
Cardiorespiratory Functioning in Youth with Persistent Post-Concussion Symptoms: A Pilot Study

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design and Setting
2.2. Participants
2.3. Instrumentation and Outcome Measures
2.3.1. Neurobehavioral Measures
2.3.2. Capnometry Instrumentation and Assessment
2.3.3. Statistical Analyses
3. Results
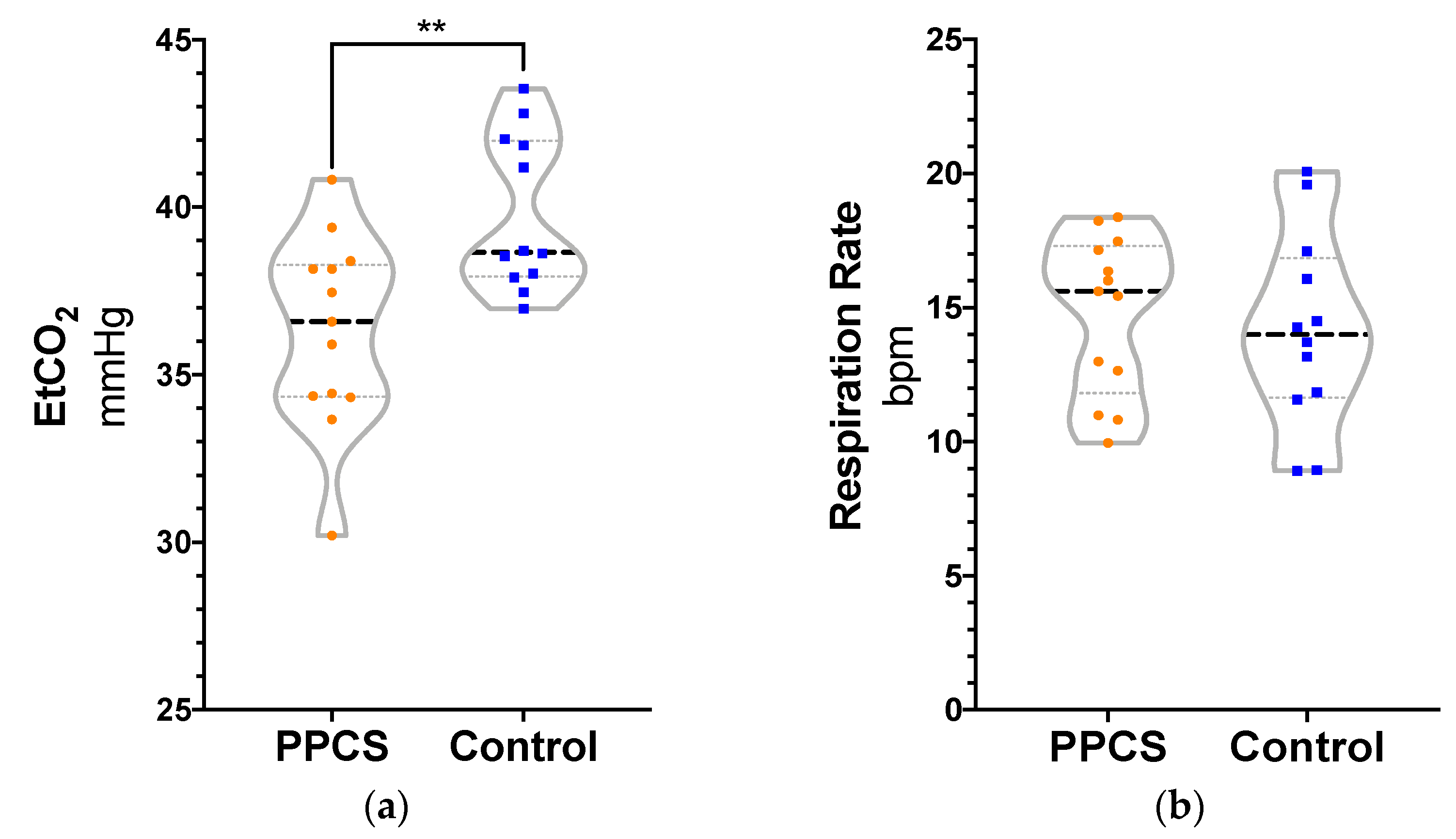
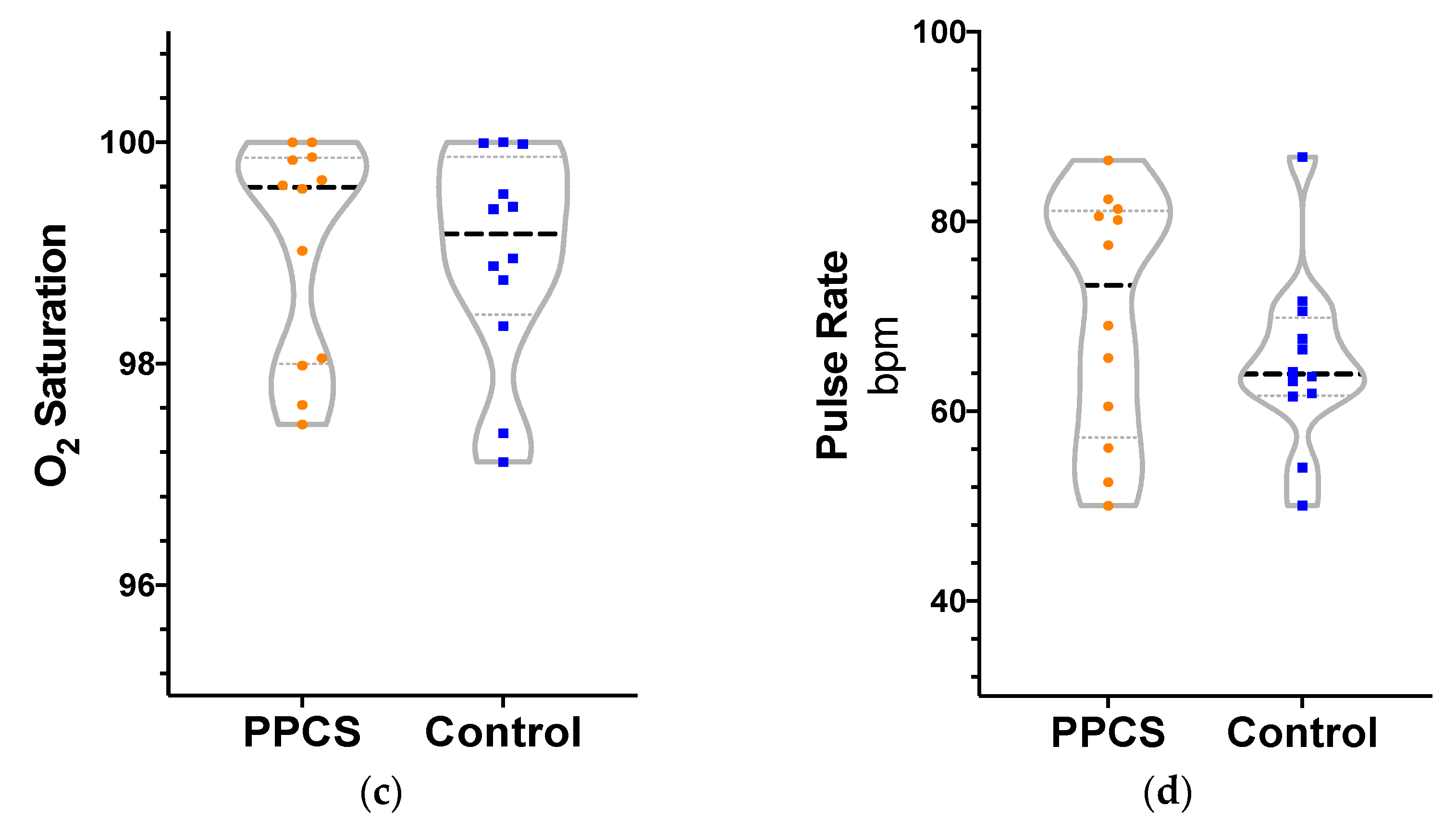
3.1. Cardiorespiratory Variables by Group
3.2. Cardiorespiratory Variables and Neurobehavioral Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carroll, L.J.; Cassidy, J.D.; Peloso, P.M.; Borg, J.; Von Holst, H.; Holm, L.; Paniak, C.; Pépin, M. Prognosis for mild traumatic brain injury: Results of the who collaborating centre task force on mild traumatic brain injury. J. Rehabil. Med. 2004, 36, 84–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losoi, H.; Silverberg, N.D.; Wäljas, M.; Turunen, S.; Rosti-Otajärvi, E.; Helminen, M.; Luoto, T.M.; Julkunen, J.; Öhman, J.; Iverson, G.L. Recovery from Mild Traumatic Brain Injury in Previously Healthy Adults. J. Neurotrauma 2016, 33, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Norrie, J.; Heitger, M.; Leathem, J.; Anderson, T.; Jones, R.; Flett, R. Mild traumatic brain injury and fatigue: A prospective longitudinal study. Brain Inj. 2010, 24, 1528–1538. [Google Scholar] [CrossRef] [PubMed]
- Åhman, S.; Saveman, B.-I.; Styrke, J.; Björnstig, U.; Stålnacke, B.-M. Long-term follow-up of patients with mild traumatic brain injury: A mixed-method study. J. Rehabil. Med. 2013, 45, 758–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlow, K.M.; Crawford, S.; Stevenson, A.; Sandhu, S.S.; Belanger, F.; Dewey, D. Epidemiology of Postconcussion Syndrome in Pediatric Mild Traumatic Brain Injury. Pediatrics 2010, 126, e374–e381. [Google Scholar] [CrossRef]
- Babcock, L.; Byczkowski, T.; Wade, S.L.; Ho, M.; Mookerjee, S.; Bazarian, J.J. Predicting Postconcussion Syndrome After Mild Traumatic Brain Injury in Children and Adolescents Who Present to the Emergency Department. JAMA Pediatr. 2013, 167, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Janak, J.C.; Cooper, D.B.; Bowles, A.O.; Alamgir, A.H.; Cooper, S.P.; Gabriel, K.P.; Pérez, A.; Orman, J.A. Completion of Multidisciplinary Treatment for Persistent Postconcussive Symptoms Is Associated with Reduced Symptom Burden. J. Head Trauma Rehabil. 2017, 32, 1–15. [Google Scholar] [CrossRef]
- Grabowski, P.; Wilson, J.; Walker, A.; Enz, D.; Wang, S. Multimodal impairment-based physical therapy for the treatment of patients with post-concussion syndrome: A retrospective analysis on safety and feasibility. Phys. Ther. Sport 2017, 23, 22–30. [Google Scholar] [CrossRef]
- Thastum, M.M.; Rask, C.U.; Naess-Schmidt, E.T.; Jensen, J.S.; Frederiksen, O.-V.; Tuborgh, A.; Svendsen, S.W.; Nielsen, J.F.; Schröder, A. Design of an early intervention for persistent post-concussion symptoms in adolescents and young adults: A feasibility study. Neurorehabilitation 2018, 43, 155–167. [Google Scholar] [CrossRef]
