
Oral Manifestations in Melanoma Patients Treated with Target or Immunomodulatory Therapies

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- PUBMED
- Ovid MEDLINE
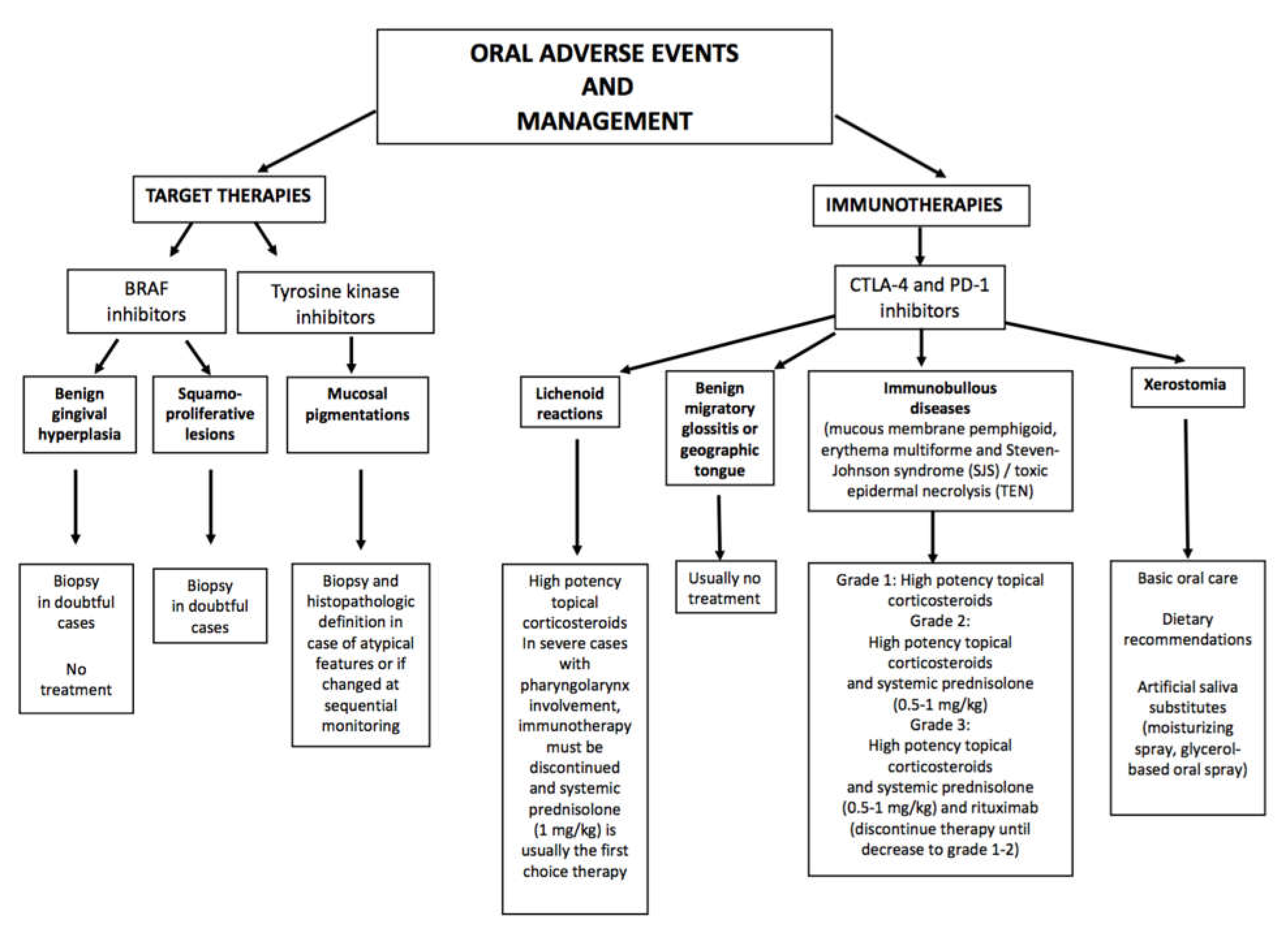
3. Target Therapies with BRAF and MEK Inhibitors and Tyrosine Kinase Inhibitors
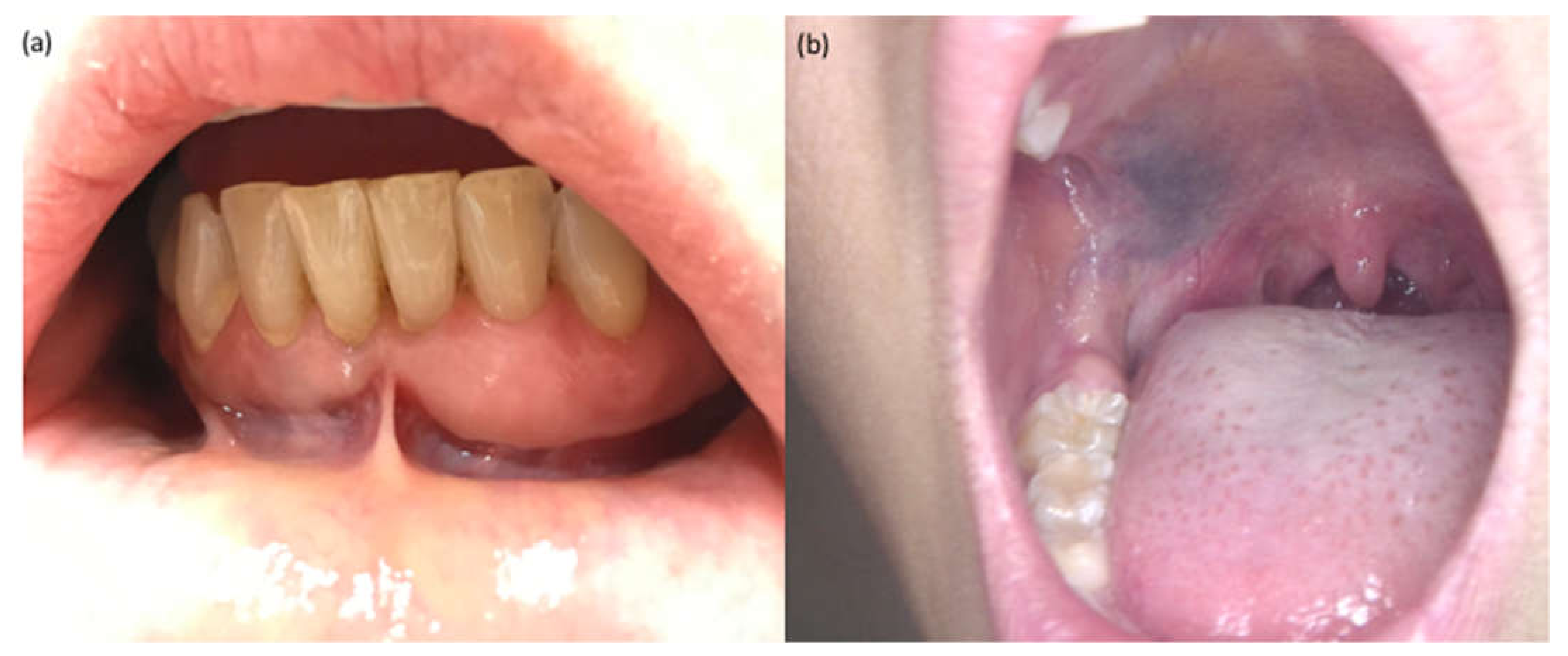
3.1. Gingival Hyperplasia
3.2. Pigmentation Disorders
3.3. Squamoproliferative Lesions
4. Immunotherapies with CTLA-4 or PD1 Inhibitors
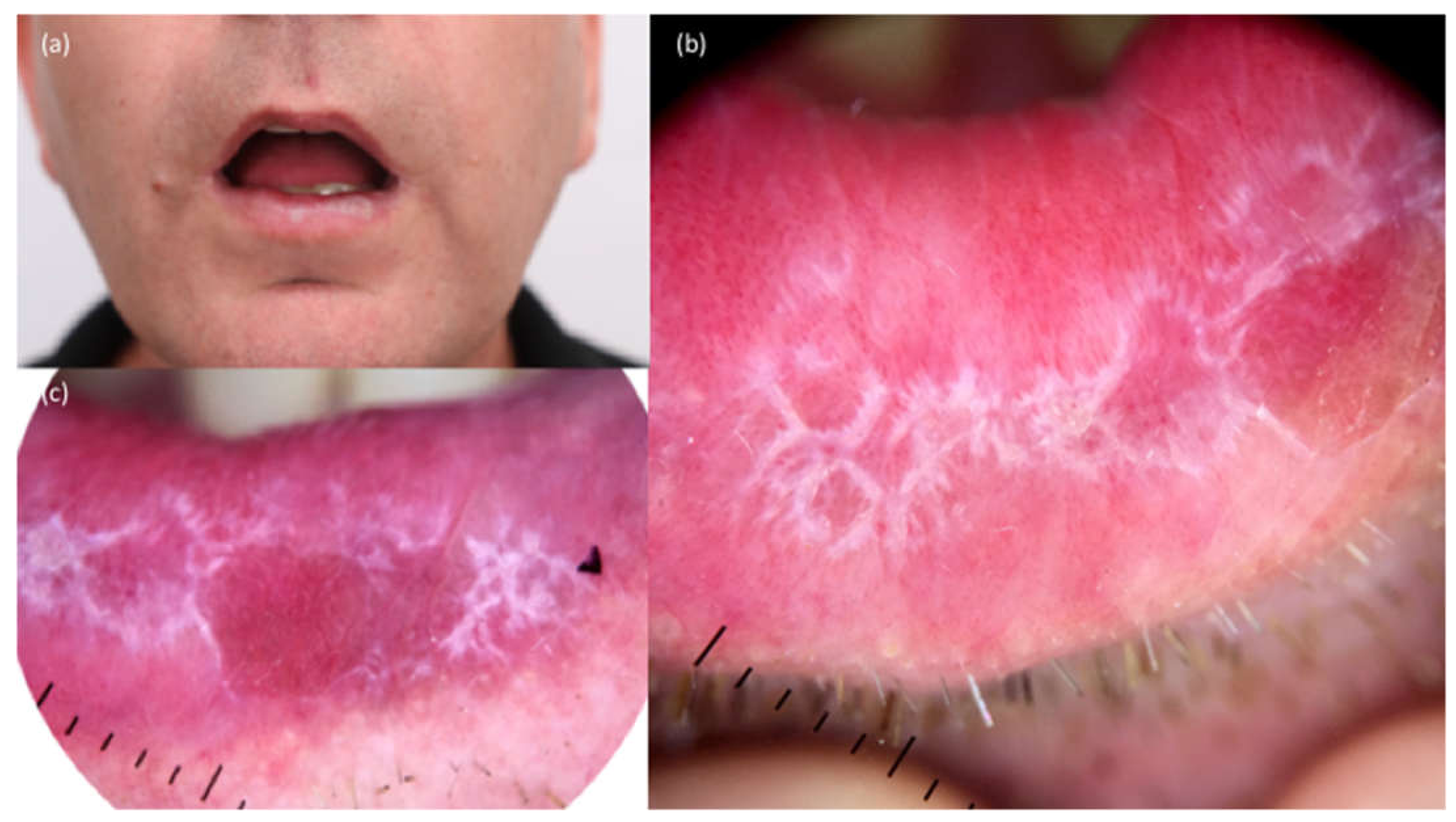
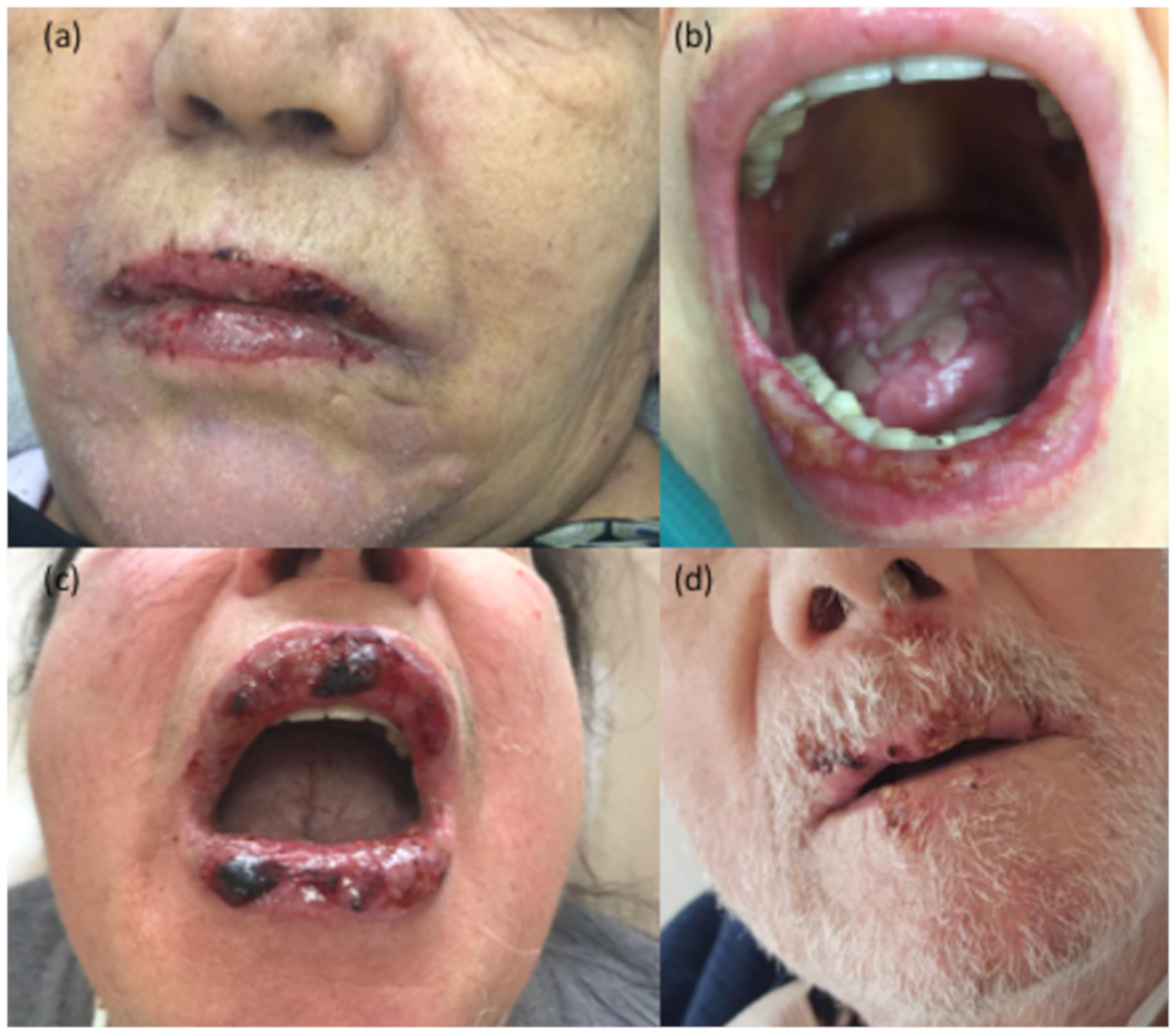
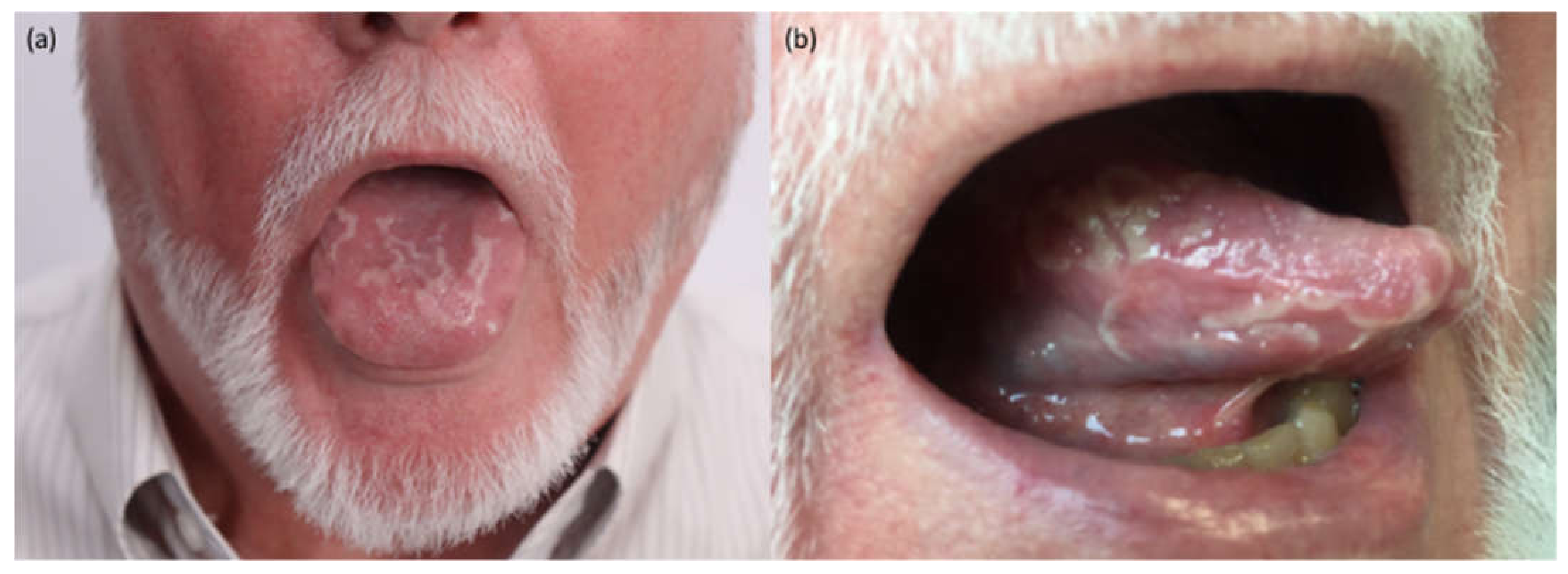
4.1. Lichenoid Reactions
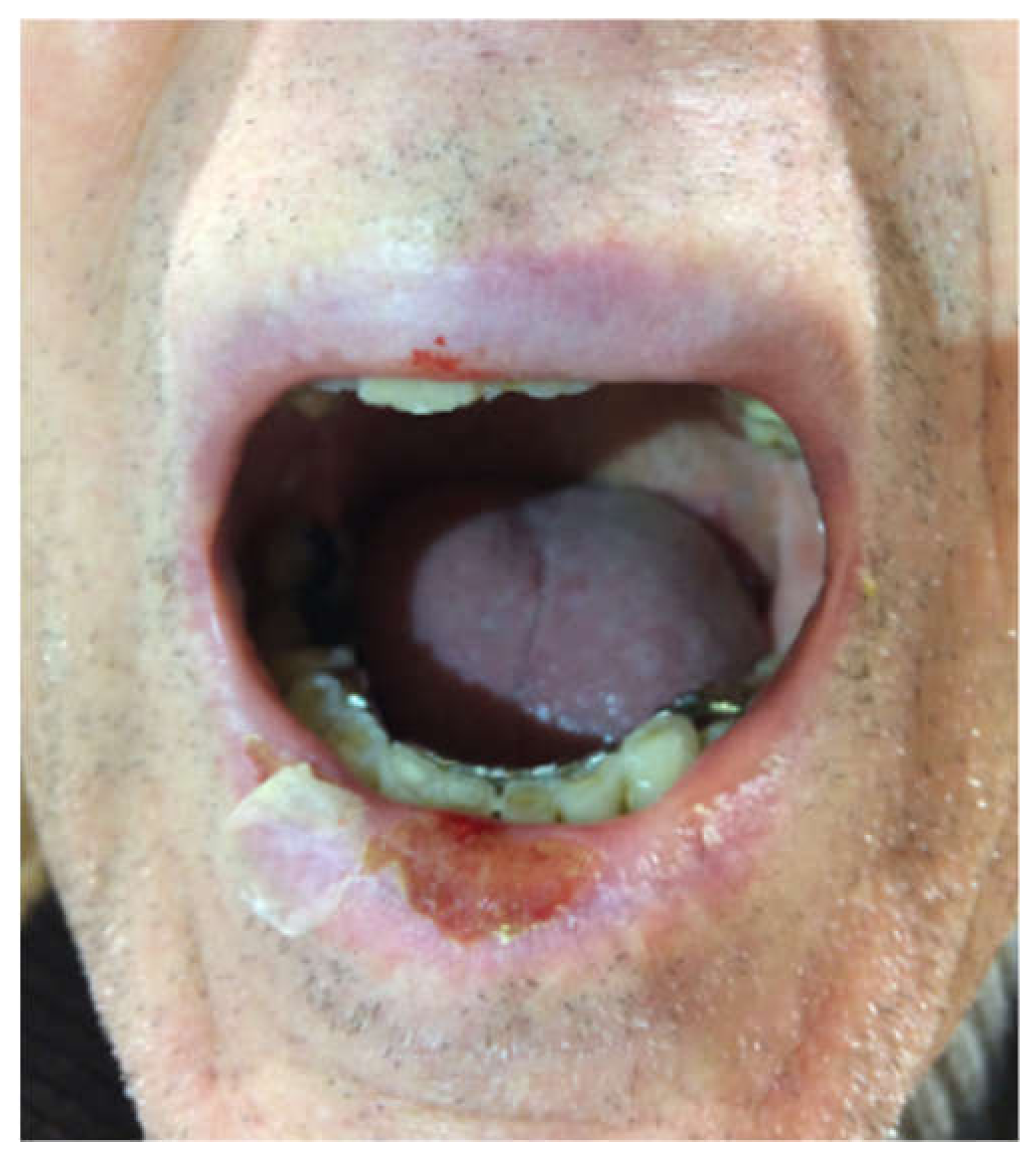
4.2. Immunobullous Reactions
4.3. Xerostomia
4.4. Other Reactions
5. Study Limitations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spain, L.; Larkin, J.; Turajlic, S. New survival standards for advanced melanoma. Br. J. Cancer 2020, 122, 1275–1276. [Google Scholar] [CrossRef] [PubMed]
- Mangold, A.R.; Bryce, A.H.; Sekulić, A. Vemurafenib-associated gingival hyperplasia in patient with metastatic melanoma. J. Am. Acad. Dermatol. 2014, 71, e205–e206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nava, C.; Hanna, N.; Michot, C.; Pereira, S.; Pouvreau, N.; Niihori, T.; Aoki, Y.; Matsubara, Y.; Arveiler, B.; Lacombe, D.; et al. Cardio-facio-cutaneous and Noonan syndromes due to mutations in the RAS/MAPK signalling pathway: Genotype phenotype relationships and overlap with Costello syndrome. J. Med Genet. 2007, 44, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Vigarios, E.; Epstein, J.B.; Sibaud, V. Oral mucosal changes induced by anticancer targeted therapies and immune checkpoint inhibitors. Support Care Cancer 2017, 25, 1713–1739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gripp, K.W.; Lin, A.E.; Nicholson, L.; Allen, W.; Cramer, A.; Jones, K.L.; Kutz, W.; Peck, D.; Rebolledo, M.A.; Wheeler, P.G.; et al. Further delineation of the phenotype resulting from BRAF or MEK1 germline mutations helps differentiate cardio-facio-cutaneous syndrome from Costello syndrome. Am. J. Med Genet. Part A 2007, 143, 1472–1480. [Google Scholar] [CrossRef] [PubMed]
