.; Sperti, C.; Vallese, L.; Grego, A.; Piangerelli, A.; Belluzzi, A.; Moletta, L. The Ratio of C-Reactive Protein to Albumin Is an Independent Predictor of Malignant Intraductal Papillary Mucinous Neoplasms of the Pancreas. J. Clin. Med. 2021, 10, 2058. https://doi.org/10.3390/jcm10102058
Serafini S, Friziero A, Sperti C, Vallese L, Grego A, Piangerelli A, Belluzzi A, Moletta L. The Ratio of C-Reactive Protein to Albumin Is an Independent Predictor of Malignant Intraductal Papillary Mucinous Neoplasms of the Pancreas. Journal of Clinical Medicine. 2021; 10(10):2058. https://doi.org/10.3390/jcm10102058
Chicago/Turabian StyleSerafini, Simone, Alberto Friziero, Cosimo Sperti, Lorenzo Vallese, Andrea Grego, Alfredo Piangerelli, Amanda Belluzzi, and Lucia Moletta. 2021. "The Ratio of C-Reactive Protein to Albumin Is an Independent Predictor of Malignant Intraductal Papillary Mucinous Neoplasms of the Pancreas" Journal of Clinical Medicine 10, no. 10: 2058. https://doi.org/10.3390/jcm10102058