- Dobney, D.M.; Grilli, L.; Kocilowicz, H.; Beaulieu, C.; Straub, M.; Friedman, D.; Gagnon, I. Evaluation of an active rehabilitation program for concussion management in children and adolescents. Brain Inj. 2017, 31, 1753–1759. [Google Scholar] [CrossRef]
- Gagnon, I.; Grilli, L.; Friedman, D.; Iverson, G.L. A pilot study of active rehabilitation for adolescents who are slow to recover from sport-related concussion. Scand. J. Med. Sci. Sports 2016, 26, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L. A biopsychosocial conceptualization of poor outcome from mTBI. In PTSD Mild Traumatic Brain Injury; The Guilford Press: New York, NY, USA, 2012; pp. 37–60. [Google Scholar]
- Kenzie, E.S.; Parks, E.L.; Bigler, E.D.; Lim, M.M.; Chesnutt, J.C.; Wakeland, W. Concussion as a Multi-Scale Complex System: An Interdisciplinary Synthesis of Current Knowledge. Front. Neurol. 2017, 8, 513. [Google Scholar] [CrossRef] [Green Version]
- McCrea, M.; Broshek, D.K.; Barth, J.T. Sports concussion assessment and management: Future research directions. Brain Inj. 2015, 29, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Wäljas, M.; Iverson, G.L.; Lange, R.T.; Hakulinen, U.; Dastidar, P.; Huhtala, H.; Liimatainen, S.; Hartikainen, K.M.; Öhman, J. A Prospective Biopsychosocial Study of the Persistent Post-Concussion Symptoms following Mild Traumatic Brain Injury. J. Neurotrauma 2015, 32, 534–547. [Google Scholar] [CrossRef]
- Voormolen, D.C.; Cnossen, M.C.; Polinder, S.; Gravesteijn, B.Y.; Von Steinbuechel, N.; Real, R.G.; Haagsma, J.A. Prevalence of post-concussion-like symptoms in the general population in Italy, The Netherlands and the United Kingdom. Brain Inj. 2019, 33, 1078–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asken, B.M.; Snyder, A.R.; Smith, M.S.; Zaremski, J.L.; Bauer, R.M. Concussion-like symptom reporting in non-concussed adolescent athletes. Clin. Neuropsychol. 2017, 31, 138–153. [Google Scholar] [CrossRef]
- Hutchison, M.G.; Mainwaring, L.; Senthinathan, A.; Churchill, N.; Thomas, S.; Richards, D. Psychological and Physiological Markers of Stress in Concussed Athletes Across Recovery Milestones. J. Head Trauma Rehabil. 2017, 32, E38–E48. [Google Scholar] [CrossRef]
- Leddy, J.J.; Kozlowski, K.; Fung, M.; Pendergast, D.R.; Willer, B. Regulatory and autoregulatory physiological dysfunction as a primary characteristic of post concussion syndrome: Implications for treatment. Neurorehabilitation 2007, 22, 199–205. [Google Scholar] [CrossRef]
- Sung, C.-W.; Lee, H.-C.; Chiang, Y.-H.; Chiu, W.-T.; Chu, S.-F.; Ou, J.-C.; Tsai, S.-H.; Liao, K.-H.; Lin, C.-M.; Lin, J.-W.; et al. Early dysautonomia detected by heart rate variability predicts late depression in female patients following mild traumatic brain injury. Psychophysiology 2016, 53, 455–464. [Google Scholar] [CrossRef]
- Howard, L.; Dumkrieger, G.; Chong, C.; Ross, K.; Berisha, V.; Schwedt, T. Symptoms of autonomic dysfunction in persistent post-traumatic headache versus migraine. In Headache; Wiley: New York, NY, USA, 2018; Volume 58, pp. 62–63. [Google Scholar]