- Pastor, P.J.A.; Vera, P.J.B.; Illueca, F.M.A.; Pizarro, M.C. Hereditary gingival fibromatosis: Characteristics and treatment approach. J. Clin. Exp. Dent. 2017, 9, e599–e602. [Google Scholar] [CrossRef] [Green Version]
- Häkkinen, L.; Csiszar, A. Hereditary Gingival Fibromatosis: Characteristics and Novel Putative Pathogenic Mechanisms. J. Dent. Res. 2007, 86, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, K.T.; Infante, J.R.; Daud, A.; Gonzalez, R.; Kefford, R.F.; Sosman, J.; Hamid, O.; Schuchter, L.; Cebon, K.; Ibrahim, N.; et al. Combined BRAF and MEK inhibition in melanoma with BRAF V600 mutations. New Engl. J. Med. 2012, 367, 1694–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, E.; Zimmer, L.; Vaubel, J.; Schadendorf, D. BRAF, MEK and KIT inhibitors for melanoma: Adverse events and their management. Chin. Clin. Oncol. 2014, 3, 29. [Google Scholar]
- Larkin, J.; Ascierto, P.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Maio, M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Combined Vemurafenib and Cobimetinib in BRAF-Mutated Melanoma. N. Engl. J. Med. 2014, 371, 1867–1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schadendorf, D.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Chiarion-Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; Haydon, A.; et al. Patient-reported outcomes in patients with resected, high-risk melanoma with BRAFV600E or BRAFV600K mutations treated with adjuvant dabrafenib plus trametinib (COMBI-AD): A randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 701–710. [Google Scholar] [CrossRef]
- Lueken, N.; Kaune, K.M.; Zutt, M. A Large Gray–Blue Macule on the Hard Palate as an Adverse Effect of Imatinib. Dtsch. Ärzteblatt Int. 2019, 116, 95. [Google Scholar] [CrossRef]
