
Urinary Titin N-Fragment as a Biomarker of Muscle Atrophy, Intensive Care Unit-Acquired Weakness, and Possible Application for Post-Intensive Care Syndrome

 ,
,  , , and
, , and
Abstract
:1. Introduction
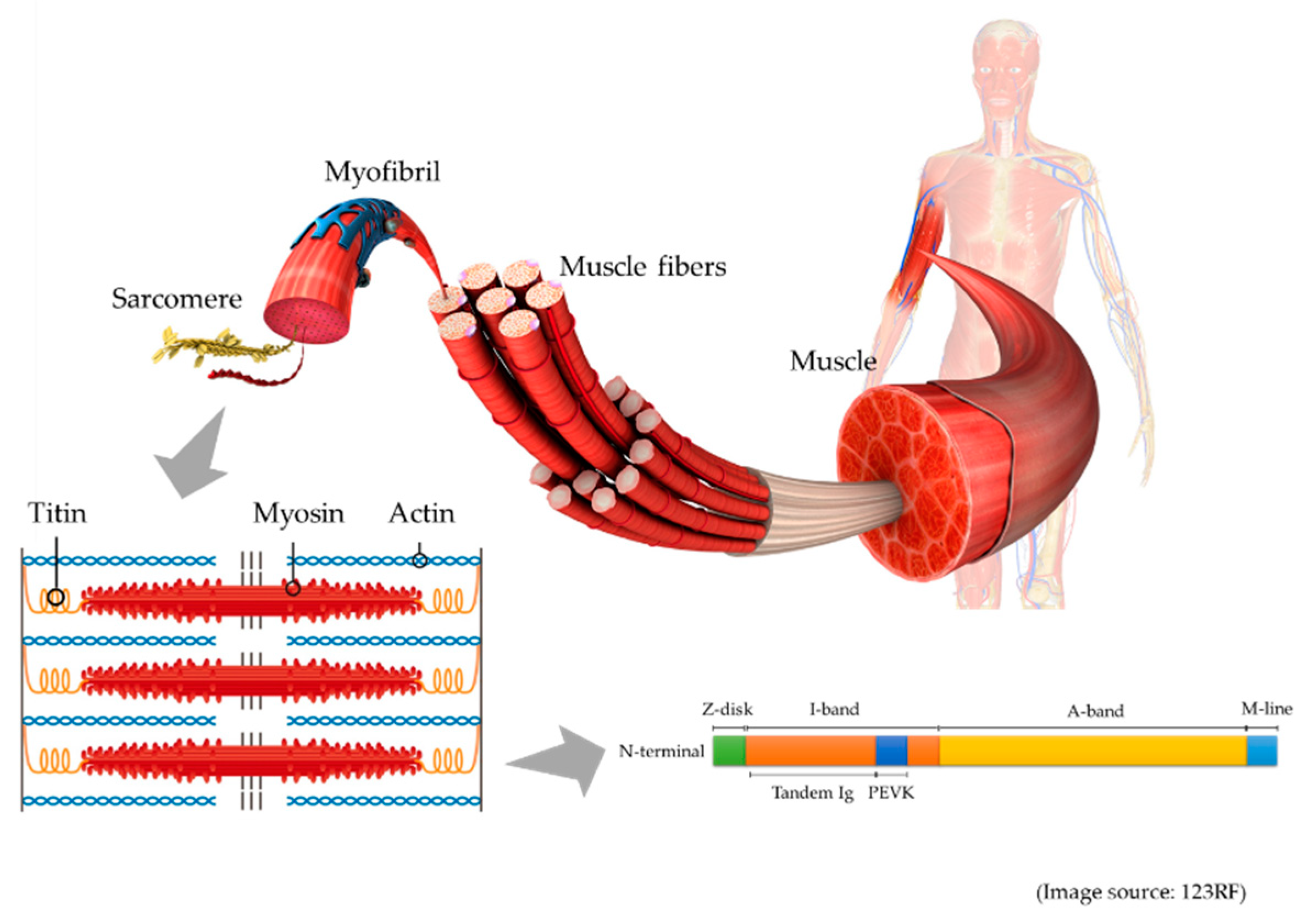
2. Titin
3. Muscle Atrophy
3.1. Limb and Trunk Muscle Atrophy
3.2. Diaphragm Muscle Atrophy
3.3. Other Respiratory Muscle Atrophy
4. ICU-Acquired Weakness
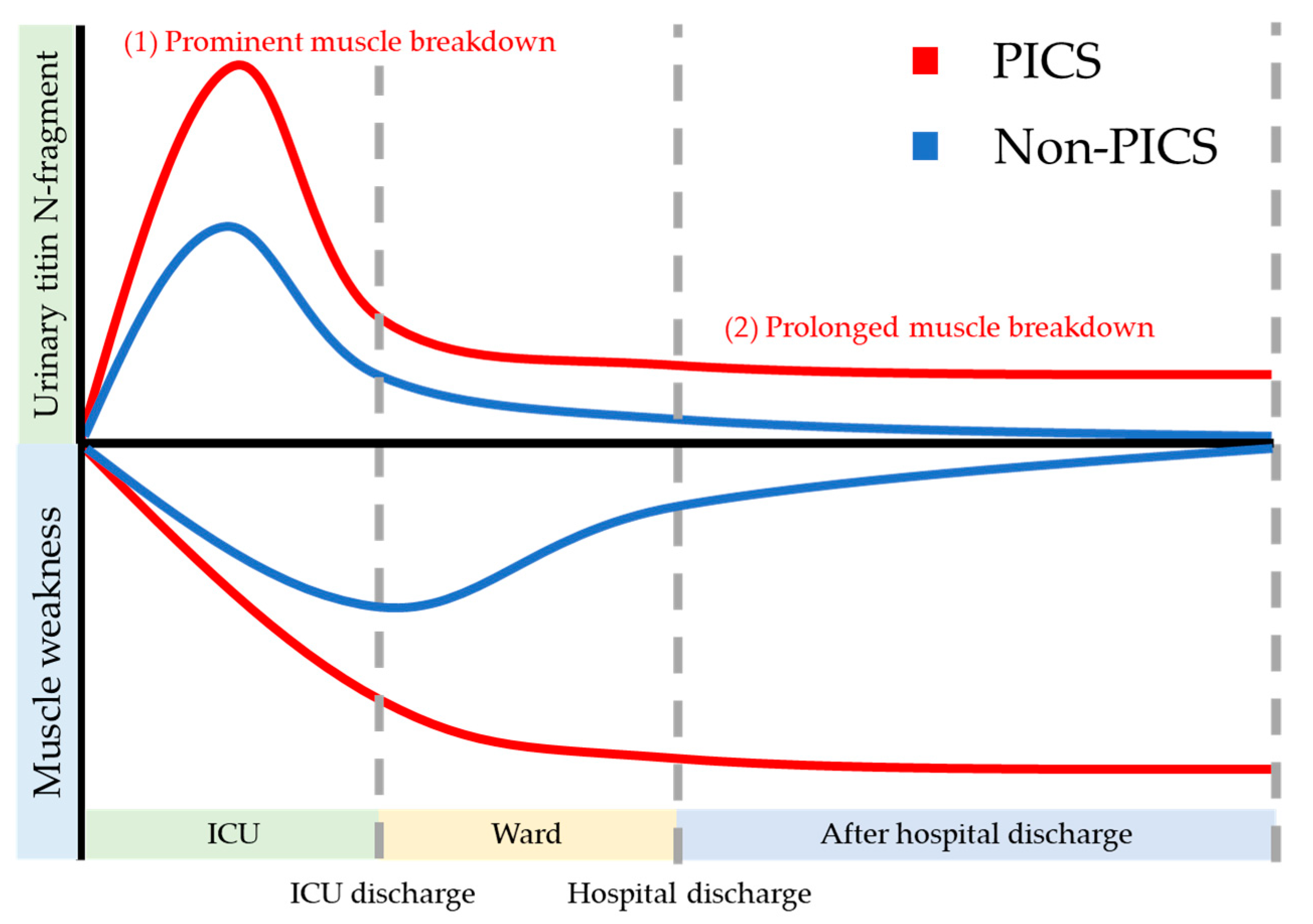
5. PICS
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Linke, W.A. Titin Gene and Protein Functions in Passive and Active Muscle. Annu. Rev. Physiol. 2018, 80, 389–411. [Google Scholar] [CrossRef]
- Maruyama, N.; Asai, T.; Abe, C.; Inada, A.; Kawauchi, T.; Miyashita, K.; Maeda, M.; Matsuo, M.; Nabeshima, Y.-I. Establishment of a highly sensitive sandwich ELISA for the N-terminal fragment of titin in urine. Sci. Rep. 2016, 6, 39375. [Google Scholar] [CrossRef]
- Awano, H.; Matsumoto, M.; Nagai, M.; Shirakawa, T.; Maruyama, N.; Iijima, K.; Nabeshima, Y.-I.; Matsuo, M. Diagnostic and clinical significance of the titin fragment in urine of Duchenne muscular dystrophy patients. Clin. Chim. Acta 2018, 476, 111–116. [Google Scholar] [CrossRef]
- Nakanishi, N.; Takashima, T.; Oto, J. Muscle atrophy in critically ill patients: A review of its cause, evaluation, and prevention. J. Med. Investig. 2020, 67, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Padhke, R.; Dew, T.; Sidhu, P.S.; et al. Acute Skeletal Muscle Wasting in Critical Illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parry, S.M.; El-Ansary, D.; Cartwright, M.S.; Sarwal, A.; Berney, S.; Koopman, R.; Annoni, R.; Puthucheary, Z.; Gordon, I.R.; Morris, P.E.; et al. Ultrasonography in the intensive care setting can be used to detect changes in the quality and quantity of muscle and is related to muscle strength and function. J. Crit. Care 2015, 30, e9–e14. [Google Scholar] [CrossRef] [PubMed]
- Kress, J.P.; Hall, J.B. ICU-Acquired Weakness and Recovery from Critical Illness. N. Engl. J. Med. 2014, 370, 1626–1635. [Google Scholar] [CrossRef] [Green Version]
- Swist, S.; Unger, A.; Li, Y.; Vöge, A.; Von Frieling-Salewsky, M.; Skärlén, Å.; Cacciani, N.; Braun, T.; Larsson, L.; Linke, W.A. Maintenance of sarcomeric integrity in adult muscle cells crucially depends on Z-disc anchored titin. Nat. Commun. 2020, 11, 1–18. [Google Scholar] [CrossRef]
- Nakanishi, N.; Tsutsumi, R.; Hara, K.; Takashima, T.; Nakataki, E.; Itagaki, T.; Matsuo, M.; Oto, J.; Sakaue, H. Urinary Titin Is a Novel Biomarker for Muscle Atrophy in Nonsurgical Critically Ill Patients: A two-center, prospective observational study. Crit. Care Med. 2020, 48, 1327–1333. [Google Scholar] [CrossRef]
- Nakano, H.; Hashimoto, H.; Mochizuki, M.; Naraba, H.; Takahashi, Y.; Sonoo, T.; Matsubara, T.; Yamakawa, K.; Nakamura, K. Urine Titin N-fragment as a Biomarker of Muscle Injury for Critical Illness Myopathy. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef]
- Nakano, H.; Matsubara, T.; Yamakawa, K.; Nakamura, K. Urine TITIN N-fragment as a novel biomarker for critical illness myopathy: A pilot study. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef]
- Inoue, S.; Hatakeyama, J.; Kondo, Y.; Hifumi, T.; Sakuramoto, H.; Kawasaki, T.; Taito, S.; Nakamura, K.; Unoki, T.; Kawai, Y.; et al. Post-intensive care syndrome: Its pathophysiology, prevention, and future directions. Acute Med. Surg. 2019, 6, 233–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional Disability 5 Years after Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, K.; Natori, R.; Nonomura, Y. New elastic protein from muscle. Nat. Cell Biol. 1976, 262, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Maciejewska-Skrendo, A.; Leźnicka, K.; Leońska-Duniec, A.; Wilk, M.; Filip, A.; Cięszczyk, P.; Sawczuk, M. Genetics of Muscle Stiffness, Muscle Elasticity and Explosive Strength. J. Hum. Kinet. 2020, 74, 143–159. [Google Scholar]
- Sun, S.; Henriksen, K.; Karsdal, M.A.; Armbrecht, G.; Belavy, D.L.; Felsenberg, D.; Rittweger, J.; Wang, Y.; Zheng, Q.; Nedergaard, A. Measurement of a MMP-2 degraded Titin fragment in serum reflects changes in muscle turnover induced by atrophy. Exp. Gerontol. 2014, 58, 83–89. [Google Scholar] [CrossRef]
