
Prospective Longitudinal Changes in the Periodontal Inflamed Surface Area Following Active Periodontal Treatment for Chronic Periodontitis

 ,
,  , , , , , , ,
, , , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Approval
2.2. Inclusion Criteria
2.3. Diagnosis and Evaluation
2.4. Evaluation of Periodontal Pathogens
2.5. Statistical Analysis
2.5.1. Mixed-Effect Modeling
| (1) | |
| Fixed effect; Patient-level: Age, sex, time, salivary levels of A. actinomycetemcomitans, P. gingivalis, and P. intermedia, mean CAL, PlI, time Random effect: Patients, random intercept Covariance Type: AR1 Link functions: Gamma |
| (1) | |
| (2) | |
| Fixed effect; Patient-level: Age, sex, days, salivary levels of A. actinomycetemcomitans, P. gingivalis, and P. intermedia Tooth-level: Mean CAL, PlI, tooth mobility, tooth type, time Random effect: Patients, random intercept Covariance Type: AR1 Link functions: Gamma |
| (1) | |
| Fixed effect; Patient-level: Proportion of A. actinomycetemcomitans, P. gingivalis, and P. intermedia in the total subgingival bacteria, time Random effect: Patients Covariance Type: AR1 Link functions: Gamma |
2.5.2. Cluster Analysis
3. Results
3.1. Patient Characteristics
3.2. Analysis of the Change in PISA at the Patient-Level
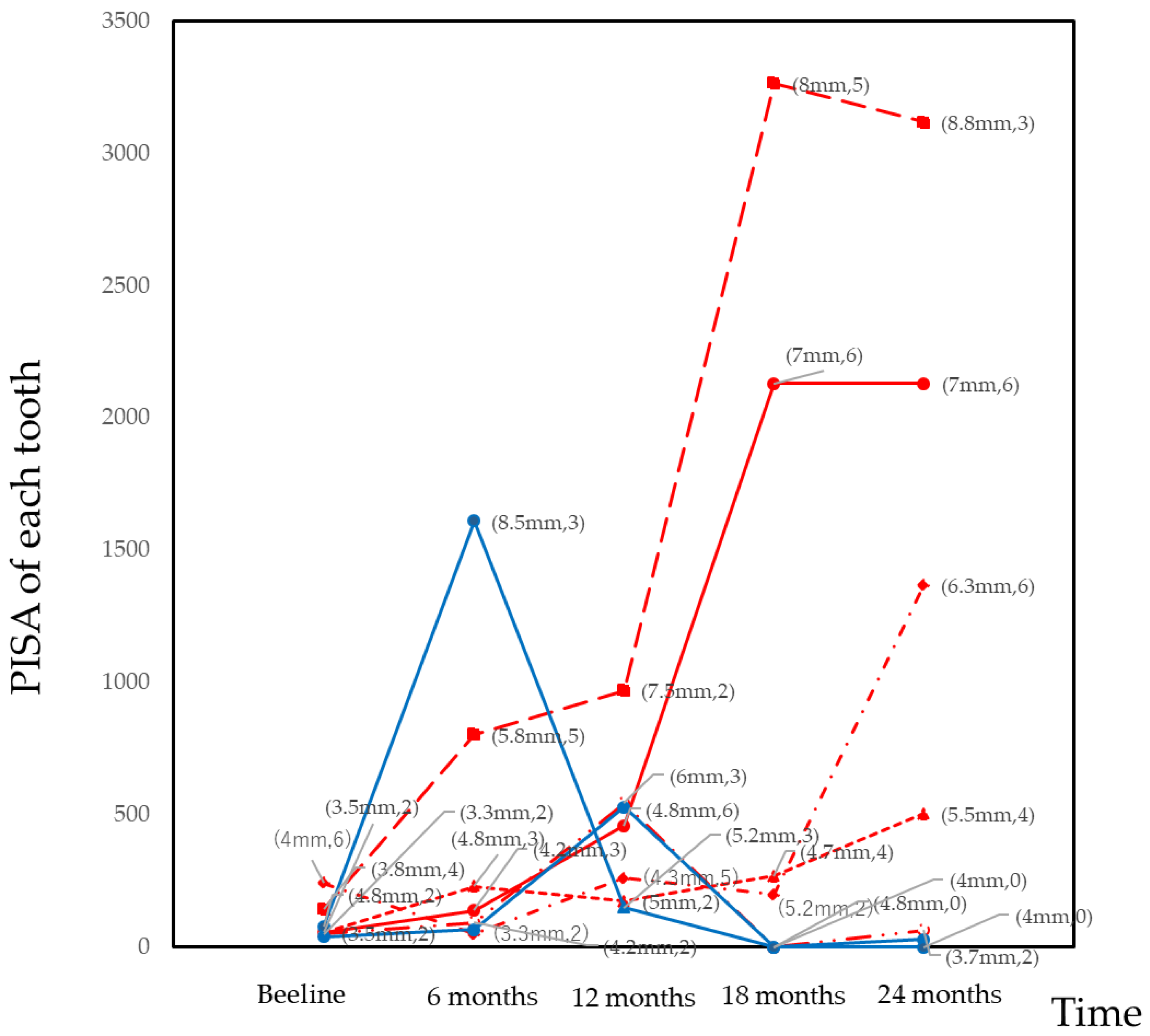
3.3. Analysis of the Change in PISA at the Tooth-Level
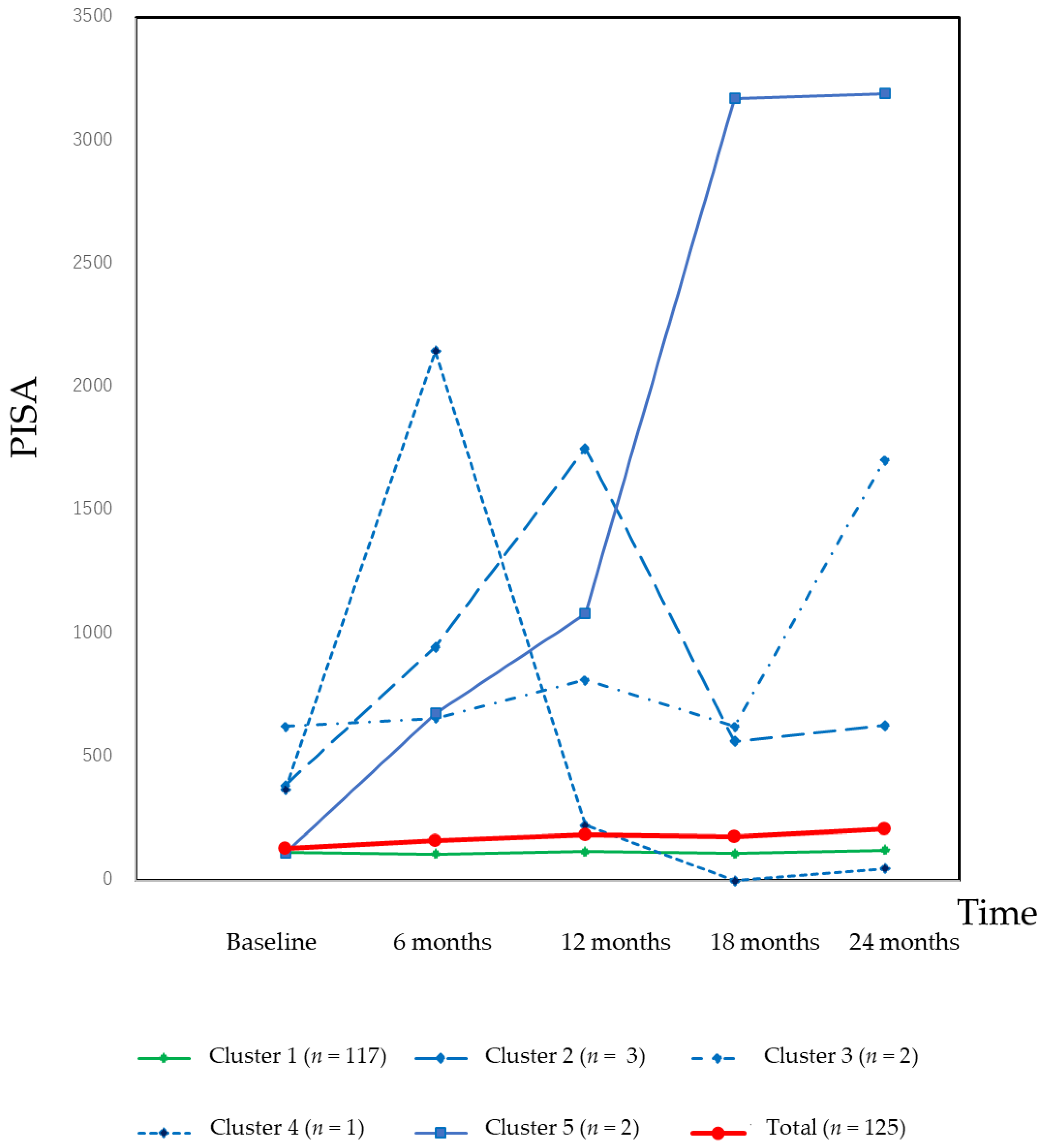
3.4. Classification of the Changes in the PISA
3.5. Association between Periodontal Pathogens and the Change in the PISA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nomura, Y.; Morozumi, T.; Nakagawa, T.; Sugaya, T.; Kawanami, M.; Suzuki, F.; Takahashi, K.; Abe, Y.; Sato, S.; Makino-Oi, A.; et al. Site-level progression of periodontal disease during a follow-up period. PLoS ONE 2017, 12, e0188670. [Google Scholar] [CrossRef] [PubMed]
- Gilthorpe, M.S.; Zamzuri, A.T.; Griffiths, G.S.; Maddick, I.H.; Eaton, K.A.; Johnson, N.W. Unification of the “burst” and “linear” theories of periodontal disease progression: A multilevel manifestation of the same phenomenon. J. Dent. Res. 2003, 82, 200–205. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Goodson, J.M.; Lindhe, J. New concepts of destructive periodontal disease. J. Clin. Periodontol. 1984, 11, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; Leroux, B.G. Evaluating the Burst Hypothesis at a Site-Specific Level Using the Lack-of-Fit Test. J. Periodontol. 1998, 69, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Gilthorpe, M.S.; Griffiths, G.S.; Maddick, I.H.; Zamzuri, A.T. An application of multilevel modelling to longitudinal perio-dontal research data. Community Dent. Health 2001, 18, 79–86. [Google Scholar] [PubMed]