- Lyne, A.; Creedon, A.; Bailey, B.M.W. Mucosal pigmentation of the hard palate in a patient taking imatinib. BMJ Case Rep. 2015, 2015, bcr2015209335. [Google Scholar] [CrossRef] [Green Version]
- Lambertini, M.; Patrizi, A.; Ravaioli, G.M.; Dika, E. Oral pigmentation in physiologic conditions, post-inflammatory affections and systemic diseases. G. Ital. Di Dermatol. E Venereol. 2018, 153, 666–671. [Google Scholar] [CrossRef]
- Oliveira, S.R.; de Azevedo Branco, L.G.; Rocha, A.L.; Travassos, D.V.; Magalhães GH, R.; Fonseca, F.P.; Mesquita, R.A.; Abreu, L.G.; da Silva, T.A. Association of oral mucosa hyperpigmentation with imatinib mesylate use: A cross-sectional study and a systematic literature review. Clin. Oral Investig. 2019, 23, 4371–4382. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Patrizi, A.; Fanti, P.; Melotti, B.; Caliceti, U.; Magnoni, C.; Misciali, C.; Baraldi, C.; Ravaioli, G.; Dika, E. Oral melanoma and other pigmentations: When to biopsy? J. Eur. Acad. Dermatol. Venereol. 2017, 32, 209–214. [Google Scholar] [CrossRef]
- Dika, E.; Starace, M.; Lambertini, M.; Patrizi, A.; Veronesi, G.; Alessandrini, A.; Piraccini, B.M. Oral and nail pigmentations: A useful parallelism for the clinician. J. Der Dtsch. Dermatol. Ges. 2019, 18, 7–14. [Google Scholar] [CrossRef]
- Dika, E.; Patrizi, A.; Ribero, S.; Fanti, P.A.; Starace, M.; Melotti, B.; Sperandi, F.; Piraccini, B.M. Hair and nail adverse events during treatment with targeted therapies for metastatic melanoma. Eur. J. Dermatol. Ejd 2016, 26, 232–239. [Google Scholar] [CrossRef]
- Chu, E.Y.; Wanat, K.A.; Miller, C.J.; Amaravadi, R.K.; Fecher, L.A.; Brose, M.S.; Mcgettigan, S.; Giles, L.R.; Schuchter, L.M.; Seykora, J.T.; et al. Diverse cutaneous side effects associated with BRAF inhibitor therapy: A clinicopathologic study. J. Am. Acad. Dermatol. 2012, 67, 1265–1272. [Google Scholar] [CrossRef] [Green Version]
