
Early Cortisol and Inflammatory Responses to Parental Cancer and Their Impact on Functional Impairment in Youth

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Sample
2.2. Assessments
2.3. Biological Measures
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mariotto, A.B.; Robin Yabroff, K.; Shao, Y.; Feuer, E.J.; Brown, M.L. Projections of the cost of cancer care in the United States: 2010–2020. J. Natl. Cancer Inst. 2011, 103, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Bradley, C.J.; Yabroff, K.R.; Dahman, B.; Feuer, E.J.; Mariotto, A.; Brown, M.L. Productivity costs of cancer mortality in the United States: 2000–2020. J. Natl. Cancer Inst. 2008, 100, 1763–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weaver, K.E.; Rowland, J.H.; Alfano, C.M.; McNeel, T.S. Parental cancer and the family. Cancer 2010, 116, 4395–4401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.N.; Martini, A.; Preen, D. The well-being of children impacted by a parent with cancer: An integrative review. Supportive Care Cancer 2016, 24, 3235–3251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brent, D.A.; Melhem, N.M.; Masten, A.S.; Porta, G.; Payne, M.W. Longitudinal Effects of Parental Bereavement on Adolescent Developmental Competence. J. Clin. Child Adolesc. Psychol. 2012, 41, 778–791. [Google Scholar] [CrossRef] [Green Version]
- Melhem, N.M.; Porta, G.; Shamseddeen, W.; Payne, M.W.; Brent, D.A. Grief in children and adolescents bereaved by sudden parental death. Arch. Gen. Psychiatry 2011, 68, 911–919. [Google Scholar] [CrossRef] [Green Version]
- Bylund-Grenklo, T.; Fürst, C.J.; Nyberg, T.; Steineck, G.; Kreicbergs, U. Unresolved grief and its consequences. A nationwide follow-up of teenage loss of a parent to cancer 6–9 years earlier. Supportive Care Cancer 2016, 24, 3095–3103. [Google Scholar] [CrossRef]
- Brent, D.; Melhem, N.; Donohoe, M.B.; Walker, M. The Incidence and Course of Depression in Bereaved Youth 21 Months after the Loss of a Parent to Suicide, Accident, or Sudden Natural Death. Am. J. Psychiatry 2009, 166, 786–794. [Google Scholar] [CrossRef]
- Miller, G.E.; Chen, E.; Parker, K.J. Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychol. Bull. 2011, 137, 959–997. [Google Scholar] [CrossRef]
- Slavich, G.M.; Irwin, M.R. From Stress to Inflammation and Major Depressive Disorder: A Social Signal Transduction Theory of Depression. Psychol. Bull. 2014, 140, 774–815. [Google Scholar] [CrossRef]
