
Longitudinal Analysis and Comparison of Six Serological Assays up to Eight Months Post-COVID-19 Diagnosis


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Cohort
2.2. Serological Assays
2.3. Neutralization Assay
2.4. Data Analysis and Statistical Analyses
3. Results
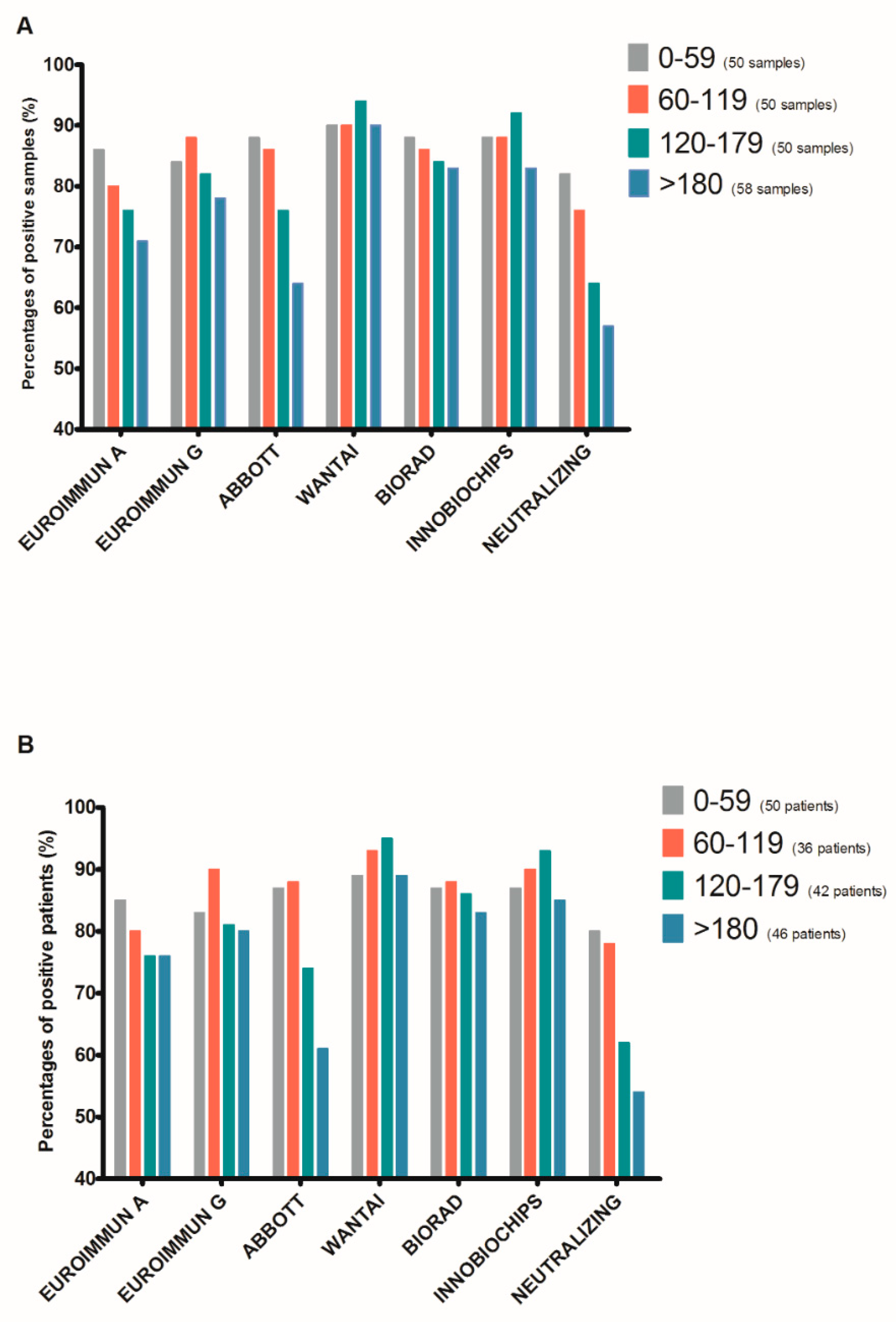
3.1. Head-to Head-Comparison of Serological and Neutralizing Assays
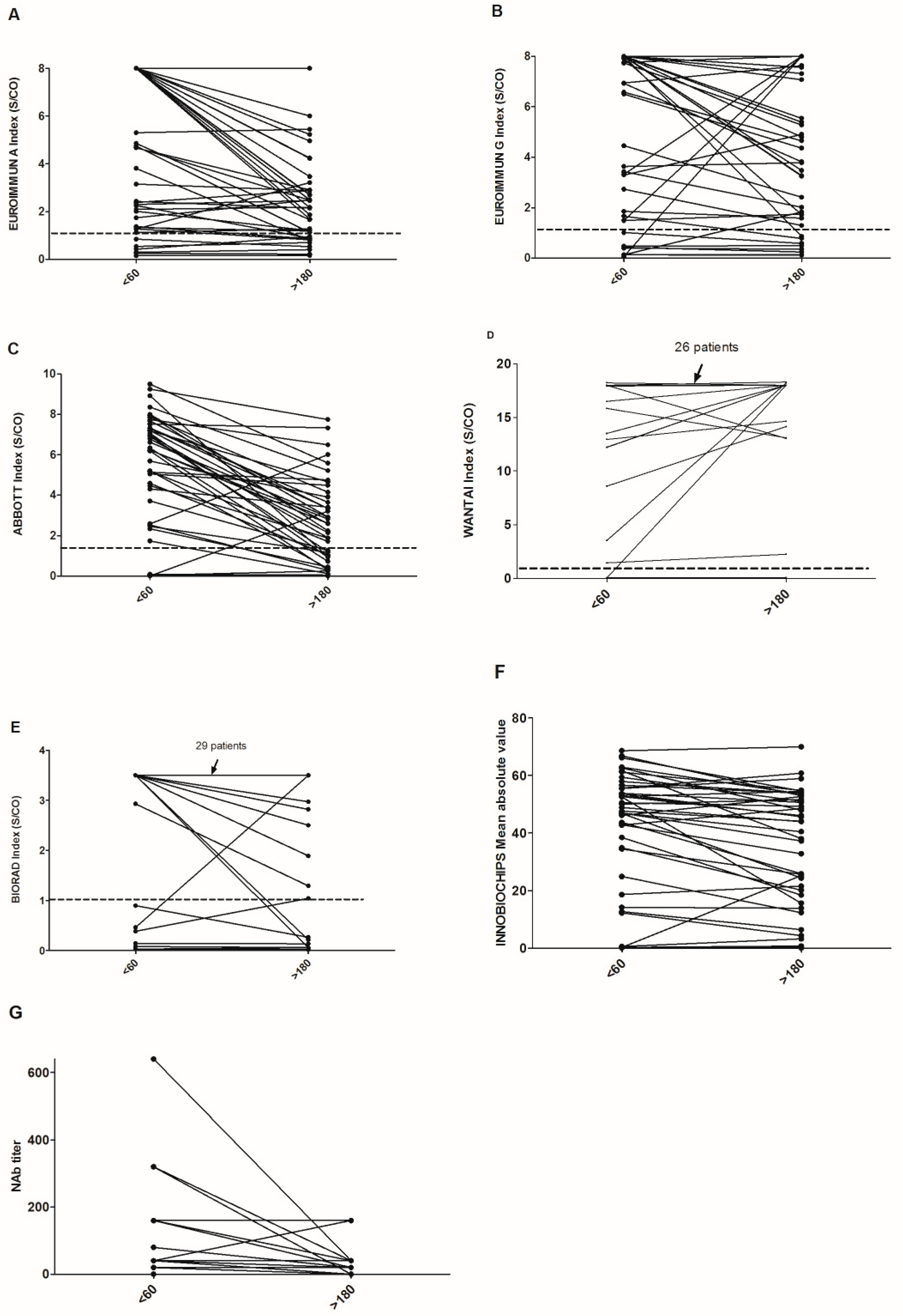
3.2. Decline of Antibody Levels Six Months Postdiagnosis
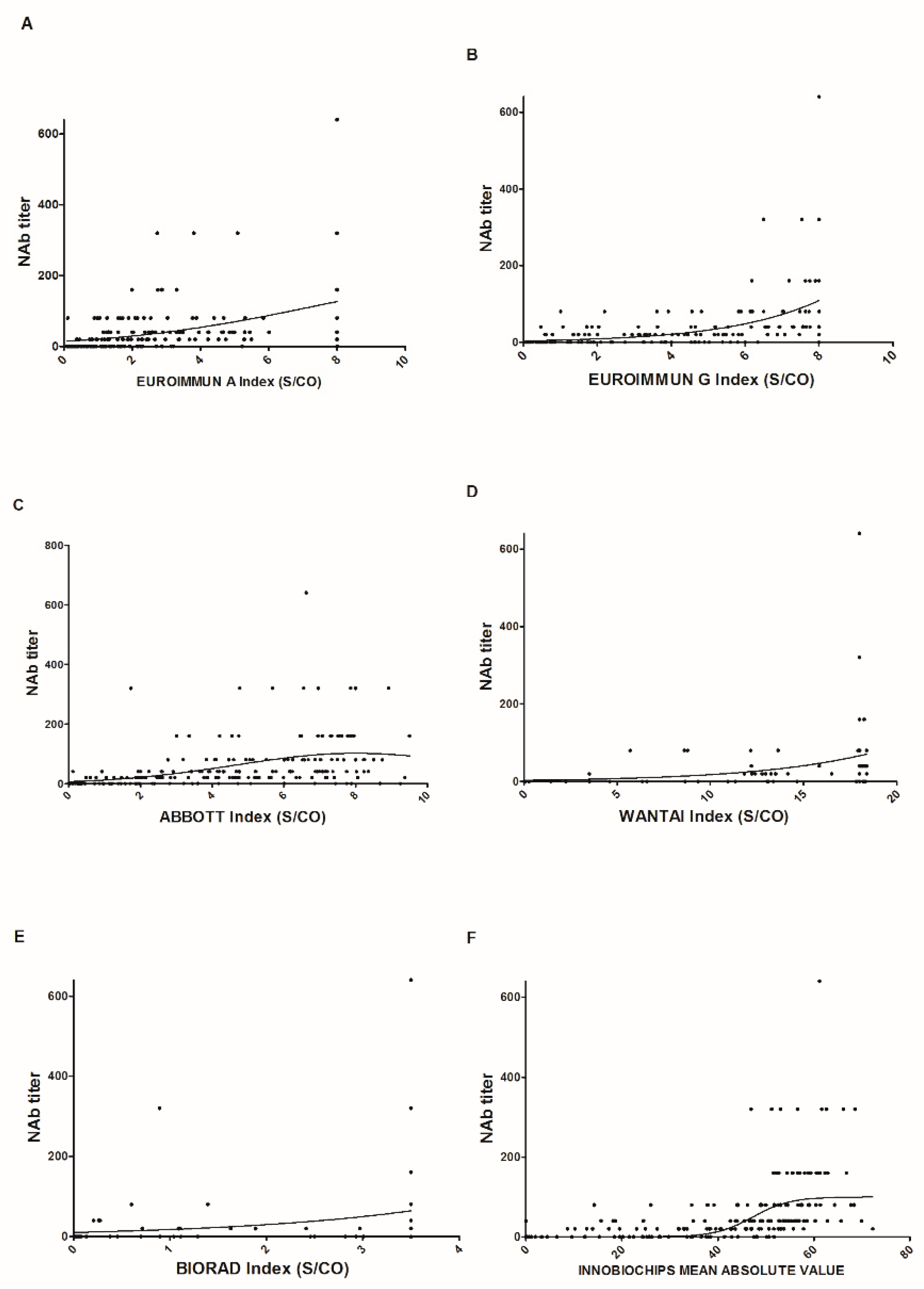
3.3. Link Between Neutralizing Titer and Serological Assays
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Brochot, E.; Demey, B.; Touzé, A.; Belouzard, S.; Dubuisson, J.; Schmit, J.-L.; Duverlie, G.; Francois, C.; Castelain, S.; Helle, F. Anti-spike, Anti-nucleocapsid and Neutralizing Antibodies in SARS-CoV-2 Inpatients and Asymptomatic Individuals. Front. Microbiol. 2020, 11, 584251. [Google Scholar] [CrossRef] [PubMed]
- Demey, B.; Daher, N.; François, C.; Lanoix, J.-P.; Duverlie, G.; Castelain, S.; Brochot, E. Dynamic profile for the detection of anti-SARS-CoV-2 antibodies using four immunochromatographic assays. J. Infect. 2020, 81, e6–e10. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Feng, Y.; Mo, X.; Zheng, P.; Wang, Q.; Li, P.; Peng, P.; Liu, X.; Chen, Z.; Huang, H.; et al. Kinetics of SARS-CoV-2 specific IgM and IgG responses in COVID-19 patients. Emerg. Microbes Infect. 