
Outcome and Predictors for Mortality in Patients with Cardiogenic Shock: A Dutch Nationwide Registry-Based Study of 75,407 Patients with Acute Coronary Syndrome Treated by PCI

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.3. Statistical Analysis
3. Results
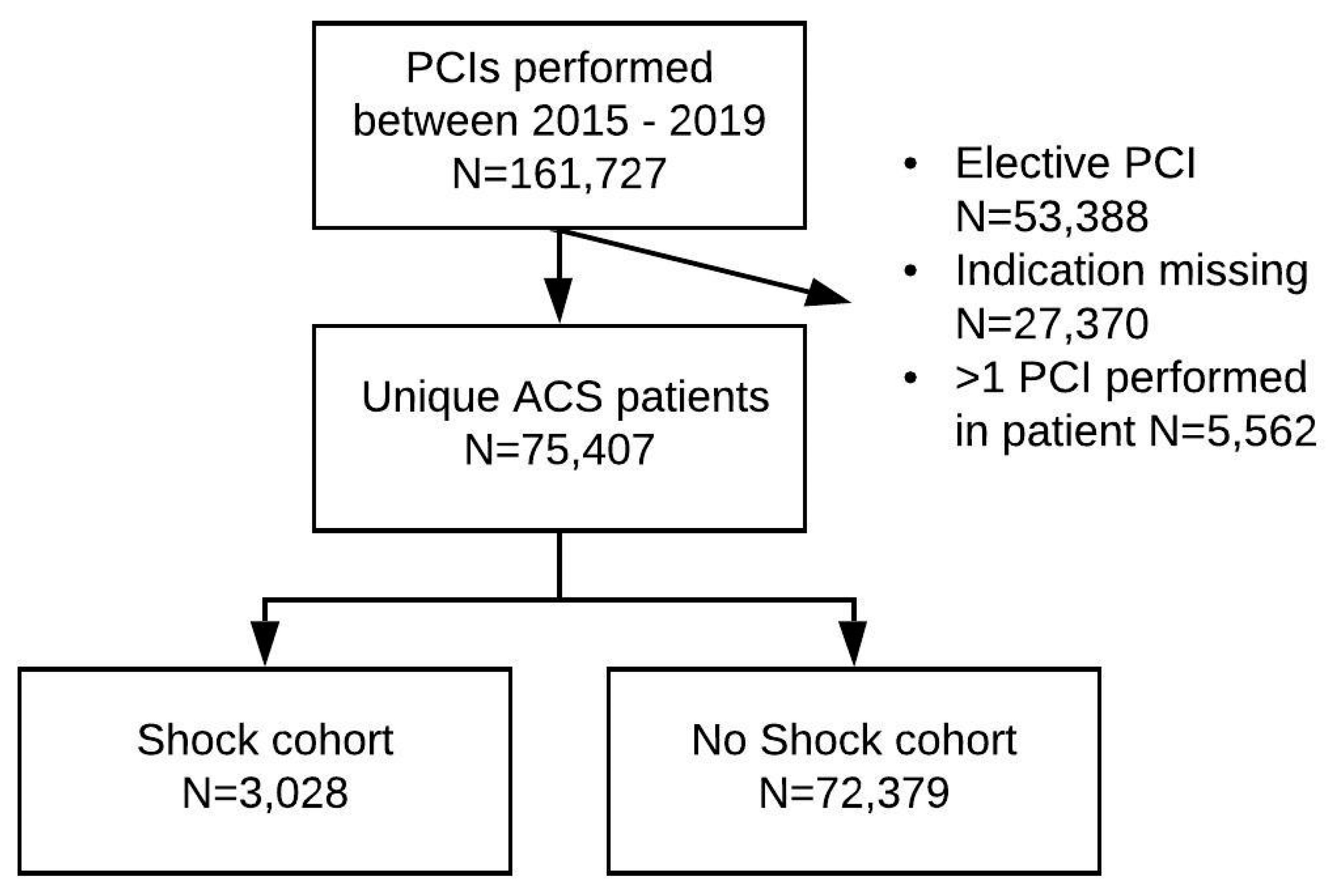
3.1. Study Population
3.2. Baseline Characteristics
3.3. Clinical Outcome
3.4. Predictors for Mortality in Cardiogenic Shock
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| G. | Amoroso | OLVG | |
| E.K. | Arkenbout | Tergooi | |
| S. | Aydin | VieCuri Medisch Centrum | |
| J. | Brouwer | Medisch Centrum Leeuwarden | |
| C. | Camaro | RadboudUMC | |
| J. | Daemen | Erasmus Medisch Centrum | |
| P. | Danse | Rijnstate | |
| S.F. | de la Fuente | Jeroen Bosch Ziekenhuis | |
| M. | van der | Ent | Maasstad Ziekenhuis |
| R. | Erdem | ZorgSaam | |
| P. | den | Heijer | Amphia |
| J.P.S. | Henriques | Amsterdam UMC, locatie AMC | |
| A.W.J. | van ‘t | Hof | Zuyderland MC |
| A.W.J. | van ‘t | Hof | Academisch Ziekenhuis Maastricht |
| I. | Karalis | Leids Universitair Medisch Centrum | |
| A. | Kraaijeveld | UMC Utrecht | |
| J.P. | van | Kuijk | Sint Antonius Ziekenhuis |
| E. | Lipsic | Universitair Medisch Centrum Groningen | |
| M. | Magro | Elisabeth-TweeSteden Ziekenhuis | |
| K.M.J. | Marques | Amsterdam UMC, locatie VUmc | |
| T. | Oude Ophuis | Canisius Wilhelmina Ziekenhuis | |
| J. | van | Ramshorst | Noordwest Ziekenhuisgroep |
| V. | Roolvink | Isala | |
| W.T. | Ruifrok | Treant Zorggroep | |
| M. | Scholte | Albert Schweitzer Ziekenhuis | |
| C.E. | Schotborgh | Haga Ziekenhuis | |
| B.J. | Sorgdrager | Haaglanden Medisch Centrum | |
| F. | Spano | Meander Medisch Centrum | |
| M.G. | Stoel | Medisch Spectrum Twente | |
| K. | Teeuwen | Catharina Ziekenhuis |
References
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Vahdatpour, C.; Collins, D.; Goldberg, S. Cardiogenic Shock. J. Am. Heart Assoc. 2019, 8, e011991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430); United Nations, Department of Economic and Social Affairs, Population Division: Washington, DC, USA, 2019. [Google Scholar]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Katus, H.A.; Apple, F.S.; Lindahl, B.; Morrow, D.A.; et al. Third Universal Definition of Myocardial Infarction. J. Am. Coll. Cardiol. 