- Danese, A.; Pariante, C.M.; Caspi, A.; Taylor, A.; Poulton, R. Childhood maltreatment predicts adult inflammation in a life-course study. Proc. Natl. Acad. Sci. USA 2007, 104, 1319–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreasen, N.C. The Family History Method Using Diagnostic Criteria. Arch. Gen. Psychiatry 1977, 34, 1229. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, D. A Children’s Global Assessment Scale (CGAS). Arch. Gen. Psychiatry 1983, 40, 1228. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale construction and psychometric characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef]
- Kovacs, M. The Children’s Depression, Inventory (CDI). Psychopharmacol. Bull. 1985, 21, 995–998. [Google Scholar]
- Foa, E.B.; Riggs, D.S.; Dancu, C.V.; Rothbaum, B.O. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J. Trauma. Stress 1993, 6, 459–473. [Google Scholar] [CrossRef]
- Pennebaker, J.W.; Susman, J.R. Disclosure of traumas and psychosomatic processes. Soc. Sci. Med. 1988, 26, 327–332. [Google Scholar] [CrossRef]
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric properties of the life events checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Hollingshead, A.A. Four-Factor Index of Social Status; Unpublished Work; Yale University: New Haven, CT, USA, 1975. [Google Scholar]
- Stalder, T.; Kirschbaum, C. Analysis of cortisol in hair—State of the art and future directions. Brain Behav. Immun. 2012, 26, 1019–1029. [Google Scholar] [CrossRef] [PubMed]
- Laudenslager, M.L.; Jorgensen, M.J.; Grzywa, R.; Fairbanks, L.A. A novelty seeking phenotype is related to chronic hypothalamic-pituitary-adrenal activity reflected by hair cortisol. Physiol. Behav. 2011, 104, 291–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Collins, L.M.; Schafer, J.L.; Kam, C.M. A comparison of inclusive and restrictive strategies in modern missing data procedures. Psychol. Methods 2001, 6, 330–351. [Google Scholar] [CrossRef]
- Pham, S.; Porta, G.; Biernesser, C.; Walker Payne, M.; Iyengar, S.; Melhem, N.; Brent, D.A. The burden of bereavement: Early-onset depression and impairment in youths bereaved by sudden parental death in a 7-year prospective study. Am. J. Psychiatry 2018, 175, 887–896. [Google Scholar] [CrossRef]