2020, 9, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, L.; Sang, L.; Ye, F.; Ruan, S.; Zhong, B.; Song, T.; Alshukairi, A.N.; Chen, R.; Zhang, Z.; et al. Kinetics of viral load and antibody response in relation to COVID-19 severity. J. Clin. Investig. 2020, 130, 5235–5244. [Google Scholar] [CrossRef] [PubMed]
- Brochot, E.; Demey, B.; Handala, L.; François, C.; Duverlie, G.; Castelain, S. Comparison of different serological assays for SARS-CoV-2 in real life. J. Clin. Virol. 2020, 130, 104569. [Google Scholar] [CrossRef] [PubMed]
- Oved, K.; Olmer, L.; Shemer-Avni, Y.; Wolf, T.; Supino-Rosin, L.; Prajgrod, G.; Shenhar, Y.; Payorsky, I.; Cohen, Y.; Kohn, Y.; et al. Multi-center nationwide comparison of seven serology assays reveals a SARS-CoV-2 non-responding seronegative subpopulation. EClinicalMedicine 2020, 29, 100651. [Google Scholar] [CrossRef] [PubMed]
- Klingler, J.; Weiss, S.; Itri, V.; Liu, X.; Oguntuyo, K.Y.; Stevens, C.; Ikegame, S.; Hung, C.-T.; Enyindah-Asonye, G.; Amanat, F.; et al. Role of IgM and IgA Antibodies in the Neutralization of SARS-CoV-2. medRxiv 2020. [Google Scholar] [CrossRef]
- Trabaud, M.-A.; Icard, V.; Milon, M.-P.; Bal, A.; Lina, B.; Escuret, V. Comparison of eight commercial, high-throughput, automated or ELISA assays detecting SARS-CoV-2 IgG or total antibody. J. Clin. Virol. 2020, 132, 104613. [Google Scholar] [CrossRef] [PubMed]