- Vassiliadis, E.; Rasmussen, L.M.; Byrjalsen, I.; Larsen, D.V.; Chaturvedi, R.; Hosbond, S.; Saabye, L.; Diederichsen, A.; Genovese, F.; Duffin, K.L.; et al. Clinical evaluation of a matrix metalloproteinase-12 cleaved fragment of titin as a cardiovascular serological biomarker. J. Transl. Med. 2012, 10, 140. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, N.; Oto, J.; Tsutsumi, R.; Iuchi, M.; Onodera, M.; Nishimura, M. Upper and lower limb muscle atrophy in critically ill patients: An observational ultrasonography study. Intensiv. Care Med. 2018, 44, 263–264. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, N.; Oto, J.; Tsutsumi, R.; Akimoto, Y.; Nakano, Y.; Nishimura, M. Upper limb muscle atrophy associated with in-hospital mortality and physical function impairments in mechanically ventilated critically ill adults: A two-center prospective observational study. J. Intensiv. Care 2020, 8, 1–9. [Google Scholar] [CrossRef]
- Lee, Z.-Y.; Ong, S.P.; Ng, C.C.; Yap, C.S.L.; Engkasan, J.P.; Barakatun-Nisak, M.Y.; Heyland, D.K.; Hasan, M.S. Association between ultrasound quadriceps muscle status with premorbid functional status and 60-day mortality in mechanically ventilated critically ill patient: A single-center prospective observational study. Clin. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Doyle, A.; Zhang, G.; Fattah, E.A.A.; Eissa, N.T.; Li, Y.-P. Toll-like receptor 4 mediates lipopolysaccharide-induced muscle catabolism via coordinate activation of ubiquitin-proteasome and autophagy-lysosome pathways. FASEB J. 2010, 25, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Schiaffino, S.; Hanzlíkovávěra, V. Studies on the effect of denervation in developing muscle. II. The lysosomal system. J. Ultrastruct. Res. 1972, 39, 1–14. [Google Scholar] [CrossRef]
- Talbert, E.E.; Smuder, A.J.; Min, K.; Kwon, O.S.; Powers, S.K. Calpain and caspase-3 play required roles in immobilization-induced limb muscle atrophy. J. Appl. Physiol. 2013, 114, 1482–1489. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Nathan, J.A.; Goldberg, A.L. Muscle wasting in disease: Molecular mechanisms and promising therapies. Nat. Rev. Drug Discov. 2015, 14, 58–74. [Google Scholar] [CrossRef] [PubMed]
- Langhans, C.; Weber-Carstens, S.; Schmidt, F.; Hamati, J.; Kny, M.; Zhu, X.; Wollersheim, T.; Koch, S.; Krebs, M.; Schulz, H.; et al. Inflammation-Induced Acute Phase Response in Skeletal Muscle and Critical Illness Myopathy. PLoS ONE 2014, 9, e92048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Files, D.C.; Sanchez, M.A.; Morris, P.E. A conceptual framework: The early and late phases of skeletal muscle dysfunction in the acute respiratory distress syndrome. Crit. Care 2015, 19, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibilla, A.; Nydahl, P.; Greco, N.; Mungo, G.; Ott, N.; Unger, I.; Rezek, S.; Gemperle, S.; Needham, D.M.; Kudchadkar, S.R. Mobilization of Mechanically Ventilated Patients in Switzerland. J. Intensiv. Care Med. 2020, 35, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Wykes, L.J.; Fiorotto, M.; Burrin, D.; Del Rosario, M.; Frazer, M.E.; Pond, W.G.; Jahoor, F. Chronic Low Protein Intake Reduces Tissue Protein Synthesis in a Pig Model of Protein Malnutrition. J. Nutr. 1996, 126, 1481–1488. [Google Scholar] [CrossRef] [Green Version]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [Green Version]
- Yatabe, T.; Egi, M.; Sakaguchi, M.; Ito, T.; Inagaki, N.; Kato, H.; Kaminohara, J.; Konishi, A.; Takahashi, M.; Tatsumi, H.; et al. Influence of Nutritional Management and Rehabilitation on Physical Outcome in Japanese Intensive Care Unit Patients: A Multicenter Observational Study. Ann. Nutr. Metab. 2019, 74, 35–43. [Google Scholar] [CrossRef]
- Looijaard, W.G.P.M.; Molinger, J.; Weijs, P.J. Measuring and monitoring lean body mass in critical illness. Curr. Opin. Crit. Care 2018, 24, 241–247. [Google Scholar] [CrossRef]