2012, 60, 1581–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunziker, L.; Radovanovic, D.; Jeger, R.; Pedrazzini, G.; Cuculi, F.; Urban, P.; Erne, P.; Rickli, H.; Pilgrim, T.; Hess, F.; et al. Twenty-Year Trends in the Incidence and Outcome of Cardiogenic Shock in AMIS Plus Registry. Circ. Cardiovasc. Interv. 2019, 12, e007293. [Google Scholar] [CrossRef] [PubMed]
- Redfors, B.; Angerås, O.; Råmunddal, T.; Dworeck, C.; Haraldsson, I.; Ioanes, D.; Petursson, P.; Libungan, B.; Odenstedt, J.; Stewart, J.; et al. 17-year trends in incidence and progno-sis of cardiogenic shock in patients with acute myocardial infarction in western Sweden. Int. J. Cardiol. 2015, 185, 256–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harjola, V.P.; Lassus, J.; Sionis, A.; Køber, L.; Tarvasmäki, T.; Spinar, J.; Parissis, J.; Banaszewski, M.; Silva-Cardoso, J.; Carubelli, V.; et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur. J. Heart Fail. 2015, 17, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Pöss, J.; Köster, J.; Fuernau, G.; Eitel, I.; de Waha, S.; Ouarrak, T.; Lassus, J.; Harjola, V.-P.; Zeymer, U.; Thiele, K.; et al. Risk Stratification for Patients in Cardiogenic Shock after Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2017, 69, 1913–1920. [Google Scholar] [CrossRef] [PubMed]
- Vora, A.N.; Wang, T.Y.; Hellkamp, A.S.; Thomas, L.; Henry, T.D.; Goyal, A.; Roe, M.T. Differences in Short- and Long-Term Outcomes Among Older Patients With ST-Elevation Versus Non–ST-Elevation Myocardial Infarction with Angiographically Proven Coronary Artery Disease. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 513–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, M.Y.; Sun, J.L.; Newby, L.K.; Shaw, L.K.; Lin, M.; Peterson, E.D.; Califf, R.M.; Kong, D.F.; Roe, M.T. Long-Term Mortality of Patients Undergoing Cardiac Catheterization for ST-Elevation and Non-ST-Elevation Myocardial Infarction. Circulationaha 2009, 119, 3110–3117. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients | Missing | Shock | No Shock | p-Value | |
|---|---|---|---|---|---|
| (n = 75,407) | (n = 3028) | (n = 72,379) | |||
| Clinical characteristics | |||||
| Age (years) | 65 ± 12 | 0 (-) | 66 ± 12 | 65 ± 12 | <0.001 |
| Male | 53,945 (72) | 0 (-) | 2158 (71) | 51,787 (72) | 0.74 |
| Diabetes mellitus | 13,957 (19) | 2084 (3) | 522 (18) | 13,435 (19) | 0.41 |
