
Elderly Patients in a Large Nephrology Unit: Who Are Our Old, Old-Old and Oldest-Old Patients?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting of Study
2.2. Characterization of Patients in the Cross-Sectional Analysis
2.3. Data Gathered
2.4. Statistical Analysis
2.5. Ethical Issues
3. Results
3.1. Baseline Data
3.2. Kidney Function Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raman, M.; Green, D.; Middleton, R.J.; Kalra, P.A. Comparing the impact of older age on outcome in chronic kidney disease of different etiologies: A prospective cohort study. J. Nephrol. 2018, 31, 931–939. [Google Scholar] [CrossRef] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Inter. Suppl. 2013, 3, 1–150. [Google Scholar]
- Aucella, F.; Corsonello, A.; Leosco, D.; Brunori, G.; Gesualdo, L.; Antonelli-Incalzi, R. Beyond chronic kidney disease: The diagnosis of Renal Disease in the Elderly as an unmet need. A position paper endorsed by Italian Society of Nephrology (SIN) and Italian Society of Geriatrics and Gerontology (SIGG). J. Nephrol. 2019, 32, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Azar, M. The elderly patient with low eGFR: Beyond the numbers. R. I. Med. J. (2013) 2014, 97, 19–23. [Google Scholar]
- Delanaye, P.; Jager, K.J.; Bokenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; van der Giet, M.; Glassock, R.J.; et al. CKD: A Call for an Age-Adapted Definition. J. Am. Soc. Nephrol. 2019, 30, 1785–1805. [Google Scholar] [CrossRef]
- Anker, D.; Santos-Eggimann, B.; Santschi, V.; Del Giovane, C.; Wolfson, C.; Streit, S.; Rodondi, N.; Chiolero, A. Screening and treatment of hypertension in older adults: Less is more? Public Health Rev. 2018, 39, 26. