
Estimation of the Periodontal Inflamed Surface Area by Simple Oral Examination

 ,
,  ,
,  , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Setting
2.1.2. Diagnosis
2.2. Research Data
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Participant Characteristics
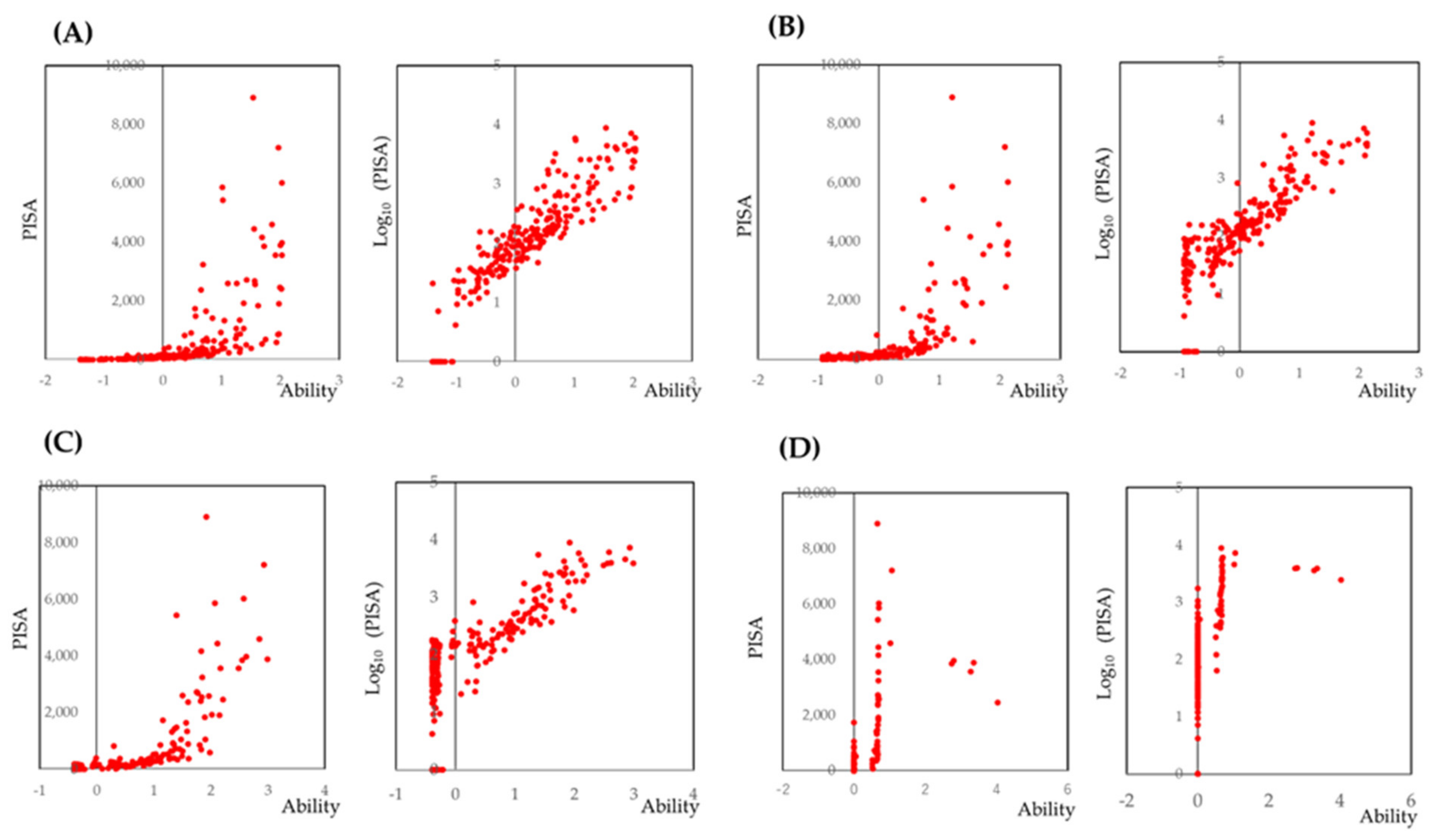
3.2. Prediction of PISA by IRT Analysis Based on the Number of BOP Sites
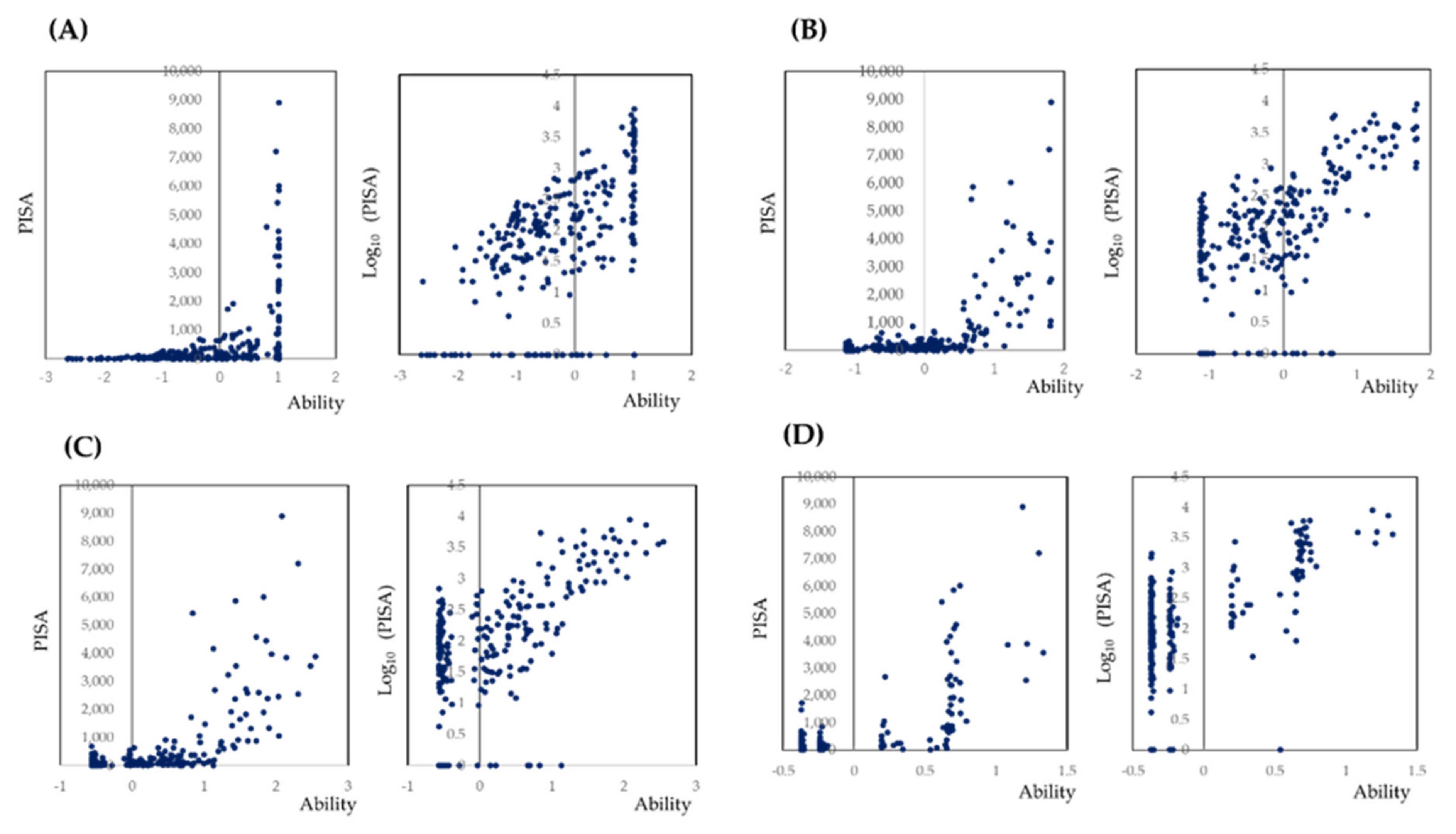
3.3. Prediction of PISA by the Maximum Value of the PD at Each Tooth by IRT Analysis
3.4. Prediction of PISA Based on the Selected Sites
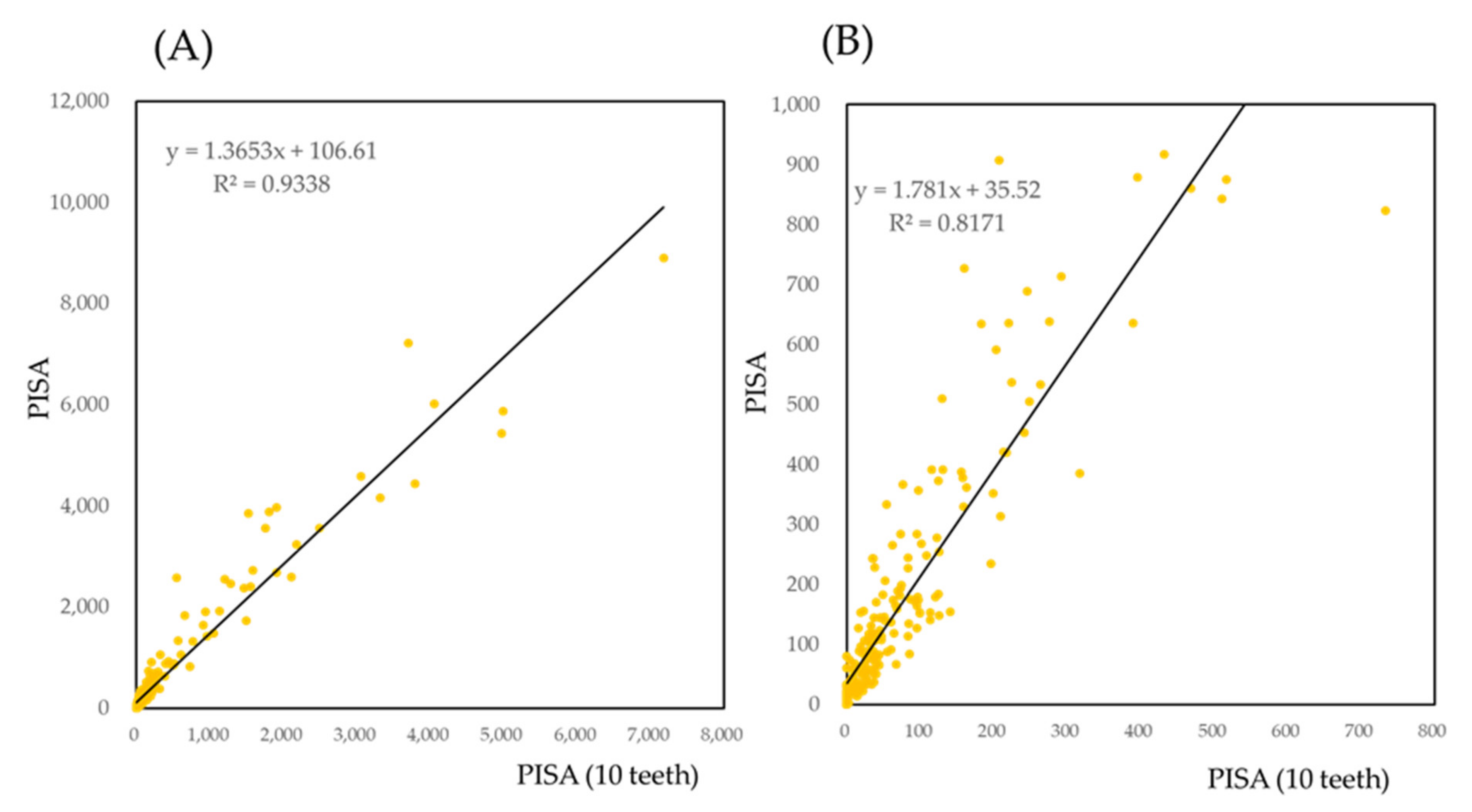
3.5. Prediction of PISA Based on the Selected Teeth
3.5.1. Correlation of PISA of Selected Teeth with PISA
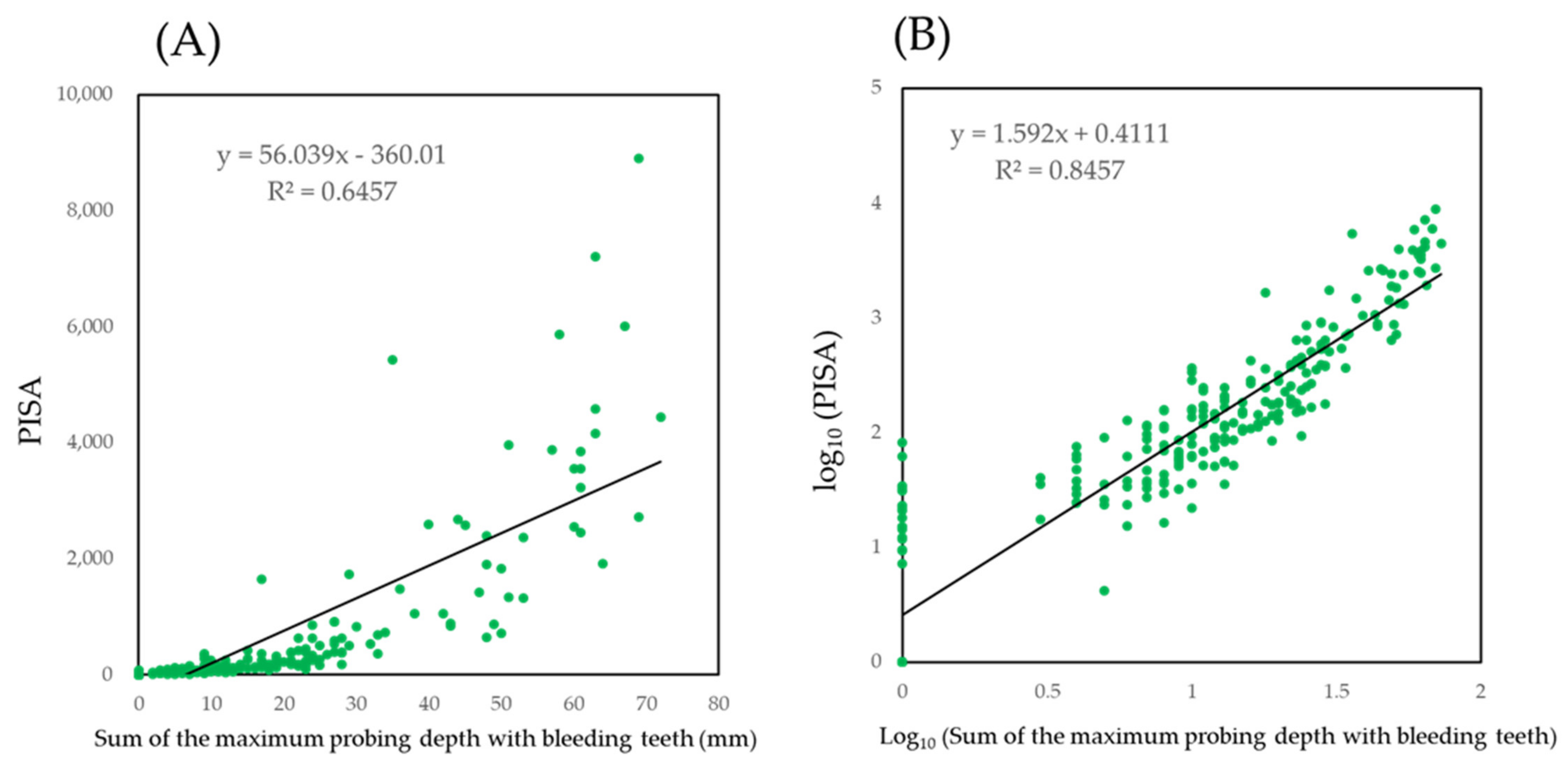
3.5.2. Prediction of PISA by the Maximum Value of PD
bleeding of selected teeth) + 0.4111
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomas, J.T.; Thomas, T.; Ahmed, M.; Kannan, S.K.; Abdullah, Z.; Alghamdi, S.A.; Joseph, B. Prevalence of Periodontal Disease among Obese Young Adult Population in Saudi Arabia-A Cross-Sectional Study. Medicina 2020, 56, 197. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Kim, J. Dairy Food Consumption is Inversely Associated with the Prevalence of Periodontal Disease in Korean Adults. Nutrients 2019, 11, 1035. [Google Scholar] [CrossRef] [Green Version]
- Cengiz, M.İ.; Zengin, B.; İçen, M.; Köktürk, F. Prevalence of periodontal disease among mine workers of Zonguldak, Kozlu District, Turkey: A cross-sectional study. BMC Public Health 2018, 18, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.Y.; Jiang, H.; Du, M.Q.; Wang, X.; Feng, X.P.; Hu, Y.; Lin, H.C.; Wang, B.; Si, Y.; Wang, C.X.; et al. The Prevalence and Associated Factors of Periodontal Disease among 35 to 44-year-old Chinese Adults in the 4th National Oral Health Survey. Chin. J. Dent. Res. 2018, 21, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, A.; Soares, S.; Lopes, H.; Santos, J.N.; Ramalho, L.M.; Cangussu, M.C.; Cury, P.R. Destructive periodontal disease in adult Indians from Northeast Brazil: Cross-sectional study of prevalence and risk indicators. J. Clin. Periodontol. 