| Dialysis | 172 (0.5) | 42,701 (57) | 13 (0.9) | 159 (0.5) | 0.03 |
| Multivessel disease | 34,781 (46) | 523 (0.7) | 1770 (59) | 33,011 (46) | <0.001 |
| Chronic total occlusion | 1657 (2) | 1245 (2) | 90 (3) | 1567 (2) | <0.01 |
| Prior myocardial infarction | 13,588 (19) | 2137 (3) | 484 (17) | 13,104 (19) | 0.02 |
| Prior PCI | 8352 (19) | 31,815 (42) | 282 (15) | 8067 (19) | <0.001 |
| Prior CABG | 5136 (7) | 1162 (2) | 149 (5) | 4989 (7) | <0.001 |
| Out of hospital cardiac arrest | 4112 (5) | 94 (0.1) | 1373 (45) | 2739 (4) | <0.001 |
| Renal function (mL/min/1.73 m2) | 8207 (11) | <0.001 | |||
| eGFR ≥60 | 52,257 (78) | 1485 (56) | 50,772 (79) | ||
| eGFR 30–59 | 13,243 (20) | 1002 (38) | 12,241 (19) | ||
| eGFR 15–29 | 1205 (2) | 130 (5) | 1075 (2) | ||
| eGFR <15 | 495 (0.7) | 45 (2) | 450 (0.7) | ||
| LVEF | 51,820 (69) | <0.001 | |||
| >50% | 14,087 (60) | 161 (22) | 13,926 (61) | ||
| 30–50% | 7562 (32) | 319 (44) | 7243 (32) | ||
| ≤30% | 1938 (8) | 241 (33) | 1697 (7) | ||
| Treatment center | 0 (-) | <0.001 | |||
| Heart center | 49,396 (66) | 2133 (70) | 47,263 (65) | ||
| PCI center | 26,011 (35) | 895 (30) | 25,116 (35) | ||
| Procedure characteristics | |||||
| PCI indication | 0 (-) | <0.001 | |||
| STEMI | 36,288 (48) | 2704 (89) | 33,584 (46) | ||
| NSTEMI | 39,119 (52) | 324 (11) | 38,795 (54) | ||
| Culprit lesion | 37,340 (50) | 0.02 | |||
| LAD | 15,425 (41) | 619 (38) | 14,806 (41) | ||
| Other | 22,642 (60) | 1018 (62) | 21,624 (60) | ||
| PCI access method (1st) | 41,448 (55) | <0.001 | |||
| Radial | 28,172 (83) | 671 (50) | 27,501 (84) | ||
| Femoral | 5704 (17) | 681 (50) | 5023 (15) | ||
| Brachial | 83 (0.2) | 4 (0.3) | 79 (0.2) | ||
| Culprit lesion PCI | 25,477 (67) | 37,327 (50) | 1034 (63) | 24,443 (67) | <0.01 |
| Multivessel PCI | 12,603 (33) | 37,327 (50) | 603 (37) | 12,000 (33) | <0.01 |
| Clinical outcome | |||||
| 30-day mortality | 2722 (4) | 462 (0.6) | 1080 (36) | 1642 (2) | <0.001 |
| 1-year mortality * | 3346 (6) | 228 (0.4) | 855 (40) | 2491 (5) | <0.001 |
| Urgent CABG within 1 day | 206 (0.3) | 2002 (3) | 38 (1) | 168 (0.2) | <0.001 |
| MI within 30 days | 393 (0.7) | 22,619 (30) | 27 (1) | 366 (0.7) | <0.01 |
| TVR within 1 year * | 2256 (5) | 12,099 (22) | 71 (5) | 2256 (5) | 0.16 |
| HR | Univariable | p-Value | HR | Multivariable | p-Value | |