- Park, S.Y.; Ahn, S.; Lee, J.T.; Yun, P.Y.; Lee, Y.J.; Lee, J.Y.; Song, Y.W.; Chang, Y.S.; Lee, H.J. Periodontal inflamed surface area as a novel numerical variable describing periodontal conditions. J. Periodontal Implant. Sci. 2017, 47, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamont, R.J.; Hajishengallis, G. Polymicrobial synergy and dysbiosis in inflammatory disease. Trends Mol. Med. 2015, 21, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Chambrone, L.A.; Chambrone, L. Tooth loss in well-maintained patients with chronic periodontitis during long-term supportive therapy in Brazil. J. Clin. Periodontol. 2006, 33, 759–764. [Google Scholar] [CrossRef]
- Carnevale, G.; Cairo, F.; Tonetti, M.S. Long-term effects of supportive therapy in periodontal patients treated with fibre retention osseous resective surgery. II: Tooth extractions during active and supportive therapy. J. Clin. Periodontol. 2007, 34, 342–348. [Google Scholar] [CrossRef]
- Fardal, Ø.; Johannessen, A.C.; Linden, G.J. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J. Clin. Periodontol. 2004, 31, 550–555. [Google Scholar] [CrossRef] [PubMed]
- McLeod, D.E.; Lainson, P.A.; Spivey, J.D. The predictability of periodontal treatment as measured by tooth loss: A retrospec-tive study. Quintessence Int. 1998, 29, 631–635. [Google Scholar]
- McLeod, D.E.; Lainson, P.A.; Spivey, J.D. Tooth Loss Due to Periodontal Abscess: A Retrospective Study. J. Periodontol. 1997, 68, 963–966. [Google Scholar] [CrossRef]
- Loesche, W.J.; Giordano, J.R.; Soehren, S.; Kaciroti, N. The nonsurgical treatment of patients with periodontal disease: Results after five years. J. Am. Dent. Assoc. 2002, 133, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G.; Glover, M.E.; Malik, A.K.; Schoen, J.A.; Dorsett, D. Tooth Loss in Maintenance Patients in a Private Periodontal Practice. J. Periodontol. 1987, 58, 231–235. [Google Scholar] [CrossRef]
- Wood, W.R.; Greco, G.W.; McFall, W.T. Tooth Loss in Patients with Moderate Periodontitis After Treatment and Long–Term Maintenance Care. J. Periodontol. 1989, 60, 516–520. [Google Scholar] [CrossRef]
- Matthews, D.C.; Smith, C.G.; Hanscom, S.L. Tooth loss in periodontal patients. J. Can. Dent. Assoc. 2001, 67, 207–210. [Google Scholar] [PubMed]
- Tonetti, M.S.; Steffen, P.; Muller-Campanile, V.; Suvan, J.; Lang, N.P. Initial extractions and tooth loss during supportive care in a periodontal population seeking comprehensive care. J. Clin. Periodontol. 2000, 27, 824–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manresa, C.; Sanz-Miralles, E.C.; Twigg, J.; Bravo, M. Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst. Rev. 2018, 1, CD009376. [Google Scholar] [CrossRef] [PubMed]
