
The Effect of Helicobacter pylori Eradication on Lipid Levels: A Meta-Analysis


Division of Community and Family Medicine, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke-City, Tochigi 329-0498, Japan
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2021, 10(5), 904; https://doi.org/10.3390/jcm10050904
Submission received: 25 December 2020
/
Revised: 18 February 2021
/
Accepted: 21 February 2021
/
Published: 25 February 2021
(This article belongs to the Section Endocrinology & Metabolism)
Abstract
:Introduction:Helicobacter pylori (H. pylori) infection is positively associated with cardiovascular diseases, but the involvement of lipids in this association remains unclear. The present study reviewed the changes in circulating lipid levels following H. pylori eradication. Methods: A PubMed database was searched until December 2020 to identify randomized control trials (RCTs) and non-RCTs investigating the effect of H. pylori eradication on the lipid levels in inverse variance-weighted, random-effects meta-analyses. Results: A total of 24 studies (four RCTs and 20 non-RCTs) with 5270 participants were identified. The post-eradication levels were increased for high-density lipoprotein cholesterol (HDL-C; mean difference (MD) 2.28 mg/dL, 95% confidence interval (CI) 1.90 to 2.66) and triglyceride (TG; MD 3.22 mg/dL, 95% CI 1.13 to 5.31) compared with the pre-eradication levels. H. pylori eradication resulted in little to no difference in the low-density lipoprotein-cholesterol levels (MD −2.33 mg/dL, 95% CI −4.92 to 0.26). In the analyses of RCTs only, the findings for elevated HDL-C levels, but not TG, were robust. Conclusions: H. pylori eradication increases the HDL-C levels. Further studies are needed to elucidate the effects of lipid changes following H. pylori eradication on cardiovascular diseases.
1. Introduction
Helicobacter pylori (H. pylori) is a bacterium that causes chronic gastric inflammation [1,2]. A positive association of H. pylori infection with cardiovascular disease (CVD, e.g., myocardial infarction and stroke) has been recognized [2,3]. As the background theory, H. pylori infection is involved in the pathogenesis of atherosclerosis via activation of a local or systemic inflammatory host reaction and a subsequent induction of plaque progression and instability [2]. As abnormal lipid metabolisms contribute to the development of CVD [4,5,6,7,8,9,10], circulating lipids may be also involved in the relationship between H. pylori and CVD [11].
The existence of H. pylori infection was shown to be associated with a low level of high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein (LDL-C), and total cholesterol (TC) or a high level of triglycerides (TG) in a recent meta-analysis of cross-sectional studies [11]. Nonetheless, the effect of H. pylori eradication on the lipid levels remains unclear. An earlier meta-analysis reported that H. pylori eradication did not alter the lipid levels [12]; however, that analysis included only three studies. Those three studies simply compared the lipid levels in the H. pylori-eradicated group with those in the H. pylori-negative group and did not compare the values before and after H. pylori eradication.
We investigated the changes in the levels of lipids after H. pylori eradication by reviewing meta-analyses of available published studies.
2. Methods
Candidate articles were searched via a PubMed search engine through 7 December 2020, using the following keywords: (“Cholesterol, HDL”[Mesh] OR “high-density lipoprotein cholesterol”[tiab] OR “Cholesterol, LDL”[Mesh] OR “low-density lipoprotein cholesterol”[tiab] OR “Triglycerides”[Mesh] OR “triglyceride”[tiab] OR “total cholesterol”[tiab] OR “Dyslipidemias”[Mesh] OR “Dyslipidemia”[tiab]) AND (“Helicobacter pylori”[Mesh] OR “Helicobacter pylori”[tiab]). Original articles that focused on H. pylori and lipid changes were included. No restrictions of age, gender, ethnicity, observation period, publication year to inclusion criteria were made. H. pylori infection was defined by positive results on either H. pylori IgG-antibody test, urea breath test, urease test, histology, culture, monoclonal stool antigen test, or a combination of these tests. Studies with data on pre- and post-lipid levels during H. pylori eradication and/or the change rates from baseline were included, and a sensitivity analysis was performed by using the changes from baseline. The exclusion criteria for the selection of articles were non-human and non-English articles. The reference lists of the extracted articles were hand-searched for further identification of additional studies.
The title and abstract of all candidate studies identified by the search were independently screened. The full texts of potentially relevant abstracts were assessed to determine whether or not the articles reported on the effect of H. pylori eradication on lipid changes. The study characteristics from the included studies were extracted, and a summary of tables was created in the quantitative synthesis. Meta-analyses were performed after excluding the articles that did not report the necessary outcomes and those with differing numbers of participants before and after H. pylori eradication.
The risk of bias was independently assessed using the Risk of Bias (RoB) 2 [13] in randomized controlled trials (RCTs) and the Newcastle-Ottawa Quality Rating Scale (NOS) [14] in non-randomized studies. In RoB 2, each of six domains (random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting) is classified into one of three categories (high risk, some concern, and low risk). The NOS assigns up to a maximum of 9 points to the highest-quality research according to three quality parameters (selection, comparability and outcome), with a higher score indicating a better quality. Any disagreement between the assessments of the two reviewers was resolved through discussion.
The mean difference (MD) with the 95% confidence interval (CI) of the mean change in HDL-C, TG, LDL-C, and total cholesterol (TC) after H. pylori eradication were calculated. The present meta-analysis was performed by comparing individual values before and after H. pylori eradication, regardless of the study design, as in the earlier studies [15,16]. The random-effects meta-analyses were performed in the Review Manager 5.4.1 software program (RevMan 2020) using the generic inverse variance method. The MD and standard deviation (SD) of continuous variables were integrated according to the method described in the Cochrane handbook [17]. The SD was substituted with the value from other studies when studies did not report the SD [17]. I2 statistics were used to assess statistical heterogeneity (I2 values of 0–40%: may not be important; 30–60%: may represent moderate heterogeneity; 50–90%: may represent substantial heterogeneity; 75–100%: may represent considerable heterogeneity) [17]. Sub-analyses were performed for the study design (RCTs, cohort studies, case–control studies, or before–after studies), follow-up duration (<1 or ≥1 year), and study location (Western or Asian countries). We performed sensitivity analyses to evaluate the robustness of our conclusions. This involved the exclusion of studies that did not describe the levels of HDL-C, TG, LDL-C, and TC before H. pylori eradication.
3. Results
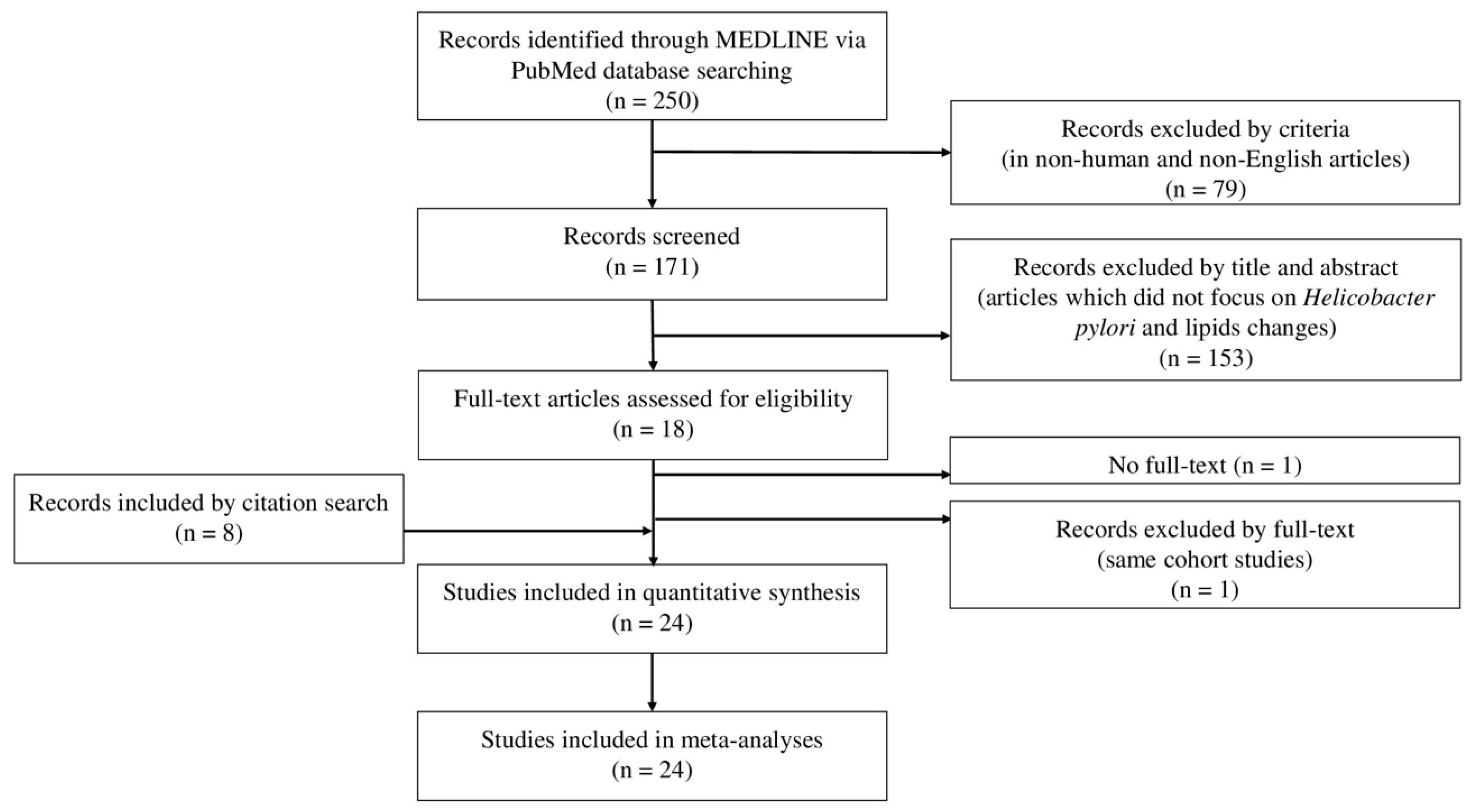
Figure 1 shows the process for selecting articles that examined the effect of H. pylori eradication on lipid changes. A total of 250 records were initially screened. After screening, eight studies were identified that had been included during the electronic hand search, and two were excluded because one did not have the full text available [18] and the other involved the same cohort as another study already included in the review [19]. Ultimately, 24 studies that evaluated the effect of H. pylori eradication on lipid changes were included in our meta-analysis [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43].