- Shechter, A.; Stewart, W.F.; Silberstein, S.D.; Lipton, R.B. Migraine and autonomic nervous system function: A population-based, case-control study. Neurology 2002, 58, 422–427. [Google Scholar] [CrossRef]
- Iverson, G.L.; McCracken, L.M. ‘Postconcussive’ symptoms in persons with chronic pain. Brain Inj. 1997, 11, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Boris, J.R. Postural orthostatic tachycardia syndrome in children and adolescents. Auton. Neurosci. Basic Clin. 2018, 215, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Aydemir, M.; Yazisiz, V.; Basarici, I.; Avci, A.B.; Erbasan, F.; Belgi, A.; Terzioglu, E. Cardiac autonomic profile in rheumatoid arthritis and systemic lupus erythematosus. Lupus 2009, 19, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Leddy, J.; Baker, J.G.; Haider, M.N.; Hinds, A.; Willer, B. A Physiological Approach to Prolonged Recovery from Sport-Related Concussion. J. Athl. Train. 2017, 52, 299–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esterov, D.; Greenwald, B.D. Autonomic Dysfunction after Mild Traumatic Brain Injury. Brain Sci. 2017, 7, 100. [Google Scholar] [CrossRef]
- Polak, P.; Leddy, J.J.; Dwyer, M.G.; Willer, B.; Zivadinov, R. Diffusion tensor imaging alterations in patients with postconcussion syndrome undergoing exercise treatment: A pilot longitudinal study. J. Head Trauma Rehabil. 2015, 30, E32–E42. [Google Scholar] [CrossRef] [PubMed]
- Heyer, G.L.; Fischer, A.; Wilson, J.; MacDonald, J.; Cribbs, S.; Ravindran, R.; Pommering, T.L.; Cuff, S. Orthostatic intolerance and autonomic dysfunction in youth with persistent postconcussion symptoms: A head-upright tilt table study. Clin. J. Sport Med. 2016, 26, 40–45. [Google Scholar] [CrossRef]
- Hilz, M.J.; Defina, P.A.; Anders, S.; Koehn, J.; Lang, C.J.; Pauli, E.; Flanagan, S.R.; Schwab, S.; Marthol, H. Frequency Analysis Unveils Cardiac Autonomic Dysfunction after Mild Traumatic Brain Injury. J. Neurotrauma 2011, 28, 1727–1738. [Google Scholar] [CrossRef]
- Bishop, S.; Dech, R.; Baker, T.; Butz, M.; Aravinthan, K.; Neary, J.P. Parasympathetic baroreflexes and heart rate variability during acute stage of sport concussion recovery. Brain Inj. 2017, 31, 247–259. [Google Scholar] [CrossRef]
- LaFountaine, M.F.; Heffernan, K.S.; Gossett, J.D.; Bauman, W.A.; De Meersman, R.E. Transient suppression of heart rate complexity in concussed athletes. Auton. Neurosci. Basic Clin. 2009, 148, 101–103. [Google Scholar] [CrossRef]
- Tan, G.; Fink, B.; Dao, T.K.; Hebert, R.; Farmer, L.S.; Sanders, A.; Pastorek, N.; Gevirtz, R. Associations among Pain, PTSD, mTBI, and Heart Rate Variability in Veterans of Operation Enduring and Iraqi Freedom: A Pilot Study. Pain Med. 2009, 10, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abaji, J.P.; Curnier, D.; Moore, R.D.; Ellemberg, D. Persisting Effects of Concussion on Heart Rate Variability during Physical Exertion. J. Neurotrauma 2016, 33, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Roberson-Nay, R.; Beadel, J.R.; Gorlin, E.I.; Latendresse, S.J.; Teachman, B.A. Examining the latent class structure of CO2 hypersensitivity using time course trajectories of panic response systems. J. Behav. Ther. Exp. Psychiatry 2015, 47, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griez, E.; Schruers, K. Experimental pathophysiology of panic. J. Psychosom. Res. 1998, 45, 493–503. [Google Scholar] [CrossRef]