- Boussemart, L.; Routier, E.; Mateus, C.; Opletalova, K.; Sebille, G.; Kamsu-Kom, N.; Thomas, M.; Vagner, S.; Favre, M.; Tomasic, G.; et al. Prospective study of cutaneous side-effects associated with the BRAF inhibitor vemurafenib: A study of 42 patients. Ann. Oncol. 2013, 24, 1691–1697. [Google Scholar] [CrossRef] [PubMed]
- Gençler, B.; Gönül, M. Cutaneous Side Effects of BRAF Inhibitors in Advanced Melanoma: Review of the Literature. Dermatol. Res. Pr. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Macdonald, J.B.; Macdonald, B.; Golitz, L.E.; LoRusso, P.; Sekulic, A. Cutaneous adverse effects of targeted therapies: Part I: Inhibitors of the cellular membrane. J. Am. Acad. Dermatol. 2015, 72, 203–218. [Google Scholar] [CrossRef]
- Oberholzer, P.A.; Kee, D.; Dziunycz, P.; Sucker, A.; Kamsukom, N.; Jones, R.; Roden, C.; Chalk, C.J.; Ardlie, K.; Palescandolo, E.; et al. RAS Mutations Are Associated with the Devel-opment of Cutaneous Squamous Cell Tumors in Patients Treated with RAF Inhibitors. J. Clin. Oncol. 2012, 30, 316–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piraccini, B.M.; Patrizi, A.; Fanti, P.A.; Starace, M.; Bruni, F.; Melotti, B.; Misciali, C.; Dika, E. RASopathic alopecia: Hair changes associated with vemurafenib therapy. J. Am. Acad. Dermatol. 2015, 72, 738–741. [Google Scholar] [CrossRef] [PubMed]
- Rosen, A.C.; Case, E.C.; Dusza, S.W.; Balagula, Y.; Gordon, J.; West, D.P.; Lacouture, M.E. Impact of Dermatologic Adverse Events on Quality of Life in 283 Cancer Patients: A Questionnaire Study in a Dermatology Referral Clinic. Am. J. Clin. Dermatol. 2013, 14, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.P.; Setser, A.; Anadkat, M.J.; Cotliar, J.; Olsen, E.A.; Garden, B.C.; Lacouture, M.E. Grading dermatologic adverse events of cancer treat-ments: The Common Terminology Criteria for Adverse Events Version 4.0. J. Am. Acad. Dermatol. 2012, 67, 1025–1039. [Google Scholar] [CrossRef] [PubMed]