|---|---|---|---|---|---|---|
| 95% CI | 95% CI | |||||
| Age (years) | 1.03 | 1.02–1.03 | <0.001 | 1.02 | 1.02–1.03 | <0.001 |
| Male | 0.13 | 0.77–0.97 | 0.01 | 0.97 | 0.84–1.11 | 0.62 |
| Diabetes mellitus | 1.57 | 1.38–1.80 | <0.001 | 1.25 | 1.08–1.45 | <0.01 |
| Multivessel disease | 1.52 | 1.35–1.71 | <0.001 | 1.22 | 1.06–1.39 | <0.01 |
| CTO | 1.29 | 0.96–1.74 | 0.09 | 1.16 | 0.82–1.64 | 0.39 |
| Prior MI | 1.36 | 1.18–1.56 | <0.001 | 1.24 | 1.06–1.45 | <0.01 |
| Prior CABG | 1.32 | 1.05–1.65 | 0.02 | 0.93 | 0.72–1.21 | 0.59 |
| eGFR (mL/min/1.73 m2) | 0.98 | 0.98–0.98 | <0.001 | 0.98 | 0.98–0.99 | <0.001 |
| OHCA | 1.44 | 1.29–1.60 | <0.001 | 1.71 | 1.50–1.94 | <0.001 |
| STEMI | 0.79 | 0.67–0.93 | <0.01 | 0.88 | 0.74–1.06 | 0.18 |
| PCI center | 0.95 | 0.84–1.07 | 0.41 | |||
| Intervention year | ||||||
| 2015 | 1.14 | 0.97–1.32 | 0.11 | 1.14 | 0.95–1.35 | 0.15 |
| 2016 | 1.19 | 1.02–1.40 | 0.03 | 1.08 | 0.91–1.30 | 0.38 |
| 2017 | 1.08 | 0.93–1.26 | 0.33 | 1.18 | 0.99–1.42 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karami, M.; Peters, E.J.; Lagrand, W.K.; Houterman, S.; den Uil, C.A.; Engström, A.E.; Otterspoor, L.C.; Ottevanger, J.P.; Ferreira, I.A.; Montero-Cabezas, J.M.; et al. Outcome and Predictors for Mortality in Patients with Cardiogenic Shock: A Dutch Nationwide Registry-Based Study of 75,407 Patients with Acute Coronary Syndrome Treated by PCI. J. Clin. Med. 2021, 10, 2047. https://doi.org/10.3390/jcm10102047
Karami M, Peters EJ, Lagrand WK, Houterman S, den Uil CA, Engström AE, Otterspoor LC, Ottevanger JP, Ferreira IA, Montero-Cabezas JM, et al. Outcome and Predictors for Mortality in Patients with Cardiogenic Shock: A Dutch Nationwide Registry-Based Study of 75,407 Patients with Acute Coronary Syndrome Treated by PCI. Journal of Clinical Medicine. 2021; 10(10):2047. https://doi.org/10.3390/jcm10102047
Chicago/Turabian StyleKarami, Mina, Elma J. Peters, Wim K. Lagrand, Saskia Houterman, Corstiaan A. den Uil, Annemarie E. Engström, Luuk C. Otterspoor, Jan Paul Ottevanger, Irlando A. Ferreira, Jose M. Montero-Cabezas, and et al. 2021. "Outcome and Predictors for Mortality in Patients with Cardiogenic Shock: A Dutch Nationwide Registry-Based Study of 75,407 Patients with Acute Coronary Syndrome Treated by PCI" Journal of Clinical Medicine 10, no. 10: 2047. https://doi.org/10.3390/jcm10102047