- Nesse, W.; Abbas, F.; Van Der Ploeg, I.; Spijkervet, F.K.L.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area: Quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Teke, E.; Kırzıoğlu, F.Y.; Korkmaz, H.; Calapoğlu, M.; Orhan, H. Does metabolic control affect salivary adipokines in type 2 diabetes mellitus? Dent. Med. Probl. 2019, 56, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, S.; Okanobu, A.; Hatano, S.; Kajiya, M.; Sasaki, S.; Hamamoto, Y.; Iwata, T.; Ouhara, K.; Takeda, K.; Mizuno, N.; et al. Relationship between periodontal inflammation and calcium channel blockers induced gingival overgrowth—A cross-sectional study in a Japanese population. Clin. Oral Investig. 2019, 23, 4099–4105. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Rodríguez-Yáñez, M.; Arias, S.; López-Dequidt, I.; Campos, F.; Sobrino, T.; D’Aiuto, F.; Castillo, J.; Blanco, J. Periodontitis is associated with systemic inflammation and vascular endothelial dysfunction in patients with lacunar infarct. J. Periodontol. 2019, 90, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Temelli, B.; Ay, Z.Y.; Aksoy, F.; Büyükbayram, H.I.; Doguc, D.K.; Uskun, E.; Varol, E. Platelet indices (mean platelet volume and platelet distribution width) have correlations with periodontal inflamed surface area in coronary artery disease patients: A pilot study. J. Periodontol. 2018, 89, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Punj, A.; Shenoy, S.B.; Subramanyam, K. Comparison of Endothelial Function in Healthy Patients and Patients with Chronic Periodontitis and Myocardial Infarction. J. Periodontol. 2017, 88, 1234–1243. [Google Scholar] [CrossRef]
- Khanuja, P.K.; Narula, S.C.; Rajput, R.; Sharma, R.K.; Tewari, S. Association of periodontal disease with glycemic control in patients with type 2 diabetes in Indian population. Front. Med. 2017, 11, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Nesse, W.; Linde, A.; Abbas, F.; Spijkervet, F.K.L.; Dijkstra, P.U.; De Brabander, E.C.; Gerstenbluth, I.; Vissink, A. Dose-response relationship between periodontal inflamed surface area and HbA1c in type 2 Diabetics. J. Clin. Periodontol. 2009, 36, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, M.; Kimura, Y.; Yamaga, T.; Yamamoto, N.; Ishikawa, M.; Wada, T.; Sakamoto, R.; Ishimoto, Y.; Fujisawa, M.; Okumiya, K.; et al. A population-based cross-sectional study of the association between periodontitis and arterial stiffness among the older Japanese population. J. Periodontal Res. 2020. [Google Scholar] [CrossRef]
- Aoyama, N.; Fujii, T.; Kida, S.; Nozawa, I.; Taniguchi, K.; Fujiwara, M.; Iwane, T.; Tamaki, K.; Minabe, M. Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan. J. Clin. Med. 2021, 10, 208. [Google Scholar] [CrossRef]