- Bal, A.; Pozzetto, B.; Trabaud, M.-A.; Escuret, V.; Rabilloud, M.; Langlois-Jacques, C.; Paul, A.; Guibert, N.; D’Aubarede-Frieh, C.; Massardier-Pilonchery, A.; et al. Evaluation of high-throughput SARS-CoV-2 serological assays in a longitudinal cohort of patients with mild COVID-19: Clinical sensitivity, specificity and association with virus neutralization test. Clin. Chem. 2021, 5. [Google Scholar] [CrossRef]
- Neto, O.P.; Kennedy, D.M.; Reis, J.C.; Wang, Y.; Brizzi AC, B.; Zambrano, G.J.; de Souza, J.M.; Pedroso, W.; de Mello Pedreiro, R.C.; de Matos Brizzi, B.; et al. Mathematical model of COVID-19 intervention scenarios for São Paulo-Brazil. Nat. Commun. 2021, 12, 1–13. [Google Scholar]
- Buss, L.F.; Prete, C.A.; Abrahim, C.M.M.; Mendrone, A.; Salomon, T.; de Almeida-Neto, C.; Franca, R.F.O.; Belotti, M.C.; Carvalho, M.P.S.S.; Costa, A.G.; et al. Three-quarters attack rate of SARS-CoV-2 in the Brazilian Amazon during a largely unmitigated epidemic. Science 2021, 371, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Belda, A.B.; Fernández-Garcés, M.; Mateo-Sanchis, E.; Madrazo, M.; Carmona, M.; Piles-Roger, L.; Artero, A. COVID -19 in older adults: What are the differences with younger patients? Geriatr. Gerontol. Int. 2021, 21, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to eight months after infection. Science 2021, 371. [Google Scholar] [CrossRef] [PubMed]