- Nakanishi, N.; Tsutsumi, R.; Okayama, Y.; Takashima, T.; Ueno, Y.; Itagaki, T.; Tsutsumi, Y.; Sakaue, H.; Oto, J. Monitoring of muscle mass in critically ill patients: Comparison of ultrasound and two bioelectrical impedance analysis devices. J. Intensiv. Care 2019, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Palakshappa, J.A.; Bakhru, R.N. Bedside Ultrasonography Can and Should Be Used in the Intensive Care Unit to Evaluate Muscle Atrophy. Ann. Am. Thorac. Soc. 2019, 16, 1107–1111. [Google Scholar] [CrossRef] [PubMed]
- Branea, O.-E.; Jugariu, A.R.; Budeanu, R.-G.; Copotoiu, S.M.; Copotoiu, M. Ultrasonography: New Insights in its Applicability to Explore Muscle Mass and Musculoskeletal Inflammation in Critically ill Patients. Acta Med. Marisiensis 2018, 64, 147–150. [Google Scholar] [CrossRef] [Green Version]
- Udaka, J.; Ohmori, S.; Terui, T.; Ohtsuki, I.; Ishiwata, S.; Kurihara, S.; Fukuda, N. Disuse-induced Preferential Loss of the Giant Protein Titin Depresses Muscle Performance via Abnormal Sarcomeric Organization. J. Gen. Physiol. 2007, 131, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouillon, J.; Zocevic, A.; Léger, T.; Garcia, C.; Camadro, J.-M.; Udd, B.; Wong, B.; Servais, L.; Voit, T.; Svinartchouk, F. Proteomics profiling of urine reveals specific titin fragments as biomarkers of Duchenne muscular dystrophy. Neuromuscul. Disord. 2014, 24, 563–573. [Google Scholar] [CrossRef]
- Raynaud, F.; Fernandez, É.; Coulis, G.; Aubry, L.; Vignon, X.; Bleimling, N.; Gautel, M.; Benyamin, Y.; Ouali, A. Calpain 1-titin interactions concentrate calpain 1 in the Z-band edges and in the N2-line region within the skeletal myofibril. FEBS J. 2005, 272, 2578–2590. [Google Scholar] [CrossRef]
- Lang, F.; Aravamudhan, S.; Nolte, H.; Türk, C.; Hölper, S.; Müller, S.; Günther, S.; Blaauw, B.; Braun, T.; Krüger, M. Dynamic changes in the mouse skeletal muscle proteome during denervation-induced atrophy. Dis. Model. Mech. 2017, 10, 881–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, R.W.; Zolfaghari, P.; Wan, Y.; Pearse, R.M.; Puthucheary, Z.; Prowle, J.R. Elevated urea-to-creatinine ratio provides a biochemical signature of muscle catabolism and persistent critical illness after major trauma. Intensiv. Care Med. 2019, 45, 1718–1731. [Google Scholar] [CrossRef] [PubMed]
- Moghadam-Kia, S.; Oddis, C.V.; Aggarwal, R. Approach to asymptomatic creatine kinase elevation. Clevel. Clin. J. Med. 2016, 83, 37–42. [Google Scholar] [CrossRef]
- Volbeda, M.; Hessels, L.; Posma, R.; Bakker, S.; Nijsten, M.W.N. Time courses of urinary creatinine excretion, measured creatinine clearance and estimated glomerular filtration rate over 30 days of ICU admission. J. Crit. Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, N.; Oto, J.; Ueno, Y.; Nakataki, E.; Itagaki, T.; Nishimura, M. Change in diaphragm and intercostal muscle thickness in mechanically ventilated patients: A prospective observational ultrasonography study. J. Intensiv. Care 2019, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Vorona, S.; Sklar, M.C.; Rittayamai, N.; Lanys, A.; et al. Mechanical Ventilation–induced Diaphragm Atrophy Strongly Impacts Clinical Outcomes. Am. J. Respir. Crit. Care Med. 2018, 197, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Smuder, A.J.; Sollanek, K.J.; Nelson, W.B.; Min, K.; Talbert, E.E.; Kavazis, A.N.; Hudson, M.B.; Sandri, M.; Szeto, H.H.; Powers, S.K. Crosstalk between autophagy and oxidative stress regulates proteolysis in the diaphragm during mechanical ventilation. Free Radic. Biol. Med. 2018, 115, 179–190. [Google Scholar] [CrossRef]
- McClung, J.M.; Kavazis, A.N.; DeRuisseau, K.C.; Falk, D.J.; Deering, M.A.; Lee, Y.; Sugiura, T.; Powers, S.K. Caspase-3 Regulation of Diaphragm Myonuclear Domain during Mechanical Ventilation–induced Atrophy. Am. J. Respir. Crit. Care Med. 2007, 175, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Van Hees, H.W.H.; Heunks, L.; Wang, F.; Shao, L.; Huang, J.; Shi, L.; Ma, S. The role of calpains in ventilator-induced diaphragm atrophy. Intensiv. Care Med. Exp. 2017, 5, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooijman, P.E.; Beishuizen, A.; Witt, C.C.; De Waard, M.C.; Girbes, A.R.J.; Man, A.M.E.S.-D.; Niessen, H.W.M.; Manders, E.; Van Hees, H.W.H.; Brom, C.E.V.D.; et al. Diaphragm Muscle Fiber Weakness and Ubiquitin–Proteasome Activation in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2015, 191, 1126–1138. [Google Scholar] [CrossRef]