2013, 40, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Salih, Y.; Nasr, A.M.; Ahmed, A.B.A.; Sharif, M.E.; Adam, I. Prevalence of and risk factors for periodontal disease among pregnant women in an antenatal care clinic in Khartoum, Sudan. BMC Res. Notes 2020, 13, 147. [Google Scholar] [CrossRef]
- García, B.M.; Plana, C.J.M.; González, A.P.I. Prevalence and severity of periodontal disease among Spanish military personnel. BMJ Mil. Health 2020. [Google Scholar] [CrossRef] [Green Version]
- Bostancı, V.; Toker, H.; Senel, S.; Sahin, S. Prevalence of periodontal disease in patients with Familial Mediterranean Fever: A cohort study from central Turkey. Quintessence Int. 2014, 45, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Bains, V.K.; Jhingran, R.; Srivastava, R.; Madan, R.; Maurya, S.C.; Rizvi, I. Prevalence of Periodontal Disease in Type 2 Diabetes Mellitus Patients: A Cross-sectional Study. Contemp Clin. Dent. 2019, 10, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Chikte, U.; Pontes, C.C.; Karangwa, I.; Dhansay, K.F.; Erasmus, R.T.; Kengne, A.P.; Matsha, T.E. Periodontal Disease Status among Adults from South Africa-Prevalence and Effect of Smoking. Int. J. Environ. Res. Public Health 2019, 16, 3662. [Google Scholar] [CrossRef] [Green Version]
- Nesse, W.; Abbas, F.; Ploeg, I.; Spijkervet, F.K.L.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area: Quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Susanto, H.; Nesse, W.; Dijkstra, P.U.; Hoedemaker, E.; van Reenen, Y.H.; Agustina, D.; Vissink, A.; Abbas, F. Periodontal inflamed surface area and C-reactive protein as predictors of HbA1c: A study in Indonesia. Clin. Oral Investig. 2012, 16, 1237–1242. [Google Scholar] [CrossRef] [Green Version]