- Lacouture, M.E.; O’Reilly, K.; Rosen, N.; Solit, D.B. Induction of Cutaneous Squamous Cell Carcinomas by RAF Inhibitors: Cause for Concern? J. Clin. Oncol. 2012, 30, 329–330. [Google Scholar] [CrossRef] [PubMed]
- Su, F.; Viros, A.; Milagre, C.; Trunzer, K.; Bollag, G.; Spleiss, O.; Reis-Filho, J.S.; Kong, X.; Koya, R.C.; Flaherty, K.T.; et al. RAS Mutations in Cutaneous Squamous-Cell Carcinomas in Patients Treated with BRAF Inhibitors. N. Engl. J. Med. 2012, 366, 207–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dika, E.; Patrizi, A.; Venturoli, S.; Fanti, P.A.; Barbieri, D.; Strammiello, R.; Melotti, B.; La PLaca, M. Human papillomavirus evaluation of vemuraf-enib-induced skin epithelial tumors: A case series. Br. J. Dermatol. 2015, 172, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Dika, E.; Lambertini, M.; Fanti, P.A.; Piraccini, B.M.; Gurioli, C.; Ravaioli, G.M.; Chessa, M.A.; Gradassi, A.T.; Melotti, B.; Sperandi, F.; et al. Sequential monitoring of pigmented lesions during dabrafenib treatment: A prospective study and a literature overview. G. Ital. Di Dermatol. E Venereol. 2019, 154, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Dika, E.; Patrizi, A.; Altimari, A.; Fiorentino, M.; La Placa, M.; Gruppioni, E.; Venturoli, S.; Vaccari, S.; Melotti, B.; Piraccini, B.M.; et al. Virologic and genetic evaluation of vemuraf-enib-induced skin cancers. Cutan. Ocul. Toxicol. 2015, 34, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Vigarios, E.; Lamant, L.; Delord, J.; Fricain, J.; Chevreau, C.; Barres, B.; Boulanger, M.; Sibaud, V.; Gomez-Roca, C. Oral squamous cell carcinoma and hyperkeratotic lesions with BRAF inhibitors. Br. J. Dermatol. 2015, 172, 1680–1682. [Google Scholar] [CrossRef] [PubMed]
- Alrashdan, M.S.; Cirillo, N.; McCullough, M. Oral lichen planus: A literature review and update. Arch. Dermatol. Res. 2016, 308, 539–551. [Google Scholar] [CrossRef]