- Steudte, S.; Kirschbaum, C.; Gao, W.; Alexander, N.; Schönfeld, S.; Hoyer, J.; Stalder, T. Hair cortisol as a biomarker of traumatization in healthy individuals and posttraumatic stress disorder patients. Biol. Psychiatry 2013, 74, 639–646. [Google Scholar] [CrossRef]
- Gray, N.A.; Dhana, A.; Van Der Vyver, L.; Van Wyk, J.; Khumalo, N.P.; Stein, D.J. Determinants of hair cortisol concentration in children: A systematic review. Psychoneuroendocrinology 2018, 87, 204–214. [Google Scholar] [CrossRef]
- White, L.O.; Ising, M.; von Klitzing, K.; Sierau, S.; Michel, A.; Klein, A.M.; Andreas, A.; Keil, J.; Quintero, L.; Müller-Myhsok, B.; et al. Reduced hair cortisol after maltreatment mediates externalizing symptoms in middle childhood and adolescence. J. Child Psychol. Psychiatry 2017, 58, 998–1007. [Google Scholar] [CrossRef]
- Ford, J.L.; Boch, S.J.; Browning, C.R. Hair cortisol and depressive symptoms in youth: An investigation of curvilinear relationships. Psychoneuroendocrinology 2019, 109, 104376. [Google Scholar] [CrossRef]
- Straub, J.; Klaubert, L.M.; Schmiedgen, S.; Kirschbaum, C.; Goldbeck, L. Hair cortisol in relation to acute and post-traumatic stress symptoms in children and adolescents. Anxiety Stress Coping 2017, 30, 661–670. [Google Scholar] [CrossRef]
- Fuchs, A.; Jaite, C.; Neukel, C.; Dittrich, K.; Bertsch, K.; Kluczniok, D.; Möhler, E.; Attar, C.H.; Brunner, R.; Bödeker, K.; et al. Link between children’s hair cortisol and psychopathology or quality of life moderated by childhood adversity risk. Psychoneuroendocrinology 2018, 90, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Bick, J.; Nguyen, V.; Leng, L.; Piecychna, M.; Crowley, M.J.; Bucala, R.; Mayes, L.C.; Grigorenko, E.L. Preliminary associations between childhood neglect, MIF, and cortisol: Potential pathways to long-term disease risk. Dev. Psychobiol. 2015, 57, 131–139. [Google Scholar] [CrossRef]
- Dietz, L.J.; Stoyak, S.; Melhem, N.; Porta, G.; Matthews, K.A.; Payne, M.W.; Brent, D.A. Cortisol response to social stress in parentally bereaved youth. Biol. Psychiatry 2013, 73, 379–387. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.A.; Sheridan, M.A.; Tibu, F.; Fox, N.A.; Zeanah, C.H.; Nelson, C.A. Causal effects of the early caregiving environment on development of stress response systems in children. Proc. Natl. Acad. Sci. USA 2015, 112, 5637–5642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.C.; Compas, B.E.; Garber, J. Relations among posttraumatic stress disorder, comorbid major depression, and HPA function: A systematic review and meta-analysis. Clin. Psychol. Rev. 2012, 32, 301–315. [Google Scholar] [CrossRef] [Green Version]