- Orlandi, M.; Graziani, F.; D’Aiuto, F. Periodontal therapy and cardiovascular risk. Periodontol. 2000 2020, 83, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Suvan, J.; Deschner, J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontol. 2000 2020, 83, 125–153. [Google Scholar] [CrossRef]
- Genco, R.J.; Sanz, M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontol. 2000 2020, 83, 7–13. [Google Scholar] [CrossRef]
- Sanz, M.; Castillo, M.D.A.; Jepsen, S.; Juanatey, G.J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Blaschke, K.; Seitz, M.W.; Schubert, I.; Listl., S. Methodological approaches for investigating links between dental and chronic diseases with claims data: A scoping study. J. Public Health Dent. 2019, 79, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 45, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.J.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriya, S. Global burden of oral diseases: Emerging concepts, management and interplay with systemic health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef]
- Nomura, Y.; Morozumi, T.; Nakagawa, T.; Sugaya, T.; Kawanami, M.; Suzuki, F.; Takahashi, K.; Abe, Y.; Sato, S.; Makino-Oi, A.; et al. Site-level progression of periodontal disease during a follow-up period. PLoS ONE 2017, 12, e0188670. [Google Scholar] [CrossRef] [PubMed]
- Morozumi, T.; Nakagawa, T.; Nomura, Y.; Sugaya, T.; Kawanami, M.; Suzuki, F.; Takahashi, K.; Abe, Y.; Sato, S.; Makino-Oi, A.; et al. Salivary pathogen and serum antibody to assess the progression of chronic periodontitis: A 24-mo prospective multicenter cohort study. J. Periodontal Res. 2016, 51, 768–778. [Google Scholar] [CrossRef]
- Kakuta, E.; Nomura, Y.; Morozumi, T.; Nakagawa, T.; Nakamura, T.; Noguchi, K.; Yoshimura, A.; Hara, Y.; Fujise, O.; Nishimura, F.; et al. Assessing the progression of chronic periodontitis using subgingival pathogen levels: A 24-month prospective multicenter cohort study. BMC Oral Health 2017, 17, 46. [Google Scholar] [CrossRef] [Green Version]