3.1. Mean Changes in Lipid Profiles after H. pylori Eradication
Table 1 summarizes the effect of H. pylori eradication on the lipid levels in 4 RCTs, 4 cohort studies, three case–control studies, and 13 before–after studies [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. The median values for HDL-C, TG, LDL-C, and TC before H. pylori eradication were 52.1 (range: 30.1 to 64.8) mg/dL, 128 (range: 80.2 to 177.0) mg/dL, 122.2 (range: 101.8 to 146.0) mg/dL, and 195.0 (range: 158.0 to 212.1) mg/dL, respectively, in Appendix A: Table A1, Table A2, Table A3 and Table A4. The median age reported in the included studies was 48.4 (range: 29.1 to 56.7) years old. The treatment period ranged from 7 to 14 days. The median rate of H. pylori eradication was 84.0% (range: 54.7% to 100%).
The quality of the reviewed randomized and non-randomized studies was scored (Supplementary Materials Figures S1–S2). The overall risks of bias in the four RCTs were classified as low risk in one and some concern in three due to an unclear randomization process, missing outcome data, and no protocol. The quality assessment of the 20 non-RCTs included moderate scores ranging from 4 to 7. The main reason for the downgrade was an unclear medication status for dyslipidemia in 16 of the non-RCTs.
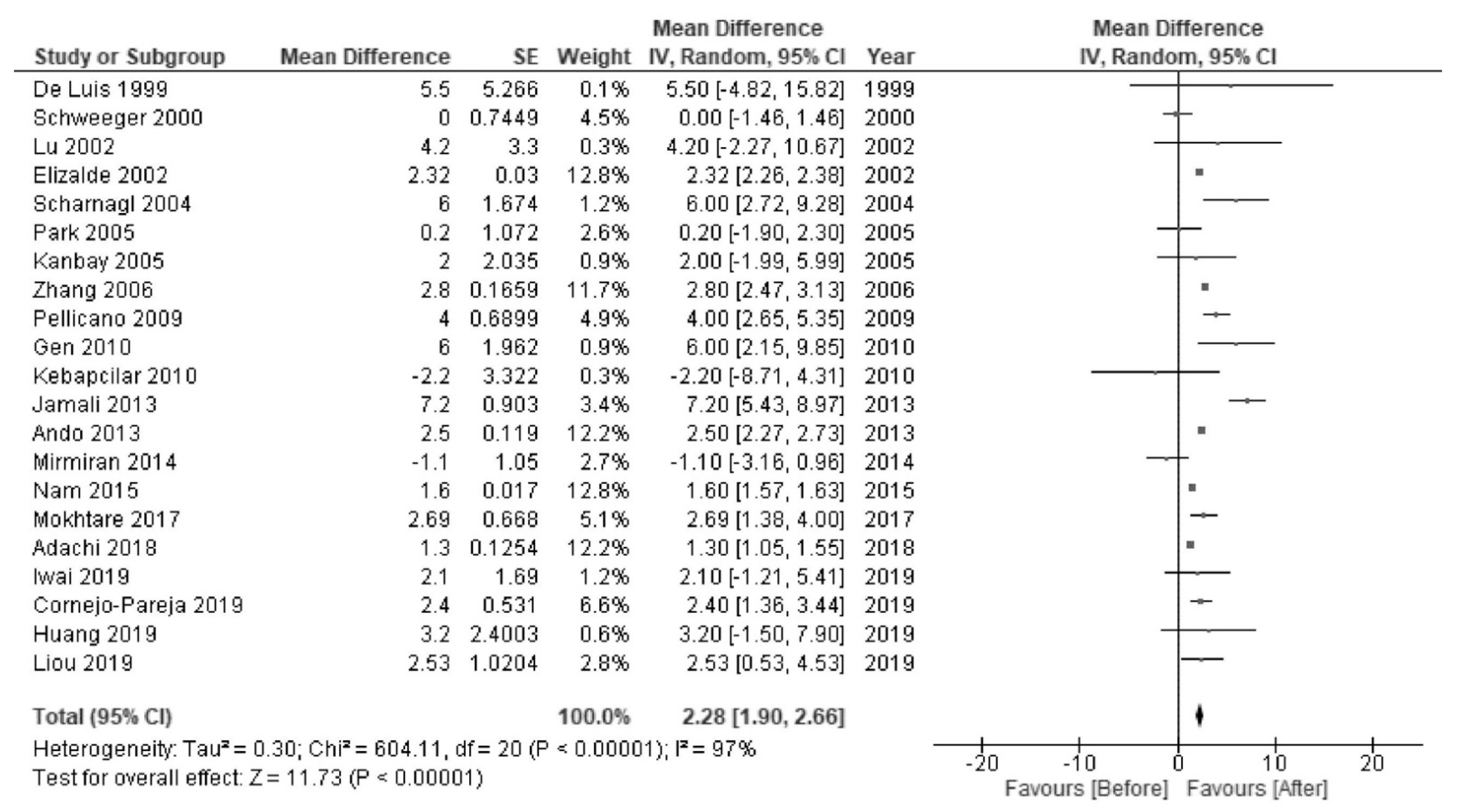
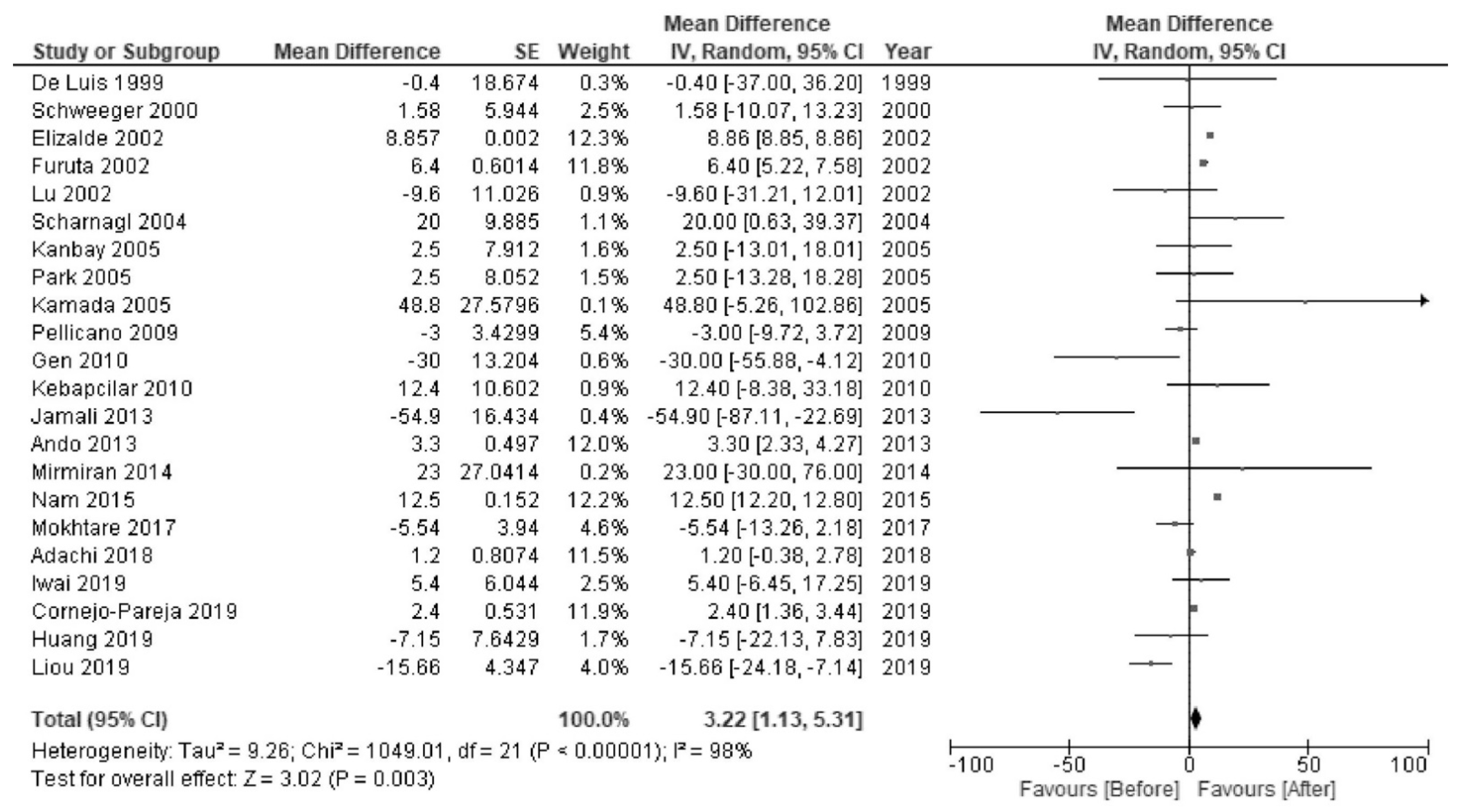
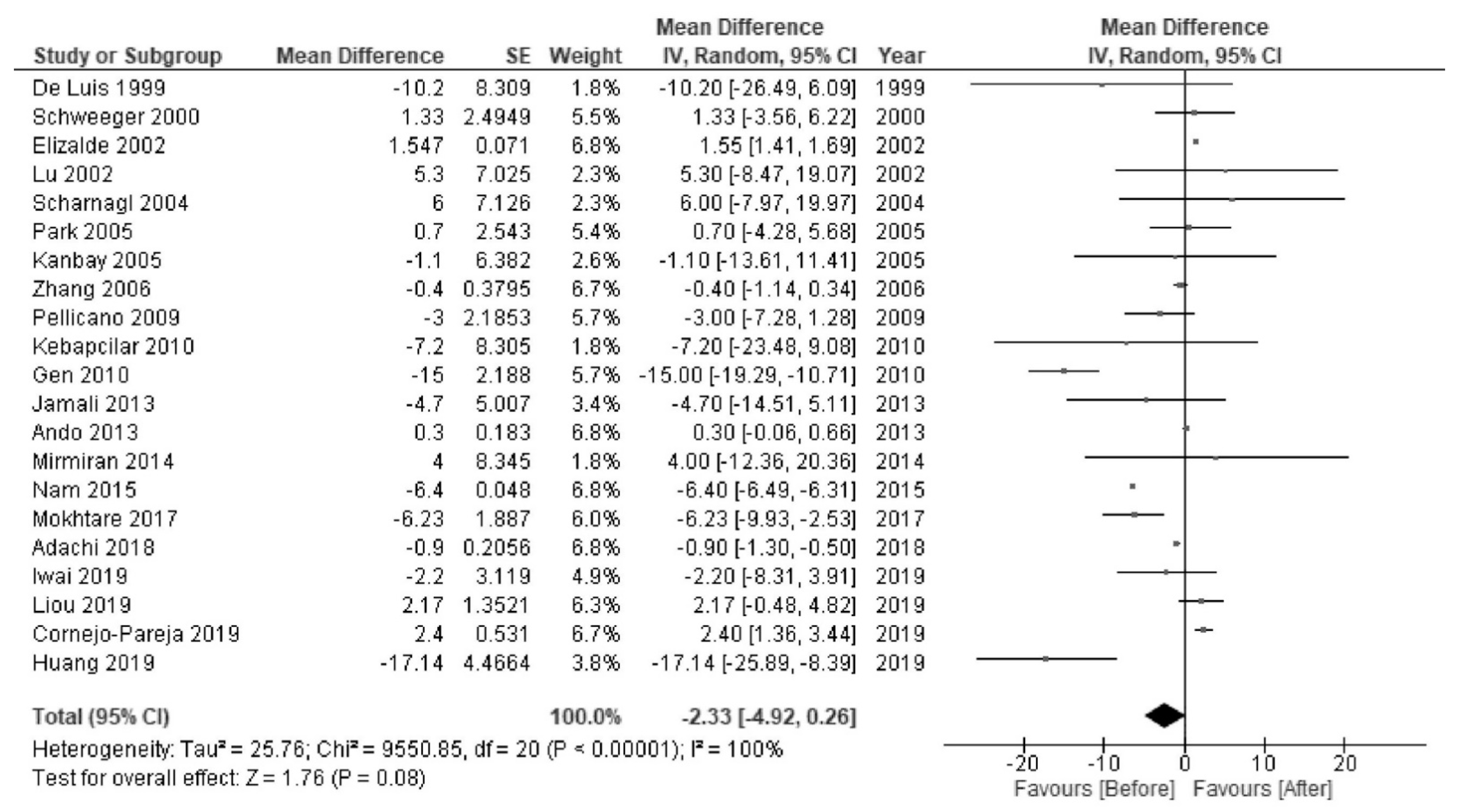
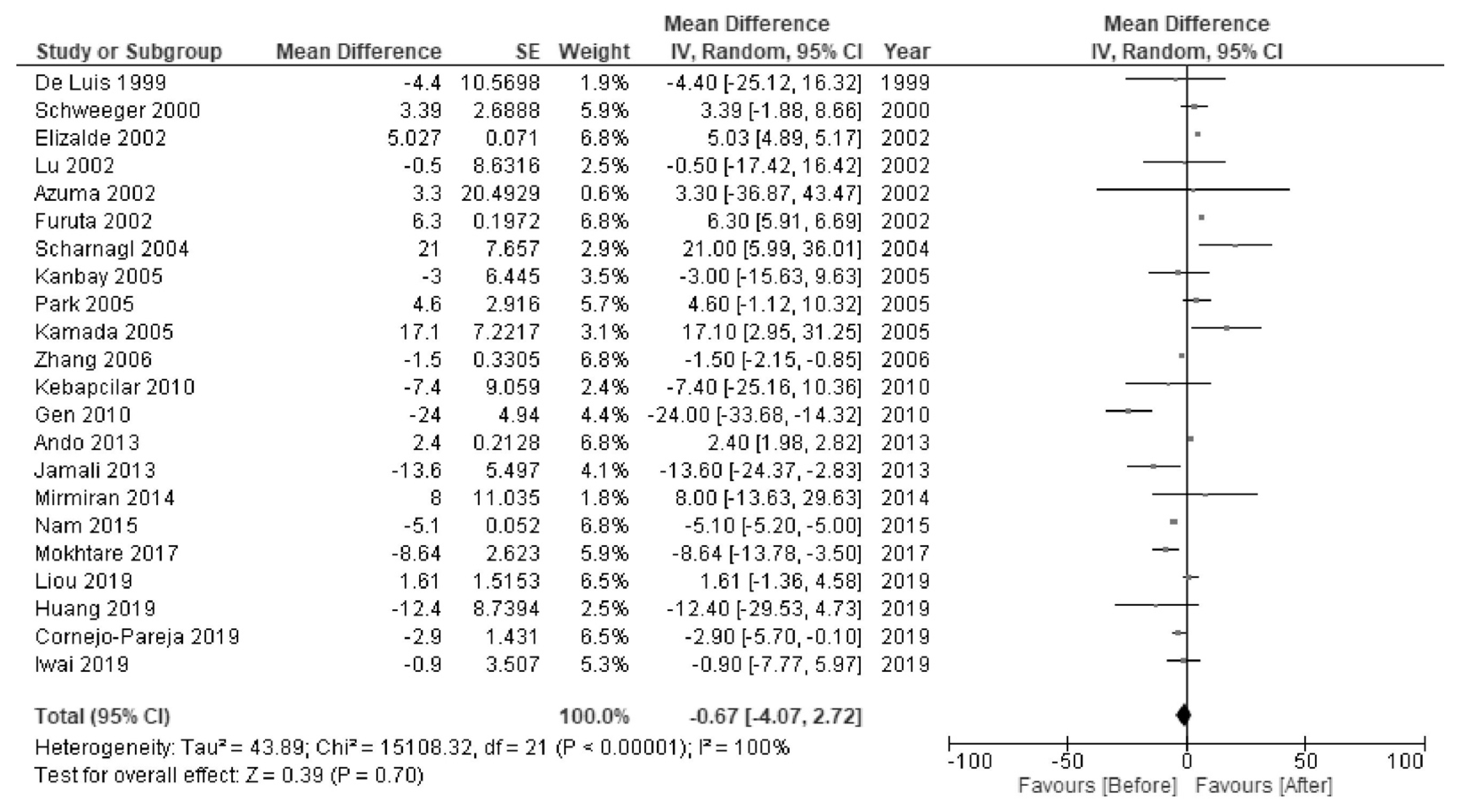
