
A Propensity Score-Matched Analysis to Assess the Outcomes in Pre- and Post-Fast-Track Hip and Knee Elective Prosthesis Patients

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Design and Setting
2.2. Implementation of the FT Protocol
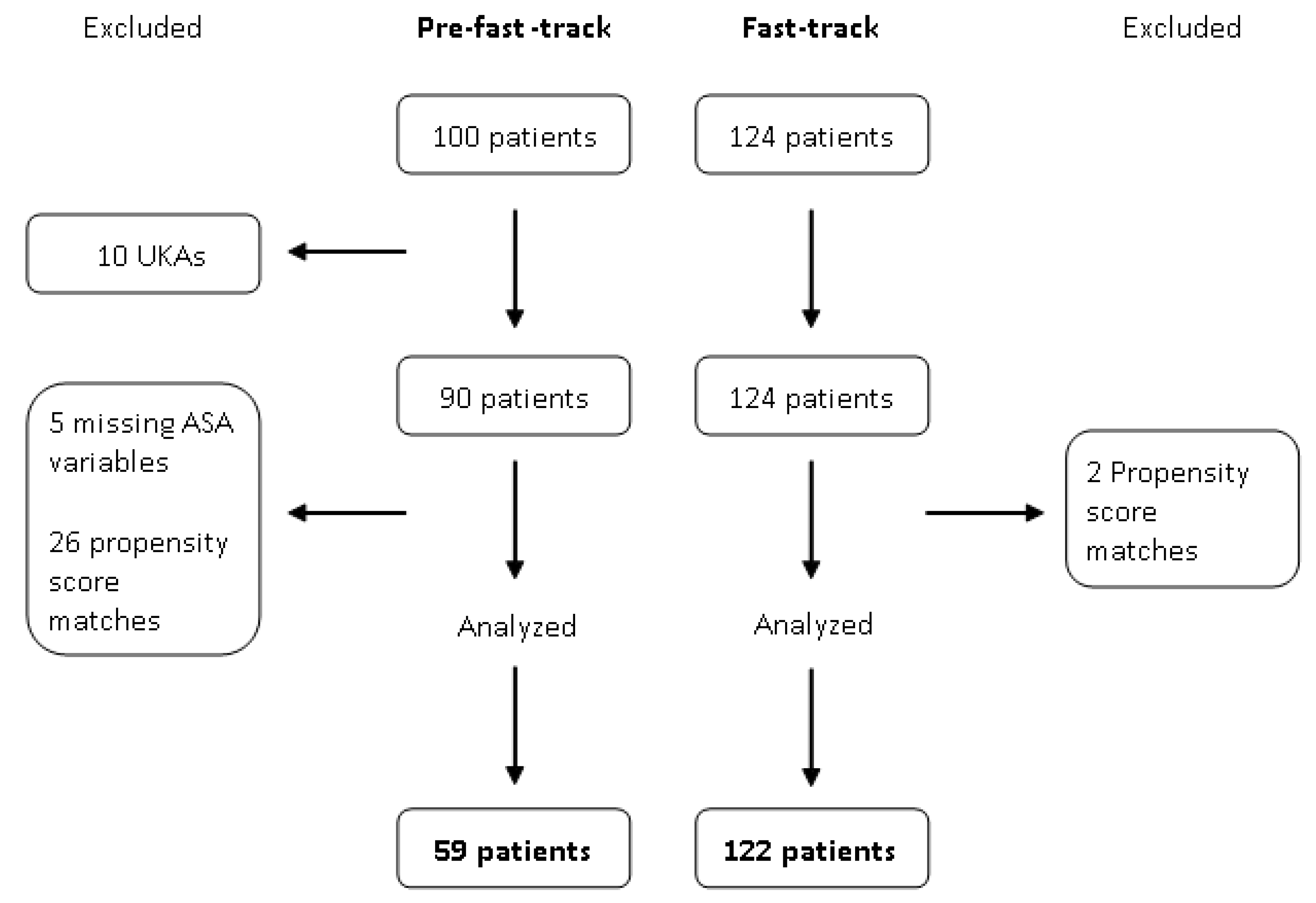
2.3. Study Population
2.4. Data Sources, Variables, and Outcomes
- mean hemoglobin drop;
- mean predischarge hemoglobin;
- number and percentages of hemotransfusions;
- number and percentages of blood reinfusions;
- first day pain score (number and percentage of patients with a numerical rating scale (NRS) < 4);
- accomplishment of postoperative ambulation;
- hospital length of stay;
- discharge setting (i.e., to home/outpatient rehabilitation or rehabilitation center).