- Hadda, V.; Kumar, R.; Tiwari, P.; Mittal, S.; Kalaivani, M.; Madan, K.; Mohan, A.; Guleria, R. Decline in diaphragm thickness and clinical outcomes among patients with sepsis. Hear. Lung 2021, 50, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Sklar, M.C.; Madotto, F.; Jonkman, A.; Rauseo, M.; Soliman, I.; Damiani, L.F.; Telias, I.; Dubo, S.; Chen, L.; Rittayamai, N.; et al. Duration of diaphragmatic inactivity after endotracheal intubation of critically ill patients. Crit. Care 2021, 25, 1–15. [Google Scholar] [CrossRef]
- Peñuelas, Ó.; Keough, E.; López-Rodríguez, L.; Carriedo, D.; Gonçalves, G.; Barreiro, E.; Lorente, J.Á. Ventilator-induced diaphragm dysfunction: Translational mechanisms lead to therapeutical alternatives in the critically ill. Intensiv. Care Med. Exp. 2019, 7, 1–25. [Google Scholar] [CrossRef]
- Van Der Pijl, R.J.; Granzier, H.L.; Ottenheijm, C. Diaphragm contractile weakness due to reduced mechanical loading: Role of titin. Am. J. Physiol. Cell Physiol. 2019, 317, C167–C176. [Google Scholar] [CrossRef]
- Van Hees, H.; Ottenheijm, C.; Granzier, H.; Dekhuijzen, P.; Heunks, L. Heart failure decreases passive tension generation of rat diaphragm fibers. Int. J. Cardiol. 2010, 141, 275–283. [Google Scholar] [CrossRef]
- Van Hees, H.W.H.; Schellekens, W.-J.M.; Acuña, G.L.A.; Linkels, M.; Hafmans, T.; Ottenheijm, C.A.C.; Granzier, H.L.; Scheffer, G.-J.; Van Der Hoeven, J.G.; Dekhuijzen, P.N.R.; et al. Titin and diaphragm dysfunction in mechanically ventilated rats. Intensiv. Care Med. 2012, 38, 702–709. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.N.A.; Cornachione, A.S.; Guichon, C.; Al Khunaizi, A.; Leite, F.D.S.; Petrof, B.J.; Mofarrahi, M.; Moroz, N.; De Varennes, B.; Goldberg, P.; et al. Prolonged controlled mechanical ventilation in humans triggers myofibrillar contractile dysfunction and myofilament protein loss in the diaphragm. Thorax 2016, 71, 436–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindqvist, J.; Berg, M.V.D.; Van Der Pijl, R.; Hooijman, P.E.; Beishuizen, A.; Elshof, J.; De Waard, M.; Girbes, A.; Man, A.S.-D.; Shi, Z.-H.; et al. Positive End-Expiratory Pressure Ventilation Induces Longitudinal Atrophy in Diaphragm Fibers. Am. J. Respir. Crit. Care Med. 2018, 198, 472–485. [Google Scholar] [CrossRef] [PubMed]
- Bogomolovas, J.; Gasch, A.; Bajoras, V.; Karčiauskaitė, D.; Šerpytis, P.; Grabauskiene, V.; Labeit, D.; Labeit, S. Cardiac specific titin N2B exon is a novel sensitive serological marker for cardiac injury. Int. J. Cardiol. 2016, 212, 232–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goligher, E.C.; Fan, E.; Herridge, M.S.; Murray, A.; Vorona, S.; Brace, D.; Rittayamai, N.; Lanys, A.; Tomlinson, G.; Singh, J.M.; et al. Evolution of Diaphragm Thickness during Mechanical Ventilation. Impact of Inspiratory Effort. Am. J. Respir. Crit. Care Med. 2015, 192, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Filyk, O. Prevention of respiratory muscle dysfunction due to diaphragm atrophy in children with respiratory failure. Eureka Health Sci. 2020, 6, 40–45. [Google Scholar] [CrossRef]
- O’Rourke, J.; Soták, M.; Curley, G.F.; Doolan, A.; Henlín, T.; Mullins, G.; Tyll, T.; Omlie, W.; Ranieri, M.V. Initial Assessment of the Percutaneous Electrical Phrenic Nerve Stimulation System in Patients on Mechanical Ventilation. Crit. Care Med. 2020, 48, e362–e370. [Google Scholar] [CrossRef]
- Spinelli, E.; Carlesso, E.; Mauri, T. Extracorporeal support to achieve lung-protective and diaphragm-protective ventilation. Curr. Opin. Crit. Care 2020, 26, 66–72. [Google Scholar] [CrossRef]
- Nakanishi, N.; Okamoto, Y.; Okahisa, T.; Oto, J. Early Initiation of Awake Veno-Venous Extracorporeal Membrane Oxygenation Can Attenuate Muscle Atrophy and Weakness in Acute Respiratory Distress Syndrome. Cureus 2020, 12, e9926. [Google Scholar] [CrossRef] [PubMed]