- Pfeffer, C.R.; Altemus, M.; Heo, M.; Jiang, H. Salivary Cortisol and Psychopathology in Children Bereaved by the September 11, 2001 Terror Attacks. Biol. Psychiatry 2007, 61, 957–965. [Google Scholar] [CrossRef]
- Stetler, C.; Miller, G.E. Depression and Hypothalamic-Pituitary-Adrenal Activation: A Quantitative Summary of Four Decades of Research. Psychosom. Med. 2011, 73, 114–126. [Google Scholar] [CrossRef]
- Copeland, W.E.; Shanahan, L.; Worthman, C.; Angold, A.; Costello, E.J. Cumulative Depression Episodes Predict Later C-Reactive Protein Levels: A Prospective Analysis. Biol. Psychiatry 2012, 71, 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, G.E.; Cole, S.W. Clustering of depression and inflammation in adolescents previously exposed to childhood adversity. Biol. Psychiatry 2012, 72, 34–40. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Controls | Cancer | Test | df | p | Cohen’s d | |
|---|---|---|---|---|---|---|
| n = 26 | n = 32 | |||||
| Demographics | ||||||
| Age, in years, Mean ± SD | 17.0 ± 3.5 | 17.0 ± 3.3 | t = 0.1 | 56 | 0.95 | 0.02 |
| Socioeconomic Status (SES), Mean ± SD | 39.2 ± 4.7 | 41.2 ± 3.8 | t = −1.6 | 45 | 0.12 | 0.47 |
| Sex, % Female (n) | 34.6 (9) | 78.1 (25) | χ2 = 11.2 | 1 | 0.001 | 0.98 |
| Body Mass Index (BMI), Mean ± SD | 24.2 ± 4.3 | 23.7 ± 6.6 | t = 0.3 | 50 | 0.77 | −0.08 |
| Prior Psychiatric Disorders and Stressors | ||||||
| Childhood Trauma, Mean ± SD | 30.5 ± 6.6 | 31.3 ± 5.4 | t = −0.5 | 46 | 0.64 | 0.14 |
| Negative Life Experiences, Mean ± SD | 5.9 ± 8.5 | 6.6 ± 4.9 | t = −0.6 | 56 | 0.81 | 0.08 |
| History of Psychiatric Disorders, % Yes (n) | 26.9 (7) | 31.2 (10) | χ2 = 0.8 | 1 | 0.38 | 0.24 |
| Psychiatric Symptoms at Intake | ||||||
| Functional Impairment, Mean ± SD | 87.8 ± 7.9 | 82.2 ± 10.5 | t = 2.1 | 48 | 0.04 | −0.60 |
| Depression Symptoms, Mean ± SD | 6.2 ± 6.7 | 11.6 ± 8.2 | t = 2.8 | 54 | 0.01 | 0.80 |
| Anxiety Symptoms, Mean ± SD | 13.1 ± 12.5 | 23.7 ± 15.6 | t = 2.5 | 50 | 0.02 | 0.73 |
| PTSD Symptoms (PSS-I), Mean ± SD | 2.0 ± 2.9 | 3.4 ± 3.8 | t = 1.0 | 33 | 0.32 | 0.39 |
| Sleep, Mean ± SD | 3.6 ± 3.3 | 4.4 ± 3.0 | t = 0.9 | 53 | 0.33 | 0.26 |
| Perceived Stress Scale, Mean ± SD | 16.8 ± 8.6 | 25.3 ± 9.9 | t = 3.4 | 53 | 0.003 | 0.95 |
| Biological Measures at Intake | ||||||