- Schaberg, K.B.; Novoa, R.A.; Wakelee, H.A.; Kim, J.; Cheung, C.; Srinivas, S.; Kwong, B.Y. Immunohistochemical analysis of lichenoid reactions in patients treated with anti-PD-L1 and anti-PD-1 therapy: Lichenoid reactions with anti-PD-L1 and anti-PD-1 therapy. J. Cutan. Pathol. 2016, 43, 339–346. [Google Scholar] [CrossRef]
- Obara, K.; Masuzawa, M.; Amoh, Y. Oral lichenoid reaction showing multiple ulcers associated with anti-programmed death cell receptor-1 treatment: A report of two cases and published work review. J. Dermatol. 2018, 45, 587–591. [Google Scholar] [CrossRef]
- Carrozzo, M.; Porter, S.; Mercadante, V.; Fedele, S. Oral lichen planus: A disease or a spectrum of tissue reactions? Types, causes, diagnostic algorhythms, prognosis, management strategies. Periodontology 2000 2019, 80, 105–125. [Google Scholar] [CrossRef]
- Enomoto, Y.; Nakatani, H.; Kondo, S.; Kasai, T.; Tsuchiya, Y. Drug-induced oral lichenoid reaction during nivolumab therapy. Int. J. Oral Maxillofac. Surg. 2019, 48, 488–491. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.G.; Hirsch, S.A.; Gordon, S.C. The malignant transformation of oral lichen planus and oral lichenoid lesions. J. Am. Dent. Assoc. 2014, 145, 45–56. [Google Scholar] [CrossRef] [Green Version]
- Dika, E.; Ravaioli, G.M.; Fanti, P.A.; Piraccini, B.M.; Lambertini, M.; Chessa, M.A.; Baraldi, C.; Ribero, S.; Andrea, A.; Melotti, B.; et al. Cutaneous adverse effects during ipilimumab treatment for metastatic melanoma: A prospective study. Eur. J. Dermatol. Ejd 2017, 27, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Bezinelli, L.M.; Eduardo, F.P.; Migliorati, C.A.; Ferreira, M.H.; Taranto, P.; Sales, D.B.; Santi, C.G.; Macarenco, R.S.; Godoy, C.P.; Corrêa, L.; et al. A Severe, Refractory Case of Mucous Membrane Pemphigoid After Treatment With Pembrolizumab: Brief Communication. J. Immunother. 