- Krebs, K.A.; Clem, D.S., 3rd. American Academy of Periodontology, Guidelines for the management of patients with periodontal diseases. J. Periodontol. 2006, 77, 1607–1611. [Google Scholar] [CrossRef] [Green Version]
- Schöffer, C.; Oliveira, L.M.; Santi, S.S.; Antoniazzi, R.P.; Zanatta, F.B. C-reactive protein levels are associated with periodontitis and periodontal inflamed surface area in adults with end-stage renal disease. J. Periodontol. 2020. [Google Scholar] [CrossRef]
- Smojver, B.K.; Altabas, K.; Knotek, M.; Jukić, N.B.; Aurer, A. Periodontal inflamed surface area in patients on haemodialysis and peritoneal dialysis: A Croatian cross-sectional study. BMC Oral Health 2020, 20, 95. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, M.; Kobayashi, T.; Ito, S.; Kaneko, C.; Murasawa, A.; Ishikawa, H.; Tabeta, K. The periodontal inflamed surface area is associated with the clinical response to biological disease-modifying antirheumatic drugs in rheumatoid arthritis: A retrospective study. Mod. Rheumatol. 2020, 30, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Teke, E.; Kırzıoğlu, E.Y.; Korkmaz, H.; Calapoğlu, M.; Orhan, H. Does metabolic control affect salivary adipokines in type 2 diabetes mellitus? Dent. Med. Probl. 2019, 56, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, S.; Okanobu, A.; Hatano, S.; Kajiya, M.; Sasaki, S.; Hamamoto, Y.; Iwata, T.; Ouhara, K.; Takeda, K.; Mizuno, N.; et al. Relationship between periodontal inflammation and calcium channel blockers induced gingival overgrowth-a cross-sectional study in a Japanese population. Clin. Oral Investig. 2019, 23, 4099–4105. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Yáñez, M.R.; Arias, S.; Dequidt, I.L.; Campos, F.; Sobrino, T.; D’Aiuto, F.; Castillo, J.; Blanco, J. Periodontitis is associated with systemic inflammation and vascular endothelial dysfunction in patients with lacunar infarct. J. Periodontol. 2019, 90, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Yáñez, M.R.; Arias, S.; Dequidt, I.L.; Campos, F.; Sobrino, T.; D’Aiuto, F.; Castillo, J.; Blanco, J. Periodontitis as a risk indicator and predictor of poor outcome for lacunar infarct. J. Clin. Periodontol. 2019, 46, 20–30. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, M.; Kimura, Y.; Ogawa, H.; Yamaga, T.; Ansai, T.; Wada, W.; Sakamoto, R.; Ishimoto, Y.; Fujisawa, M.; Okumiya, K.; et al. Periodontitis, periodontal inflammation, and mild cognitive impairment: A 5-year cohort study. J. Periodontal Res. 2019, 54, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Temelli, B.; Ay, Z.Y.; Aksoy, F.; Büyükbayram, H.İ.; Doğuç, D.K.; Uskun, E.; Varol, E. Platelet indices (mean platelet volume and platelet distribution width) have correlations with periodontal inflamed surface area in coronary artery disease patients: A pilot study. J. Periodontol. 2018, 89, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Epping, L.; Miesbach, W.; Nickles, K.; Eickholz, P. Is gingival bleeding a symptom of type 2 and 3 von Willebrand disease? PLoS ONE 2018, 13, e0191291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punj, A.; Santhosh, B.; Shenoy, A.B.; Subramanyam, K. Comparison of endothelial function in healthy patients and patients with chronic periodontitis and myocardial infarction. J. Periodontol. 2017, 88, 1234–1243. [Google Scholar] [CrossRef]
- Yoshihara, A.; Sugita, N.; Iwasaki, M.; Wang, Y.; Miyazaki, H.; Yoshie, H.; Nakamura, K. Relationship between renal function and periodontal disease in community-dwelling elderly women with different genotypes. J. Clin. Periodontol. 