- Roth, W.T. Physiological markers for anxiety: Panic disorder and phobias. Int. J. Psychophysiol. 2005, 58, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Krapf, R.; Beeler, I.; Hertner, D.; Hulter, H.N. Chronic Respiratory Alkalosis. N. Engl. J. Med. 1991, 324, 1394–1401. [Google Scholar] [CrossRef] [PubMed]
- Rafferty, G.F.; Saisch, S.; Gardner, W. Relation of hypocapnic symptoms to rate of fall of end-tidal PCO2 in normal subjects. Respir. Med. 1992, 86, 335–340. [Google Scholar] [CrossRef]
- Blau, J.N.; Wiles, C.M.; Solomon, F.S. Unilateral somatic symptoms due to hyperventilation. BMJ 1983, 286, 1108. [Google Scholar] [CrossRef] [Green Version]
- Wilhelm, F.H.; Gevirtz, R.; Roth, W.T. Respiratory Dysregulation in Anxiety, Functional Cardiac, and Pain Disorders: Assessment, phenomenology, and treatment. Behav. Modif. 2001, 25, 513–545. [Google Scholar] [CrossRef] [Green Version]
- Paulus, M.P. The breathing conundrum-interoceptive sensitivity and anxiety. Depress. Anxiety 2013, 30, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Siedlecki, P.; Sanzo, P.; Zerpa, C.; Newhouse, I. End-tidal carbon dioxide levels in patients with post-concussion syndrome during neurocognitive and physical tasks compared to a normative control group. Brain Inj. 2018, 32, 1824–1833. [Google Scholar] [CrossRef] [PubMed]
- Sady, M.D.; Vaughan, C.G.; Gioia, G.A. Psychometric Characteristics of the Postconcussion Symptom Inventory in Children and Adolescents. Arch. Clin. Neuropsychol. 2014, 29, 348–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.-T.; Golub, E.; Katz, E.P. Electrostatic side chain complementarity in collagen fibrils. J. Mol. Biol. 1975, 98, 835–839. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An Inventory for Measuring Clinical Anxiety: Psychometric Properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Schatz, P. Repeatable Battery for the Assessment of Neuropsychological Status. In Encyclopedia of Clinical Neuropsychology; The Psychological Corporation: San Antonio, TX, USA, 2018. [Google Scholar] [CrossRef]
- IBM Corp. SPSS Statistics, Version 26.0; IBM Software Business Analytics: Armonk, NY, USA, 2019. [Google Scholar]
- Coffman, K.E.; Cheuvront, S.N.; Salgado, R.M.; Kenefick, R.W. Biological variation of resting measures of ventilation and gas exchange in a large healthy cohort. Eur. J. Appl. Physiol. 2019, 119, 2033–2040. [Google Scholar] [CrossRef]
- Soleimanpour, H.; Taghizadieh, A.; Niafar, M.; Rahmani, F.; Golzari, S.E.J.; Esfanjani, R.M. Predictive Value of Capnography for Suspected Diabetic Ketoacidosis in the Emergency Department. West. J. Emerg. Med. 2013, 14, 590–594. [Google Scholar] [CrossRef]
- Dony, P.; Dramaix, M.; Boogaerts, J.G. Hypocapnia measured by end-tidal carbon dioxide tension during anesthesia is associated with increased 30-day mortality rate. J. Clin. Anesth. 2017, 36, 123–126. [Google Scholar] [CrossRef]