H. pylori eradication was associated with increased levels of HDL-C (MD 2.28 mg/dL; 95% CI 1.90 to 2.66; I2 = 97%; Figure 2) and TG (MD 3.22 mg/dL; 95% CI 1.13 to 5.31; I2 = 98%; Figure 3). There were no significant changes in the levels of LDL-C (MD −2.33 mg/dL; 95% CI −4.92 to 0.26; I2 = 100%; Figure 4) or TC (MD −0.67 mg/dL; 95% CI −4.07 to 2.72; I2 = 100%; Figure 5).
3.2. Sub-Group Analyses
In RCTs, H. pylori eradication increased the HDL-C levels (MD 2.90 mg/dL; 95% CI 0.38 to 5.42; I2 = 92%; Supplementary Materials Figure S3). H. pylori eradication resulted in little to no difference in the levels of TG, LDL-C and TC (Supplementary Materials Figures S4–S6). In sub-group analyses of the follow-up period, H. pylori eradication was associated with increased HDL-C levels at follow-up periods of both <1 year (MD 2.35 mg/dL; 1.81 to 2.89; I2 = 80%) and ≥1 year (MD 2.26 mg/dL; 1.67 to 2.85; I2 = 91%) (Supplementary Materials Figure S7). The sub-group analyses of TG, LDL-C, and TC showed no significant differences (Supplementary Materials Figures S8–S10). In sub-group analyses by country (study location), H. pylori eradication increased the levels of HDL-C regardless of country: Western countries (MD 2.81 mg/dL; 95% CI 1.73 to 3.90; I2 = 83%) and Asian countries (MD 2.00 mg/dL; 95% CI 1.90 to 2.66; I2 = 93%) (Supplementary Figure S11). There were no significant effects of H. pylori eradication on the TG, LDL-C, or TC levels in Western or Asian countries (Supplementary Materials Figures S12–S14).