2019, 42, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.J.; Carlos, G.; Chou, S.; Wakade, D.; Carlino, M.S.; Fernandez-Penas, P. Bullous pemphigoid, an autoantibody-mediated disease, is a novel immune-related adverse event in patients treated with anti-programmed cell death 1 antibodies. Melanoma Res. 2016, 26, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.Y.; Hwang, S.J.E.; Consuegra, G.; Chou, S.; Fernandez-Peñas, P. Anti-programmed cell death-1 therapy-associated bullous disorders: A systematic review of the literature. Melanoma Res. 2018, 28, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Jour, G.; Glitza, I.C.; Ellis, R.M.; Torres-Cabala, C.A.; Tetzlaff, M.T.; Li, J.Y.; Nagarajan, B.; Huen, A.; Aung, P.P.; Ivan, D.; et al. Autoimmune dermatologic toxicities from immune checkpoint blockade with anti-PD-1 antibody therapy: A report on bullous skin eruptions: Bullous skin toxicities from anti-PD-1 antibody therapy. J. Cutan. Pathol. 2016, 43, 688–696. [Google Scholar] [CrossRef]
- Naidoo, J.; Schindler, K.; Querfeld, C.; Busam, K.; Cunningham, J.; Page, D.B.; Postow, M.A.; Weinstein, A.; Lucas, A.S.; Ciccolini, K.T.; et al. Autoimmune Bullous Skin Disorders with Immune Checkpoint Inhibitors Targeting PD-1 and PD-L1. Cancer Immunol. Res. 2016, 4, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Logan, I.T.; Zaman, S.; Hussein, L.; Perrett, C.M. Combination Therapy of Ipilimumab and Nivolumab-associated Toxic Epidermal Necrolysis (TEN) in a Patient with Metastatic Melanoma: A Case Report and Literature Review. J. Immunother. 2020, 43, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Bs, N.J.M.; Ravi, V.; Cheng, K.; Bach, D.Q.; Worswick, S. Stevens-Johnson syndrome and toxic epidermal necrolysis-like reactions to checkpoint inhibitors: A systematic review. Int. J. Dermatol. 2020, 59. [Google Scholar] [CrossRef]