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; Torreggiani, M.; Arazzi, M.; Serpieri, N.; Scaramuzzi, M.L.; Manini, A.; Grosjean, F.; Esposito, V.; Catucci, D.; La Porta, E.; et al. Loss of renal function in the elderly Italians: A physiologic or pathologic process? J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1387–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Nicola, L.; Minutolo, R.; Chiodini, P.; Borrelli, S.; Zoccali, C.; Postorino, M.; Iodice, C.; Nappi, F.; Fuiano, G.; Gallo, C.; et al. The effect of increasing age on the prognosis of non-dialysis patients with chronic kidney disease receiving stable nephrology care. Kidney Int. 2012, 82, 482–488. [Google Scholar] [CrossRef] [Green Version]
- Tonelli, M.; Riella, M.C. Chronic kidney disease and the aging population. Kidney Int. 2014, 85, 487–491. [Google Scholar] [CrossRef] [Green Version]
- United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020.
- World Health Organization. Men Ageing and Health. Achieving Health across the Life Span. 2008. Available online: https://apps.who.int/iris/bitstream/handle/10665/66941/WHO_NMH_NPH_01.2.pdf?sequence=1 (accessed on 15 February 2021).
- Bowling, C.B.; Muntner, P. Epidemiology of chronic kidney disease among older adults: A focus on the oldest old. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1379–1386. [Google Scholar] [CrossRef] [Green Version]
- Chou, K.L.; Chi, I. Successful aging among the young-old, old-old, and oldest-old Chinese. Int. J. Aging Hum. Dev. 2002, 54, 1–14. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Shmotkin, D.; Blumstein, Z.; Shorek, A.; Eyal, N.; Hazan, H.; Team, C. The old, old-old, and the oldest old: Continuation or distinct categories? An examination of the relationship between age and changes in health, function, and wellbeing. Int. J. Aging Hum. Dev. 2013, 77, 37–57. [Google Scholar] [CrossRef] [PubMed]