| C-Reactive Protein (ln), Mean ± SD | −3.7 ± 1.9 | −3.4 ± 2.1 | t = 0.7 | 50 | 0.48 | 0.20 |
| Total Diurnal Cortisol, AUCcort * (ln), Mean ± SD | 13.3 ± 0.8 | 13.2 ± 0.9 | t = −0.04 | 41 | 0.94 | −0.01 |
| Cortisol Awakening Response, CAR (/1000), Mean ± SD | −0.3 ± 0.9 | 0.3 ± 1.2 | t = −1.7 | 38 | 0.10 | −0.53 |
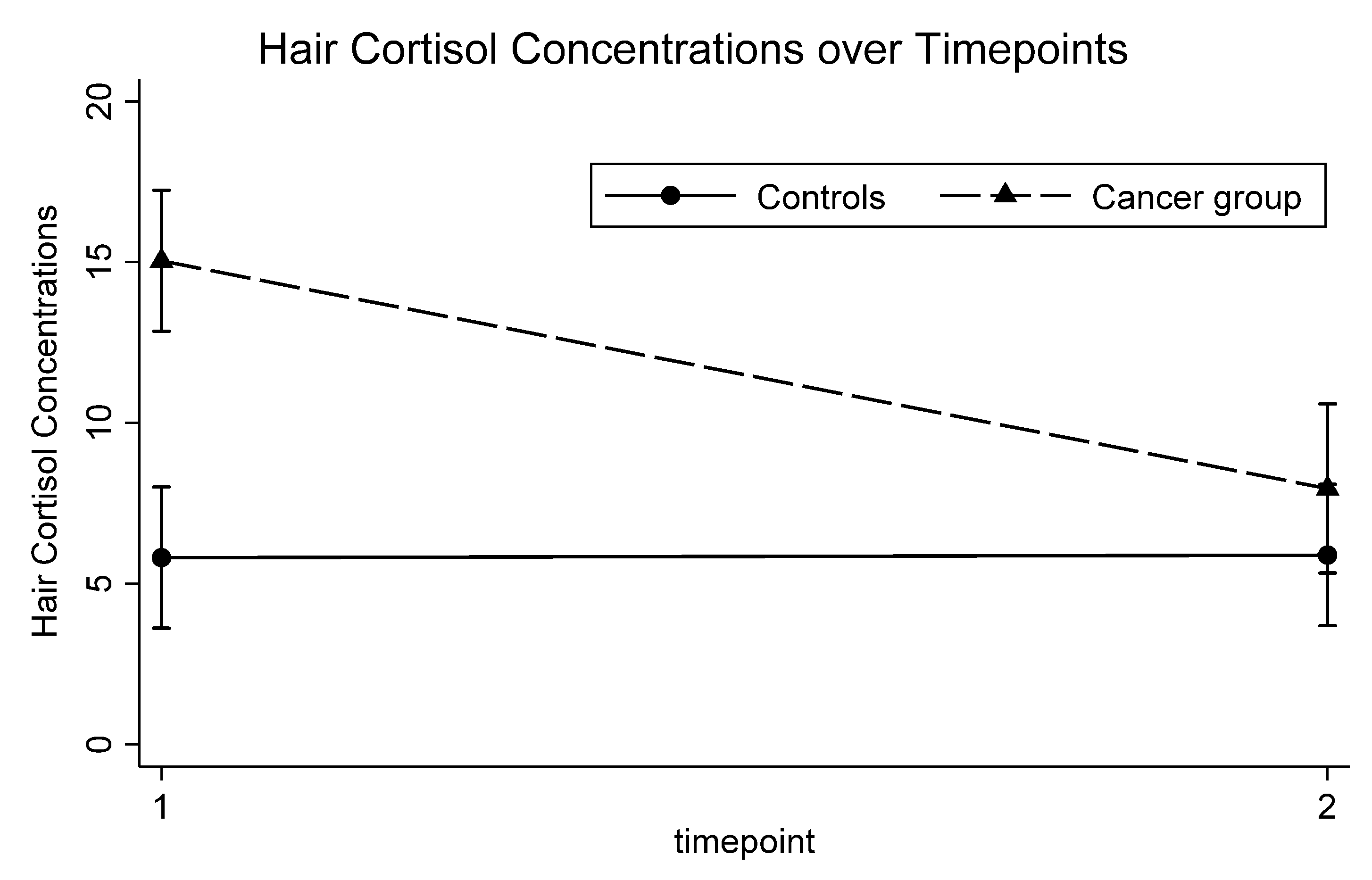
| Hair Cortisol Concentrations (HCC), Mean ± SD | 5.8 ± 2.3 | 15.0 ± 8.5 | t = 5.0 | 44 | <0.001 | 2.21 |
| Glucocorticoid Receptor or GR Sensitivity (AUC, /1000) ± SD | 124.3 ± 81.6 | 121.0 ± 75.3 | t = 0.2 | 48 | 0.88 | −0.04 |
| Stimulated IL-6 Production (/1000) ± SD | 40.4 ± 22.5 | 34.2 ± 21.4 | t = 1.0 | 48 | 0.32 | −0.23 |
| Group (Cancer vs. Controls) | ||||
|---|---|---|---|---|
| β | 95% CI | p | d | |
| Psychiatric Symptoms | ||||
| Functional Impairment (CGAS) | −5.5 | −11.7, 0.7 | 0.08 | −0.33 |
| Depression Symptoms (CDI) | 5.7 | 1.4, 9.9 | 0.01 | 0.50 |
| Anxiety Symptoms (SCARED) | 7.8 | −2.6, 18.2 | 0.14 | 0.3 |
| Perceived Stress Scale (PSS) | 7.8 | 1.4, 14.3 | 0.02 | 0.48 |
| Biological Measures | ||||
| CRP (ln) | 0.4 | −0.7, 1.5 | 0.46 | 0.19 |
| AUCcort (ln) | −0.1 | −0.8, 0.6 | 0.78 | −0.09 |
| CAR | 0.4 | −0.7, 1.5 | 0.46 | 0.21 |
| HCC | 9.2 | 4.3, 14.1 | 0.001 | 1.47 |
| GR Sensitivity | −1.5 | −6.8, 3.7 | 0.57 | −0.17 |
| Stimulated Production of IL-6 | −9.3 | −22.1, 3.5 | 0.15 | −0.43 |
| Model 1 | Model 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p | d | β | 95% CI | p | d | |
| Functional Impairment | ||||||||
| Group * | −5.5 | −10.4, −0.6 | 0.03 | −0.40 | −4.7 | −9.8, 0.4 | 0.07 | −0.31 |
| Time | −0.001 | −0.01, 0.01 | 0.92 | −0.02 | −0.001 | −0.01, 0.01 | 0.90 | 0.01 |
| Group X Time | 0.005 | −0.01, 0.02 | 0.60 | 0.09 | 0.005 | −0.01, 0.02 | 0.56 | 0.07 |
| Sex ** | — | — | — | — | −1.9 | −6.3, 2.5 | 0.40 | −0.11 |
| Age | — | — | — | — | −0.6 | −1.1, 0.1 | 0.09 | −0.30 |
| C-Reactive Protein (ln) | ||||||||
| Group * | 0.6 | −0.5, 1.7 | 0.27 | 0.24 | 0.52 | −0.5, 1.6 | 0.34 | 0.21 |
| Time | 0.001 | −0.002, 0.003 | 0.66 | 0.09 | 0.001 | −0.002, 0.003 | 0.80 | 0.06 |
| Group X Time | −0.001 | −0.01, 0.002 | 0.45 | −0.16 | −0.001 | −0.01, 0.002 | 0.45 | −0.16 |
| Sex ** | — | — | — | — | 0.1 | −0.9, 1.2 | 0.78 | 0.06 |
| Age | — | — | — | — | 0.07 | −0.1, 0.2 | 0.29 | 0.23 |
| BMI | — | — | — | — | 0.2 | 0.08, 0.2 | <0.001 | 0.93 |
| Total Diurnal Cortisol (AUCcortƒ, ln) | ||||||||