- Corne, S.; Webster, K.; Younes, M. Hypoxic Respiratory Response during Acute Stable Hypocapnia. Am. J. Respir. Crit. Care Med. 2003, 167, 1193–1199. [Google Scholar] [CrossRef]
- Meuret, A.E.; Wilhelm, F.H.; Ritz, T.; Roth, W.T. Feedback of end-tidal pCO2 as a therapeutic approach for panic disorder. J. Psychiatr. Res. 2008, 42, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porges, S.W. Cardiac vagal tone: A physiological index of stress. Neurosci. Biobehav. Rev. 1995, 19, 225–233. [Google Scholar] [CrossRef]
- Wilhelm, F.H.; Trabert, W.; Roth, W.T. Physiologic instability in panic disorder and generalized anxiety disorder. Biol. Psychiatry 2001, 49, 596–605. [Google Scholar] [CrossRef]
- Papp, L.A.; Martinez, J.M.; Klein, D.F.; Coplan, J.D.; Norman, R.G.; Cole, R.; De Jesus, M.J.; Ross, D.; Goetz, R.; Gorman, J.M. Respiratory psychophysiology of panic disorder: Three respiratory challenges in 98 subjects. Am. J. Psychiatry 1997, 154, 1557–1565. [Google Scholar] [PubMed]
- Dimitriadis, Z.; Kapreli, E.; Strimpakos, N.; Oldham, J. Hypocapnia in patients with chronic neck pain: Association with pain, muscle function, and psychologic states. Am. J. Phys. Med. Rehabil. 2013, 92, 746–754. [Google Scholar] [CrossRef] [Green Version]
- Masaoka, Y.; Homma, I. Anxiety and respiratory patterns: Their relationship during mental stress and physical load. Int. J. Psychophysiol. 1997, 27, 153–159. [Google Scholar] [CrossRef]
- Blom, E.H.; Serlachius, E.; Chesney, M.A.; Olsson, E.M.G. Adolescent girls with emotional disorders have a lower end-tidal CO2 and increased respiratory rate compared with healthy controls. Psychophysiology 2014, 51, 412–418. [Google Scholar] [CrossRef] [Green Version]
- Oldenhof, H.; Prätzlich, M.; Ackermann, K.; Baker, R.; Batchelor, M.; Baumann, S.; Bernhard, A.; Clanton, R.; Dikeos, D.; Dochnal, R.; et al. Baseline autonomic nervous system activity in female children and adolescents with conduct disorder: Psychophysiological findings from the FemNAT-CD study. J. Crim. Justice 2019, 65, 101564. [Google Scholar] [CrossRef]
- Silverberg, N.; Iverson, G.; Panenka, W. Accepted Abstracts from the International Brain Injury Association’s 12th World Congress on Brain Injury. Brain Inj. 2017, 31, 719–1017. [Google Scholar]
- Silverberg, N.D.; Panenka, W.J.; Iverson, G.L. Fear Avoidance and Clinical Outcomes from Mild Traumatic Brain Injury. J. Neurotrauma 2018, 35, 1864–1873. [Google Scholar] [CrossRef]
- Greenberg, J.; Mace, R.A.; Funes, C.J.; Silverberg, N.D.; Iverson, G.L.; Caplan, D.N.; Vranceanu, A.-M. Pain Catastrophizing and Limiting Behavior Mediate the Association between Anxiety and Postconcussion Symptoms. J. Psychosom. Res. 2020, 61, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Hilz, M.J.; Aurnhammer, F.; Flanagan, S.R.; Intravooth, T.; Wang, R.; Hösl, K.M.; Pauli, E.; Koehn, J. Eyeball Pressure Stimulation Unveils Subtle Autonomic Cardiovascular Dysfunction in Persons with a History of Mild Traumatic Brain Injury. J. Neurotrauma 2015, 32, 1796–1804. [Google Scholar] [CrossRef] [PubMed]