2017, 44, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, A.; Iwasaki, M.; Miyazaki, H.; Nakamura, K. Bidirectional relationship between renal function and periodontal disease in older Japanese women. J. Clin. Periodontol. 2016, 43, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Khanuja, P.K.; Narula, S.C.; Rajput, R.; Sharma, R.K.; Tewar, I.S. Association of periodontal disease with glycemic control in patients with type 2 diabetes in Indian population. Front. Med. 2017, 11, 110–119. [Google Scholar] [CrossRef]
- Sato, M.; Iwasaki, M.; Yoshihara, A.; Miyazaki, M. Association between periodontitis and medical expenditure in older adults: A 33-month follow-up study. Geriatr. Gerontol. Int. 2016, 16, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Jaedicke, K.M.; Bissett, S.M.; Finch, T.; Thornton, J.; Preshaw, P.M. Exploring changes in oral hygiene behaviour in patients with diabetes and periodontal disease: A feasibility study. Int. J. Dent. Hyg. 2019, 17, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Weickert, L.; Miesbach, W.; Alesci, S.R.; Eickholz, P.; Nickles, K. Is gingival bleeding a symptom of patients with type 1 von Willebrand disease? A case-control study. J. Clin. Periodontol. 2014, 41, 766–771. [Google Scholar] [CrossRef]
- Iwasaki, M.; Taylor, G.W.; Nesse, W.; Vissink, A.; Yoshihara, A.; Miyazaki, H. Periodontal disease and decreased kidney function in Japanese elderly. Am. J. Kidney Dis. 2012, 59, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Nesse, W.; Linde, A.; Abbas, F.; Spijkervet, F.K.L.; Dijkstra, P.U.; Brabander, E.C.; Gerstenbluth, I.; Vissink, A. Dose-response relationship between periodontal inflamed surface area and HbA1c in type 2 diabetics. J. Clin. Periodontol. 2009, 36, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.; Gürbüz, N.; Özbalci, F.İ.; Koşkan, Ö.; Yetkin, A.Z. Increase in serum and salivary neutrophil gelatinase-associated lipocalin levels with increased periodontal inflammation. J. Appl. Oral Sci. 2020, 28, e20200276. [Google Scholar] [CrossRef]