| Group * | −0.01 | −0.5, 0.5 | 0.98 | −0.01 | −0.07 | −0.6, 0.5 | 0.80 | −0.06 |
| Time | −0.001 | −0.003, 0.002 | 0.65 | −0.11 | −0.001 | −0.003, 0.002 | 0.51 | −0.17 |
| Group X Time | −0.001 | −0.004, 0.002 | 0.71 | −0.09 | −0.001 | −0.004, 0.003 | 0.74 | −0.08 |
| Sex ** | — | — | — | — | 0.4 | −0.04, 0.9 | 0.07 | 0.46 |
| Age | — | — | — | — | −0.001 | −0.06, 0.06 | 0.97 | −0.01 |
| BMI | — | — | — | — | 0.04 | −0.01, 0.1 | 0.12 | 0.40 |
| Cortisol Awakening Response | ||||||||
| Group * | 0.4 | −0.3, 1.1 | 0.26 | 0.30 | 0.1 | −0.6, 0.8 | 0.70 | 0.10 |
| Time | 0.001 | −0.002, 0.003 | 0.48 | 0.18 | 0.001 | −0.001, 0.004 | 0.29 | 0.29 |
| Group X Time | 0.001 | −0.002, 0.005 | 0.45 | 0.20 | 0.001 | −0.002, 0.005 | 0.36 | 0.25 |
| Sex ** | — | — | — | — | 0.6 | −0.1, 1.3 | 0.10 | 0.45 |
| Age | — | — | — | — | −0.09 | −0.2, −0.004 | 0.04 | 0.58 |
| BMI | — | — | — | — | 0.01 | −0.07, 0.09 | 0.08 | 0.08 |
| Hair Cortisol Concentrations | ||||||||
| Group * | 10.8 | 7.1, 14.4 | <0.001 | 1.62 | 10.5 | 6.6, 14.5 | <0.001 | 1.43 |
| Time | −0.001 | −0.01, 0.01 | 0.81 | −0.05 | −0.001 | −0.01, 0.01 | 0.79 | −0.06 |
| Group X Time | −0.03 | −0.04, −0.01 | <0.001 | −1.14 | −0.03 | −0.04, −0.01 | <0.001 | −1.08 |
| Sex ** | — | — | — | — | 1.0 | −2.2, 4.2 | 0.54 | 0.14 |
| Age | — | — | — | — | 0.3 | −0.1, 0.8 | 0.14 | 0.33 |
| BMI | — | — | — | — | 0.06 | −0.2, 0.3 | 0.66 | 0.10 |
| GR Sensitivity * | ||||||||
| Group | 4.8 | −4.2, 5.1 | 0.84 | 0.05 | −1.7 | −4.9, 4.5 | 0.94 | −0.02 |
| Time | −0.03 | −0.2, 0.2 | 0.72 | −0.08 | −0.1 | −0.2, 0.1 | 0.61 | −0.12 |
| Group X Time | −0.1 | −0.3, 0.2 | 0.69 | −0.09 | −0.02 | −0.3, 0.2 | 0.86 | −0.04 |
| Sex ** | — | — | — | — | −6.1 | −4.2, 3.0 | 0.74 | −0.08 |
| Age | — | — | — | — | 4.4 | −0.5, 9.4 | 0.08 | 0.41 |
| BMI | — | — | — | — | 0.05 | −3.2, 3.3 | 0.98 | 0.01 |
| Stimulated Production of IL-6 * | ||||||||
| Group | −4.5 | −1.7, 0.8 | 0.48 | −0.16 | −7.0 | −1.9, 0.5 | 0.26 | −0.26 |
| Time | 0.01 | −0.05, 0.06 | 0.73 | 0.08 | −0.01 | −0.07, 0.04 | 0.61 | −0.12 |
| Group X Time | −0.03 | −0.1, 0.04 | 0.43 | −0.18 | −0.002 | −0.07, 0.07 | 0.94 | −0.02 |
| Sex ** | — | — | — | — | 2.5 | −8.3, 13.3 | 0.65 | 0.10 |
| Age | — | — | — | — | 1.6 | 0.2, 3.0 | 0.02 | 0.54 |
| BMI | — | — | — | — | −0.1 | −1.0, 0.8 | 0.78 | −0.06 |
| Functional Impairment | ||||
|---|---|---|---|---|
| β | 95% CI | p | d | |
| C-Reactive Protein | ||||