- Williamson, J.B.; Heilman, K.M.; Porges, E.; Lamb, D.G.; Porges, S.W. A possible mechanism for PTSD symptoms in patients with traumatic brain injury: Central autonomic network disruption. Front. Neuroeng. 2013, 6, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Len, T.K.; Neary, J.P.; Asmundson, G.J.G.; Candow, D.G.; Goodman, D.G.; Bjornson, B.H.; Bhambhani, Y.N. Serial monitoring of CO2 reactivity following sport concussion using hypocapnia and hypercapnia. Brain Inj. 2013, 27, 346–353. [Google Scholar] [CrossRef]
- AlBalawi, T.; Hamner, J.W.; Lapointe, M.; Meehan, W.P.; Tan, C.O. The Relationship between Cerebral Vasoreactivity and Post-Concussive Symptom Severity. J. Neurotrauma 2017, 34, 2700–2705. [Google Scholar] [CrossRef]
- Bishop, S.A.; Dech, R.T.; Guzik, P.; Neary, J.P. Heart rate variability and implication for sport concussion. Clin. Physiol. Funct. Imaging 2018, 38, 733–742. [Google Scholar] [CrossRef]
- Houtveen, J.H.; Rietveld, S.; de Geus, E.J.C. Contribution of tonic vagal modulation of heart rate, central respiratory drive, respiratory depth, and respiratory frequency to respiratory sinus arrhythmia during mental stress and physical exercise. Psychophysiology 2002, 39, 427–436. [Google Scholar] [CrossRef]
- Pöyhönen, M.; Syväoja, S.; Hartikainen, J.; Ruokonen, E.; Takala, J. The effect of carbon dioxide, respiratory rate and tidal volume on human heart rate variability. Acta Anaesthesiol. Scand. 2003, 48, 93–101. [Google Scholar] [CrossRef]
- Laffey, J.G.; Kavanagh, B.P. Hypocapnia. N. Engl. J. Med. 2002, 347, 43–53. [Google Scholar] [CrossRef]
- Colasanti, A.; Salamon, E.; Schruers, K.; Van Diest, R.; Van Duinen, M.; Griez, E. Carbon Dioxide-Induced Emotion and Respiratory Symptoms in Healthy Volunteers. Neuropsychopharmacology 2008, 33, 3103–3110. [Google Scholar] [CrossRef] [Green Version]
- Dhokalia, A.; Parsons, D.J.; Anderson, D.E. Resting End-Tidal CO2 Association with Age, Gender, and Personality. Psychosom. Med. 1998, 60, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Pennebaker, J.W. Health Complaints, Stress, and Distress: Exploring the Central Role of Negative Affectivity. Psychol. Rev. 1989, 96, 234–254. [Google Scholar] [CrossRef] [PubMed]
- Courtney, R. The functions of breathing and its dysfunctions and their relationship to breathing therapy. Int. J. Osteopat. Med. 2009, 12, 78–85. [Google Scholar] [CrossRef]
- Oneda, B.; Ortega, K.C.; Gusmao, J.L.; Araujo, T.G.; Mion, D. Sympathetic nerve activity is decreased during device-guided slow breathing. Hypertens. Res. 2010, 33, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, H.; Cayir, Y.; Kosan, Z.; Tastan, K. Effectiveness of breathing exercises during the second stage of labor on labor pain and duration: A randomized controlled trial. J. Integr. Med. 2017, 15, 456–461. [Google Scholar] [CrossRef]
- Toschi-Dias, E.; Tobaldini, E.; Solbiati, M.; Costantino, G.; Sanlorenzo, R.; Doria, S.; Irtelli, F.; Mencacci, C.; Montano, N. Sudarshan Kriya Yoga improves cardiac autonomic control in patients with anxiety-depression disorders. J. Affect. Disord. 2017, 214, 74–80. [Google Scholar] [CrossRef]