- Kasai, S.; Onizuka, S.; Katagiri, S.; Nakamura, T.; Hanatani, T.; Kudo, T.; Sugata, Y.; Ishimatsu, M.; Usui, M.; Nakashima, K. Associations of cytokine levels in gingival crevicular fluid of mobile teeth with clinical improvement after initial periodontal treatment. J. Oral Sci 2020, 62, 189–196. [Google Scholar] [CrossRef] [Green Version]
- Leira, Y.; Ameijeira, P.; Domínguez, C.; Arias, E.L.; Gómez, Á.P.; Mato, M.P.; Sobrino, T.; Campos, F.; D’Aiuto, F.; Leira, R.; et al. Periodontal inflammation is related to increased serum calcitonin gene-related peptide levels in patients with chronic migraine. J. Periodontol. 2019, 90, 1088–1095. [Google Scholar] [CrossRef]
- Chaparro, A.; Zúñiga, E.; Godoy, M.V.; Albers, D.; Ramírez, V.; Hernández, M.; Kusanovic, J.P.; Gallardo, S.A.; Rice, G.; Illanes, S.E. Periodontitis and placental growth factor in oral fluids are early pregnancy predictors of gestational diabetes mellitus. J. Periodontol. 2018, 89, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Lancharro, P.M.; Blanco, J. Periodontal inflamed surface area and periodontal case definition classification. Acta Odontol. Scand 2018, 76, 195–198. [Google Scholar] [CrossRef]
- Park, S.Y.; Ahn, S.; Lee, J.T.; Yun, P.Y.; Lee, Y.J.; Lee, J.Y.; Song, Y.W.; Chang, Y.S.; Lee, H.J. Periodontal inflamed surface area as a novel numerical variable describing periodontal conditions. J. Periodontal Implant. Sci. 2017, 47, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakanaka, A.; Kuboniwa, M.; Hashino, E.; Bamba, T.; Fukusaki, E.; Amano, A. Distinct signatures of dental plaque metabolic by products dictated by periodontal inflammatory status. Sci. Rep. 2017, 7, 42818. [Google Scholar] [CrossRef]
- Ramfjord, S.P. Indices for prevalence and incidence of periodontal disease. J. Periodontol. 1959, 30, 51–59. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bleeding on Probing | Maximum Value of Probing Depth | ||||||