- Salhi, L.; Albert, A.; Seidel, L.; Lambert, F. Respective Effects of Oral Hygiene Instructions and Periodontal Nonsurgical Treatment (Debridement) on Clinical Parameters and Patient-Reported Outcome Measures with Respect to Smoking. J. Clin. Med. 2020, 9, 2491. [Google Scholar] [CrossRef]
- Echeverría, J.J.; Manau, G.C.; Guerrero, A. Supportive care after active periodontal treatment: A review. J. Clin. Periodontol. 1996, 23. [Google Scholar] [CrossRef]
- Morozumi, T.; Nakagawa, T.; Nomura, Y.; Sugaya, T.; Kawanami, M.; Suzuki, F.; Takahashi, K.; Abe, Y.; Sato, S.; Makino-Oi, A.; et al. Salivary pathogen and serum antibody to assess the progression of chronic periodontitis: A 24-mo prospective multicenter cohort study. J. Periodontal Res. 2016, 51, 768–778. [Google Scholar] [CrossRef] [PubMed]
- Kakuta, E.; Nomura, Y.; Morozumi, T.; Nakagawa, T.; Nakamura, T.; Noguchi, K.; Yoshimura, A.; Hara, Y.; Fujise, O.; Nishimura, F.; et al. Assessing the progression of chronic periodontitis using subgingival pathogen levels: A 24-month prospective multicenter cohort study. BMC Oral Health 2017, 17, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, K.A.; Clem, D.S., 3rd. American Academy of Periodontology, Guidelines for the Management of Patients with Periodontal Diseases. J. Periodontol. 2006, 77, 1607–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Tadokoro, K.; Yamaguchi, T.; Kawamura, K.; Shimizu, H.; Egashira, T.; Minabe, M.; Yoshino, T.; Oguchi, H. Rapid quantification of periodontitis-related bacteria using a novel modification of Invader PLUS technologies. Microbiol. Res. 2010, 165, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Tada, A.; Takeuchi, H.; Shimizu, H.; Tadokoro, K.; Tanaka, K.; Kawamura, K.; Yamaguchi, T.; Egashira, T.; Nomura, Y.; Hanada, N. Quantification of Periodontopathic Bacteria in Saliva Using the Invader Assay. Jpn. J. Infect. Dis. 2012, 65, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Lyons, S.R.; Griffen, A.L.; Leys, E.J. Quantitative real-time PCR for Porphyromonas gingivalis and total bacteria. J. Clin. Microbiol. 2000, 38, 2362–2365. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S.; Smith, C.; Dibart, S. Relation of baseline microbial parameters to future periodontal attachment loss. J. Clin. Periodontol. 1991, 18, 744–750. [Google Scholar] [CrossRef]
- Tomita, S.; Komiya-Ito, A.; Imamura, K.; Kita, D.; Ota, K.; Takayama, S.; Makino-Oi, A.; Kinumatsu, T.; Ota, M.; Saito, A. Prevalence of Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis and Tannerella forsythia in Japanese patients with generalized chronic and aggressive periodontitis. Microb. Pathog. 2013, 61–62, 11–15. [Google Scholar] [CrossRef]
- Nomura, Y.; Otsuka, R.; Wint, W.Y.; Okada, A.; Hasegawa, R.; Hanada, N. Tooth-Level Analysis of Dental Caries in Primary Dentition in Myanmar Children. Int. J. Environ. Res. Public Health 2020, 17, 7613. [Google Scholar] [CrossRef]