- Formenti, P.; Umbrello, M.; Dres, M.; Chiumello, D. Ultrasonographic assessment of parasternal intercostal muscles during mechanical ventilation. Ann. Intensiv. Care 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ijland, M.M.; Lemson, J.; Van Der Hoeven, H.G.; Heunks, L. The impact of critical illness on the expiratory muscles and the diaphragm assessed by ultrasound in mechanical ventilated children. Ann. Intensiv. Care 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lopate, G.; Pestronk, A.; Yee, W.-C. N lines in a myopathy with myosin loss. Muscle Nerve 1998, 21, 1216–1219. [Google Scholar] [CrossRef]
- Jonkman, A.H.; Frenzel, T.; McCaughey, E.J.; McLachlan, A.J.; Boswell-Ruys, C.L.; Collins, D.W.; Gandevia, S.C.; Girbes, A.R.J.; Hoiting, O.; Kox, M.; et al. Breath-synchronized electrical stimulation of the expiratory muscles in mechanically ventilated patients: A randomized controlled feasibility study and pooled analysis. Crit. Care 2020, 24, 1–11. [Google Scholar] [CrossRef]
- Wieske, L.; Dettling-Ihnenfeldt, D.S.; Verhamme, C.; Nollet, F.; Van Schaik, I.N.; Schultz, M.J.; Horn, J.; Van Der Schaaf, M. Impact of ICU-acquired weakness on post-ICU physical functioning: A follow-up study. Crit. Care 2015, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Stevens, R.D.; Marshall, S.A.; Cornblath, D.R.; Hoke, A.; Needham, D.M.; De Jonghe, B.; Ali, N.A.; Sharshar, T. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit. Care Med. 2009, 37, S299–S308. [Google Scholar] [CrossRef]
- Van Aerde, N.; Meersseman, P.; Debaveye, Y.; Wilmer, A.; Gunst, J.; Casaer, M.P.; Bruyninckx, F.; Wouters, P.J.; Gosselink, R.; Berghe, G.V.D.; et al. Five-year impact of ICU-acquired neuromuscular complications: A prospective, observational study. Intensiv. Care Med. 2020, 46, 1184–1193. [Google Scholar] [CrossRef]
- Wieske, L.; Witteveen, E.; Petzold, A.; Verhamme, C.; Schultz, M.J.; Van Schaik, I.N.; Horn, J. Neurofilaments as a plasma biomarker for ICU-acquired weakness: An observational pilot study. Crit. Care 2014, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, O.; Diermeier, S.; Larsson, L. Weak by the machines: Muscle motor protein dysfunction—A side effect of intensive care unit treatment. Acta Physiol. 2018, 222, e12885. [Google Scholar] [CrossRef] [PubMed]
- Larsson, L.; Li, X.; Edström, L.; Eriksson, L.I.; Zackrisson, H.; Argentini, C.; Schiaffino, S. Acute quadriplegia and loss of muscle myosin in patients treated with nondepolarizing neuromuscular blocking agents and corticosteroids: Mechanisms at the cellular and molecular levels. Crit. Care Med. 2000, 28, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-P.; Sheu, J.-R.; Lin, A.C.-M.; Hsiao, G.; Fong, T.-H. Decline in titin content in rat skeletal muscle after denervation. Muscle Nerve 2005, 32, 798–807. [Google Scholar] [CrossRef]
- Ishihara, M.; Nakanishi, N.; Tsutsumi, R.; Hara, K.; Machida, K.; Yamamoto, N.; Kanematsu, Y.; Sakaue, H.; Oto, J.; Takagi, Y. Elevated Urinary Titin and its Associated Clinical Outcomes after Acute Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105561. [Google Scholar] [CrossRef] [PubMed]
- De Jonghe, B.; Sharshar, T.; Lefaucheur, J.-P.; Authier, F.-J.; Durand-Zaleski, I.; Boussarsar, M.; Cerf, C.; Renaud, E.; Mesrati, F.; Carlet, J.; et al. Paresis Acquired in the Intensive Care Unit—A Prospective Multicenter Study. JAMA 2002, 288, 2859–2867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Hu, W.; Cai, Z.; Liu, J.; Wu, J.; Deng, Y.; Yu, K.; Chen, X.; Zhu, L.; Ma, J.; et al. Early mobilization of critically ill patients in the intensive care unit: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0223185. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.; Li, Z.; Jiang, L.; Xi, X. Corticosteroid use and intensive care unit-acquired weakness: A systematic review and meta-analysis. Crit. Care 2018, 22, 187. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, K.S.; Patel, B.K.; MacKenzie, E.L.; Giovanni, S.P.; Pohlman, A.S.; Churpek, M.M.; Hall, J.B.; Kress, J.P. Impact of Vasoactive Medications on ICU-Acquired Weakness in Mechanically Ventilated Patients. Chest 2018, 154, 781–787. [Google Scholar] [CrossRef]
- Chan, K.S.; Mourtzakis, M.; Friedman, L.A.; Dinglas, V.D.; Hough, C.L.; Ely, E.W.; Morris, P.E.; Hopkins, R.O.; Needham, D.M. Evaluating Muscle Mass in Survivors of acute respiratory distress syndrome: A 1-year multi-center longitudinal study. Crit. Care Med. 2018, 46, 1238–1246. [Google Scholar] [CrossRef]