- Warner, B.M.; Baer, A.N.; Lipson, E.J.; Allen, C.; Hinrichs, C.; Rajan, A.; Pelayo, E.; Beach, M.; Gulley, J.L.; Madan, R.A.; et al. Sicca Syndrome Associated with Immune Checkpoint Inhibitor Therapy. Oncologist 2019, 24, 1259–1269. [Google Scholar] [CrossRef] [Green Version]
- Gavrilovic, I.T.; Balagula, Y.; Rosen, A.C.; Ramaswamy, V.; Dickler, M.N.; Dunkel, I.J.; Lacouture, M.E. Characteristics of oral mucosal events re-lated to bevacizumab treatment. Oncologist 2012, 17, 274–278. [Google Scholar] [CrossRef] [Green Version]
- Hubiche, T.; Valenza, B.; Chevreau, C.; Fricain, J.-C.; Del Giudice, P.; Sibaud, V. Geographic Tongue Induced by Angiogenesis Inhibitors. Oncologist 2013, 18, 265–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, A.C.; Gavrilovic, I.T.; Balagula, Y.; Ramaswamy, V.; Dickler, M.N.; Dunkel, I.J.; Lacouture, M.E. RE: Geographic Tongue Induced by Angiogenesis Inhibitors. Oncologist 2013, 18, e18. [Google Scholar] [PubMed] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dika, E.; Lambertini, M.; Gouveia, B.; Mussi, M.; Marcelli, E.; Campione, E.; Gurioli, C.; Melotti, B.; Alessandrini, A.; Ribero, S. Oral Manifestations in Melanoma Patients Treated with Target or Immunomodulatory Therapies. J. Clin. Med. 2021, 10, 1283. https://doi.org/10.3390/jcm10061283
Dika E, Lambertini M, Gouveia B, Mussi M, Marcelli E, Campione E, Gurioli C, Melotti B, Alessandrini A, Ribero S. Oral Manifestations in Melanoma Patients Treated with Target or Immunomodulatory Therapies. Journal of Clinical Medicine. 2021; 10(6):1283. https://doi.org/10.3390/jcm10061283
Chicago/Turabian StyleDika, Emi, Martina Lambertini, Bruna Gouveia, Martina Mussi, Emanuela Marcelli, Elena Campione, Carlotta Gurioli, Barbara Melotti, Aurora Alessandrini, and Simone Ribero. 2021. "Oral Manifestations in Melanoma Patients Treated with Target or Immunomodulatory Therapies" Journal of Clinical Medicine 10, no. 6: 1283. https://doi.org/10.3390/jcm10061283