- Nakahodo, N.; Nomura, Y.; Oshiro, T.; Otsuka, R.; Kakuta, E.; Okada, A.; Inai, Y.; Takei, N.; Hanada, N. Effect of Mucosal Brushing on the Serum Levels of C-Reactive Protein for Patients Hospitalized with Acute Symptoms. Medicina 2020, 56, 549. [Google Scholar] [CrossRef]
- Otsuka, R.; Nomura, Y.; Okada, A.; Uematsu, H.; Nakano, M.; Hikiji, K.; Hanada, N.; Momoi, Y. Properties of manual toothbrush that influence on plaque removal of interproximal surface in vitro. J. Dent. Sci. 2020, 15, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Maung, K.; Kay Khine, E.M.; Sint, K.M.; Lin, M.P.; Win Myint, M.K.; Aung, T.; Sogabe, K.; Otsuka, R.; Okada, A.; et al. Prevalence of Dental Caries in 5- and 6-Year-Old Myanmar Children. Int. J. Dent. 2019, 2019, 5948379. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Takei, N.; Ishii, T.; Takada, K.; Amitani, Y.; Koganezawa, H.; Fukuhara, S.; Asai, K.; Uozumi, R.; Bessho, K. Factors That Affect Oral Care Outcomes for Institutionalized Elderly. Int. J. Dent. 2018, 2018, 2478408. [Google Scholar] [CrossRef] [Green Version]
- Sanz-Martín, I.; Cha, J.-K.; Yoon, S.W.; Sanz-Sánchez, I.; Jung, U.W. Long-term assessment of periodontal disease progression after surgical or non-surgical treatment: A systematic review. J. Periodontal Implant. Sci. 2019, 49, 60–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramseier, C.A.; Nydegger, M.; Walter, C.; Fischer, G.; Sculean, A.; Lang, N.P.; Salvi, G.E. Time between recall visits and residual probing depths predict long-term stability in patients enrolled in supportive periodontal therapy. J. Clin. Periodontol. 2019, 46, 218–230. [Google Scholar] [CrossRef]
- Eickholz, P.; Kaltschmitt, J.; Berbig, J.; Reitmeir, P.; Pretzl, B. Tooth loss after active periodontal therapy. 1: Patient-related factors for risk, prognosis, and quality of outcome. J. Clin. Periodontol. 2008, 35, 165–174. [Google Scholar] [CrossRef]
- König, J.; Plagmann, H.-C.; Rühling, A.; Kocher, T. Tooth loss and pocket probing depths in compliant periodontally treated patients: A retrospective analysis. J. Clin. Periodontol. 2002, 29, 1092–1100. [Google Scholar] [CrossRef]
- Haririan, H.; Andrukhov, O.; Bertl, K.; Lettner, S.; Kierstein, S.; Moritz, A.; Rausch-Fan, X. Microbial Analysis of Subgingival Plaque Samples Compared to That of Whole Saliva in Patients with Periodontitis. J. Periodontol. 2014, 85, 819–828. [Google Scholar] [CrossRef] [PubMed]
- Belstrøm, D.; Sembler-Møller, M.L.; Grande, M.A.; Kirkby, N.; Cotton, S.L.; Paster, B.J.; Holmstrup, P. Microbial profile comparisons of saliva, pooled and site-specific subgingival samples in periodontitis patients. PLoS ONE 2017, 12, e0182992. [Google Scholar] [CrossRef] [Green Version]