- Meyer-Frießem, C.H.; Malewicz, N.M.; Rath, S.; Ebel, M.; Kaisler, M.; Tegenthoff, M.; Schildhauer, T.A.; Pogatzki-Zahn, E.M.; Maier, C.; Zahn, P.K. Incidence, Time Course and Influence on Quality of Life of Intensive Care Unit-Acquired Weakness Symptoms in Long-Term Intensive Care Survivors. J. Intensiv. Care Med. 2020. [Google Scholar] [CrossRef]
- Kamdar, B.B.; Sepulveda, K.A.; Chong, A.; Lord, R.K.; Dinglas, V.D.; Mendez-Tellez, P.A.; Shanholtz, C.; Colantuoni, E.; Von Wachter, T.M.; Pronovost, P.J.; et al. Return to work and lost earnings after acute respiratory distress syndrome: A 5-year prospective, longitudinal study of long-term survivors. Thorax 2018, 73, 125–133. [Google Scholar] [CrossRef]
- Bektas, A.; Schurman, S.H.; Franceschi, C.; Ferrucci, L. A public health perspective of aging: Do hyper-inflammatory syndromes such as COVID-19, SARS, ARDS, cytokine storm syndrome, and post-ICU syndrome accelerate short- and long-term inflammaging? Immun. Ageing 2020, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sacanella, E.; Pérez-Castejón, J.M.; Nicolas, J.M.; Masanés, F.; Navarro, M.; Castro, P.; Soto, A.L. Functional status and quality of life 12 months after discharge from a medical ICU in healthy elderly patients: A prospective observational study. Crit. Care 2011, 15, R105. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Wang, Z.; Sun, R.; Wang, X.; Gu, S.; Zhang, X.; Huang, H.-B. Timely rehabilitation for critical patients with COVID-19: Another issue should not be ignored. Crit. Care 2020, 24, 273. [Google Scholar] [CrossRef]
- Van Aerde, N.; Berghe, G.V.D.; Wilmer, A.; Gosselink, R.; Hermans, G. Intensive care unit acquired muscle weakness in COVID-19 patients. Intensiv. Care Med. 2020, 46, 2083–2085. [Google Scholar] [CrossRef] [PubMed]
- Stam, H.; Stucki, G.; Bickenbach, J. Covid-19 and Post Intensive Care Syndrome: A Call for Action. J. Rehabil. Med. 2020, 52, jrm00044. [Google Scholar] [CrossRef]
- Hickmann, C.E.; Castanares-Zapatero, D.; Deldicque, L.; Bergh, P.V.D.; Caty, G.; Robert, A.; Roeseler, J.; Francaux, M.; Laterre, P.-F. Impact of Very Early Physical Therapy During Septic Shock on Skeletal Muscle: A randomized controlled trial. Crit. Care Med. 2018, 46, 1436–1443. [Google Scholar] [CrossRef]
- Schujmann, D.S.; Gomes, T.T.; Lunardi, A.C.; Lamano, M.Z.; Fragoso, A.; Pimentel, M.; Peso, C.N.; Araujo, P.; Fu, C. Impact of a Progressive Mobility Program on the Functional Status, Respiratory, and Muscular Systems of ICU Patients: A randomized and controlled trial. Crit. Care Med. 2020, 48, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, N.; Oto, J.; Tsutsumi, R.; Yamamoto, T.; Ueno, Y.; Nakataki, E.; Itagaki, T.; Sakaue, H.; Nishimura, M. Effect of Electrical Muscle Stimulation on Upper and Lower Limb Muscles in Critically Ill Patients: A two-center randomized controlled trial. Crit. Care Med. 2020, 48, e997–e1003. [Google Scholar] [CrossRef]
- Nakamura, K.; Nakano, H.; Naraba, H.; Mochizuki, M.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Morimura, N. High protein versus medium protein delivery under equal total energy delivery in critical care: A randomized controlled trial. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Nakamura, K.; Ogura, K.; Nakano, H.; Naraba, H.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Morimura, N. C-reactive protein clustering to clarify persistent inflammation, immunosuppression and catabolism syndrome. Intensiv. Care Med. 2020, 46, 437–443. [Google Scholar] [CrossRef]
- Nakamura, K.; Ogura, K.; Nakano, H.; Naraba, H.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Goto, T. Disseminated Intravascular Coagulopathy Is Associated with the Outcome of Persistent Inflammation, Immunosuppression and Catabolism Syndrome. J. Clin. Med. 2020, 9, 2662. [Google Scholar] [CrossRef] [PubMed]