- Jyotsna, V.P.; Ambekar, S.; Singla, R.; Joshi, A.; Dhawan, A.; Kumar, N.; Gupta, N.; Sreenivas, V.; Deepak, K.K. Prospective randomized controlled intervention trial: Comprehensive Yogic Breathing Improves Cardiac autonomic functions and Quality of life in Diabetes. Indian J. Endocrinol. Metab. 2012, 16, S489–S491. [Google Scholar] [CrossRef]
- Teng, H.-C.; Yeh, M.-L.; Wang, M.-H. Walking with controlled breathing improves exercise tolerance, anxiety, and quality of life in heart failure patients: A randomized controlled trial. Eur. J. Cardiovasc. Nurs. 2018, 17, 717–727. [Google Scholar] [CrossRef]
- Lampert, R.; Ickovics, J.; Horwitz, R.; Lee, F. Depressed autonomic nervous system function in African Americans and individuals of lower social class: A potential mechanism of race- and class-related disparities in health outcomes. Am. Heart J. 2005, 150, 153–160. [Google Scholar] [CrossRef]
- Fuller-Rowell, T.E.; Williams, D.R.; Love, G.D.; McKinley, P.S.; Sloan, R.P.; Ryff, C.D. Race Differences in Age-Trends of Autonomic Nervous System Functioning. J. Aging Health 2013, 25, 839–862. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| PPCS | Control | p-Value | |
|---|---|---|---|
| Demographics | (n = 13) | (n = 12) | |
| Sex (n) | |||
| Male (n) | 4 | 6 | 0.33 |
| Female (n) | 9 | 6 | |
| Age (years) | 16.15 (1.86) | 18.50 (3.12) | 0.03 * |
| Education completed (years) | 9.77 (2.01) | 12.58 (2.97) | 0.01 * |
| Medical History | |||
| Migraine (yes) | 3 | 2 | 1 |
| Depression (yes) | 1 | 1 | 1 |
| Anxiety (yes) | 5 | 1 | 0.16 |
| AD/HD (yes) | 1 | 1 | 1 |
| Learning disorder (yes) | 1 | 0 | 1 |
| Taking medication (yes) | 4 | 2 | 0.64 |
| Previously diagnosed concussions | 2.00 (1.08) | 0 (0.0) | <0.001 ** |
| Days since most recent injury | 138.85 (75.76) | -- | -- |
| PPCS | Control | p-Value | |
|---|---|---|---|
| Neurobehavioral Outcomes | (n = 13) | (n = 12) | |
| Pain Catastrophizing Scale | 25.15 (9.66) | 12.33 (8.25) | 0.002 ** |
| PCSI | |||
| Physical | 12.08 (8.77) | 3.42 (5.25) | 0.008 ** |
| Emotional | 8.62 (5.84) | 4.67 (5.84) | .05 |
| Cognitive | 12.85 (8.03) | 3.58 (5.48) | 0.004 ** |
| Sleep/Fatigue | 5.31 (3.99) | 2.08 (2.35) | 0.03 * |
| Total | 39.38 (23.68) | 13.75 (16.86) | 0.002 ** |
| Pre-Injury Total | 5.38 (6.80) | -- | -- |
| Beck Anxiety Inventory | 10.25 (7.57) | 7.58 (6.76) | 0.35 |
| Beck Depression Inventory, 2nd Ed. | 14.08 (7.32) | 7.67 (8.60) | 0.06 |
| Pittsburgh Sleep Quality Index | 8.58 (3.66) | 6.33 (3.92) | 0.16 |
| Neurocognitive Outcomes | |||
| RBANS | |||
| List Learning Total Score | 27.38 (4.23) | 32.17 (2.33) | 0.002 ** |
| Semantic Fluency | 17.92 (2.87) | 21.92 (3.34) | 0.004 ** |
| Coding | 52.85 (8.00) | 59.33 (9.08) | 0.07 |
| List Recall | 6.38 (1.81) | 8.42 (0.90) | 0.002 ** |
| EtCO2 (mmHg) | SaO2 (%) | RR (Breaths per Minute) | PR (Beats per Minute) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PPCS | Control | Combined | PPCS | Control | Combined | PPCS | Control | Combined | PPCS | Control | Combined | |
| Neurobehavioral Outcomes | (n = 13) | (n = 12) | (n = 12) | (n = 12) | (n = 13) | (n = 12) | (n = 13) | (n = 12) | ||||