- Tarke, A.; Sidney, J.; Kidd, C.K.; Dan, J.M.; Ramirez, S.I.; Yu, E.D.; Mateus, J.; da Silva Antunes, R.; Moore, E.; Rubiro, P.; et al. Comprehensive analysis of T cell immunodominance and immunoprevalence of SARS-CoV-2 epitopes in COVID-19 cases. Cell Rep. Med. 2021, 2, 100204. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, K.R.; Rennick, L.J.; Nambulli, S.; Robinson-McCarthy, L.R.; Bain, W.G.; Haidar, G.; Duprex, W.P. Recurrent deletions in the SARS-CoV-2 spike glycoprotein drive antibody escape. Science 2021, 371, 1139–1142. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Number of patients | 61 |
| Female | 36 |
| Male | 25 |
| Age (Years): | |
| Median | 74 |
| Range | 26–98 |
| >65 years | 41 |
| Hospitalized patients | 27 |
| Nonhospitalized patients | 34 |
| Immunocompromised patients | 6 (2 kidney transplant, 2 bone marrow transplant, 2 chemotherapy |
| Numbers of samples (days post-PCR): | |
| 0–59 | 50 |
| 60–119 | 50 |
| 120–179 | 50 |
| ≥180 | 58 |
| (range: 180–237) | |
| Numbers of patients (days post-PCR): | |
| 0–59 | 50 |
| 60–119 | 36 |
| 120–179 | 42 |
| ≥180 | 46 |
| Serological Assay | All | Female | Male | p-Value | Inpatients | Outpatients | p Value | >65 | ≤65 | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| EUROIMMUN A | 24 | 27 | 20 | 0.58 | 9 | 37 | 0.02 | 23 | 25 | 0.9 |