- Garfein, A.J.; Herzog, A.R. Robust aging among the young-old, old-old, and oldest-old. J. Gerontol. B Psychol. Sci. Soc. Sci. 1995, 50, S77–S87. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Sofronie, A.C.; Coindre, J.P. The strange case of Mr. H. Starting dialysis at 90 years of age: Clinical choices impact on ethical decisions. BMC Med. Ethics 2017, 18, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorsteinsdottir, B.; Swetz, K.M.; Albright, R.C. The Ethics of Chronic Dialysis for the Older Patient: Time to Reevaluate the Norms. Clin. J. Am. Soc. Nephrol. 2015, 10, 2094–2099. [Google Scholar] [CrossRef] [Green Version]
- Muthalagappan, S.; Johansson, L.; Kong, W.M.; Brown, E.A. Dialysis or conservative care for frail older patients: Ethics of shared decision-making. Nephrol. Dial. Transplant. 2013, 28, 2717–2722. [Google Scholar] [CrossRef] [Green Version]
- Berar Yanay, N.; Hochman, O. [the Role of Comprehensive Conservative Management in Elderly Patients with End Stage Renal Disease]. Harefuah 2019, 158, 48–52. [Google Scholar] [PubMed]
- Douglas, C.A. Palliative care for patients with advance chronic kidney disease. J. R. Coll. Physicians Edinb. 2014, 44, 224–231. [Google Scholar] [CrossRef]
- Berger, J.R.; Jaikaransingh, V.; Hedayati, S.S. End-Stage Kidney Disease in the Elderly: Approach to Dialysis Initiation, Choosing Modality, and Predicting Outcomes. Adv. Chronic Kidney Dis. 2016, 23, 36–43. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Nyman, U.; Grubb, A.; Larsson, A.; Hansson, L.O.; Flodin, M.; Nordin, G.; Lindstrom, V.; Bjork, J. The revised Lund-Malmo GFR estimating equation outperforms MDRD and CKD-EPI across GFR, age and BMI intervals in a large Swedish population. Clin. Chem. Lab. Med. 2014, 52, 815–824. [Google Scholar] [CrossRef]
- Pottel, H.; Hoste, L.; Dubourg, L.; Ebert, N.; Schaeffner, E.; Eriksen, B.O.; Melsom, T.; Lamb, E.J.; Rule, A.D.; Turner, S.T.; et al. An estimated glomerular filtration rate equation for the full age spectrum. Nephrol. Dial. Transplant. 2016, 31, 798–806. [Google Scholar] [CrossRef] [Green Version]