| Pain Catastrophizing Scale | −0.09 | −0.16 | −0.42 * | 0.34 | 0.02 | 0.15 | −0.07 | 0.5 | 0.22 | 0.38 | 0.58 * | 0.50 * |
| Rumination | 0.03 | −0.22 | −0.40 | 0.07 | −0.18 | 0.01 | 0.00 | 0.52 | 0.27 | 0.38 | 0.62 * | 0.51 * |
| Magnification | −0.12 | 0.03 | −0.21 | 0.5 | −0.04 | 0.24 | −0.29 | 0.34 | 0.01 | 0.16 | 0.33 | 0.26 |
| Helplessness | −0.14 | −0.13 | −0.45 * | 0.38 | 0.13 | 0.2 | 0.04 | 0.37 | 0.23 | 0.42 | 0.45 | .47 * |
| Total | −0.09 | −0.16 | −0.42 * | 0.34 | 0.02 | 0.15 | −0.07 | 0.5 | 0.22 | 0.38 | 0.58 * | 0.50 * |
| PCSI | ||||||||||||
| Physical | −0.07 | −0.34 | −0.42 * | 0.43 | 0.26 | 0.35 | 0.05 | −0.22 | −0.02 | −0.07 | −0.02 | 0.06 |
| Emotional | −0.35 | −0.22 | −0.42 * | 0.69 * | 0.18 | 0.38 | −0.02 | 0.31 | 0.18 | −0.01 | 0.54 | 0.27 |
| Cognitive | −0.20 | −0.16 | −0.45 * | 0.58 * | 0.14 | 0.38 | 0.20 | 0.10 | 0.18 | −0.17 | 0.23 | 0.09 |
| Sleep/Fatigue | −0.05 | −0.43 | −0.38 | 0.29 | −0.18 | 0.20 | 0.25 | 0.14 | 0.22 | −0.28 | 0.43 | 0.03 |
| Total | −0.17 | −0.26 | −0.46 * | 0.70 * | 0.07 | 0.38 | 0.15 | 0.09 | 0.15 | −0.12 | 0.32 | 0.14 |
| Pre-Injury Total | 0.26 | -- | -- | 0.24 | -- | -- | −0.13 | -- | -- | −0.24 | -- | -- |
| Beck Anxiety Inventory | −0.31 | −0.18 | −0.32 | 0.46 | −0.03 | 0.16 | −0.12 | 0.22 | 0.08 | 0.47 | 0.43 | 0.47 * |
| Beck Depression Inventory, 2nd Ed. | −0.53 | −0.35 | −0.55 ** | 0.73 * | 0.16 | 0.35 | 0.37 | 0.42 | 0.41 * | 0.67 * | 0.53 | 0.61 ** |
| Pittsburgh Sleep Quality Index | 0.10 | 0.31 | −0.01 | 0.42 | −0.09 | 0.08 | 0.36 | 0.29 | 0.32 | −0.19 | 0.41 | 0.14 |
| Neurocognitive Outcomes | ||||||||||||
| RBANS | ||||||||||||
| List Learning Total Score | 0.05 | 0.13 | 0.38 | 0.03 | −0.03 | −0.02 | −0.34 | 0.05 | −0.20 | −0.16 | 0.32 | −0.16 |
| Semantic Fluency | −0.12 | 0.28 | 0.36 | −0.07 | −0.51 | −0.32 | 0.38 | −0.42 | −0.12 | 0.18 | −0.51 | −0.23 |
| Coding | −0.15 | 0.33 | 0.26 | −0.41 | −0.01 | −0.20 | −0.33 | −0.60 * | −0.48 * | −0.15 | −0.65 * | −0.42 * |
| List Recall | 0.05 | 0.03 | 0.37 | −0.18 | 0.15 | −0.16 | −0.1 | −0.38 | −0.21 | 0.23 | −0.04 | −0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Snyder, A.; Sheridan, C.; Tanner, A.; Bickart, K.; Sullan, M.; Craske, M.; Choe, M.; Babikian, T.; Giza, C.; Asarnow, R. Cardiorespiratory Functioning in Youth with Persistent Post-Concussion Symptoms: A Pilot Study. J. Clin. Med. 2021, 10, 561. https://doi.org/10.3390/jcm10040561
Snyder A, Sheridan C, Tanner A, Bickart K, Sullan M, Craske M, Choe M, Babikian T, Giza C, Asarnow R. Cardiorespiratory Functioning in Youth with Persistent Post-Concussion Symptoms: A Pilot Study. Journal of Clinical Medicine. 2021; 10(4):561. https://doi.org/10.3390/jcm10040561
Chicago/Turabian StyleSnyder, Aliyah, Christopher Sheridan, Alexandra Tanner, Kevin Bickart, Molly Sullan, Michelle Craske, Meeryo Choe, Talin Babikian, Christopher Giza, and Robert Asarnow. 2021. "Cardiorespiratory Functioning in Youth with Persistent Post-Concussion Symptoms: A Pilot Study" Journal of Clinical Medicine 10, no. 4: 561. https://doi.org/10.3390/jcm10040561