3.3. Sensitivity Analyses
The sensitivity analyses with the exclusion of studies that did not describe the levels of HDL-C, TG, LDL-C, or TC before H. pylori eradication were consistent with the primary findings that H. pylori eradication increased the HDL-C levels (Supplementary Materials Figures S15–S18).
4. Discussion
The present study meta-analyzed the changes in the lipid levels following H. pylori eradication. The post-eradication HDL-C levels were increased compared with pre-eradication. However, the post-eradication change in TG levels were unclear, as the results of sub-analyses were not consistent across study designs. The post-eradication LDL-C levels showed little to no change. Since H. pylori infection is positively associated with CVD [2,3], finding a relationship of HDL-C (as a protective factor of CVD) with H. pylori eradication, among the evaluated lipids, is of interest. Understanding the overall changes in lipids following H. pylori eradication may also help us ponder over the connection between bacteria and lipid metabolism.
The increase of 2.28 mg/dL of HDL-C by H. pylori eradication might be slight. Furthermore, recent evidence indicates that an increase of HDL-C with drug therapies may not always be beneficial of the prevention of CVD events [44], and in this line, not only HDL-C levels but also HDL functionals (e.g., anti-inflammatory/oxidant capacity, cholesterol efflux) may be crucial [44]. The clinical relevance of change of HDL-C by H. pylori eradication would be thus discussed. For instance, a 1 mg/dL increase of HDL-C is reported to result in a 3–5% reduction in CVD risk [45]. The linear inverse association between HDL-C and CVD events is also reported at least up to 90 mg/dL in HDL-C [46]. In lifestyle modifications against CVD, exercise and diet increased approximately 1 mg/dL in HDL-C [47] and smoking secession increased approximately 4 mg/dL [48]. Therefore, the changes in HDL-C levels by H. pylori eradication, as observed in the present review, is thought to have clinical relevance on CVD, while there have been no studies on CVD outcomes or HDL functions by HDL-C levels after H. pylori eradication.
H. pylori infection leads to systemic inflammation [49] and oxidative stress [50]. Inflammation and oxidative stress cause a reduction in HDL-C levels [51,52]. Cytokines induce the inflammatory molecule, serum amyloid A, which replaces a major HDL component (apolipoprotein A-I), thereby reducing the HDL-C levels [53]. In addition, inflammation and oxidative stress alter HDL-C-related enzymes; for example, lecithin-cholesterol acyltransferase, cholesterol ester transfer protein, and hepatic lipase levels are reduced while endothelial lipase levels are increased, which can reduce the HDL-C levels [54,55]. Abnormal cholesterol transport is another reason for the reduction in HDL-C levels, a phenomenon seen in H. pylori infection [39,40]. As another etiological mechanism, the microbiome may be involved [56]. H. pylori infection alters the gut microbiota [57], and eradication with antibiotic treatments has been shown to alter the microbiota and reduce H. pylori-induced inflammation [58]. Microbial diversity in the gut microbiota (a favorable phenomenon) can increase the HDL-C levels as it improves the suppression of lipid metabolism (with inflammation and oxidative stress) via bacteria-derived bile acids and short-chain fatty acids [59]. As above-mentioned, in recent evidence [44], not only HDL-C levels but also HDL functions affect the development of CVD. As the functions can be associated with inflammation, oxidative stress and gut microbiota [60,61], future work on HDL, in relation to biomolecules of inflammation/oxidative stress and gut environment, under H. pylori eradication is expected to explain comprehensively the results of the present review.
The existence of H. pylori infection was cross-sectionally associated with a high level of TG [11], and the present review found a slight but additional increase in TG levels following H. pylori eradication. H. pylori eradication increases the appetite [49,62] and improves nutrition [24,63,64], which can often promote obesity. Reductions in hepatic lipase and cholesterol ester transfer protein by the suppression of inflammation following H. pylori eradication or the reduction in the activity of lipoprotein lipase by obesity (insulin resistance) can lead to an increase of TG following H. pylori eradication [48,65,66]. However, according to the results of a sub-analysis of RCTs only, the TG levels were not increased following H. pylori eradication. This may be partly explained by the notion that physiological changes in TG levels are unstably affected by fluctuating factors, such as the diet and individual responses to the diet [67].
The levels of LDL-C and TC did not change markedly following H. pylori eradication, the reasons for which were unclear. First, interestingly, the degree of gastric mucosal atrophy is indicated to be associated with the LDL-C levels [37,39,68]. As advanced atrophy does not clearly change even after H. pylori eradication, this may partially explain the finding of no marked post-eradication changes in the levels of LDL-C or TC. Second, the type of antibiotics in the H. pylori eradication regimen might be considered because antibiotics, especially metronidazole, can reduce serum cholesterol, especially LDL-C levels [69]. In the present review, two studies using metronidazole reduced LDL-C [21,26]. Further studies focusing on the types of antibiotics in the H. pylori eradication regimen, especially metronidazole, are needed to see the changes in the LDL-C and TC levels after eradication.
In the present review, the heterogeneity of the analysis of the effects of H. pylori eradication on HDL-C appeared to be high. The results of a sub-analysis of RCTs showed high heterogeneity relative to non-RCTs. This heterogeneity might depend not only on the study design but also the follow-up period, as a sub-analysis based on the follow-up periods (short- and long-term after eradication) alleviated the heterogeneity. Antibacterial agents for H. pylori eradication are effective at eliminating inflammation in the short term, while improvements in gastric mucosal atrophy and microbial diversification are gradually seen in the long term [58,70,71].
Several limitations associated with the present study warrant mention. First, most studies were not controlled for covariates, such as underlying diseases related to lipid levels (e.g., liver cirrhosis, nephrotic syndrome) [72,73]; however, patients with such diseases might have been inadvertently excluded from the view of no indication of drugs for eradication. Second, the methods for detecting H. pylori infection (e.g., a urea breath test with a comparatively high accuracy among diagnostic methods [74] or a combination of tests) differed among studies. Third, the CVD outcomes following changes in lipid values after H. pylori eradication was not observed in all studies. Forth, we could not perform the subgroup analyses (i.e., participants’ sex, successful/unsuccessful eradication of H. pylori), which seemed to give more information, since the individual data were not obtained from the original studies or only limited data on such items were available in the reviewed studies. In the present review including 24 studies, there were only four non-RCTs with the data regarding successful/unsuccessful eradication therapy.
In conclusion, H. pylori eradication increased the HDL-C levels. The findings suggested that H. pylori eradication alters lipid profiles favorably for CVD. The results of more RCTs are required to derive more definitive conclusions.
Supplementary Materials
The following are available online at https://www.mdpi.com/2077-0383/10/5/904/s1, Figure S1: Quality scores for the reviewed randomized studies, Figure S2: Quality scores for the reviewed non-randomized studies, Figure S3: Forest plot of the mean changes in high-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication for each study design, Figure S4: Forest plot of the mean changes in triglyceride levels before and after Helicobacter pylori eradication for each study design, Figure S5: Forest plot of the mean changes in low-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication for each study design, Figure S6: Forest plot of the mean changes in total cholesterol levels before and after Helicobacter pylori eradication for each study design, Figure S7: Forest plot of the mean changes in high-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication during < 1- or ≥ 1-year follow-up, Figure S8: Forest plot of the mean changes in triglyceride levels before and after Helicobacter pylori eradication during < 1- or ≥ 1-year follow-up, Figure S9: Forest plot of the mean changes in low-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication during < 1- or ≥ 1-year follow-up, Figure S10: Forest plot of the mean changes in total cholesterol levels before and after Helicobacter pylori eradication during < 1- or ≥ 1-year follow-up, Figure S11: Forest plot of the mean changes in high-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication in Western countries or Asia, Figure S12: Forest plot of the mean changes in triglyceride levels before and after Helicobacter pylori eradication in Western countries or Asia, Figure S13: Forest plot of the mean changes in low-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication in Western countries or Asia, Figure S14: Forest plot of the mean changes in total cholesterol levels before and after Helicobacter pylori eradication excluding studies which did not show the levels of HDL-C, TG, LDL-C and TC before H. pylori eradication, Figure S15: Forest plot of the mean changes in high-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication excluding studies which did not show the levels of high-density lipoprotein cholesterol before H. pylori eradication, Figure S16: Forest plot of the mean changes in triglyceride levels before and after Helicobacter pylori eradication excluding studies which did not show the levels of triglycerides before H. pylori eradication, Figure S17: Forest plot of the mean changes in low-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication excluding studies which did not show the levels of low-density lipoprotein cholesterol before H. pylori eradication.