- median tourniquet time (knee replacement);
- median surgery time (hip and knee replacements);
- use of bladder catheter or surgical drain;
- type of anesthesia (i.e., subarachnoid, general, or combined anesthesia performed as selective subarachnoid anesthesia and short-acting sedative hypnotic agents, see Table 1).
2.5. Statistical Analyses
3. Results
3.1. Patient Cohorts
3.2. Short-Term Outcomes
3.3. Compliance with the FT Protocol
3.4. Complications and Readmissions
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of total hip and knee replacement in the United States. J. Bone Jt. Surg. Am. 2015, 97, 1386–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aasvang, E.K.; Luna, I.E.; Kehlet, H. Challenges in postdischarge function and recovery: The case of fast-track hip and knee arthroplasty. Br. J. Anaesth. 2015, 115, 861–866. [Google Scholar] [CrossRef] [Green Version]
- Sutton, J.C.; Antoniou, J.; Epure, L.M.; Huk, O.L.; Zukor, D.J.; Bergeron, S.G. Hospital discharge within 2 days following total hip or knee arthroplasty does not increase major-complication and readmission rates. J. Bone Jt. Surg. Am. 2016, 98, 1419–1428. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, S.E.; Holm, H.B.; Jørgensen, M.; Gromov, K.; Kjærsgaard-Andersen, P.; Husted, H. Time-Driven activity-based cost of fast-track total hip and knee arthroplasty. J. Arthroplast. 2017, 32, 1747–1755. [Google Scholar] [CrossRef]
- Kehlet, H. Fast-Track colorectal surgery. Lancet Lond. Engl. 2008, 371, 791–793. [Google Scholar] [CrossRef]
- Kehlet, H. Fast-Track hip and knee arthroplasty. Lancet Lond. Engl. 2013, 381, 1600–1602. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Pros and cons of fast-track total knee arthroplasty. Int. J. Orthop. 2015, 2, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Ansari, D.; Gianotti, L.; Schröder, J.; Andersson, R. Fast-Track surgery: Procedure-specific aspects and future direction. Langenbecks Arch. Surg. 2013, 398, 29–37. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Hubner, M. Enhanced Recovery after Surgery-ERAS-Principles, practice and feasibility in the elderly. Aging Clin. Exp. Res. 2018, 30, 249–252. [Google Scholar] [CrossRef] [Green Version]
- Zhu, S.; Qian, W.; Jiang, C.; Ye, C.; Chen, X. Enhanced recovery after surgery for hip and knee arthroplasty: A systematic review and meta-analysis. Postgrad. Med. J. 2017, 93, 736–742. [Google Scholar] [CrossRef]
- Wainwright, T.W.; Kehlet, H. Fast-Track hip and knee arthroplasty—Have we reached the goal? Acta Orthop. 2019, 90, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Coenders, M.J.; Mathijssen, N.M.C.; Vehmeijer, S.B.W. Three and a half years’ experience with outpatient total hip arthroplasty. Bone Jt. J. 2020, 102-B, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Merchán, E.C. Outpatient total knee arthroplasty: Is it worth considering? EFORT Open Rev. 2020, 5, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.B. Fast Track in Hip Arthroplasty. EFORT Open Rev. 2017, 2, 179–188. [Google Scholar] [CrossRef]
- Soffin, E.M.; YaDeau, J.T. Enhanced recovery after surgery for primary hip and knee arthroplasty: A review of the evidence. Br. J. Anaesth. 2016, 117, iii62–iii72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memtsoudis, S.G.; Poeran, J.; Kehlet, H. Enhanced recovery after surgery in the United States: From evidence-based practice to uncertain science? JAMA 2019, 321, 1049–1050. [Google Scholar] [CrossRef]
- Kehlet, H.; Memtsoudis, S.G. ERAS Guidelines for hip and knee replacement—Need for reanalysis of evidence and recommendations? Acta Orthop. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponti, M.; Zanella, M.; Bartoli, D.; Chiti, L.J.; Baldini, A. Programma di recupero funzionale “Fast-Track” dopo protesi totale di anca e ginocchio: Selezione del paziente, educazione preoperatoria, controllo sanguinamento e dolore, scelta dell’approccio chirurgico. GIOT 2015, 41 (Suppl. 1), S237–S244. [Google Scholar]