- Testa, M.; Ruiz de Valladares, R.; Benito de Cárdenas, I.L. Correlation between bacterial counts in saliva and subgingival plaque. Acta Odontol Latinoam 1999, 12, 63–74. [Google Scholar]
- Darout, I.A.; Albandar, J.M.; Skaug, N. Correlations between bacterial levels in autologous subgingival plaque and saliva of adult Sudanese. Clin. Oral Investig. 2002, 6, 210–216. [Google Scholar] [CrossRef]
- Könönen, E.; Jousimies-Somer, H.; Asikainen, S. The most frequently isolated gram-negative anaerobes in saliva and subgingival samples taken from young women. Oral Microbiol. Immunol. 1994, 9, 126–128. [Google Scholar] [CrossRef]
- Okada, A.; Sogabe, K.; Takeuchi, H.; Okamoto, M.; Nomura, Y.; Hanada, N. Characterization of specimens obtained by different sampling methods for evaluation of periodontal bacteria. J. Oral Sci. 2017, 59, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Yang, N.-Y.; Zhang, Q.; Li, J.L.; Yang, S.H.; Shi, Q. Progression of periodontal inflammation in adolescents is associated with increased number of Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythensis, and Fusobacterium nucleatum. Int. J. Paediatr. Dent. 2013, 24, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.C.B.; Napimoga, M.H.; Klein, M.I.; Höfling, J.F.; Gonçalves, R.B. Increase in Probing Depth Is Correlated With a Higher Number ofPrevotella intermediaGenotypes. J. Periodontol. 2006, 77, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Schmid, B.; Rutar, A.; Lang, N.P. Persistence Patterns ofPorphyromonas gingivalis, Prevotella intermedia/ nigrescens, and Actinobacillus actinomycetemcomitans After Mechanical Therapy of Periodontal Disease. J. Periodontol. 2000, 71, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Shiloah, J.; Patters, M.R. Repopulation of Periodontal Pockets by Microbial Pathogens in the Absence of Supportive Therapy. J. Periodontol. 1996, 67, 130–139. [Google Scholar] [CrossRef] [Green Version]
- Venezia, E.; Shapira, L. Use of antimicrobial agents during supportive periodontal therapy. Oral Dis. 2003, 9 (Suppl. 1), 63–70. [Google Scholar] [CrossRef]
- Yashima, A.; Morozumi, T.; Yoshie, H.; Hokari, T.; Izumi, Y.; Akizuki, T.; Mizutani, K.; Takamatsu, H.; Minabe, M.; Miyauchi, S.; et al. Biological responses following one-stage full-mouth scaling and root planing with and without azithromycin: Multicenter randomized trial. J. Periodontal Res. 2019, 54, 709–719. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Coefficient (95% CI) | p-Value | |
|---|---|---|
| Sex | −0.124 (−0.507–0.258) | 0.524 |
| Age (years) | 0.012 (−0.010–0.033) | 0.276 |
| Salivary levels of A. a (%) | −3.275 (−39.368–32.818) | 0.859 |