- Schaeffner, E.S.; Ebert, N.; Delanaye, P.; Frei, U.; Gaedeke, J.; Jakob, O.; Kuhlmann, M.K.; Schuchardt, M.; Tolle, M.; Ziebig, R.; et al. Two novel equations to estimate kidney function in persons aged 70 years or older. Ann. Intern. Med. 2012, 157, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Neild, G.H. Primary renal disease in young adults with renal failure. Nephrol. Dial. Transplant. 2010, 25, 1025–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanda, E.; Kanno, Y.; Katsukawa, F. Identifying progressive CKD from healthy population using Bayesian network and artificial intelligence: A worksite-based cohort study. Sci. Rep. 2019, 9, 5082. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age Groups | |||||||
|---|---|---|---|---|---|---|---|
| <50 | 50–59 | 60–69 | 70–79 | 80–89 | ≥90 | p-Values | |
| N (total: 1992) | 379 | 216 | 414 | 431 | 436 | 116 | |
| Males/females | 154/225 | 114/102 | 263/151 | 302/129 | 245/191 | 56/60 | <0.001 |
| Creatinine (mg/dL), median (IQR) | 0.85 (0.48) | 1.09 (0.95) | 1.39 (0.94) | 1.65 (1.07) | 1.67 (0.84) | 1.88 (1.13) | <0.001 |
| eGFR EPI (mL/min/1.73 m2), median (IQR) | 100 (47) | 66 (58) | 47 (35) | 38 (27) | 33 (17) | 27 (18) | <0.001 |
| Proteinuria (g/L), n (%) | 0.147 | ||||||
| <0.3 | 213 (69.4%) | 119 (65.0%) | 212 (60.7%) | 240 (65.0%) | 239 (62.3%) | 67 (64.4%) | |
| 0.3–1 | 59 (19.2%) | 29 (15.8%) | 83 (23.5%) | 53 (14.4%) | 93 (24.5%) | 25 (24.0%) | |
| ≥1 | 35 (11.4%) | 35 (19.1%) | 55 (15.8%) | 76 (20.6%) | 50 (3.2%) | 12 (11.5%) | |
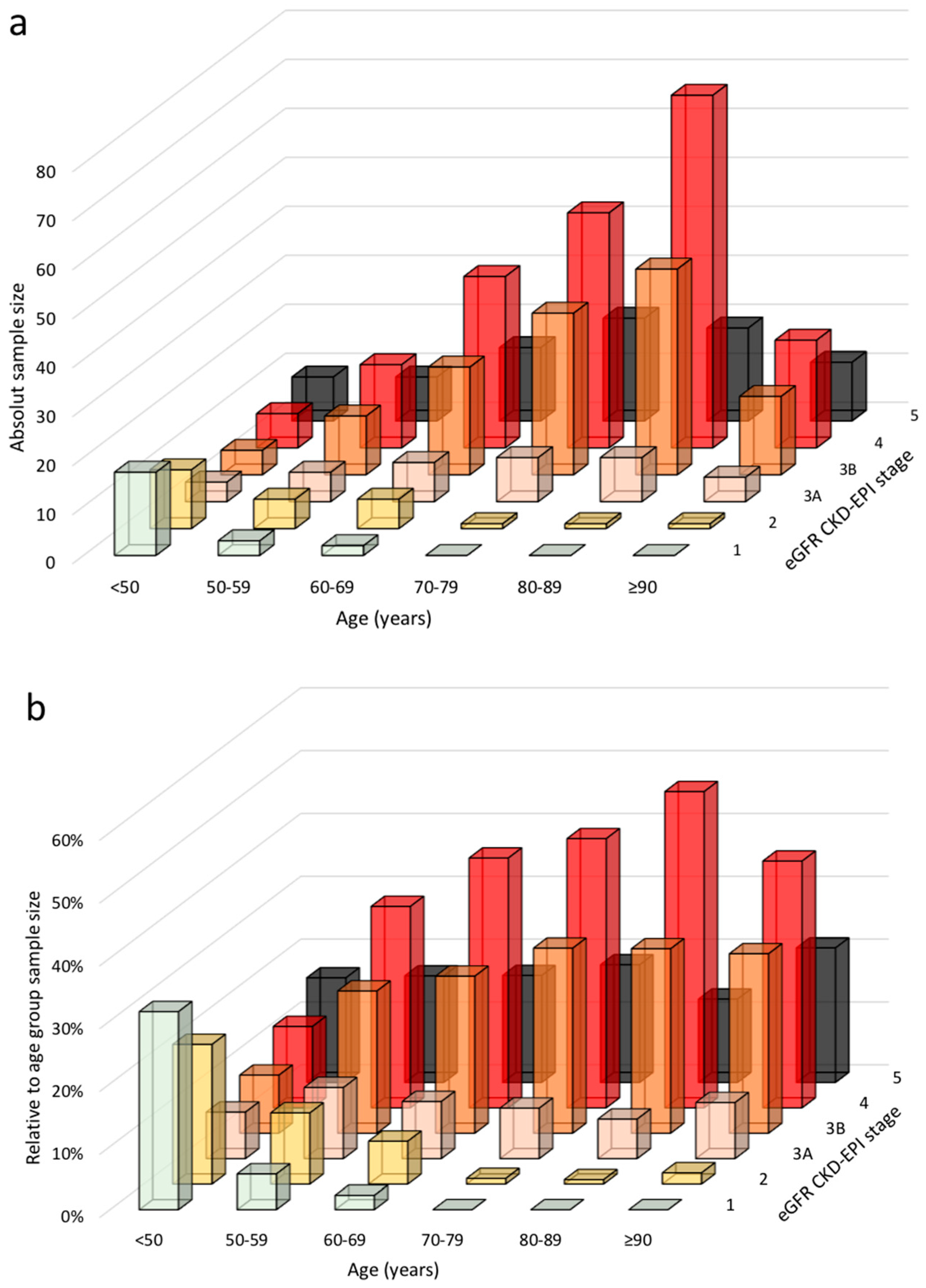
| CKD stage according to CKD-EPI, n (%) | <0.001 | ||||||
| 1 | 226 (62.3%) | 63 (29.4%) | 38 (9.3%) | 10 (2.3%) | 1 (0.2%) | 0 (0%) | |
| 2 | 58 (16%) | 51 (23.8%) | 96 (23.6%) | 57 (13.4%) | 27 (6.2%) | 2 (1.7%) | |
| 3A | 27 (7.4%) | 36 (16.8%) | 86 (21.1%) | 84 (19.7%) | 60 (13.8%) | 7 (6%) | |