- Moráis, S.; Ortega-Andreu, M.; Rodríguez-Merchán, E.C.; Padilla-Eguiluz, N.G.; Pérez-Chrzanowska, H.; Figueredo-Zalve, R.; Gómez-Barrena, E. Blood transfusion after primary total knee arthroplasty can be significantly minimised through a multimodal blood-loss prevention approach. Int. Orthop. 2014, 38, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Rigoni, M.; Torri, E.; Nollo, G.; Zarantonello, D.; Laudon, A.; Sottini, L.; Guarrera, G.M.; Brunori, G. Survival and time-to-transplantation of peritoneal dialysis versus hemodialysis for end-stage renal disease patients: Competing-risks regression model in a single Italian center experience. J. Nephrol. 2017, 30, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Lovecchio, F.; Alvi, H.; Sahota, S.; Beal, M.; Manning, D. Is outpatient arthroplasty as safe as fast-track inpatient arthroplasty? A propensity score matched analysis. J. Arthroplasty 2016, 31, 197–201. [Google Scholar] [CrossRef]
- Lindberg-Larsen, M.; Pitter, F.T.; Husted, H.; Kehlet, H.; Jørgensen, C.C. Lundbeck Foundation Centre for Fast-Track Hip and Knee Replacement Collaborative Group simultaneous vs staged bilateral total knee arthroplasty: A propensity-matched case-control study from nine fast-track centers. Arch. Orthop. Trauma Surg. 2019, 139, 709–716. [Google Scholar] [CrossRef]
- Berg, U.; BüLow, E.; Sundberg, M.; Rolfson, O. No increase in readmissions or adverse events after implementation of fast-track program in total hip and knee replacement at 8 Swedish hospitals: An observational before-and-after study of 14,148 total joint replacements 2011–2015. Acta Orthop. 2018, 89, 522–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masaracchio, M.; Hanney, W.J.; Liu, X.; Kolber, M.; Kirker, K. Timing of rehabilitation on length of stay and cost in patients with hip or knee joint arthroplasty: A systematic review with meta-analysis. PLoS ONE 2017, 12, e0178295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maempel, J.F.; Clement, N.D.; Ballantyne, J.A.; Dunstan, E. Enhanced recovery programmes after total hip arthroplasty can result in reduced length of hospital stay without compromising functional outcome. Bone Jt. J. 2016, 98-B, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.-F.; Gu, H.-Y.; Peng, W.-Y.; Zhang, Q.; Huang, Z.-D.; Zhang, C.; Yu, Y.-X. Impact of enhanced recovery after surgery on postoperative recovery after joint arthroplasty: Results from a systematic review and meta-analysis. Postgrad. Med. J. 2018, 94, 678–693. [Google Scholar] [CrossRef]
- Hu, Z.-C.; He, L.-J.; Chen, D.; Li, X.-B.; Feng, Z.-H.; Fu, C.-W.; Xuan, J.-W.; Ni, W.-F.; Wu, A.-M. An enhanced recovery after surgery program in orthopedic surgery: A systematic review and meta-analysis. J. Orthop. Surg. 2019, 14, 77. [Google Scholar] [CrossRef] [Green Version]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced recovery after surgery: A review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| FT Elements and Care Phases | FT Protocol Practices | Pre-FT |
|---|---|---|
| Preadmission Care | ||
| Education and counseling |
|
|
| Assessment and optimization of diseases/comorbidities |
|
|
| Preoperative and Intraoperative Care | ||
| Liberal fasting and carbohydrate loading |
| |
| Pre-emptive oral analgesia |
|
|
| Standardized anesthetic protocol and multimodal analgesia |
|
|
| Minimally invasive surgery |
|
|
| Blood conservation |
|
|
| Avoidance of drains and tubes |
| |
| Perioperative fluid management |
|
|
| Prevention of hypothermia |
|
|
| Postoperative care | ||
| Postoperative analgesia |
|
|
| Blood conservation and wound management |
|
|
| Preventing and treating postoperative nausea and vomiting |
|
|