- Rugg, C.; Ströhle, M.; Treml, B.; Bachler, M.; Schmid, S.; Kreutziger, J. ICU-Acquired Hypernatremia Is Associated with Persistent Inflammation, Immunosuppression and Catabolism Syndrome. J. Clin. Med. 2020, 9, 3017. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.M.; Kempen, L.J.A.P.; Hardy, R.S.; Langen, R.C.J. Inflammation and Skeletal Muscle Wasting During Cachexia. Front. Physiol. 2020, 11, 597675. [Google Scholar] [CrossRef] [PubMed]
- Puthucheary, Z.A.; Gensichen, J.S.; Cakiroglu, A.S.; Cashmore, R.; Edbrooke, L.; Heintze, C.; Neumann, K.; Wollersheim, T.; Denehy, L.; Schmidt, K.F.R. Implications for post critical illness trial design: Sub-phenotyping trajectories of functional recovery among sepsis survivors. Crit. Care 2020, 24, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Fuke, R.; Hifumi, T.; Kondo, Y.; Hatakeyama, J.; Takei, T.; Yamakawa, K.; Inoue, S.; Nishida, O. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: A systematic review and meta-analysis. BMJ Open 2018, 8, e019998. [Google Scholar] [CrossRef] [Green Version]
- Snell, K.P.; Beiter, C.L.; Hall, E.L.; Junod, A.S.; Wilson, B.J.; Lepone, D.K.; McIntyre, J.R.; Swartz, D.P.; Berger, A.L.; Kirchner, H.L.; et al. A Novel Approach to ICU Survivor Care: A Population Health Quality Improvement Project. Crit. Care Med. 2020, 48, e1164–e1170. [Google Scholar] [CrossRef]
- Haines, K.J.; McPeake, J.; Hibbert, E.; Boehm, L.M.; Aparanji, K.; Bakhru, R.N.; Bastin, A.J.; Beesley, S.J.; Beveridge, L.; Butcher, B.W.; et al. Enablers and Barriers to Implementing ICU Follow-Up Clinics and Peer Support Groups Following Critical Illness: The thrive collaboratives. Crit. Care Med. 2019, 47, 1194–1200. [Google Scholar] [CrossRef]
- Mikkelsen, M.E.; Still, M.; Anderson, B.J.; Bienvenu, O.J.; Brodsky, M.B.; Brummel, N.; Butcher, B.; Clay, A.S.; Felt, H.; Ferrante, L.E.; et al. Society of Critical Care Medicine’s International Consensus Conference on Prediction and Identification of Long-Term Impairments After Critical Illness. Crit. Care Med. 2020, 48, 1670–1679. [Google Scholar] [CrossRef]
- Oshida, N.; Shida, T.; Oh, S.; Kim, T.; Isobe, T.; Okamoto, Y.; Kamimaki, T.; Okada, K.; Suzuki, H.; Ariizumi, S.-I.; et al. Urinary Levels of Titin-N Fragment, a Skeletal Muscle Damage Marker, are Increased in Subjects with Nonalcoholic Fatty Liver Disease. Sci. Rep. 2019, 9, 19498. [Google Scholar] [CrossRef]
- Pillen, S.; Tak, R.O.; Zwarts, M.J.; Lammens, M.M.; Verrijp, K.N.; Arts, I.M.; Van Der Laak, J.A.; Hoogerbrugge, P.M.; Van Engelen, B.G.; Verrips, A. Skeletal Muscle Ultrasound: Correlation Between Fibrous Tissue and Echo Intensity. Ultrasound Med. Biol. 2009, 35, 443–446. [Google Scholar] [CrossRef]
- Miyoshi, K.; Shimoda, M.; Udo, R.; Oshiro, Y.; Suzuki, S. Urinary titin N-terminal fragment concentration is an indicator of preoperative sarcopenia and nutritional status in patients with gastrointestinal tract and hepatobiliary pancreatic malignancies. Nutrition 2020, 79, 110957. [Google Scholar] [CrossRef]
- Matsuo, M.; Awano, H.; Maruyama, N.; Nishio, H. Titin fragment in urine: A noninvasive biomarker of muscle degradation. Adv. Clin. Chem. 2019, 90, 1–23. [Google Scholar]
- Tanihata, J.; Nishioka, N.; Inoue, T.; Bando, K.; Minamisawa, S. Urinary Titin Is Increased in Patients After Cardiac Surgery. Front. Cardiovasc. Med. 2019, 6, 7. [Google Scholar] [CrossRef]
- Kim, K.W.; Cho, H.-J.; Khaliq, S.A.; Son, K.H.; Yoon, M.-S. Comparative Analyses of mTOR/Akt and Muscle Atrophy-Related Signaling in Aged Respiratory and Gastrocnemius Muscles. Int. J. Mol. Sci. 2020, 21, 2862. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Goral, K.; Flis, D.; Skrobot, W.; Cieminski, K.; Olek, R.; Akimoto, T.; Ziolkowski, W. Changes in Urinary Titin Fragment in Response to Different Types of Dynamic Eccentric Exercises. J. Sport Med. 2020. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Suzuki, K.; Kanda, K.; Inami, T.; Okada, J. Changes in urinary titin N-terminal fragments as a biomarker of exercise-induced muscle damage in the repeated bout effect. J. Sci. Med. Sport 2020, 23, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Suzuki, K.; Inami, T.; Kanda, K.; Hanye, Z.; Okada, J. Changes in urinary titin N-terminal fragment concentration after concentric and eccentric exercise. J. Sports Sci. Med. 2020, 19, 121–129. [Google Scholar]