| 3B | 22 (6.1%) | 23 (10.7%) | 98 (24.1%) | 129 (30.3%) | 180 (41.3%) | 37 (31.9%) | |
| 4 | 14 (3.9%) | 23 (10.7%) | 60 (14.7%) | 110 (25.8%) | 131 (30%) | 53 (45.7%) | |
| 5 | 16 (4.4%) | 18 (8.4%) | 29 (7.1%) | 36 (8.5%) | 37 (8.5%) | 17 (14.7%) | |
| Main diagnosis of kidney disease | <0.001 | ||||||
| Glomerulonephritis | 52 (13.7%) | 22 (10.2%) | 30 (7.2%) | 22 (5.1%) | 10 (2.3%) | 3 (2.6%) | |
| Nephroangiosclerosis/hypertensive nephropathy | 13 (3.4%) | 15 (6.9%) | 60 (14.5%) | 107 (24.8%) | 205 (47%) | 70 (60.3%) | |
| Diabetic kidney disease | 17 (4.5%) | 29 (13.4%) | 98 (23.7%) | 109 (25.3%) | 85 (19.5%) | 16 (13.8%) | |
| CAKUT/obstructive/systemic disease/solitary kidney | 39 (10.3%) | 16 (7.4%) | 27 (6.5%) | 35 (8.1%) | 24 (5.5%) | 7 (6%) | |
| ADPKD | 25 (6.6%) | 17 (7.9%) | 18 (4.3%) | 7 (1.6%) | 8 (1.8%) | 0 (0%) | |
| Isolated urinary abnormalities | 12 (3.2%) | 4 (1.9%) | 6 (1.4%) | 4 (0.9%) | 1 (0.2%) | 0 (0%) | |
| Multifactorial | 25 (6.6%) | 27 (12.5%) | 70 (16.9%) | 78 (18.1%) | 80 (18.3%) | 13 (11.2%) | |
| Other/post AKI/not known | 29 (7.6%) | 15 (6.9%) | 24 (5.7%) | 26 (6.1%) | 12 (2.7%) | 6 (5.2%) | |
| Postpartum-preeclampsia | 68 (17.9%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Renal stones | 99 (26.1%) | 71 (32.9%) | 81 (19.6%) | 43 (10%) | 11 (2.5%) | 1 (0.9%) |
| Age Groups | ||||||
|---|---|---|---|---|---|---|
| <50 | 50–59 | 60–69 | 70–79 | 80–89 | ≥90 | |
| N (total = 1992) | 379 | 216 | 414 | 431 | 436 | 116 |
| Creatinine (mg/L), median (IQR) | 0.85 (0.48) | 1.09 (0.95) | 1.39 (0.94) | 1.65 (1.07) | 1.67 (0.84) | 1.88 (1.13) |
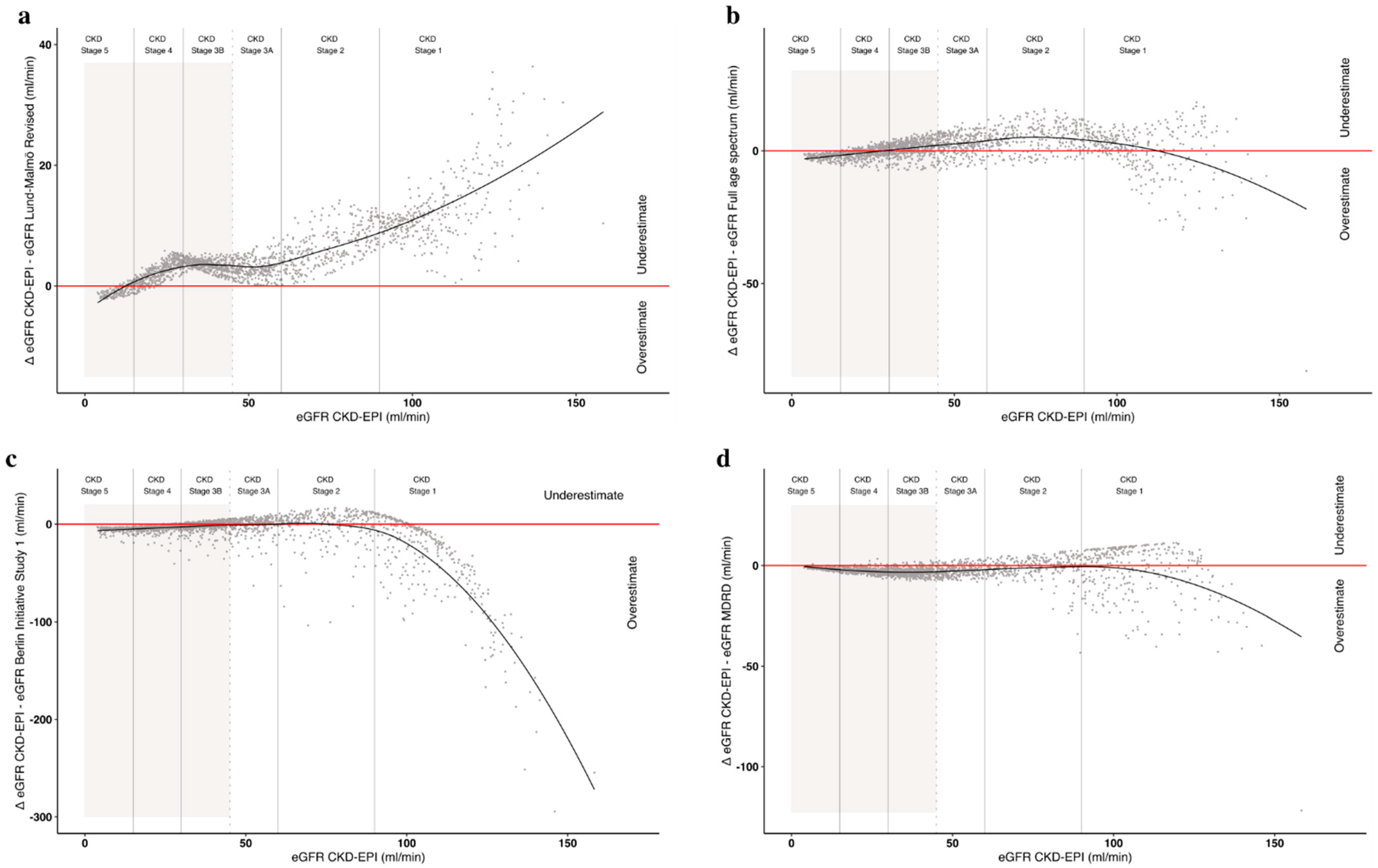
| eGFR (mL/min/1.73 m2), median (IQR) | ||||||
| CKD-EPI | 100 (47) | 66 (58) | 47 (35) | 38 (27) | 33 (17) | 27 (18) |
| Lund–Malmö Revised | 88 (34) | 64 (51) | 45 (35) | 34 (27) | 29 (17) | 22 (15) |
| Full age spectrum | 96 (41) | 65 (49) | 46 (29) | 36 (22) | 31 (14) | 25 (13) |