| Early oral intake |
|
|
| Early mobilization andphysiotherapy |
|
|
| Characteristics | Pre-FT (59 Patients) | FT (122 Patients) | p-Value |
|---|---|---|---|
| Age, median (Q1–Q3), years | 73 (68–77) | 70 (64–77) | 0.06 |
| Male, n (%) | 28 (47) | 67 (55) | 0.35 |
| Female, n (%) | 31 (53) | 55 (45) | |
| Hip, n (%) | 30 (51) | 63 (52) | 0.92 |
| Knee, n (%) | 29 (49) | 59 (48) | |
| Presurgery Hb, mean (SD) g/dL | 14.2 (1.3) | 14.1 (1.3) | 0.71 |
| ASA physical status classification system 1, n (%) | 11 (19%) | 35 (29%) | 0.15 |
| ASA physical status classification system 2, n (%) | 41 (69%) | 66 (54%) | 0.15 |
| ASA physical status classification system 3, n (%) | 7 (12%) | 21 (17%) | 0.15 |
| Outcomes | Pre-FT | FT | Effect Measures (95% CI) | p-Value |
|---|---|---|---|---|
| 59 patients | 122 patients | |||
| Mean Hb drop (g/dl), mean (SD) | 3.7 (1.3) | 3.1 (1.2) | <0.01 § | |
| Mean predischarge Hb (g/dl), mean (SD) | 10.5 (1.1) | 11.0 (1.3) | 0.01 § | |
| Hemotransfusion, n (%) | 26 (44) | 17 (14) | 0.19 (0.09–0.40) $ | <0.01 |
| Blood reinfusion, n (%) | 37 (63) | 0 (0) | −0.63 (−0.75 to −0.50) * | <0.01 |
| Pain NRS scale <4 (first day), n (%) | 21 (35) | 94 (77) | 6.34 (3.15–12.79) $ | <0.01 |
| Patients ambulating in the first 24 h, n (%) | 0 (0) | 111 (91) | 0.91 (0.86–0.96) * | <0.01 |
| Hospital length of stay, median (Q1–Q3) | 8 (8–10) | 5 (4–6) | <0.01 # | |
| Discharge to hospital rehabilitation center, n (%) | 57 (97) | 45 (37) | 0.02 (0.01–0.06) $ | <0.01 |
| Home discharge, n (%) | 2 (3) | 72 (59) | 41.9 (12.1–144.9) $ | <0.01 |
| Measure | Pre-FT | FT | Effect Measures (95% CI) | p-Value |
|---|---|---|---|---|
| 59 patients | 122 patients | |||
| Tourniquet time, median (Q1–Q3), minutes | 61 (54–69.5) | 35 (30–41) | <0.01 # | |
| Surgery time, median (Q1–Q3), minutes | 106 (94–115) | 86 (77–92) | <0.01 # | |
| Bladder catheter, n (%) | 16 (27) | 10 (8) | 0.19 (0.08–0.43) $ | <0.01 |
| Surgical drain, n (%) | 54 (92) | 0 (0) | −0.92 (−0.99 to −0.84) * | <0.01 |
| Subarachnoidanesthesia, n (%) | 34 (57) | 6 (5) | −0.53 (−0.66 to −0.40) * | <0.01 |
| General anesthesia, n (%) | 17 (28) | 11 (10) | −0.20 (−0.32 to −0.07) * | <0.01 |
| Combined anesthesia, n (%) | 9 (15) | 104 (85) | 0.70 (0.59 to 0.81) * | <0.01 |
| Outcomes | Pre-FT | FT | Crude OR (95% CI) | p-Value |
|---|---|---|---|---|
| Patients with 1 or more complications | 59 patients | 122 patients | ||
| 1 month, n (%) | 25 (43.1) | 47 (38.2) | 0.85 (0.45–1.61) OR | 0.63 |
| 6 months, n (%) | 14 (23.7) | 10 (8.0) | 0.29 (0.12–0.67) OR | <0.01 |
| 12 months, n (%) | 15 (25.4) | 6 (4.9) | 0.15 (0.06–0.38) OR | <0.01 |
| 24 months, n (%) | 11 (18.6) | 2 (1.6) | 0.07 (0.02–0.25) OR | <0.01 |
| 36 months, n (%) | 9 (15.2) | 1 (0.8) | 0.05 (0.01–0.21) OR | <0.01 |
| Hospital readmissions within 36 months, n (%) | 4 (6.8) | 4 (3.3) | 0.46 (0.11–1.88) OR | 0.44 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, L.U.; Rigoni, M.; Torri, E.; Nella, M.; Morandi, M.; Casetti, P.; Nollo, G. A Propensity Score-Matched Analysis to Assess the Outcomes in Pre- and Post-Fast-Track Hip and Knee Elective Prosthesis Patients. J. Clin. Med. 2021, 10, 741. https://doi.org/10.3390/jcm10040741
Romano LU, Rigoni M, Torri E, Nella M, Morandi M, Casetti P, Nollo G. A Propensity Score-Matched Analysis to Assess the Outcomes in Pre- and Post-Fast-Track Hip and Knee Elective Prosthesis Patients. Journal of Clinical Medicine. 2021; 10(4):741. https://doi.org/10.3390/jcm10040741
Chicago/Turabian StyleRomano, Luigi U., Marta Rigoni, Emanuele Torri, Marilena Nella, Monica Morandi, Piergiorgio Casetti, and Giandomenico Nollo. 2021. "A Propensity Score-Matched Analysis to Assess the Outcomes in Pre- and Post-Fast-Track Hip and Knee Elective Prosthesis Patients" Journal of Clinical Medicine 10, no. 4: 741. https://doi.org/10.3390/jcm10040741