Author Contributions
Conceptualization, J.W. and K.K.; methodology, J.W. and K.K.; software, J.W.; validation, J.W., M.H. and K.K.; formal analysis, J.W. and K.K.; investigation, J.W., M.H. and K.K.; resources, N/A; data curation, J.W., M.H. and K.K.; writing—original draft preparation, J.W.; writing, review and editing, J.W., M.H. and K.K.; visualization, J.W.; supervision, K.K.; project administration, J.W. and K.K.; funding acquisition, N/A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data have already been published in the academic literature.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
Summary of levels of high-density lipoprotein cholesterol before and after eradication.
| Authors (ref no.) | High-Density Lipoprotein Cholesterol Levels (mg/dL) | ||
|---|---|---|---|
| Before Eradication | After Eradication | Change Levels | |
| De Luis [20] | 59.7 ± 18.9 | 65.2 ± 15.9 | 5.5 |
| Schweeger [21] * | 45 ± 6 52 ± 5 | 45 ± 5 52 ± 5 | 0 0 |
| Elizalde [23] | - | - | 2.3 |
| Lu [25] | 49.7 ± 18.3 | 53.9 ± 13.7 | 4.2 |
| Scharnagl [26] | 36 ± 10 | 42 ± 12 | 6.0 |
| Kanbay [28] | 49.5 ± 10.3 | 51.5 ± 11.4 | 2.0 |
| Park [29] | 52.7 ± 13.7 | - | 0.2 |
| Zhank [30] | 56.8 ± 1.5 | 59.6 ± 1.2 | 2.8 |
| Pellicano [31] | 48 | 52 | 4.0 |
| Gen [32] | 37 ± 10 | 43 ± 9 | 6.0 |
| Kebapcilar [33] | 56.8 ± 13.5 | 54.6 ± 12.2 | −2.2 |
| Ando [34] | 63.2 ± 1.33 | 65.7 ± 1.27 | 2.5 |
| Jamali [35] | 44.5 ± 5.7 | 51.7 ± 7.0 | 7.2 |
| Mirmiran [36] | 30.1 ± 4.0 | 29.0 ± 3.4 | −1.1 |
| Nam [37] | - | - | 1.6 |
| Mokhtare [38] | - | - | 2.7 |
| Adachi [39] | 64.8 ± 1.2 | 66.1 ± 1.3 | 1.3 |
| Iwai [40] | 61.2 ± 14.7 | 63.3 ± 15.8 | 2.1 |
| Cornejo-Pareja [41] | 53.0 ± 2.0 | 55.4 ± 2.7 | 2.4 |
| Haung [42] | 33.6 ± 18.8 | 36.8 ± 19.0 | 3.2 |
| Liou [43] ** | 54.2 ± 16.3 53.0 ± 16.0 52.1 ± 16.1 | 58.2 ± 18.8 55.8 ± 17.5 52.7 ± 16.3 | 4.0 3.1 0.6 |
ref no., reference number. * Smoker and non-smoker ** Triple therapy for 14 days, concomitant therapy for 10 days, and bismuth quadruple therapy.
Table A2.
Summary of levels of triglycerides before and after eradication.
| Authors [ref no.] | Triglycerides Levels (mg/dL) | ||
|---|---|---|---|
| Before Eradication | After Eradication | Change Levels | |
| De Luis [20] | 103.2 ± 67.1 | 102.8 ± 56.3 | −0.4 |
| Schweeger [21] * | 171 ± 47 124 ± 36 | 169 ± 51 128 ± 37 | −2.0 4.0 |
| Elizalde [23] | - | - | 8.9 |
| Furuta [24] | 120.0 ± 10.0 | 126.4 ± 7.23 | 6.4 |
| Lu [25] | 110.5 ± 58.6 | 100.9 ± 49.0 | −9.6 |
| Scharnagl [26] | 128 ± 55 | 148 ± 74 | 20.0 |
| Kamada [27] | 125.3 ± 67.4 | 174.1 ± 183 | 48.8 |
| Kanbay [28] | 127.9 ± 63.7 | 129.6 ± 49.3 | 2.5 |
| Park [29] | 177.0 ± 192.9 | - | 2.5 |
| Pellicano [31] | 132 | 129 | −3.0 |
| Gen [32] | 159 ± 63 | 129 ± 65 | −30.0 |
| Kebapcilar [33] | 80.2 ± 30.2 | 92.6 ± 49.6 | 12.4 |
| Ando [34] | 109.3 ± 4.1 | 112.6 ± 6.6 | 3.3 |
| Jamali [35] | 174.8 ± 103.2 | 119.9 ± 48.1 | −54.9 |
| Mirmiran [36] | 131 ± 80 | 154 ± 109 | 23.0 |
| Nam [37] | - | - | 12.5 |
| Mokhtare [38] | - | - | −5.5 |
| Adachi [39] | 110.1 ± 7.8 | 111.3 ± 8.3 | 1.2 |
| Iwai [40] | 98.1 ± 50.9 | 103.5 ± 58.0 | 5.4 |
| Cornejo-Pareja [41] | 97.2 ± 6.3 | 93.5 ± 5.9 | 2.4 |
| Huang [42] | 157.5 ± 61.3 | 150.3 ± 59.1 | −7.2 |
| Liou [43] ** | 128.1 ± 94.8 139.1 ± 106.0 141.2 ± 97.6 | 119.0 ± 75.8 115.4 ± 63.0 127.0 ± 81.6 | −9.1 −23.7 −14.2 |
ref no., reference number. * Smoker and non-smoker ** Triple therapy for 14 days, concomitant therapy for 10 days, and bismuth quadruple therapy.
Table A3.
Summary of levels of low-density lipoprotein cholesterol before and after eradication.
| Authors [ref no.] | Low-Density Lipoprotein Cholesterol Levels (mg/dL) | ||
|---|---|---|---|
| Before Eradication | After Eradication | Change Levels | |
| De Luis [20] | 111.9 ± 28.2 | 101.7 ± 26.9 | −10.2 |
| Schweeger [21] * | 129 ± 17 114 ± 17 | 128 ± 18 118 ± 17 | −1.0 4.0 |
| Elizalde [23] | - | - | 1.5 |
| Lu [25] | 135.1 ± 37.6 | 140.4 ± 30.9 | 5.3 |
| Scharnagl [26] | 146 ± 47 | 157 ± 47 | 6.0 |
| Kanbay [28] | 125.4 ± 32.8 | 124.3 ± 35.3 | −1.1 |
| Park [29] | 123.6 ± 27.1 | - | 0.7 |
| Zhang [30] | 115.6 ± 3.1 | 115.2 ± 3.1 | −0.4 |
| Pellicano [31] | 140 | 137 | −3.0 |
| Gen [32] | 119 ± 12 | 104 ± 9 | −15.0 |
| Kebapcilar [33] | 111.7 ± 33.1 | 104.5 ± 31.2 | −7.2 |
| Ando [34] | 124.7 ± 2.0 | 125.0 ± 2.0 | 0.3 |
| Jamali [35] | 101.8 ± 25.7 | 91.5 ± 19.3 | −4.7 |
| Mirmiran [36] | 104 ± 29 | 108 ± 30 | 4.0 |
| Nam [37] | - | - | −6.4 |
| Mokhtare [38] | - | - | −6.2 |
| Adachi [39] | 131.1 ± 2.1 | 130.2 ± 2.0 | −0.9 |
| Iwai [40] | 121.2 ± 28.7 | 119.0 ± 27.6 | −2.2 |
| Cornejo-Pareja [41] | 121.5 ± 5.7 | 118.0 ± 5.2 | 2.4 |
| Huang [42] | 128.4 ± 39.4 | 111.3 ± 30.3 | −17.1 |
| Liou [43] ** | 122.2 ± 33.3 121.0 ± 31.0 122.3 ± 33.9 | 123.9 ± 34.0 124.1 ± 33.5 123.9 ± 34.3 | 1.7 3.1 1.6 |
ref no., reference number. * Smoker and non-smoker ** Triple therapy for 14 days, concomitant therapy for 10 days, and bismuth quadruple therapy.
Table A4.
Summary of levels of total cholesterol before and after eradication.
| Authors (ref no.) | Total Cholesterol Levels (mg/dL) | ||
|---|---|---|---|
| Before Eradication | After Eradication | Change Levels | |
| De Luis [20] | 191.2 ± 35.7 | 186.8 ± 34.4 | −4.4 |
| Schweeger [21] * | 215 ± 25 196 ± 17 | 216 ± 19 201 ± 16 | 1.0 5.0 |
| Azuma [22] | 200.8 ± 31.6 | 204.1 ± 36.8 | 3.3 |
| Elizalde [23] | - | - | 5.0 |
| Furuta [24] | 191.1 ± 3.1 | 197.4 ± 2.6 | |
| Lu [25] | 209.2 ± 44.0 | 208.7 ± 40.5 | −0.5 |
| Scharnagl [26] | 208 ± 50 | 229 ± 51 | 21.0 |
| Kamada [27] | 204.1 ± 33.2 | 221.2 ± 38.8 | 17.1 |
| Kanbay [28] | 208 ± 33.8 | 205 ± 35 | −3.0 |
| Park [29] | 212.1 ± 38.7 | - | 4.6 |
| Zhang [30] | 190.6 ± 2.7 | 189.1 ± 2.7 | −1.5 |
| Gen [32] | 212 ± 28 | 188 ± 19 | −24.0 |
| Kebapcilar [33] | 180.2 ± 31.3 | 172.8 ± 38.5 | −7.4 |
| Ando [34] | 209.9 ± 2.27 | 212.3 ± 2.4 | 2.4 |
| Jamali [35] | 180.8 ± 31.9 | 167.2 ± 20.8 | −13.6 |
| Mirmiran [36] | 158 ± 38 | 166 ± 40 | 8.0 |
| Nam [37] | - | - | −5.1 |
| Mokhtare [38] | - | - | −8.6 |
| Iwai [40] | 206.0 ± 32.5 | 205.1 ± 30.8 | −0.9 |
| Cornejo-Pareja [41] | 194.2 ± 6.5 | 191.3 ± 6.3 | −2.9 |
| Huang [42] | 182.7 ± 70.2 | 170.3 ± 67.4 | −12.4 |
| Liou [43] ** | 194.8 ± 38.4 194.0 ± 35.0 195.0 ± 37.0 | 197.0 ± 36.6 196.7 ± 37.5 196.0 ± 38.9 | 1.0 2.7 1.0 |
ref no., reference number. * Smoker and non-smoker ** Triple therapy for 14 days, concomitant therapy for 10 days, and bismuth quadruple therapy.