| EUROIMMUN G | 20 | 19 | 20 | 0.94 | 9 | 29 | 0.09 | 13 | 31 | 0.14 |
| ABBOTT | 39 | 42 | 35 | 0.61 | 36 | 42 | 0.71 | 27 | 62 | 0.02 |
| WANTAI | 11 | 15 | 10 | 0.26 | 5 | 17 | 0.19 | 7 | 19 | 0.21 |
| BIORAD | 17 | 23 | 10 | 0.24 | 14 | 21 | 0.52 | 10 | 31 | 0.07 |
| INNOBIOCHIPS | 15 | 19 | 10 | 0.74 | 5 | 25 | 0.05 | 10 | 25 | 0.18 |
| Neutralizing antibodies (titer = 0) | 46 | 50 | 40 | 0.49 | 41 | 50 | 0.53 | 47 | 44 | 0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aubry, A.; Demey, B.; François, C.; Duverlie, G.; Castelain, S.; Helle, F.; Brochot, E. Longitudinal Analysis and Comparison of Six Serological Assays up to Eight Months Post-COVID-19 Diagnosis. J. Clin. Med. 2021, 10, 1815. https://doi.org/10.3390/jcm10091815
Aubry A, Demey B, François C, Duverlie G, Castelain S, Helle F, Brochot E. Longitudinal Analysis and Comparison of Six Serological Assays up to Eight Months Post-COVID-19 Diagnosis. Journal of Clinical Medicine. 2021; 10(9):1815. https://doi.org/10.3390/jcm10091815
Chicago/Turabian StyleAubry, Aurélien, Baptiste Demey, Catherine François, Gilles Duverlie, Sandrine Castelain, François Helle, and Etienne Brochot. 2021. "Longitudinal Analysis and Comparison of Six Serological Assays up to Eight Months Post-COVID-19 Diagnosis" Journal of Clinical Medicine 10, no. 9: 1815. https://doi.org/10.3390/jcm10091815