| CRP (ln) | 0.6 | −0.4, 1.6 | 0.27 | 0.24 |
| Group * | −4.8 | −10.3, 0.6 | 0.08 | −0.38 |
| Time | −0.01 | −0.02, 0.01 | 0.29 | −0.23 |
| Group X Time | −0.001 | −0.02, 0.02 | 0.92 | −0.02 |
| Total Diurnal Cortisol | ||||
| AUCcort ** (ln) | −3.0 | −5.5, −0.5 | 0.02 | −0.60 |
| Group * | −5.9 | −11.6, −0.1 | 0.04 | −0.51 |
| Time | −0.002 | −0.02, 0.02 | 0.80 | −0.06 |
| Group X Time | −0.003 | −0.03, 0.02 | 0.79 | 0.07 |
| Cortisol Awakening Response | ||||
| CAR | −0.4 | −2.0, 1.3 | 0.64 | −0.12 |
| Group * | −5.0 | −11.5, 1.5 | 0.13 | −0.40 |
| Time | 0.001 | −0.02, 0.02 | 0.89 | 0.04 |
| Group X Time | −0.004 | −0.03, 0.02 | 0.73 | −0.09 |
| Hair Cortisol Concentrations | ||||
| HCC | −0.3 | −0.6, 0.1 | 0.16 | −0.31 |
| Group * | −3.0 | −9.1, 3.1 | 0.34 | −0.21 |
| Time | −0.01 | −0.03, 0.01 | 0.31 | −0.22 |
| Group X Time | −0.002 | −0.03, 0.02 | 0.87 | 0.03 |
| GR Sensitivity | ||||
| GR Sensitivity | −0.003 | −0.03, 0.02 | 0.82 | −0.05 |
| Group * | −3.6 | −9.5, 2.3 | 0.23 | −0.26 |
| Time | −0.003 | −0.02, 0.02 | 0.77 | −0.06 |
| Group X Time | −0.01 | −0.03, 0.02 | 0.60 | −0.11 |
| Stimulated Production of IL-6 | ||||
| Stimulated Production of IL-6 | −0.001 | −0.08, 0.08 | 0.98 | 0.01 |
| Group * | −3.6 | −9.5, 2.3 | 0.23 | −0.27 |
| Time | −0.003 | −0.02, 0.02 | 0.79 | −0.06 |
| Group X Time | −0.01 | −0.03, 0.02 | 0.60 | −0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, B.; Brent, J.; Zhong, Y.; Bazmi, S.; Porta, G.; Bovbjerg, D.H.; Tarhini, A.; Kirkwood, J.M.; Brent, D.A.; Marsland, A.; et al. Early Cortisol and Inflammatory Responses to Parental Cancer and Their Impact on Functional Impairment in Youth. J. Clin. Med. 2021, 10, 576. https://doi.org/10.3390/jcm10040576
Hayes B, Brent J, Zhong Y, Bazmi S, Porta G, Bovbjerg DH, Tarhini A, Kirkwood JM, Brent DA, Marsland A, et al. Early Cortisol and Inflammatory Responses to Parental Cancer and Their Impact on Functional Impairment in Youth. Journal of Clinical Medicine. 2021; 10(4):576. https://doi.org/10.3390/jcm10040576
Chicago/Turabian StyleHayes, Benjamin, Jacob Brent, Yongqi Zhong, Shervin Bazmi, Giovanna Porta, Dana H. Bovbjerg, Ahmad Tarhini, John M. Kirkwood, David A. Brent, Anna Marsland, and et al. 2021. "Early Cortisol and Inflammatory Responses to Parental Cancer and Their Impact on Functional Impairment in Youth" Journal of Clinical Medicine 10, no. 4: 576. https://doi.org/10.3390/jcm10040576