References
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG clinical guideline: Treatment of Helicobacter pylori infection. Am. J. Gastroenterol. 2017, 112, 212–238. [Google Scholar] [CrossRef]
- Budzyński, J.; Koziński, M.; Kłopocka, M.; Kubica, J.M.; Kubica, J. Clinical significance of Helicobacter pylori infection in patients with acute coronary syndromes: An overview of current evidence. Clin. Res. Cardiol. 2014, 103, 855–886. [Google Scholar] [CrossRef] [PubMed]
- Katsiki, N.; Athyros, V.G.; Karagiannis, A.; Mikhailidis, D.P. High-density lipoprotein, vascular risk, cancer and infection: A case of quantity and quality? Curr. Med. Chem. 2014, 21, 2917–2926. [Google Scholar] [CrossRef]
- McNeill, A.M.; Rosamond, W.D.; Girman, C.J.; Golden, S.H.; Schmidt, M.I.; East, H.E.; Ballantyne, C.M.; Heiss, G. The metabolic syndrome and 11-year risk of incident cardiovascular disease in the atherosclerosis risk in communities study. Diabetes Care 2005, 28, 385–390. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Levy, D.; Vasan, R.S.; Wang, T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: A historical perspective. Lancet 2014, 383, 999–1008. [Google Scholar] [CrossRef]
- Toth, P.P. Triglyceride-rich lipoproteins as a causal factor for cardiovascular disease. Vasc. Health Risk Manag. 2016, 12, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Saito, I.; Yamagishi, K.; Kokubo, Y.; Yatsuya, H.; Iso, H.; Sawada, N.; Inoue, M.; Tsugane, S. Association of high-density lipoprotein cholesterol concentration with different types of stroke and coronary heart disease: The Japan Public Health Center-based prospective (JPHC) study. Atherosclerosis 2017, 265, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, R.; Hoogeveen, R.M.; Langsted, A.; Stiekema, L.C.A.; Verweij, S.L.; Hovingh, G.K.; Wareham, N.J.; Khaw, K.T.; Boekholdt, S.M.; Nordestgaard, B.G.; et al. Cardiovascular disease risk associated with elevated lipoprotein(a) attenuates at low low-density lipoprotein cholesterol levels in a primary prevention setting. Eur. Heart J. 2018, 39, 2589–2596. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Couret, D.; Tran-Dinh, A.; Duranteau, J.; Montravers, P.; Schwendeman, A.; Meilhac, O. High-density lipoproteins during sepsis: From bench to bedside. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef]
- Afshar, M.; Rong, J.; Zhan, Y.; Chen, H.Y.; Engert, J.C.; Sniderman, A.D.; Larson, M.G.; Vasan, R.S.; Thanassoulis, G. Risks of incident cardiovascular disease associated with concomitant elevations in lipoprotein(a) and low-density lipoprotein cholesterol-the Framingham Heart Study. J. Am. Heart Assoc. 2020, 9, e014711. [Google Scholar] [CrossRef] [PubMed]
- Shimamoto, T.; Yamamichi, N.; Gondo, K.; Takahashi, Y.; Takeuchi, C.; Wada, R.; Mitsushima, T.; Koike, K. The association of Helicobacter pylori infection with serum lipid profiles: An evaluation based on a combination of meta-analysis and a propensity score-based observational approach. PLoS ONE 2020, 15, e0234433. [Google Scholar] [CrossRef] [PubMed]
- Upala, S.; Sanguankeo, A.; Saleem, S.A.; Jaruvongvanich, V. Effects of Helicobacter pylori eradication on insulin resistance and metabolic parameters: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2017, 29, 153–159. [Google Scholar] [CrossRef]
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Losos, M.; Tugwell, P.; Ottawa Hospital Research Institute. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses, 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 December 2020).
- Goudet, S.M.; Bogin, B.A.; Madise, N.J.; Griffiths, P.L. Nutritional interventions for preventing stunting in children (Birth to 59 months) living in urban slums in low-and middle-income countries (LMIC). Cochrane Database Syst. Rev. 2019, 6, CD011695.1. [Google Scholar] [CrossRef] [PubMed]
- Jayaraman, S.; Sethi, D.; Wong, R. Advanced training in trauma life support for ambulance crews. Cochrane Database Syst. Rev. 2014, 2014, CD003109.1. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (Updated July 2019). Cochrane 2019. Available online: https://training.cochrane.org/handbook/current (accessed on 16 December 2020).
- Kowalski, M. Helicobacter pylori (H. pylori) infection in coronary artery disease: Influence of H. pylori eradication on coronary artery lumen after percutaneous transluminal coronary angioplasty. The detection of H. pylori specific DNA in human coronary atherosclerotic plaque. J. Physiol. Pharmacol. 2001, 52, 3–31. [Google Scholar]
- Adachi, K.; Mishiro, T.; Toda, T.; Kano, N.; Fujihara, H.; Mishima, Y.; Konishi, A.; Mochida, M.; Takahashi, K.; Kinoshita, Y. Effects of Helicobacter pylori eradication on serum lipid levels. J. Clin. Biochem. Nutr. 2018, 62, 264–269. [Google Scholar] [CrossRef]
- De Luis, D.A.; Avello, A.G.; Lasuncion, M.A.; Aller, R.; De Argila, C.M.; De Miquel, D.B.; De La Calle, H. Improvement in lipid and haemostasis patterns after Helicobacter pylori infection eradication in type 1 diabetic patients. Clin. Nutr. 1999, 18, 227–231. [Google Scholar] [CrossRef]
- Schweeger, I.; Fitscha, P.; Sinzinger, H. Successful eradication of Helicobacter pylori as determined by 13C-urea breath test does not alter fibrinogen and acute phase response markers. Thromb. Res. 2000, 97, 411–420. [Google Scholar] [CrossRef]
- Azuma, T.; Suto, H.; Ito, Y.; Muramatsu, A.; Ohtani, M.; Dojo, M.; Yamazaki, Y.; Kuriyama, M.; Kato, T. Eradication of Helicobacter pylori infection induces an increase in body mass index. Aliment. Pharmacol. Ther. 2002, 16, 240–244. [Google Scholar] [CrossRef]
- Elizalde, J.I.; Piqué, J.M.; Moreno, V.; Morillas, J.D.; Elizalde, I.; Bujanda, L.; De Argila, C.M.; Cosme, A.; Castiella, A.; Ros, E. Influence of Helicobacter pylori infection and eradication on blood lipids and fibrinogen. Aliment Pharmaco. Ther. 2002, 16, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Shirai, N.; Xiao, F.; Takashima, M.; Hanai, H. Effect of Helicobacter pylori infection and its eradication on nutrition. Aliment. Pharmacol. Ther. 2002, 16, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.H.; Yen, H.W.; Lin, T.H.; Huang, C.H.; Lee, K.T.; Wang, W.M.; Wu, D.C.; Voon, W.C.; Lai, W.T.; Sheu, S.H. Changes of coronary risk factors after eradication of Helicobacter pylori infection. Kaohsiung J. Med. Sci. 2002, 18, 266–272. [Google Scholar] [PubMed]
- Scharnagl, H.; Kist, M.; Grawitz, A.B.; Koenig, W.; Wieland, H.; März, W. Effect of Helicobacter pylori eradication on high-density lipoprotein cholesterol. Am. J. Cardiol. 2004, 93, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Hata, J.; Kusunoki, H.; Ito, M.; Tanaka, S.; Kawamura, Y.; Chayama, K.; Haruma, K. Eradication of Helicobacter pylori increases the incidence of hyperlipidaemia and obesity in peptic ulcer patients. Dig. Liver Dis. 2005, 37, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; Gür, G.; Yücel, M.; Yilmaz, U.; Boyacioĝlu, S. Does eradication of Helicobacter pylori infection help normalize serum lipid and CRP levels? Dig. Dis. Sci. 2005, 50, 1228–1231. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Jeon, W.K.; Kim, S.H.; Kim, H.J.; Park, D.; Cho, Y.K.; Sung, I.K.; Sohn, C.; Kim, B.I.; Keum, D.K. Helicobacter pylori eradication has no effect on metabolic and inflammatory parameters. J. Natl. Med. Assoc. 2005, 97, 508–513. [Google Scholar]
- Zhang, L.; Gail, M.H.; Wang, Y.Q.; Brown, L.M.; Pan, K.F.; Ma, J.L.; Amagase, H.; You, W.C.; Moslehi, R. A randomized factorial study of the effects of long-term garlic and micronutrient supplementation and of 2-wk antibiotic treatment for Helicobacter pylori infection on serum cholesterol and lipoproteins. Am. J. Clin. Nutr. 2006, 84, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, R.; Oliaro, E.; Fagoonee, S.; Astegiano, M.; Berrutti, M.; Saracco, G.; Smedile, A.; Repici, A.; Leone, N.; Castelli, A.; et al. Clinical and biochemical parameters related to cardiovascular disease after Helicobacter pylori eradication. Int. Angiol. 2009, 28, 469–473. [Google Scholar]