|---|---|---|---|---|---|---|---|
| 1 Site | 2 Sites | 3 Sites | 3 Mm | 4 mm | 5 mm | ||
| Maxillary | 2nd Molar | 27.0 | 35.9 | 128.7 | 22.4 | 29.9 | 32.1 |
| 1st Molar | 25.4 | 23.3 | 35.9 | 24.0 | 35.9 | 43.8 | |
| 2nd Premolar | 30.7 | 32.3 | 47.0 | 35.1 | 41.0 | 47.8 | |
| 1st Premolar | 33.7 | 39.9 | 53.8 | 30.5 | 40.1 | 43.7 | |
| Canine | 28.5 | 35.1 | 48.0 | 32.2 | 43.5 | 429.5 | |
| Lateral incisor | 27.8 | 48.4 | 71.7 | 30.8 | 44.8 | 49.8 | |
| Central incisor | 30.7 | 32.1 | 42.4 | 28.7 | 38.5 | 41.4 | |
| Mandibular | 2nd Molar | 28.0 | 27.3 | 36.6 | 24.6 | 34.5 | 30.5 |
| 1st Molar | 27.8 | 27.6 | 39.1 | 15.0 | 37.7 | 47.6 | |
| 2nd Premolar | 26.7 | 27.2 | 32.8 | 32.3 | 34.6 | 31.7 | |
| 1st Premolar | 32.6 | 27.9 | 33.6 | 31.1 | 43.9 | 39.0 | |
| Canine | 24.8 | 30.3 | 35.1 | 35.3 | 47.7 | 51.6 | |
| Lateral incisor | 32.0 | 32.6 | 32.6 | 43.1 | 48.3 | 41.3 | |
| Central incisor | 36.8 | 32.7 | 34.8 | 42.8 | 46.2 | 35.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, Y.; Morozumi, T.; Numabe, Y.; Ogata, Y.; Nakayama, Y.; Sugaya, T.; Nakamura, T.; Sato, S.; Takashiba, S.; Sekino, S.; et al. Estimation of the Periodontal Inflamed Surface Area by Simple Oral Examination. J. Clin. Med. 2021, 10, 723. https://doi.org/10.3390/jcm10040723
Nomura Y, Morozumi T, Numabe Y, Ogata Y, Nakayama Y, Sugaya T, Nakamura T, Sato S, Takashiba S, Sekino S, et al. Estimation of the Periodontal Inflamed Surface Area by Simple Oral Examination. Journal of Clinical Medicine. 2021; 10(4):723. https://doi.org/10.3390/jcm10040723
Chicago/Turabian StyleNomura, Yoshiaki, Toshiya Morozumi, Yukihiro Numabe, Yorimasa Ogata, Yohei Nakayama, Tsutomu Sugaya, Toshiaki Nakamura, Soh Sato, Shogo Takashiba, Satoshi Sekino, and et al. 2021. "Estimation of the Periodontal Inflamed Surface Area by Simple Oral Examination" Journal of Clinical Medicine 10, no. 4: 723. https://doi.org/10.3390/jcm10040723