| Salivary levels of P. g (%) | 1.141 (0.148–2.136) | 0.025 |
| Salivary levels of P. i (%) | 0.206 (−0.282–0.694) | 0.408 |
| Mean CAL (mm) | 0.737 (0.540–0.934) | <0.001 |
| PlI | 1.069 (0.637–1.500) | <0.001 |
| Time (6 months) | 0.008 (−0.030–0.045) | 0.693 |
| Intercept | 1.338 (0.009–2.677) | 0.048 |
| Coefficient (95% CI) | p-Value | ||
|---|---|---|---|
| Patient-level variables | |||
| Age | −0.002 (−0.010–0.007) | 0.736 | |
| Sex | −0.076 (−0.225–0.074) | 0.320 | |
| Salivary levels of A. a (%) | −3.624 (−17.577–10.329) | 0.611 | |
| Salivary levels of P. g (%) | 0.669 (0.323–1.015) | <0.001 | |
| Salivary levels of P. i (%) | −0.028 (−0.230–0.173) | 0.782 | |
| Tooth-level variables | |||
| Mean CAL/teeth (mm) | 0.293 (0.266–0.320) | <0.001 | |
| PlI/teeth | 0.234 (0.157–0.310) | <0.001 | |
| Tooth mobility | 0 | Reference | |
| 1 | −0.044 (−0.136–0.048) | 0.348 | |
| 2 and 3 | 0.697 (0.472–0.923) | <0.001 | |
| Tooth-type | Mandibular anterior | Reference | |
| Mandibular premolar | −0.033 (−0.124–0.058) | 0.477 | |
| Mandibular molar | −0.016 (−0.105–0.074) | 0.732 | |
| Maxillary anterior | −0.116 (−0.197–−0.035) | 0.005 | |
| Maxillary premolar | 0.444 (0.359–0.530) | <0.001 | |
| Maxillary molar | 0.680 (0.590–0.770) | <0.001 | |
| Time | −0.004 (−0.022–0.014) | 0.632 | |
| Intercept | 1.516 (0.972–2.061) | <0.001 | |
| PISA | ||
|---|---|---|
| Coefficient (95% CI) | p-Value | |
| A. a | −0.221 (−1.054–0.612) | 0.602 |
| P. g | 0.033 (0.022–0.044) | <0.001 |
| P. i | 0.116 (0.024–0.208) | 0.014 |
| Time | 0.033 (−0.010–0.077) | 0.130 |
| Intercept | 2.847 (2.377–3.070) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, Y.; Morozumi, T.; Saito, A.; Yoshimura, A.; Kakuta, E.; Suzuki, F.; Nishimura, F.; Takai, H.; Kobayashi, H.; Noguchi, K.; et al. Prospective Longitudinal Changes in the Periodontal Inflamed Surface Area Following Active Periodontal Treatment for Chronic Periodontitis. J. Clin. Med. 2021, 10, 1165. https://doi.org/10.3390/jcm10061165
Nomura Y, Morozumi T, Saito A, Yoshimura A, Kakuta E, Suzuki F, Nishimura F, Takai H, Kobayashi H, Noguchi K, et al. Prospective Longitudinal Changes in the Periodontal Inflamed Surface Area Following Active Periodontal Treatment for Chronic Periodontitis. Journal of Clinical Medicine. 2021; 10(6):1165. https://doi.org/10.3390/jcm10061165
Chicago/Turabian StyleNomura, Yoshiaki, Toshiya Morozumi, Atsushi Saito, Atsutoshi Yoshimura, Erika Kakuta, Fumihiko Suzuki, Fusanori Nishimura, Hideki Takai, Hiroaki Kobayashi, Kazuyuki Noguchi, and et al. 2021. "Prospective Longitudinal Changes in the Periodontal Inflamed Surface Area Following Active Periodontal Treatment for Chronic Periodontitis" Journal of Clinical Medicine 10, no. 6: 1165. https://doi.org/10.3390/jcm10061165