- Gen, R.; Demir, M.; Ataseven, H. Effect of Helicobacter pylori eradication on insulin resistance, serum lipids and low-grade inflammation. South. Med. J. 2010, 103, 190–196. [Google Scholar] [CrossRef]
- Kebapcilar, L.; Bilgir, O.; Cetinkaya, E.; Akyol, M.; Bilgir, F.; Bozkaya, G. The effect of Helicobacter pylori eradication on macrophage migration inhibitory factor, c-reactive protein and fetuin-a levels. Clinics 2010, 65, 799–802. [Google Scholar] [CrossRef]
- Ando, T.; Ishikawa, T.; Takagi, T.; Imamoto, E.; Kishimoto, E.; Okajima, A.; Uchiyama, K.; Handa, O.; Yagi, N.; Kokura, S.; et al. Impact of Helicobacter pylori eradication on circulating adiponectin in humans. Helicobacter 2013, 18, 158–164. [Google Scholar] [CrossRef]
- Jamali, R.; Mofid, A.; Vahedi, H.; Farzaneh, R.; Dowlatshahi, S. The effect of Helicobacter pylori eradication on liver fat content in subjects with non-alcoholic fatty liver disease: A randomized open-label clinical trial. Hepat. Mon. 2013, 13, e14679. [Google Scholar] [CrossRef] [PubMed]
- Mirmiran, P.; Bahadoran, Z.; Golzarand, M.; Zojaji, H.; Azizi, F. A comparative study of broccoli sprouts powder and standard triple therapy on cardiovascular risk factors following H. pylori eradication: A randomized clinical trial in patients with type 2 diabetes. J. Diabetes Metab. Disord. 2014, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.Y.; Ryu, K.H.; Park, B.J.; Park, S. Effects of Helicobacter pylori infection and its eradication on lipid profiles and cardiovascular diseases. Helicobacter 2015, 20, 125–132. [Google Scholar] [CrossRef]
- Mokhtare, M.; Mirfakhraee, H.; Arshad, M.; Samadani Fard, S.H.; Bahardoust, M.; Movahed, A.; Masoodi, M. The effects of Helicobacter pylori eradication on modification of metabolic syndrome parameters in patients with functional dyspepsia. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S1031–S1035. [Google Scholar] [CrossRef]
- Adachi, K.; Mishiro, T.; Okimoto, E.; Kinoshita, Y. Influence of the degree of gastric mucosal atrophy on the serum lipid levels before and after the eradication of Helicobacter pylori infection. Intern. Med. 2018, 57, 3067–3073. [Google Scholar] [CrossRef] [PubMed]
- Iwai, N.; Okuda, T.; Oka, K.; Hara, T.; Inada, Y.; Tsuji, T.; Komaki, T.; Inoue, K.; Dohi, O.; Konishi, H.; et al. Helicobacter pylori eradication increases the serum high density lipoprotein cholesterol level in the infected patients with chronic gastritis: A single-center observational study. PLoS ONE 2019, 14, e0221349. [Google Scholar]
- Cornejo-Pareja, I.; Martín-Núñez, G.; Roca-Rodríguez, M.; Cardona, F.; Coin-Aragüez, L.; Sánchez-Alcoholado, L.; Gutiérrez-Repiso, C.; Muñoz-Garach, A.; Fernández-García, J.; Moreno-Indias, I.; et al. H. pylori Eradication Treatment Alters Gut Microbiota and GLP-1 Secretion in Humans. J. Clin. Med. 2019, 8, 451. [Google Scholar] [CrossRef]
- Huang, B.; Yan, S.; Chen, C.; Ye, S. Correction to: Effect of 25-hydroxyvitaminD on Helicobacter pylori eradication in patients with type 2 diabetes. Wien Klin. Wochenschr. 2019, 131, 48. [Google Scholar] [CrossRef]
- Liou, J.M.; Chen, C.C.; Chang, C.M.; Fang, Y.J.; Bair, M.J.; Chen, P.Y.; Chang, C.Y.; Hsu, Y.C.; Chen, M.J.; Chen, C.C.; et al. Taiwan Gastrointestinal Disease and Helicobacter Consortium. Long-term changes of gut microbiota, antibiotic resistance, and metabolic parameters after Helicobacter pylori eradication: A multicentre, open-label, randomised trial. Lancet Infect. Dis. 2019, 19, 1109–1120. [Google Scholar] [CrossRef]
- Smit, R.A.; Jukema, J.W.; Trompet, S. Increasing HDL-C levels with medication: Current perspectives. Curr. Opin. Lipidol. 2017, 28, 361–366. [Google Scholar] [CrossRef]
- Chirovsky, D.R.; Fedirko, V.; Cui, Y.; Sazonov, V.; Barter, P. Prospective studies on the relationship between high-density lipoprotein cholesterol and cardiovascular risk: A systematic review. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 404–423. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, J.T.; Ning, H.; Stone, N.J.; Criqui, M.H.; Zhao, L.; Greenland, P.; Lloyd-Jones, D.M. Coronary heart disease risks associated with high levels of HDL cholesterol. J. Am. Heart Assoc. 2014, 3, e000519. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Devlin, H.M.; Smith, B.; Imperatore, G.; Thomas, W.; Lobelo, F.; Ali, M.K.; Norris, K.; Gruss, S.; Bardenheier, B.; et al. Effect of lifestyle interventions on cardiovascular risk factors among adults without impaired glucose tolerance or diabetes: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0176436. [Google Scholar] [CrossRef] [PubMed]
- Kar, D.; Gillies, C.; Zaccardi, F.; Webb, D.; Seidu, S.; Tesfaye, S.; Davies, M.; Khunti, K. Relationship of cardiometabolic parameters in non-smokers, current smokers, and quitters in diabetes: A systematic review and meta-analysis. Cardiovasc. Diabetol. 2016, 15, 158. [Google Scholar] [CrossRef]
- Shiotani, A.; Miyanishi, T.; Uedo, N.; Iishi, H. Helicobacter pylori infection is associated with reduced circulating ghrelin levels independent of body mass index. Helicobacter 2005, 10, 373–378. [Google Scholar] [CrossRef]
- Aslan, M.; Horoz, M.; Nazligul, Y.; Bolukbas, C.; Bolukbas, F.F.; Selek, S.; Celik, H.; Erel, O. Insulin resistance in H pylori infection and its association with oxidative stress. World J. Gastroenterol. 2006, 12, 6865–6868. [Google Scholar] [CrossRef]
- Rohrer, L.; Hersberger, M.; von Eckardstein, A. High density lipoproteins in the intersection of diabetes mellitus, inflammation and cardiovascular disease. Curr. Opin. Lipidol. 2004, 15, 269–278. [Google Scholar] [CrossRef]
- Nessler, K.; Windak, A.; Grzybczak, R.; Nessler, M.B.; Siniarski, A.; Gajos, G. High-density lipoprotein (Hdl) cholesterol– more complicated than we think? Ann. Agric. Environ. Med. 2018, 25, 517–526. [Google Scholar] [CrossRef]
- Yanai, H.; Yoshida, H. Beneficial effects of adiponectin on glucose and lipid metabolism and atherosclerotic progression: Mechanisms and perspectives. Int. J. Mol. Sci. 2019, 20, 1190. [Google Scholar] [CrossRef]
- Feingold, K.R.; Grunfeld, C. Effect of inflammation on HDL structure and function. Curr. Opin. Lipidol. 2016, 27, 521–530. [Google Scholar] [CrossRef]
- Aslan, M.; Nazligul, Y.; Horoz, M.; Bolukbas, C.; Bolukbas, F.F.; Gur, M.; Celik, H.; Erel, O. Serum paraoxonase-1 activity in Helicobacter pylori infected subjects. Atherosclerosis 2008, 196, 270–274. [Google Scholar] [CrossRef]
- Schoeler, M.; Caesar, R. Dietary lipids, gut microbiota and lipid metabolism. Rev. Endocr. Metab. Disord. 2019, 20, 461–472. [Google Scholar] [CrossRef]
- Brawner, K.M.; Kumar, R.; Serrano, C.A.; Ptacek, T.; Lefkowitz, E.; Morrow, C.D.; Zhi, D.; Kyanam-Kabir-Baig, K.R.; Smythies, L.E.; Harris, P.R.; et al. Helicobacter pylori infection is associated with an altered gastric microbiota in children. Mucosal Immunol. 2017, 10, 1169–1177. [Google Scholar] [CrossRef]
- Rolig, A.S.; Cech, C.; Ahler, E.; Carter, J.E.; Ottemann, K.M. The degree of Helicobacter pylori-triggered inflammation is manipulated by preinfection host microbiota. Infect. Immun. 2013, 81, 1382–1389. [Google Scholar] [CrossRef]
- Vojinovic, D.; Radjabzadeh, D.; Kurilshikov, A.; Amin, N.; Wijmenga, C.; Franke, L.; Ikram, M.A.; Uitterlinden, A.G.; Zhernakova, A.; Fu, J.; et al. Relationship between gut microbiota and circulating metabolites in population-based cohorts. Nat. Commun. 2019, 10, 5813. [Google Scholar] [CrossRef]
- Tsoupras, A.; Lordan, R.; Zabetakis, I. Inflammation, not cholesterol, is a cause of chronic disease. Nutrients 2018, 10, 604. [Google Scholar] [CrossRef]