| Berlin Initiative Study 1 | 125 (81) | 69 (47) | 49 (27) | 39 (20) | 33 (13) | 27 (12) |
| MDRD | 92 (47) | 65 (54) | 49 (35) | 41 (28) | 37 (19) | 32 (20) |
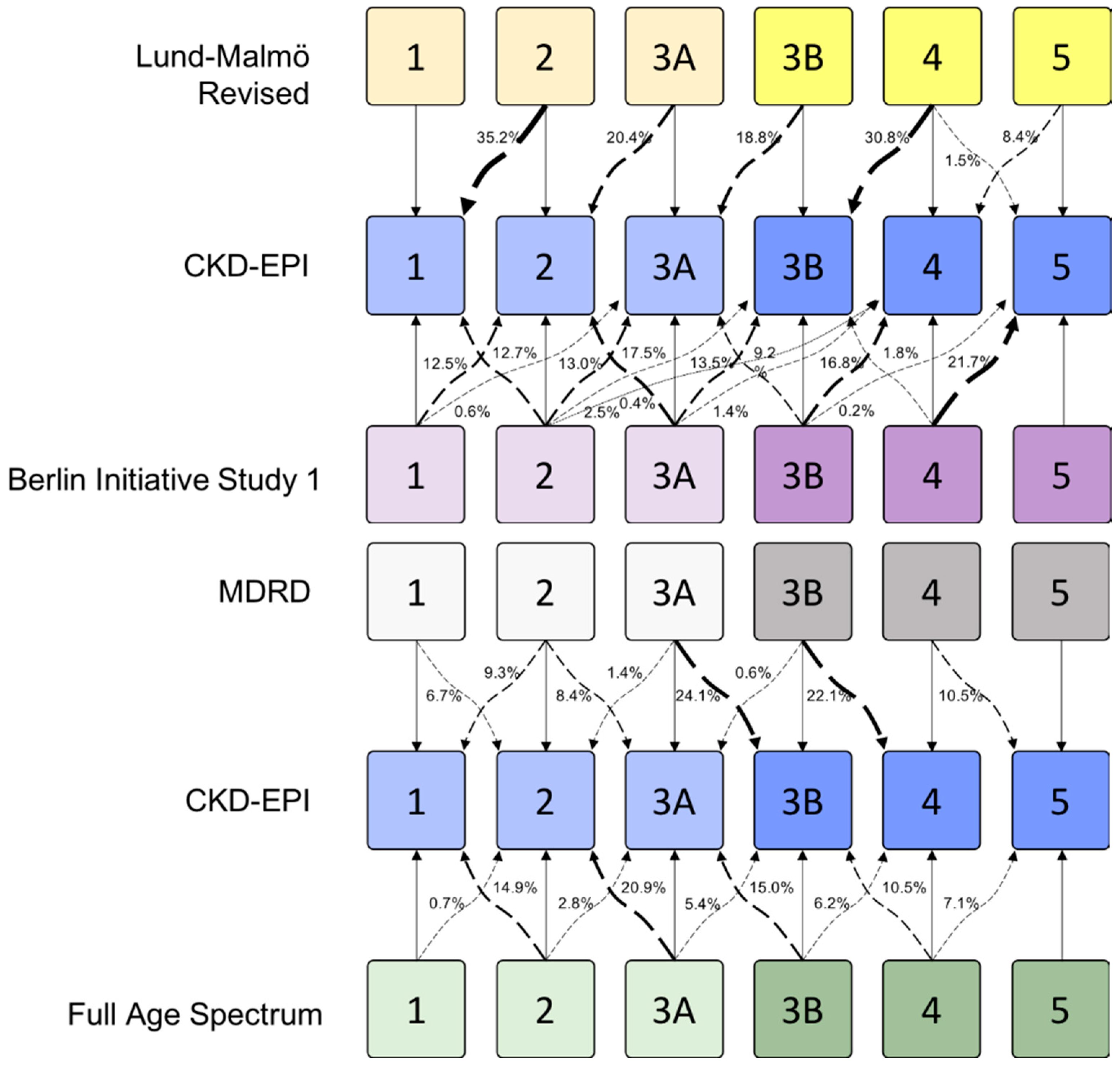
| eGFR Estimation Formula | |||||
|---|---|---|---|---|---|
| CKD-EPI | Lund–Malmö Revised | Full Age Spectrum | Berlin Initiative Study 1 | MDRD | |
| Overall | |||||
| % vs. CKD-EPI | 0 | 7.2% | 5.86% | 0.1% | −8.52% |
| N | 1044 | 1125 | 1109 | 1045 | 962 |
| <60 years of age | |||||
| % vs. CKD-EPI | 0 | 7.09% | −13.46% | −45.68% | 1.67% |
| N | 118 | 127 | 104 | 81 | 120 |
| ≥60 to <80 years of age | |||||
| % vs. CKD-EPI | 0 | 6.96% | 5.84% | −1.3% | −8.84% |
| N | 468 | 503 | 497 | 462 | 430 |
| ≥80 years of age | |||||
| % vs. CKD-EPI | 0 | 7.47% | 9.84% | 8.76% | −11.17% |
| N | 458 | 495 | 508 | 502 | 412 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torreggiani, M.; Chatrenet, A.; Fois, A.; Moio, M.R.; Mazé, B.; Coindre, J.P.; Crochette, R.; Sigogne, M.; Wacrenier, S.; Lecointre, L.; et al. Elderly Patients in a Large Nephrology Unit: Who Are Our Old, Old-Old and Oldest-Old Patients? J. Clin. Med. 2021, 10, 1168. https://doi.org/10.3390/jcm10061168
Torreggiani M, Chatrenet A, Fois A, Moio MR, Mazé B, Coindre JP, Crochette R, Sigogne M, Wacrenier S, Lecointre L, et al. Elderly Patients in a Large Nephrology Unit: Who Are Our Old, Old-Old and Oldest-Old Patients? Journal of Clinical Medicine. 2021; 10(6):1168. https://doi.org/10.3390/jcm10061168
Chicago/Turabian StyleTorreggiani, Massimo, Antoine Chatrenet, Antioco Fois, Maria Rita Moio, Béatrice Mazé, Jean Philippe Coindre, Romain Crochette, Mickael Sigogne, Samuel Wacrenier, Léna Lecointre, and et al. 2021. "Elderly Patients in a Large Nephrology Unit: Who Are Our Old, Old-Old and Oldest-Old Patients?" Journal of Clinical Medicine 10, no. 6: 1168. https://doi.org/10.3390/jcm10061168