- Tanabe, Y.; Shimizu, K.; Kondo, E.; Yasumatsu, M.; Nakamura, D.; Sagayama, H.; Takahashi, H. Urinary N-Terminal Fragment of Titin Reflects Muscle Damage After a Soccer Match in Male Collegiate Soccer Players. J. Strength Cond. Res. 2021, 35, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Tharp, C.; Mestroni, L.; Taylor, M. Modifications of Titin Contribute to the Progression of Cardiomyopathy and Represent a Therapeutic Target for Treatment of Heart Failure. J. Clin. Med. 2020, 9, 2770. [Google Scholar] [CrossRef] [PubMed]
- Yoshihisa, A.; Kimishima, Y.; Kiko, T.; Sato, Y.; Watanabe, S.; Kanno, Y.; Abe, S.; Miyata, M.; Sato, T.; Suzuki, S.; et al. Usefulness of Urinary N-Terminal Fragment of Titin to Predict Mortality in Dilated Cardiomyopathy. Am. J. Cardiol. 2018, 121, 1260–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wischmeyer, P.E.; Puthucheary, Z.; Millán, I.S.; Butz, D.; Grocott, M.P. Muscle mass and physical recovery in ICU: Innovations for targeting of nutrition and exercise. Curr. Opin. Crit. Care 2017, 23, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.M.; Lee, A.C.; Zeleznik, H.; Scott, J.P.C.; Fatima, A.; Needham, D.M.; Ohtake, P.J. Home and Community-Based Physical Therapist Management of Adults With Post–Intensive Care Syndrome. Phys. Ther. 2020, 100, 1062–1073. [Google Scholar] [CrossRef] [PubMed]
- Denehy, L.; Skinner, E.H.; Edbrooke, L.; Haines, K.; Warrillow, S.; Hawthorne, G.; Gough, K.; Hoorn, S.V.; Morris, M.E.; Berney, S. Exercise rehabilitation for patients with critical illness: A randomized controlled trial with 12 months of follow-up. Crit. Care 2013, 17, R156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.; Puthucheary, Z. Is rehabilitation post critical illness a new anti-inflammatory agent? Thorax 2016, 71, 783–784. [Google Scholar] [CrossRef] [Green Version]
- Brook, M.S.; Wilkinson, D.J.; Atherton, P.J. Nutrient modulation in the management of disease-induced muscle wasting: Evidence from human studies. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Ulanova, A.; Gritsyna, Y.; Salmov, N.; Lomonosova, Y.; Belova, S.; Nemirovskaya, T.; Shenkman, B.; Vikhlyantsev, I.M. Effect of L-Arginine on Titin Expression in Rat Soleus Muscle After Hindlimb Unloading. Front. Physiol. 2019, 10, 1221. [Google Scholar] [CrossRef] [Green Version]
- Oh, E.; Shim, H.; Yon, H.J.; Moon, J.S.; Kang, D.R.; Jang, J.Y. Effectiveness of a multidisciplinary team for nutrition support in a trauma intensive care unit. Acute Crit. Care 2020, 35, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Lopes, M.C.B.R.; Ceniccola, G.D.; Araújo, W.M.C.; Akutsu, R. Nutrition support team activities can improve enteral nutrition administration in intensive care units. Nutrients 2019, 57, 275–281. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factors | Level of Urinary Titin N-Fragment | Evidence |
|---|---|---|
| Age | 2.3, 4.3, 5.7 pmol/mg/Cr in ≤30, 31–60, ≥61 years old | [99] |
| Exercise | 40–100 pmol/mg/Cr in exercise-induced muscle damage | [106,107] |
| Surgery | 30–50 pmol/mg/Cr after cardiac surgery | [103] |
| Cardiac damage | ≥7.26 pmol/mg/Cr in a third of dilated cardiomyopathy | [110] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakanishi, N.; Tsutsumi, R.; Hara, K.; Matsuo, M.; Sakaue, H.; Oto, J. Urinary Titin N-Fragment as a Biomarker of Muscle Atrophy, Intensive Care Unit-Acquired Weakness, and Possible Application for Post-Intensive Care Syndrome. J. Clin. Med. 2021, 10, 614. https://doi.org/10.3390/jcm10040614
Nakanishi N, Tsutsumi R, Hara K, Matsuo M, Sakaue H, Oto J. Urinary Titin N-Fragment as a Biomarker of Muscle Atrophy, Intensive Care Unit-Acquired Weakness, and Possible Application for Post-Intensive Care Syndrome. Journal of Clinical Medicine. 2021; 10(4):614. https://doi.org/10.3390/jcm10040614
Chicago/Turabian StyleNakanishi, Nobuto, Rie Tsutsumi, Kanako Hara, Masafumi Matsuo, Hiroshi Sakaue, and Jun Oto. 2021. "Urinary Titin N-Fragment as a Biomarker of Muscle Atrophy, Intensive Care Unit-Acquired Weakness, and Possible Application for Post-Intensive Care Syndrome" Journal of Clinical Medicine 10, no. 4: 614. https://doi.org/10.3390/jcm10040614