- Tang, W.H.W.; Bäckhed, F.; Landmesser, U.; Hazen, S.L. Intestinal microbiota in cardiovascular health and disease: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2019, 73, 2089–2105. [Google Scholar] [CrossRef]
- Mantero, P.; Matus, G.S.; Corti, R.E.; Cabanne, A.M.; Gabriel, G.; De Palma, Z.; Olid, L.M.; Piskorz, M.M.; Zubillaga, M.B.; De Palma, G.G.Z.; et al. Helicobacter pylori and corpus gastric pathology are associated with lower serum ghrelin. World J. Gastroenterol. 2018, 24, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, T.; Fukuda, S.; Tanaka, M.; Mikami, T.; Yamagata, R.; Yoshimura, T.; Haga, Y.; Murata, Y.; Munakata, A. Healing of cimetidine-resistant Menetrier’s disease by eradication of Helicobacter pylori infection. J. Clin. Gastroenterol. 1998, 27, 348–350. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, M.; Hizawa, K.; Aoyagi, K.; Nakamura, S.; Fujishima, M. Ménétrièr’s disease associated with Helicobacter pylori infection: Resolution of enlarged gastric folds and hypoproteinemia after antibacterial treatment. Am. J. Gastroenterol. 1997, 92, 1909–1912. [Google Scholar] [PubMed]
- Dongiovanni, P.; Stender, S.; Pietrelli, A.; Mancina, R.M.; Cespiati, A.; Petta, S.; Pelusi, S.; Pingitore, P.; Badiali, S.; Maggioni, M.; et al. Causal relationship of hepatic fat with liver damage and insulin resistance in nonalcoholic fatty liver. J. Intern. Med. 2018, 283, 356–370. [Google Scholar] [CrossRef]
- Kolovou, G.; Anagnostopoulou, K.; Kostakou, P.; Mikhailidis, D. Cholesterol ester transfer protein (CETP), postprandial lipemia and hypolipidemic drugs. Curr. Med. Chem. 2009, 16, 4345–4360. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.; Britton, A.; Black, N.; McPherson, K.; Sanderson, C.; Bain, C. Methods in health services research. Interpreting the evidence: Choosing between randomised and non-randomised studies. BMJ 1999, 319, 312–315. [Google Scholar] [CrossRef]
- Kucukazman, M.; Yavuz, B.; Sacikara, M.; Asilturk, Z.; Ata, N.; Ertugrul, D.T.; Yalcin, A.A.; Yenigun, E.C.; Kizilca, G.; Okten, H.; et al. The relationship between updated Sydney system score and LDL cholesterol levels in patients infected with Helicobacter pylori. Dig. Dis. Sci. 2009, 54, 604–607. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Kendall, C.W.; Hamidi, M.; Vidgen, E.; Faulkner, D.; Parker, T.; Irani, N.; Wolever, T.M.; Fong, I.; Kopplin, P.; et al. Effect of antibiotics as cholesterol-lowering agents. Metabolism 2005, 54, 103–112. [Google Scholar] [CrossRef]
- Salih, B.A.; Abasiyanik, M.F.; Saribasak, H.; Huten, O.; Sander, E. A follow-up study on the effect of Helicobacter pylori eradication on the severity of gastric histology. Dig. Dis. Sci. 2005, 50, 1517–1522. [Google Scholar] [CrossRef]
- Ye, Q.; Shao, X.; Shen, R.; Chen, D.; Shen, J. Changes in the human gut microbiota composition caused by Helicobacter pylori eradication therapy: A systematic review and meta-analysis. Helicobacter 2020, 25, e12713. [Google Scholar] [CrossRef]
- Navarese, E.P.; Robinson, J.G.; Kowalewski, M.; Kołodziejczak, M.; Andreotti, F.; Bliden, K.; Tantry, U.; Kubica, J.; Raggi, P.; Gurbel, P.A. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering a systematic review and meta-analysis. JAMA 2018, 319, 1566–1579. [Google Scholar] [CrossRef]
- Haskell, S.G.; Bathulapalli, H.; Pham, T.; Goulet, J.; Skanderson, M.; Driscoll, M.; Brandt, C.; Dziura, J. Sex differences in patient and provider response to elevated low-density lipoprotein cholesterol. Women’s Health Issues 2014, 24, 575–580. [Google Scholar] [CrossRef]
- Best, L.M.J.; Takwoingi, Y.; Siddique, S.; Selladurai, A.; Gandhi, A.; Low, B.; Yaghoobi, M.; Gurusamy, K.S. Non-invasive diagnostic tests for Helicobacter pylori infection. Cochrane Database Syst. Rev. 2018, 3, CD012080. [Google Scholar] [PubMed]
Figure 1.
Flow chart of article selection.

Figure 2.
Forest plot of the mean changes in high-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication.
Figure 2.
Forest plot of the mean changes in high-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication.

Figure 3.
Forest plot of the mean changes in triglyceride levels before and after Helicobacter pylori eradication.
Figure 3.
Forest plot of the mean changes in triglyceride levels before and after Helicobacter pylori eradication.

Figure 4.
Forest plot of the mean changes in low-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication.
Figure 4.
Forest plot of the mean changes in low-density lipoprotein cholesterol levels before and after Helicobacter pylori eradication.

Figure 5.
Forest plot of the mean changes in total cholesterol levels before and after Helicobacter pylori eradication.
Figure 5.
Forest plot of the mean changes in total cholesterol levels before and after Helicobacter pylori eradication.

Table 1.
Summary of the characteristics of the included studies.
| Authors [ref no.] | Year | Design | Country | Subjects (n) | Age (Years) | Therapy Duration (Days) | Follow-Up (Months) | Eradication Rate (%) |
|---|---|---|---|---|---|---|---|---|
| De Luis [20] | 1999 | Before–after study | Spain | 22 | 45.1 | 10 | 0.25 | 73.3 |
| Schweeger [21] | 2000 | Before–after study | Austria | 100 | 50.3 | 14 | 1 | - |
| Azuma [22] | 2002 | Cohort study | Japan | 241 | 42.9 | 7 | 12 | 79.8 |
| Elizalde [23] | 2002 | Before–after study | Spain | 368 | 47 | 7 | 0.25 | 79.0 |
| Furuta [24] | 2002 | Cohort study | Japan | 421 | 48 | 7 | 12 | - |
| Lu [25] | 2002 | Before–after study | Taiwan | 48 | 50.8 | 7 | 0.17 | 100 |
| Scharnagl [26] | 2004 | Before–after study | Austria | 87 | 52 | 7–14 | 1.00 | - |
| Kamada [27] | 2005 | Cohort study | Japan | 50 | 50.9 | 7 | 12 | 71.4 |
| Kanbay [28] | 2005 | Before–after study | Turkey | 57 | 49.9 | 14 | 0.17 | 100 |
| Park [29] | 2005 | Case–control study | Korea | 87 | 44.7 | 7 | 1.00 | 100 |
| Zhang [30] | 2006 | Randomized control trial | China | 136 | 51.1 | 14 | 48 | - |
| Pellicano [31] | 2009 | Before–after study | Itary | 496 | 59.7 | - | <60 | - |
| Gen [32] | 2010 | Before–after study | Tukey | 47 | 32.8 | 14 | 6.00 | 54.7 |
| Kebapcilar [33] | 2010 | Case–control study | Tukey | 30 | 29.1 | 14 | - | 65.2 |
| Ando [34] | 2013 | Before–after study | Japan | 241 | - | 7 | 0.13 | 71.3 |
| Jamali [35] | 2013 | Randomized control trial | Iran | 48 | 43.8 | 14 | 0.46 | 96.0 |
| Mirmiran [36] | 2014 | Randomized control trial | Iran | 25 | - | 14 | 0.08 | 89.3 |
| Nam [37] | 2015 | Cohort study | Korea | 529 | - | 7 | 1–3 | 88.6 |
| Mokhtare [38] | 2017 | Before–after study | Iran | 91 | 41.2 | 14 | 0.25 | 62.6 |
| Adachi [39] | 2018 | Cohort study | Japan | 199 | 53.2 | - | 12 | - |
| Iwai [40] | 2019 | Before–after study | Japan | 163 | 56.7 | 14 | 1.41 | 84.0 |
| Cornejo-Pareja [41] | 2019 | Case–control study | Spain | 40 | 40 | 10 | 3 | 97.5 |
| Hung [42] | 2019 | Cohort study | China | 124 | 48.4 | 14 | 1 | 93.8 |
| Liou [43] | 2019 | Randomized control trial | Taiwan | 1620 | 53 | 10 or 14 | 12 | 87–95 |
n, number; ref no., reference number.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Watanabe, J.; Hamasaki, M.; Kotani, K. The Effect of Helicobacter pylori Eradication on Lipid Levels: A Meta-Analysis. J. Clin. Med. 2021, 10, 904. https://doi.org/10.3390/jcm10050904
AMA Style
Watanabe J, Hamasaki M, Kotani K. The Effect of Helicobacter pylori Eradication on Lipid Levels: A Meta-Analysis. Journal of Clinical Medicine. 2021; 10(5):904. https://doi.org/10.3390/jcm10050904
Chicago/Turabian StyleWatanabe, Jun, Masato Hamasaki, and Kazuhiko Kotani. 2021. "The Effect of Helicobacter pylori Eradication on Lipid Levels: A Meta-Analysis" Journal of Clinical Medicine 10, no. 5: 904. https://doi.org/10.3390/jcm10050904
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.